
Programmatic Cost-Effectiveness of a Second-Time Visit to Detect New Tuberculosis and Diabetes Mellitus in TB Contact Tracing in Myanmar


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Setting
2.3. Contact Tracing in the Study
2.4. Data Collection
2.5. Evaluation of Healthcare Programmatic Operational Costs
2.5.1. Human Resource Costs
2.5.2. Capital Costs
2.5.3. Recurrent Costs
2.5.4. Overhead Costs
2.5.5. Compliance to Screening
2.5.6. Disability-Adjusted Life Year Averted
2.5.7. Decision Tree
2.6. Data Analysis
2.6.1. Probabilistic Sensitivity Analysis
2.6.2. One-Way Sensitivity Analysis
3. Results
3.1. Compliance to Screening
3.2. Operational Costs and DALY Averted
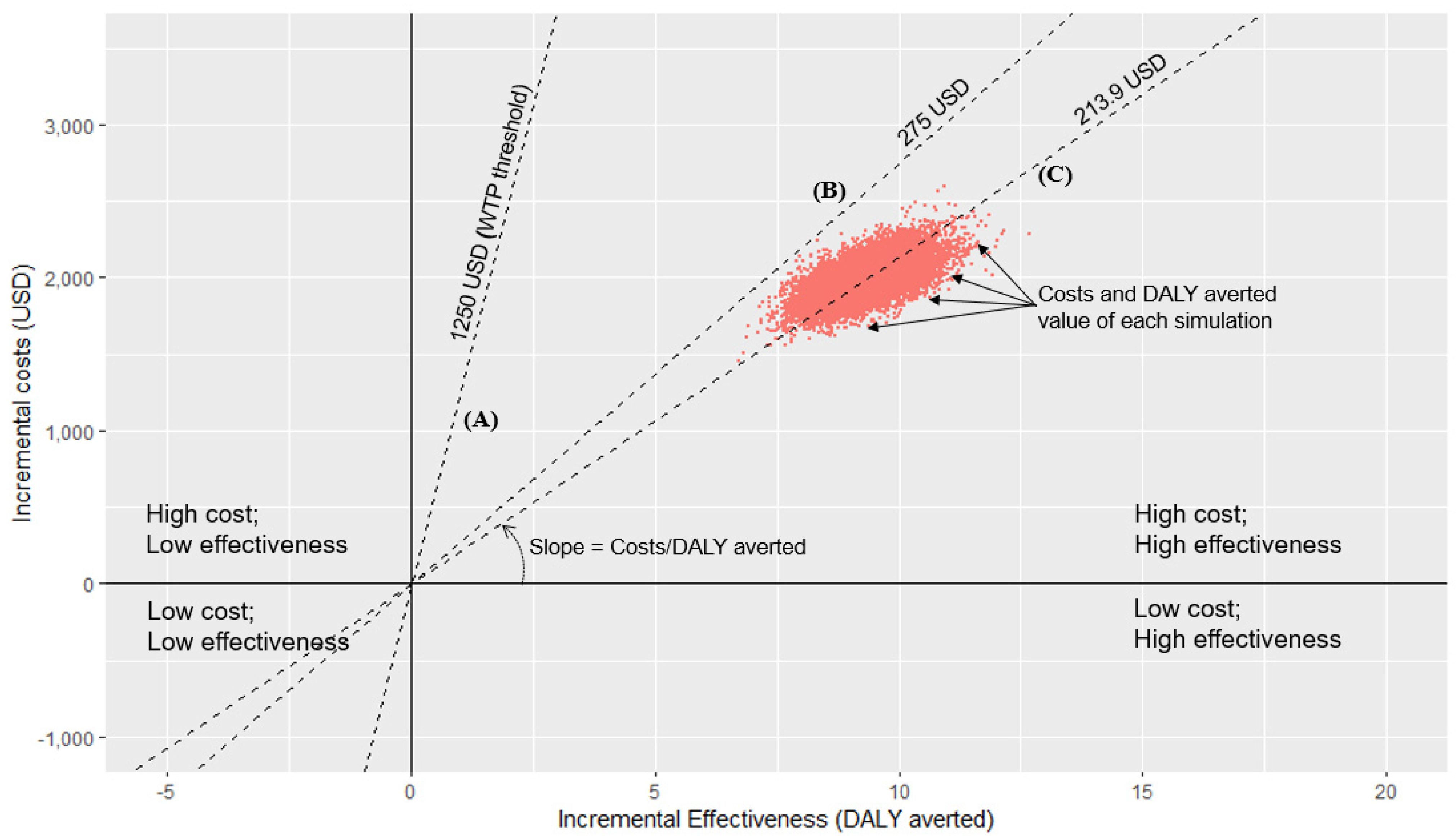
3.3. Cost-Effectiveness Analysis of All Contacts Using Monte Carlo Simulation
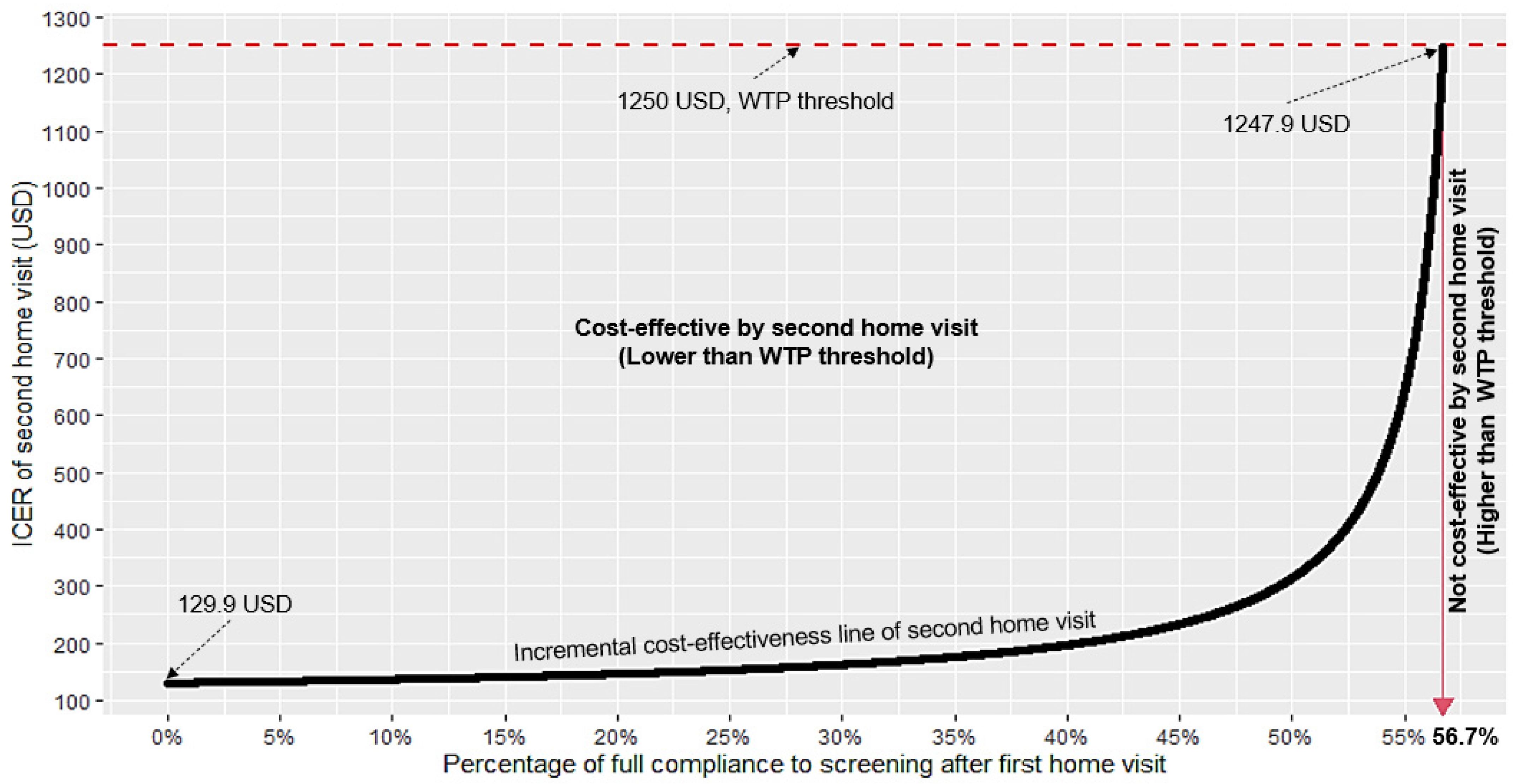
3.4. One-Way Sensitivity Analysis for Different Percentages of Full Compliance after the First Home Visit to Assess the Cost-Effectiveness of a Second-Time Visit
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DM | diabetes mellitus |
| TB | tuberculosis |
| DALY | disability-adjusted life years |
| GDP | gross domestic product |
| USD | US dollars |
| WHO | World Health Organization |
| CXR | chest X-ray |
| RBG | random blood glucose |
| FBG | fasting blood glucose |
| MMK | Myanmar kyat |
| ICER | incremental cost-effectiveness ratio |
| WTP | willingness to pay |
| LMICs | low- and middle-income countries |
References
- World Health Organization. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019; ISBN 978-92-4-156571-4.
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009.
- IDF Diabetes Atlas 9th Edition 2019. Available online: https://www.diabetesatlas.org/en/ (accessed on 16 September 2020).
- Global Tuberculosis Report. 2020. Available online: https://www.who.int/publications-detail-redirect/9789240013131 (accessed on 20 March 2022).
- Latt, T.; Zaw, K.; Ko, K.; Ohnmar, M.; Hlaing, M.; Oo, E.; Thein, K. Report on National Survey of Diabetes Mellitus and Risk Factors for Non Communicable Diseases in Myanmar in 2014; Ministry of Health and Sports: Nay Pyi Taw, Myanmar, 2014.
- Lönnroth, K.; Roglic, G.; Harries, A.D. Improving Tuberculosis Prevention and Care through Addressing the Global Diabetes Epidemic: From Evidence to Policy and Practice. Lancet Diabetes Endocrinol. 2014, 2, 730–739. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Working Group on the Inclusion of NCDs in Other Programmatic Areas: WHO Global Coordination Mechanism on the Prevention and Control of Noncommunicable Diseases (Working Group 3.1 (2016–2017); World Health Organization: Geneva, Switzerland, 2018.
- Shah, L.; Rojas, M.; Mori, O.; Zamudio, C.; Kaufman, J.S.; Otero, L.; Gotuzzo, E.; Seas, C.; Brewer, T.F. Cost-Effectiveness of Active Case-Finding of Household Contacts of Pulmonary Tuberculosis Patients in a Low HIV, Tuberculosis-Endemic Urban Area of Lima, Peru. Epidemiol. Infect. 2017, 145, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Yadav, R.P.; Nishikiori, N.; Satha, P.; Eang, M.T.; Lubell, Y. Cost-Effectiveness of a Tuberculosis Active Case Finding Program Targeting Household and Neighborhood Contacts in Cambodia. Am. J. Trop. Med. Hyg. 2014, 90, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Aye, L.L.; Tripathy, J.P.; Maung Maung, T.; Oo, M.M.; Nwe, M.L.; Thu, H.M.M.; Ko, K.; Kaung, K.K. Experiences from the Pilot Implementation of the Package of Essential Non-Communicable Disease Interventions (PEN) in Myanmar, 2017–2018: A Mixed Methods Study. PLoS ONE 2020, 15, e0229081. [Google Scholar] [CrossRef] [PubMed]
- TB/DM Collaborative Activities Guideline, 1st ed.; National Tuberculosis Program, Ministry of Health and Sports: Nay Pyi Taw, Myanmar, 2018.
- American Diabetes Association Professional Practice Committee 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S17–S38. [Google Scholar] [CrossRef]
- Pastakia, S.D.; Ali, S.M.; Kamano, J.H.; Akwanalo, C.O.; Ndege, S.K.; Buckwalter, V.L.; Vedanthan, R.; Bloomfield, G.S. Screening for Diabetes and Hypertension in a Rural Low Income Setting in Western Kenya Utilizing Home-Based and Community-Based Strategies. Glob. Health 2013, 9, 1–9. [Google Scholar] [CrossRef][Green Version]
- Gebregergs, G.B.; Alemu, W.G. Household Contact Screening Adherence among Tuberculosis Patients in Northern Ethiopia. PLoS ONE 2015, 10, e0125767. [Google Scholar] [CrossRef]
- Tornee, S.; Kaewkungwal, J.; Fungladda, W.; Silachamroon, U. others Factors Associated with the Household Contact Screening Adherence of Tuberculosis Patients. Southeast Asian J. Trop. Med. Public Health 2005, 36, 331. [Google Scholar]
- Kigozi, N.G.; Heunis, J.C.; Engelbrecht, M.C. Yield of Systematic Household Contact Investigation for Tuberculosis in a High-Burden Metropolitan District of South Africa. BMC Public Health 2019, 19, 867. [Google Scholar] [CrossRef]
- Morrison, J.; Pai, M.; Hopewell, P.C. Tuberculosis and Latent Tuberculosis Infection in Close Contacts of People with Pulmonary Tuberculosis in Low-Income and Middle-Income Countries: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2008, 8, 359–368. [Google Scholar] [CrossRef]
- Aung, W.P.; Htet, A.S.; Bjertness, E.; Stigum, H.; Chongsuvivatwong, V.; Kjøllesdal, M.K.R. Urban–Rural Differences in the Prevalence of Diabetes Mellitus among 25–74 Year-Old Adults of the Yangon Region, Myanmar: Two Cross-Sectional Studies. BMJ Open 2018, 8, e020406. [Google Scholar] [CrossRef] [PubMed]
- Annual Report 2016; National Tuberculosis Programme, Ministry of Health and Sports: Nay Pyi Taw, Myanmar, 2016.
- Tuberculosis Contact Investigation Standard Operating Procedure; National Tuberculosis Programme, Ministry of Health and Sports: Nay Pyi Taw, Myanmar, 2019.
- World Health Organization. Evidence and Research Gaps Identified during Development of Policy Guidelines for Tuberculosis; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-004047-2.
- Jo, Y.; Mirzoeva, F.; Chry, M.; Qin, Z.Z.; Codlin, A.; Bobokhojaev, O.; Creswell, J.; Sohn, H. Standardized Framework for Evaluating Costs of Active Case-Finding Programs: An Analysis of Two Programs in Cambodia and Tajikistan. PLoS ONE 2020, 15, e0228216. [Google Scholar] [CrossRef] [PubMed]
- Htet, K.K.K.; Liabsuetrakul, T.; Thein, S. Cost-Effectiveness of a New Strategy to Detect Pulmonary Tuberculosis in Household Contacts in Myanmar. Int. J. Tuberc. Lung Dis. 2017, 21, 181–187. [Google Scholar] [CrossRef]
- Reference Exchange Rate—History. Available online: https://forex.cbm.gov.mm/index.php/fxrate/history (accessed on 6 June 2022).
- Myanmar—Corporate—Deductions. Available online: https://taxsummaries.pwc.com/myanmar/corporate/deductions (accessed on 22 April 2022).
- Shwe, A.W.; Riewpaiboon, A. Unit Cost Analysis of Medical Services at Different Levels of Health Facilities of a Township in Myanmar. Pharm Sci Asia 2019, 46, 250–259. [Google Scholar] [CrossRef]
- Health Impacts: Averted Disability-Adjusted Life Years (ADALYs)|The Gold Standard. Available online: https://www.goldstandard.org/articles/health-impacts-averted-disability-adjusted-life-years-adalys (accessed on 6 June 2022).
- Kheang, S.T.; Theang, H.; Eam, K.K.; Eang, M.T.; Kong, S.; Loun, C.; Olkkonen, A.; AlMossawi, H.J.; Kak, N. Bidirectional Screening of Diabetes Mellitus and Tuberculosis in Cambodia. J. Trop. Dis. 2019, 7, 1–5. [Google Scholar] [CrossRef][Green Version]
- World Health Organization; Baltussen, R.M.P.M.; Adam, T.; Tan-Torres Edejer, T.; Hutubessy, R.C.W.; Acharya, A.; Evans, D.B.; Murray, C.J.L. WHO-CHOICE Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis; Tan-Torres Edejer, T., Ed.; World Health Organization: Geneva, Switzerland, 2003. Available online: https://apps.who.int/iris/handle/10665/42699 (accessed on 6 June 2022).
- Vassall, A.; van Kampen, S.; Sohn, H.; Michael, J.S.; John, K.R.; den Boon, S.; Davis, J.L.; Whitelaw, A.; Nicol, M.P.; Gler, M.T.; et al. Rapid Diagnosis of Tuberculosis with the Xpert MTB/RIF Assay in High Burden Countries: A Cost-Effectiveness Analysis. PLOS Med. 2011, 8, e1001120. [Google Scholar] [CrossRef] [PubMed]
- Hussain, H.; Mori, A.T.; Khan, A.J.; Khowaja, S.; Creswell, J.; Tylleskar, T.; Robberstad, B. The Cost-Effectiveness of Incentive-Based Active Case Finding for Tuberculosis (TB) Control in the Private Sector Karachi, Pakistan. BMC Health Serv. Res. 2019, 19, 690. [Google Scholar] [CrossRef]
- Woldesemayat, E.M. Cost-Effectiveness of Follow-Up of Chronic Coughers in Detecting Smear-Positive Tuberculosis in South Ethiopia. CEOR 2021, 13, 737–744. [Google Scholar] [CrossRef]
- Basu, S.; Flood, D.; Geldsetzer, P.; Theilmann, M.; Marcus, M.E.; Ebert, C.; Mayige, M.; Wong-McClure, R.; Farzadfar, F.; Saeedi Moghaddam, S.; et al. Estimated Effect of Increased Diagnosis, Treatment, and Control of Diabetes and Its Associated Cardiovascular Risk Factors among Low-Income and Middle-Income Countries: A Microsimulation Model. Lancet Glob. Health 2021, 9, e1539–e1552. [Google Scholar] [CrossRef]
- EpiData Software—Http://Www.Epidata.Dk. Available online: http://www.epidata.dk/examples.php (accessed on 5 August 2020).
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 21 January 2020).
- GDP per Capita (Current US$)—Myanmar|Data. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=MM (accessed on 19 March 2022).
- Jain, R.; Grabner, M.; Onukwugha, E. Sensitivity Analysis in Cost-Effectiveness Studies: From Guidelines to Practice. Pharmacoeconomics 2011, 29, 297–314. [Google Scholar] [CrossRef]
- Hatswell, A.J.; Bullement, A.; Briggs, A.; Paulden, M.; Stevenson, M.D. Probabilistic Sensitivity Analysis in Cost-Effectiveness Models: Determining Model Convergence in Cohort Models. PharmacoEconomics 2018, 36, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Ordóñez, J.E.; Orozco, J.J. Cost-Effectiveness Analysis of the Available Pneumococcal Conjugated Vaccines for Children under Five Years in Colombia. Cost Eff. Resour. Alloc. 2015, 13, 6. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Picot, J.; Cooper, K.; Bryant, J.; Clegg, A.J. The Clinical Effectiveness and Cost-Effectiveness of Bortezomib and Thalidomide in Combination Regimens with an Alkylating Agent and a Corticosteroid for the First-Line Treatment of Multiple Myeloma: A Systematic Review and Economic Evaluation. Health Technol. Assess. 2011, 15, 1–204. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.M.; Clarke, P.M.; Wolstenholme, J.L.; Wordsworth, S. Applied Methods of Cost-Effectiveness Analysis in Healthcare; OUP: Oxford, UK, 2010; Volume 3, ISBN 0-19-100803-6. [Google Scholar]
- Papadopoulos, C.E.; Yeung, H. Uncertainty Estimation and Monte Carlo Simulation Method. Flow Meas. Instrum. 2001, 12, 291–298. [Google Scholar] [CrossRef]
- World Health Organization. Compendium of WHO Guidelines and Associated Standards: Ensuring Optimum Delivery of the Cascade of Care for Patients with Tuberculosis, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-151410-1.
- Kigozi, G.; Engelbrecht, M.; Heunis, C.; Rensburg, A.J. van Household Contact Non-Attendance of Clinical Evaluation for Tuberculosis: A Pilot Study in a High Burden District in South Africa. BMC Infect. Dis. 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Hussain, H.; Malik, A.; Ahmed, J.F.; Siddiqui, S.; Amanullah, F.; Creswell, J.; Tylleskär, T.; Robberstad, B. Cost-Effectiveness of Household Contact Investigation for Detection of Tuberculosis in Pakistan. BMJ Open 2021, 11, e049658. [Google Scholar] [CrossRef]
- Toscano, C.M.; Zhuo, X.; Imai, K.; Duncan, B.B.; Polanczyk, C.A.; Zhang, P.; Engelgau, M.; Schmidt, M.I. Cost-Effectiveness of a National Population-Based Screening Program for Type 2 Diabetes: The Brazil Experience. Diabetol. Metab. Syndr. 2015, 7, 95. [Google Scholar] [CrossRef]
- Dukpa, W.; Teerawattananon, Y.; Rattanavipapong, W.; Srinonprasert, V.; Tongsri, W.; Kingkaew, P.; Yothasamut, J.; Wangchuk, D.; Dorji, T.; Wangmo, K. Is Diabetes and Hypertension Screening Worthwhile in Resource-Limited Settings? An Economic Evaluation Based on a Pilot of a Package of Essential Non-Communicable Disease Interventions in Bhutan. Health Policy Plan. 2015, 30, 1032–1043. [Google Scholar] [CrossRef]
- Duncan, B.B.; Cousin, E.; Naghavi, M.; Afshin, A.; França, E.B.; Passos, V.M.d.A.; Malta, D.; Nascimento, B.R.; Schmidt, M.I. The Burden of Diabetes and Hyperglycemia in Brazil: A Global Burden of Disease Study 2017. Popul. Health Metr. 2020, 18, 9. [Google Scholar] [CrossRef]
- Chhetri, V.; Pokhrel, H.P.; Zangmo, L.; Dzed, L. Diabetes Case Burden at Central Regional Referral Hospital, Gelephu, Bhutan; A Retrospective Study. IHRJ 2020, 4, 38–43. [Google Scholar] [CrossRef]
- Htet, K.K.K.; Liabsuetrakul, T.; Thein, S.; McNeil, E.B.; Chongsuvivatwong, V. Improving Detection of Tuberculosis among Household Contacts of Index Tuberculosis Patients by an Integrated Approach in Myanmar: A Cross-Sectional Study. BMC Infect. Dis. 2018, 18, 660. [Google Scholar] [CrossRef]
- Li, L.; Lin, Y.; Mi, F.; Tan, S.; Liang, B.; Guo, C.; Shi, L.; Liu, L.; Gong, F.; Li, Y.; et al. Screening of Patients with Tuberculosis for Diabetes Mellitus in China. Trop. Med. Int. Health 2012, 17, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, C.R.; Forouhi, N.G.; Roglic, G.; Williams, B.G.; Lauer, J.A.; Dye, C.; Unwin, N. Diabetes and Tuberculosis: The Impact of the Diabetes Epidemic on Tuberculosis Incidence. BMC Public Health 2007, 7, 234. [Google Scholar] [CrossRef] [PubMed]
- Armstrong-Hough, M.; Turimumahoro, P.; Meyer, A.J.; Ochom, E.; Babirye, D.; Ayakaka, I.; Mark, D.; Ggita, J.; Cattamanchi, A.; Dowdy, D.; et al. Drop-out from the Tuberculosis Contact Investigation Cascade in a Routine Public Health Setting in Urban Uganda: A Prospective, Multi-Center Study. PLoS ONE 2017, 12, e0187145. [Google Scholar] [CrossRef] [PubMed]
- The End TB Strategy. Available online: https://www.who.int/teams/global-tuberculosis-programme/the-end-tb-strategy (accessed on 25 November 2022).



{kind=link}
{kind=link}
| First-Time Visit n = 519 | Second-Time Visit n = 291 | Two-Time Visits n = 519 | |
|---|---|---|---|
| Level of compliance | |||
| Full compliance | 221 (42.5) | 178 (65.0) | 399 (76.9) |
| Compliance to TB screening | 231 (44.5) | 184 (67.2) | 415 (79.9) |
| Compliance to DM screening | 127 (40.6) | 167 (89.8) | 294 (93.9) |
| New TB cases detected | 15 | 5 | 20 |
| DALY averted * | 27.0 | 9.0 | 36.0 |
| New DM case detected | 4 | 9 | 13 |
| DALY averted * | 0.2 | 0.3 | 0.5 |
| Total DALY averted | 27.2 | 9.3 | 36.5 |
| Operational costs (USD) | |||
| Total costs | 3280.95 | 1989.02 | 5269.97 |
| Costs per household contact | 6.32 | 6.83 | 10.15 |
| Costs per DALY averted | 120.62 | 213.87 *** | 144.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zayar, N.N.; Chotipanvithayakul, R.; Htet, K.K.K.; Chongsuvivatwong, V. Programmatic Cost-Effectiveness of a Second-Time Visit to Detect New Tuberculosis and Diabetes Mellitus in TB Contact Tracing in Myanmar. Int. J. Environ. Res. Public Health 2022, 19, 16090. https://doi.org/10.3390/ijerph192316090
Zayar NN, Chotipanvithayakul R, Htet KKK, Chongsuvivatwong V. Programmatic Cost-Effectiveness of a Second-Time Visit to Detect New Tuberculosis and Diabetes Mellitus in TB Contact Tracing in Myanmar. International Journal of Environmental Research and Public Health. 2022; 19(23):16090. https://doi.org/10.3390/ijerph192316090
Chicago/Turabian StyleZayar, Nyi Nyi, Rassamee Chotipanvithayakul, Kyaw Ko Ko Htet, and Virasakdi Chongsuvivatwong. 2022. "Programmatic Cost-Effectiveness of a Second-Time Visit to Detect New Tuberculosis and Diabetes Mellitus in TB Contact Tracing in Myanmar" International Journal of Environmental Research and Public Health 19, no. 23: 16090. https://doi.org/10.3390/ijerph192316090
APA StyleZayar, N. N., Chotipanvithayakul, R., Htet, K. K. K., & Chongsuvivatwong, V. (2022). Programmatic Cost-Effectiveness of a Second-Time Visit to Detect New Tuberculosis and Diabetes Mellitus in TB Contact Tracing in Myanmar. International Journal of Environmental Research and Public Health, 19(23), 16090. https://doi.org/10.3390/ijerph192316090