
Nursing Home-Sensitive Hospitalizations and the Relevance of Telemedicine: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
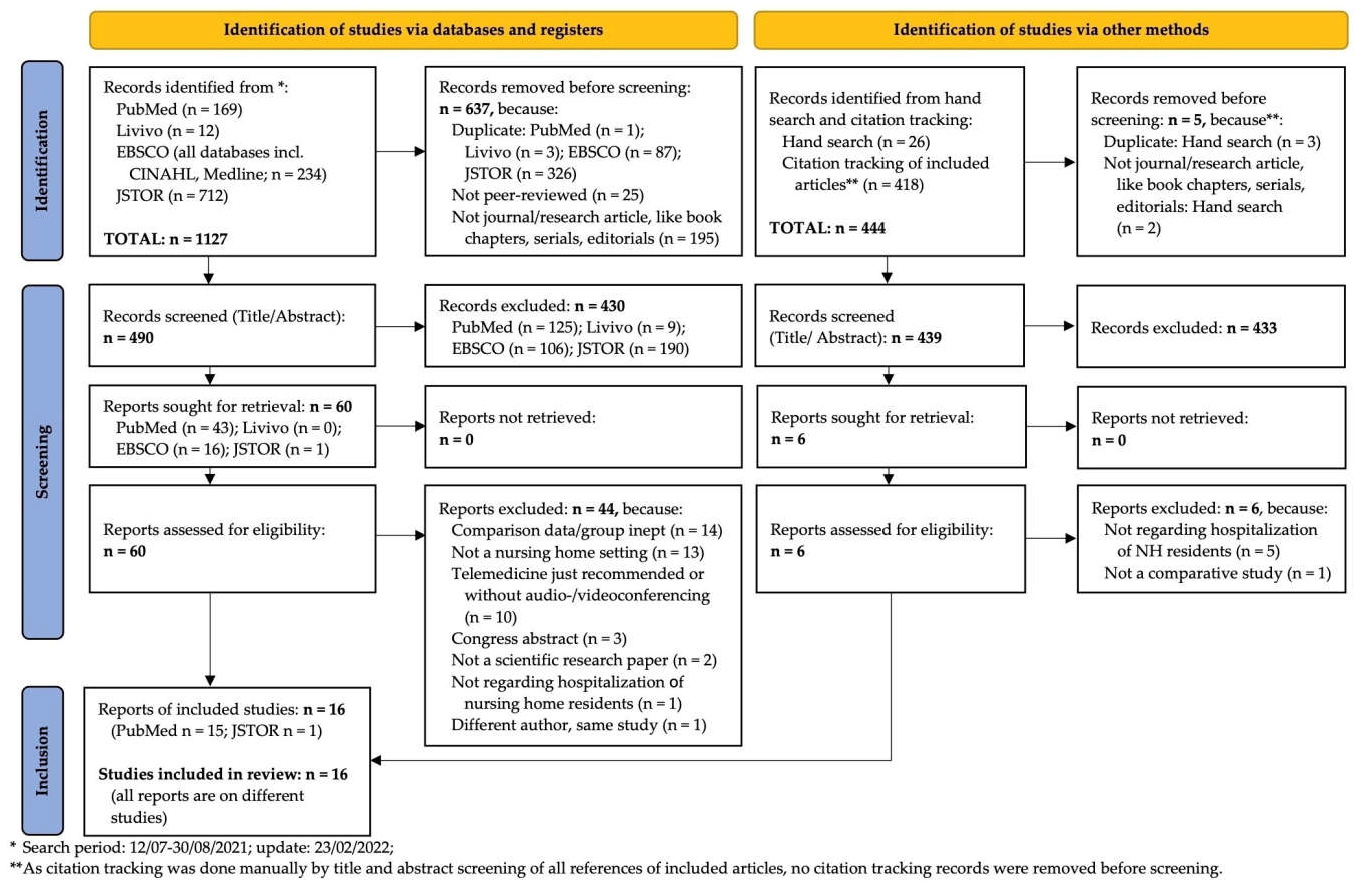
2.3. Study Selection
2.4. Data Evaluation
2.5. Data Extraction
- (1)
- Study descriptors (year and country of origin, study design, study aim/objective and population descriptors, such as age, gender and (co)morbidities).
- (2)
- Focus (telemedicine intervention details/technology(s)/strategies, involved health care professionals as well as duration of intervention and service hours in which telemedicine was offered (weekdays/after hours) and the purpose of telemedicine, which is operationalized into monitoring, diagnostic and therapeutic properties).
- (3)
- Health outcomes for the primary research question (in this study, emergency department visits, hospitalization and mortality rate).
- (4)
- Procedural/facility outcomes for the secondary research question (in this study, cost-effectiveness and satisfaction of health care professionals).
3. Results
3.1. Study Design
3.2. Setting
3.3. Population
3.4. (Co)Morbidity and Involved Medical Specialties
3.5. Telemedicine Intervention
3.6. Outcomes on the Primary Review Question
3.7. Outcomes on the Secondary Review Questions
4. Discussion
4.1. Limitations
4.2. Recommendations for Future Research
4.3. Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APN | advanced practice nurse |
| C | control group |
| CMS | Center for Medicare and Medicaid Services |
| ED | Emergency Department |
| e.g., | for instance |
| etc. | etcetera |
| HRRP | Hospital Readmissions Reduction Program |
| I | intervention group |
| ICT | information and communication technology |
| JBI | Joanna Briggs Institute; |
| LTC | long-term care facility/facilities |
| M.P.V.-D. | author’s initials of first author |
| n.a. | not applicable |
| n.i. | not indicated |
| NH | nursing home/s; |
| NHR | nursing home resident/s |
| NHSC | nursing home-sensitive condition/s |
| ONC | U.S. Department of Health and Human Services’ Office of the National Coordinator for Health Information Technology |
| PRISMA-ScR | Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. |
| PU | pressure ulcer |
| RCT | randomized controlled trial |
| S.B.-J. | author’s initials of second author |
| SNF | skilled nursing facility/facilities |
| Tmed | telemedicine |
| USD | United States Dollar/s |
| X (Table 2) | involved |
| ↓ (Table 2) | goes down |
| ↑ (Table 2) | goes up |
| ? (Table 2) | ambivalent study results |
References
- Burke, R.E.; Whitfield, E.A.; Hittle, D.; Min, S.-J.; Levy, C.; Prochazka, A.V.; Coleman, E.A.; Schwartz, R.; Ginde, A.A. Hospital Readmission from Post-Acute Care Facilities: Risk Factors, Timing, and Outcomes. J. Am. Med. Dir. Assoc. 2016, 17, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Bohnet-Joschko, S.; Valk-Draad, M.P.; Schulte, T.; Groene, O. Nursing home-sensitive conditions: Analysis of routine health insurance data and modified Delphi analysis of potentially avoidable hospitalizations. F1000Research 2022, 10, 1223. [Google Scholar] [CrossRef]
- Mor, V.; Intrator, O.; Feng, Z.; Grabowski, D.C. The Revolving Door of Rehospitalization from Skilled Nursing Facilities. Health Aff. 2010, 29, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Ouslander, J.G.; Lamb, G.; Perloe, M.; Givens, J.H.; Kluge, L.; Rutland, T.; Atherly, A.; Saliba, D. Potentially Avoidable Hospitalizations of Nursing Home Residents: Frequency, Causes, and Costs. J. Am. Geriatr. Soc. 2010, 58, 627–635. [Google Scholar] [CrossRef]
- Gozalo, P.; Teno, J.M.; Mitchell, S.L.; Skinner, J.; Bynum, J.; Tyler, D.; Mor, V. End-of-Life Transitions among Nursing Home Residents with Cognitive Issues. N. Engl. J. Med. 2011, 365, 1212–1221. [Google Scholar] [CrossRef] [Green Version]
- Federal Statistical Office of Germany (Destatis). Ältere Menschen in Deutschland und der EU; Statistisches Bundesamt: Wiesbaden, Germany, 2016. [Google Scholar]
- Federal Statistical Office of Germany (Destatis). Ausblick auf die Bevölkerungsentwicklung in Deutschland und den Bundesländern nach dem Corona-Jahr 2020. Erste Mittelfristige Bevölkerungsvorausberechnung 2021 bis 2035; Statistisches Bundesamt: Wiesbaden, Germany, 2021. [Google Scholar]
- Federal Ministry of Health of Germany (BMG). Zahlen und Fakten zur Pflegeversicherung. Available online: https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Statistiken/Pflegeversicherung/Zahlen_und_Fakten/Zahlen_und_Fakten_der_SPV_Juni_2021_bf.pdf (accessed on 10 April 2022).
- Federal Statistical Office of Germany (Destatis). Pflegestatistik. Pflege im Rahmen der Pflegeversicherung. Deutschlandergebnisse 2019; Statistisches Bundesamt: Wiesbaden, Germany, 2020. [Google Scholar]
- OECD. Long-Term Care Resources and Utilisation. Available online: https://stats.oecd.org/viewhtml.aspx?datasetcode=HEALTH_LTCR&lang=en# (accessed on 30 June 2022).
- Nowossadeck, E. Population Aging and Hospitalization for Chronic Disease in Germany. Dtsch. Arztebl. Int. 2012, 109, 151–157. [Google Scholar] [CrossRef]
- Palleschi, L.; De Alfieri, W.; Salani, B.; Fimognari, F.L.; Marsilii, A.; Pierantozzi, A.; Di Cioccio, L.; Zuccaro, S.M. Functional Recovery of Elderly Patients Hospitalized in Geriatric and General Medicine Units. The PROgetto DImissioni in GEriatria Study. J. Am. Geriatr. Soc. 2011, 59, 193–199. [Google Scholar] [CrossRef]
- Page, D.B.; Donnelly, J.; Wang, H.E. Community-, Healthcare-, and Hospital-Acquired Severe Sepsis Hospitalizations in the University HealthSystem Consortium. Crit. Care Med. 2015, 43, 1945–1951. [Google Scholar] [CrossRef] [Green Version]
- Palese, A.; Gonella, S.; Moreale, R.; Guarnier, A.; Barelli, P.; Zambiasi, P.; Allegrini, E.; Bazoli, L.; Casson, P.; Marin, M.; et al. Hospital-acquired functional decline in older patients cared for in acute medical wards and predictors: Findings from a multicentre longitudinal study. Geriatr. Nurs. 2016, 37, 192–199. [Google Scholar] [CrossRef]
- Haley, R.W.; Culver, D.H.; White, J.W.; Morgan, W.M.; Emori, T.G. The Nationwide Nosocomial Infection Rate. Am. J. Epidemiol. 1985, 121, 159–167. [Google Scholar] [CrossRef]
- Krumholz, H.M. Post-Hospital Syndrome—An Acquired, Transient Condition of Generalized Risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef] [Green Version]
- Donzé, J.; Lipsitz, S.; Bates, D.W.; Schnipper, J.L. Causes and patterns of readmissions in patients with common comorbidities: Retrospective cohort study. BMJ 2013, 347, f7171. [Google Scholar] [CrossRef] [Green Version]
- Ouslander, J.G.; Berenson, R.A. Reducing Unnecessary Hospitalizations of Nursing Home Residents. N. Engl. J. Med. 2011, 365, 1165–1167. [Google Scholar] [CrossRef] [Green Version]
- Rantz, M.J.; Popejoy, L.; Vogelsmeier, A.; Galambos, C.; Alexander, G.; Flesner, M.; Crecelius, C.; Ge, B.; Petroski, G. Successfully Reducing Hospitalizations of Nursing Home Residents: Results of the Missouri Quality Initiative. J. Am. Med. Dir. Assoc. 2017, 18, 960–966. [Google Scholar] [CrossRef]
- Hullick, C.; Conway, J.; Higgins, I.; Hewitt, J.; Dilworth, S.; Holliday, E.; Attia, J. Emergency department transfers and hospital admissions from residential aged care facilities: A controlled pre-post design study. BMC Geriatr. 2016, 16, 102. [Google Scholar] [CrossRef] [Green Version]
- Grabowski, D.C.; Aschbrenner, K.A.; Rome, V.F.; Bartels, S.J. Review: Quality of Mental Health Care for Nursing Home Residents: A Literature Review. Med. Care Res. Rev. 2010, 67, 627–656. [Google Scholar] [CrossRef] [Green Version]
- Cooper, S.L.; Carleton, H.L.; Chamberlain, S.; Cummings, G.G.; Bambrick, W.; Estabrooks, C.A. Burnout in the nursing home health care aide: A systematic review. Burn. Res. 2016, 3, 76–87. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Marston, L.; Barber, J.; Livingston, D.; Rapaport, P.; Higgs, P.; Livingston, G. Do care homes deliver person-centred care? A cross-sectional survey of staff-reported abusive and positive behaviours towards residents from the MARQUE (Managing Agitation and Raising Quality of Life) English national care home survey. PLoS ONE 2018, 13, e0193399. [Google Scholar] [CrossRef]
- Song, Y.; Hoben, M.; Norton, P.; Estabrooks, C.A. Association of Work Environment with Missed and Rushed Care Tasks among Care Aides in Nursing Homes. JAMA Netw. Open 2020, 3, e1920092. [Google Scholar] [CrossRef]
- Quigley, D.D.; Chastain, A.M.; Kang, J.A.; Bronstein, D.; Dick, A.W.; Stone, P.W.; Shang, J. Systematic Review of Rural and Urban Differences in Care Provided by Home Health Agencies in the United States. J. Am. Med. Dir. Assoc. 2022, in press, uncorrected proof. [Google Scholar] [CrossRef]
- Chulz, M.; Czwikla, J.; Schmidt, A.; Tsiasioti, C.; Schwinger, A.; Gerhardus, A.; Schmiemann, G.; Wolf-Ostermann, K.; Rothgang, H. Medical specialist undertreatment in nursing home residents-Prevalence and extrapolation. Z Gerontol. Geriatr. 2021, 54, 479–484. [Google Scholar] [CrossRef]
- Valk-Draad, M.P.; Schulte, T.; Bohnet-Joschko, S. Reduzierung der Hospitalisierung unter Pflegeheimbewohnenden in Deutschland durch Sensibilisierung für Pflegeheim-sensitive Diagnosen. In20. Deutscher Kongress für Versorgungsforschung (DKVF) sine loco [digital], 6-8 October 2021; German Medical Science GMS Publishing House: Düsseldorf, Germany, 2021; Doc21dkvf431. [Google Scholar] [CrossRef]
- Trahan, L.M.; Spiers, J.A.; Cummings, G.G. Decisions to Transfer Nursing Home Residents to Emergency Departments: A Scoping Review of Contributing Factors and Staff Perspectives. J. Am. Med. Dir. Assoc. 2016, 17, 994–1005. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.L.; Georgiou, A.; Doughty, K.; Hornblow, A.; Livingstone, A.; Dougherty, M.; Jacobs, S.; Fisk, M.J. Advancing health information technology roadmaps in long term care. Int. J. Med. Inform. 2020, 136, 104088. [Google Scholar] [CrossRef] [PubMed]
- McDermott, C.; Coppin, R.; Little, P.; Leydon, G.M. Hospital admissions from nursing homes: A qualitative study of GP decision making. Br. J. Gen. Pract. 2012, 62, e538–e545. [Google Scholar] [CrossRef] [Green Version]
- Ramroth, H.; Specht-Leible, N.; König, H.-H.; Mohrmann, M.; Brenner, H. Inanspruchnahme stationärer Kranken-hausleistungen durch Pflegeheimbewohner. Dtsch. Ärzteblatt. 2021, 103, 2710–2713. [Google Scholar]
- American Medical Association. Coverage of and Payment for Telemedicine (Reference Committee A). Report 7 of the Council on Medical Service (A-14). Available online: https://www.jonesday.com/files/upload/AMA%20Policy%20on%20Telehealth%20%28June%202014%29.PDF (accessed on 28 September 2021).
- WHO Telemedicine. Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth 2009; World Health Organisation: Geneva, Switzerland, 2010; p. 96. [Google Scholar]
- ONC. What is Telehealth? How is Telehealth Different from Telemedicine? Available online: https://www.healthit.gov/faq/what-telehealth-how-telehealth-different-telemedicine (accessed on 28 September 2021).
- Centers for Medicare and Medicaid Services. Telemedicine. Available online: https://www.medicaid.gov/medicaid/benefits/telemedicine/index.html (accessed on 28 September 2021).
- Centers for Medicare and Medicaid Services. Medicare Telemedicine Health Care Provider Fact Sheet. Available online: https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet (accessed on 28 September 2021).
- American Telemedicine Association Telehealth: Defining 21st Century Care. Available online: https://marketing.americantelemed.org/hubfs/Files/Resources/ATA_Telehealth_Taxonomy_9-11-20.pdf (accessed on 28 September 2021).
- Bundesaerztekammer. Telemedizin. Available online: https://www.bundesaerztekammer.de/aerzte/telematiktelemedizin/telemedizin/ (accessed on 4 October 2021).
- VFR Verlag für Rechtsjournalismus GmbH Telemedizin: Besondere Herausforderung für den Datenschutz. Available online: https://www.datenschutz.org/telemedizin/ (accessed on 4 October 2021).
- Batsis, J.A.; DiMilia, P.R.; Bs, L.M.S.; Fortuna, K.L.; Kennedy, M.A.; Blunt, H.; Bagley, P.; Brooks, J.; Brooks, E.; Kim, S.Y.; et al. Effectiveness of Ambulatory Telemedicine Care in Older Adults: A Systematic Review. J. Am. Geriatr. Soc. 2019, 67, 1737–1749. [Google Scholar] [CrossRef]
- Edirippulige, S.; Martin-Khan, M.; Beattie, E.; Smith, A.C.; Gray, L.C. A Systematic Review of Telemedicine Services for Residents in Long Term Care Facilities. J. Telemed. Telecare 2013, 19, 127–132. [Google Scholar] [CrossRef]
- Friedman, D.M.; Goldberg, J.M.; Molinsky, R.L.; Hanson, M.A.; Castaño, A.; Raza, S.-S.; Janas, N.; Celano, P.; Kapoor, K.; Telaraja, J.; et al. A Virtual Cardiovascular Care Program for Prevention of Heart Failure Readmissions in a Skilled Nursing Facility Population: Retrospective Analysis. JMIR Cardio 2021, 5, e29101. [Google Scholar] [CrossRef]
- Markus, H.S.; Martins, S. COVID-19 and stroke—Understanding the relationship and adapting services. A global World Stroke Organisation perspective. Int. J. Stroke 2021, 16, 241–247. [Google Scholar] [CrossRef]
- Demaerschalk, B.M.; Raman, R.; Ernstrom, K.; Meyer, B.C. Efficacy of Telemedicine for Stroke: Pooled Analysis of the Stroke Team Remote Evaluation Using a Digital Observation Camera (STRokE DOC) and STRokE DOC Arizona Telestroke Trials. Telemed. J. E Health 2012, 18, 230–237. [Google Scholar] [CrossRef]
- Bashshur, R.L.; Shannon, G.W.; Smith, B.R.; Alverson, D.C.; Antoniotti, N.; Barsan, W.G.; Bashshur, N.; Brown, E.M.; Coye, M.J.; Doarn, C.; et al. The Empirical Foundations of Telemedicine Interventions for Chronic Disease Management. Telemed. J. E Health 2014, 20, 769–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hailey, D.; Roine, R.; Ohinmaa, A.; Dennett, L. The status of telerehabilitation in neurological applications. J. Telemed. Telecare 2013, 19, 307–310. [Google Scholar] [CrossRef]
- Brignell, M.; Wootton, R.; Gray, L. The application of telemedicine to geriatric medicine. Age Ageing 2007, 36, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgoshaei, B.; Mobinizadeh, M.; Mojdekar, R.; Afzal, E.; Arabloo, J.; Mohamadi, E. Telemedicine: A systematic review of economic evaluations. Med. J. Islam. Repub. Iran 2017, 31, 113. [Google Scholar] [CrossRef]
- Groom, L.L.; McCarthy, M.M.; Stimpfel, A.W.; Brody, A.A. Telemedicine and Telehealth in Nursing Homes: An Integrative Review. J. Am. Med. Dir. Assoc. 2021, 22, 1784–1801.e7. [Google Scholar] [CrossRef]
- Arendts, G.; Quine, S.; Howard, K. Decision to transfer to an emergency department from residential aged care: A systematic review of qualitative research. Geriatr. Gerontol. Int. 2013, 13, 825–833. [Google Scholar] [CrossRef]
- Bandurchin, A.; McNally, M.J.; Ferguson-Paré, M. Bringing back the house call: How an emergency mobile nursing service is reducing avoidable emergency department visits for residents in long-term care homes. Nurs. Leadersh. (Tor. Ont.) 2011, 24, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Debatin, J. Pusht Die Corona-Krise Die Telemedizin? Und Was Bleibt Davon Langfristig Erhalten? Podcast. Available online: https://www.aerztezeitung.de/Podcasts/Pusht-die-Corona-Krise-die-Telemedizin-409613.html (accessed on 18 September 2022).
- National Policy Telehealth Resource Center COVID-19: Service Expansion. Available online: https://www.cchpca.org/topic/service-expansion/ (accessed on 28 September 2021).
- Daras, L.C.; Wang, J.M.; Ingber, M.J.; Ormond, C.; Breg, N.W.; Khatutsky, G.; Feng, Z. What Are Nursing Facilities Doing to Reduce Potentially Avoidable Hospitalizations? J. Am. Med. Dir. Assoc. 2017, 18, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Seifert, A.; Batsis, J.A.; Smith, A.C. Telemedicine in Long-Term Care Facilities During and Beyond COVID-19: Challenges Caused by the Digital Divide. Front. Public Health 2020, 8, 601595. [Google Scholar] [CrossRef]
- Guilfoyle, C.; Wootton, R.; Hassall, S.; Offer, J.; Warren, M.; Smith, D.; Eddie, M. Videoconferencing in facilities providing care for elderly people. J. Telemed. Telecare 2002, 8, 22–24. [Google Scholar] [CrossRef]
- Gagnon, M.-P.; Desmartis, M.; Labrecque, M.; Car, J.; Pagliari, C.; Pluye, P.; Frémont, P.; Gagnon, J.; Tremblay, N.; Légaré, F. Systematic Review of Factors Influencing the Adoption of Information and Communication Technologies by Healthcare Professionals. J. Med. Syst. 2012, 36, 241–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeRouge, C.; Garfield, M.J.; Collins, R.W. Telemedicine: Technology mediated service relationship, encounter, or something else? Int. J. Med. Inform. 2012, 81, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Chang, S. Scoping Reviews and Systematic Reviews: Is It an Either/Or Question? Ann. Intern. Med. 2018, 169, 502–503. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Zarin, W.; Ghassemi, M.; Nincic, V.; Lillie, E.; Page, M.J.; Shamseer, L.; Antony, J.; Rios, P.; Hwee, J.; et al. Same family, different species: Methodological conduct and quality varies according to purpose for five types of knowledge synthesis. J. Clin. Epidemiol. 2018, 96, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Soobiah, C.; Antony, J.; Cogo, E.; MacDonald, H.; Lillie, E.; Tran, J.; D’Souza, J.; Hui, W.; Perrier, L.; et al. A scoping review identifies multiple emerging knowledge synthesis methods, but few studies operationalize the method. J. Clin. Epidemiol. 2016, 73, 19–28. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.; Khalil, H. Chapter 11 on Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 9 July 2021). [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- PRISMA Checklist PRISMA Extension for Scoping Reviews (PRISMA-ScR). Available online: https://www.equator-network.org/reporting-guidelines/prisma-scr/ (accessed on 9 July 2021).
- Archbald-Pannone, L.; Harris, D.; Steele, R.; Kaur, J.; Albero, K.; Mutter, J.; Cattell-Gordon, D.; Rheuban, K. Virtual Daily Rounding for COVID-19 Facility Outbreaks: A Standardized Telehealth-Centered Approach May Reduce Hospital Transfers and Mortality. Telemed J. E Health 2021, 27, 915–918. [Google Scholar] [CrossRef]
- Chen, Y.H.; Ho, Y.L.; Huang, H.C.; Wu, H.W.; Lee, C.Y.; Hsu, T.P.; Cheng, C.L.; Chen, M.F. Assessment of the clinical outcomes and cost-effectiveness of the management of systolic heart failure in Chinese patients using a home-based intervention. J. Int. Med. Res. 2010, 38, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.; Bratan, T.; Kulkarni, S.; Jones, R. The impact of remote patient monitoring in managing silent myocardial infarction in a residential home setting. Anadolu Kardiyol Derg 2007, 7 (Suppl. 1), 186–188. [Google Scholar] [CrossRef] [PubMed]
- Crotty, M.; Killington, M.; van den Berg, M.; Morris, C.; Taylor, A.; Carati, C. Telerehabilitation for older people using off-the-shelf applications: Acceptability and feasibility. J. Telemed Telecare 2014, 20, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Bender, M.; Smith, T.; Broad, J. Feasibility and Acute Care Utilization Outcomes of a Post-Acute Transitional Telemonitoring Program for Underserved Chronic Disease Patients. Telemed. J. E-Health Off. J. Am. Telemed. Assoc. 2015, 21, 705–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBlois, D.; Millefoglie, M. Telehealth: Enhancing collaboration, improving care coordination. Nurs. Manag. 2015, 46, 10–12. [Google Scholar] [CrossRef]
- Dy, P.; Morin, P.C.; Weinstock, R.S. Use of telemedicine to improve glycemic management in a skilled nursing facility: A pilot study. Telemed J. E Health 2013, 19, 643–645. [Google Scholar] [CrossRef]
- Eckardt, P.; Guran, R.; Hennemyre, J.; Arikupurathu, R.; Poveda, J.; Miller, N.; Katz, R.; Frum, J. Hospital affiliated long term care facility COVID-19 containment strategy by using prevalence testing and infection control best practices. Am. J. Infect. Control 2020, 48, 1552–1555. [Google Scholar] [CrossRef]
- Errasti, U.; Pérez-Fernández, N.; Elola, M.; Fuertes, A.; Vaquero, M.; Berroeta, A.; Alberdi, A.; Zubeltzu, B.; Mitxelena, A.; Zubeldia, J.J.; et al. Evolution of a multipronged and multi-intevention strategy for patients with high comorbidity. Int. J. Integr. Care (IJIC) 2019, 19, 43. [Google Scholar] [CrossRef]
- Fong, R.; Tsai, K.C.F.; Tong, M.C.F.; Lee, K.Y.S. Management of Dysphagia in Nursing Homes During the COVID-19 Pandemic: Strategies and Experiences. SN Compr. Clin. Med. 2020, 2, 1361–1365. [Google Scholar] [CrossRef]
- Freedman, M.; Binns, M.A.; Serediuk, F.; Wolf, M.U.; Danieli, E.; Pugh, B.; Gale, D.; Abdellah, E.; Teleg, E.; Halper, M.; et al. Virtual Behavioural Medicine Program: A Novel Model of Care for Neuropsychiatric Symptoms in Dementia. J. Alzheimer‘S Dis 2022, 86, 1169–1184. [Google Scholar] [CrossRef] [PubMed]
- Gomes, V.M.G.; Butzke, B.; Kubitschek, M. Developing an innovative, integrated care pathway for PMV patients. Int. J. Integr. Care (IJIC) 2016, 16, A177. [Google Scholar] [CrossRef] [Green Version]
- Gray, L.C.; Edirippulige, S.; Smith, A.C.; Beattie, E.; Theodoros, D.; Russell, T.; Martin-Khan, M. Telehealth for nursing homes: The utilization of specialist services for residential care. J. Telemed. Telecare 2012, 18, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Guilfoyle, C.; Wootton, R.; Hassall, S.; Offer, J.; Waaren, M.; Smith, D. Preliminary experience of allied health assessments delivered face to face and by videoconference to a residential facility for elderly people. J. Telemed. Telecare 2003, 9, 230–233. [Google Scholar] [CrossRef]
- Guilfoyle, C.; Wootton, R.; Hassall, S.; Offer, J.; Warren, M.; Smith, D.; Eddie, M. User satisfaction with allied health services delivered to residential facilities via videoconferencing. J. Telemed. Telecare 2003, 9 (Suppl. 1), 52–54. [Google Scholar] [CrossRef]
- Harris, D.A.; Archbald-Pannone, L.; Kaur, J.; Cattell-Gordon, D.; Rheuban, K.S.; Ombres, R.L.; Albero, K.; Steele, R.; Bell, T.D.; Mutter, J.B. Rapid Telehealth-Centered Response to COVID-19 Outbreaks in Postacute and Long-Term Care Facilities. Telemed J. E Health 2021, 27, 102–106. [Google Scholar] [CrossRef]
- Harry, M.; Woehrle, T.; Renier, C.; Furcht, M.; Enockson, M. Predictive utility of the Activity Measure for Post-Acute Care ‘6-Clicks’ short forms on discharge disposition and effect on readmissions: A retrospective observational cohort study. BMJ Open 2021, 11, e044278. [Google Scholar] [CrossRef]
- Hassall, S.; Wootton, R.; Guilfoyle, C. The cost of allied health assessments delivered by videoconference to a residential facility for elderly people. J. Telemed. Telecare 2003, 9, 234–237. [Google Scholar] [CrossRef]
- Hernández, C.; Alonso, A.; Garcia-Aymerich, J.; Grimsmo, A.; Vontetsianos, T.; García Cuyàs, F.; Altes, A.G.; Vogiatzis, I.; Garåsen, H.; Pellise, L.; et al. Integrated care services: Lessons learned from the deployment of the NEXES project. Int. J. Integr. Care 2015, 15, e006. [Google Scholar] [CrossRef] [Green Version]
- Hicks, S.A.; Cimarolli, V.R. The effects of telehealth use for post-acute rehabilitation patient outcomes. J. Telemed. Telecare 2018, 24, 179–184. [Google Scholar] [CrossRef]
- Hullick, C.; Conway, J.; Hall, A.; Murdoch, W.; Cole, J.; Hewitt, J.; Oldmeadow, C.; Attia, J. Video-telehealth to support clinical assessment and management of acutely unwell older people in Residential Aged Care: A pre-post intervention study. BMC Geriatr. 2022, 22, 40. [Google Scholar] [CrossRef] [PubMed]
- Kaldy, J. Telehealth enables senior care pharmacists to reach beyond facility walls. Consult. Pharm. 2005, 20, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Lapane, K.L.; Hughes, C.M.; Daiello, L.A.; Cameron, K.A.; Feinberg, J. Effect of a pharmacist-led multicomponent intervention focusing on the medication monitoring phase to prevent potential adverse drug events in nursing homes. J. Am. Geriatr. Soc. 2011, 59, 1238–1245. [Google Scholar] [CrossRef]
- Lewis, G. Career development. Virtual wards: Real nursing. Prim. Health Care 2007, 17, 47. [Google Scholar] [CrossRef]
- Mahlknecht, A.; Krisch, L.; Nestler, N.; Bauer, U.; Letz, N.; Zenz, D.; Schuler, J.; Fährmann, L.; Hempel, G.; Flamm, M.; et al. Impact of training and structured medication review on medication appropriateness and patient-related outcomes in nursing homes: Results from the interventional study InTherAKT. BMC Geriatr. 2019, 19, 257. [Google Scholar] [CrossRef] [Green Version]
- Martin-Khan, M.G.; Edwards, H.; Wootton, R.; Counsell, S.R.; Varghese, P.; Lim, W.K.; Darzins, P.; Dakin, L.; Klein, K.; Gray, L.C. Reliability of an Online Geriatric Assessment Procedure Using the interRAI Acute Care Assessment System. J. Am. Geriatr. Soc. 2017, 65, 2029–2036. [Google Scholar] [CrossRef] [PubMed]
- Mateos-Nozal, J.; Pérez-Panizo, N.; Zárate-Sáez, C.M.; Vaquero-Pinto, M.N.; Roldán-Plaza, C.; Mejía Ramírez-Arellano, M.V.; Sánchez García, E.; Garza-Martínez, A.J.; Cruz-Jentoft, A.J. Proactive Geriatric Comanagement of Nursing Home Patients by a New Hospital-Based Liaison Geriatric Unit: A New Model for the Future. J. Am. Med. Dir. Assoc. 2022, 23, 308–310. [Google Scholar] [CrossRef]
- Mullen-Fortino, M.; Sites, F.D.; Soisson, M.; Galen, J. Innovative use of tele-ICU in long-term acute care hospitals. AACN Adv. Crit. Care 2012, 23, 330–336. [Google Scholar] [CrossRef]
- Nishita, C.M.; Johnson, J.; Silverman, M.; Ozaki, R.; Koller, L. Hawai’i’s “Going Home Plus” project: A new option to support community living. Hawaii Med. J. 2009, 68, 166–168. [Google Scholar]
- Ohligs, M.; Stocklassa, S.; Rossaint, R.; Czaplik, M.; Follmann, A. Employment of Telemedicine in Nursing Homes: Clinical Requirement Analysis, System Development and First Test Results. Clin. Interv. Aging 2020, 15, 1427–1437. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y. Improvement in palliative care quality in rural nursing homes through information and communication technology-driven interprofessional collaboration. Rural Remote Health 2021, 21, 6450. [Google Scholar] [CrossRef] [PubMed]
- Ošmera, O.; Bulava, A. The benefits of remote monitoring in long-term care for patients with implantable cardioverter-defibrillators. Neuro Endocrinol. Lett. 2014, 35 (Suppl. 1), 40–48. [Google Scholar] [PubMed]
- Pallawala, P.M.; Lun, K.C. EMR-based TeleGeriatric system. Stud. Health Technol Inform. 2001, 84 Pt 1, 849–853. [Google Scholar] [CrossRef]
- Peterson-Sgro, K. Reducing acute care hospitalization and emergent care use through home health disease management: One agency’s success story. Home Healthc. Nurse 2007, 25, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Rantz, M.; Lane, K.; Phillips, L.J.; Despins, L.A.; Galambos, C.; Alexander, G.L.; Koopman, R.J.; Hicks, L.; Skubic, M.; Miller, S.J. Enhanced registered nurse care coordination with sensor technology: Impact on length of stay and cost in aging in place housing. Nurs. Outlook 2015, 63, 650–655. [Google Scholar] [CrossRef]
- Rantz, M.J.; Skubic, M.; Alexander, G.; Aud, M.A.; Wakefield, B.J.; Galambos, C.; Koopman, R.J.; Miller, S.J. Improving nurse care coordination with technology. CIN Comput. Inform. Nurs. 2010, 28, 325–332. [Google Scholar] [CrossRef]
- Roques, C.; Hovanec, L. Tele-medicine and the reduction of psychiatric admissions for dementia patients—Social work as the core discipline. J. Soc. Work Long-Term Care 2002, 1, 35–41. [Google Scholar] [CrossRef]
- Sabesan, S.; Larkins, S.; Evans, R.; Varma, S.; Andrews, A.; Beuttner, P.; Brennan, S.; Young, M. Telemedicine for rural cancer care in North Queensland: Bringing cancer care home. Aust J. Rural Health 2012, 20, 259–264. [Google Scholar] [CrossRef]
- Sävenstedt, S.; Bucht, G.; Norberg, L.; Sandman, P.O. Nurse-doctor interaction in teleconsultations between a hospital and a geriatric nursing home. J. Telemed. Telecare 2002, 8, 11–18. [Google Scholar] [CrossRef]
- Specht, J.K.; Wakefield, B.; Flanagan, J. Evaluating the cost of one telehealth application connecting an acute and long-term care setting. J. Gerontol Nurs. 2001, 27, 34–39. [Google Scholar] [CrossRef]
- Tappen, R.M.; Newman, D.; Huckfeldt, P.; Yang, Z.; Engstrom, G.; Wolf, D.G.; Shutes, J.; Rojido, C.; Ouslander, J.G. Evaluation of Nursing Facility Resident Safety During Implementation of the INTERACT Quality Improvement Program. J. Am. Med. Dir. Assoc. 2018, 19, 907. [Google Scholar] [CrossRef] [PubMed]
- Vitacca, M.; Paneroni, M.; Grossetti, F.; Ambrosino, N. Is There Any Additional Effect of Tele-Assistance on Long-Term Care Programmes in Hypercapnic COPD Patients? A Retrospective Study. COPD 2016, 13, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Wade, V.; Whittaker, F.; Hamlyn, J. An evaluation of the benefits and challenges of video consulting between general practitioners and residential aged care facilities. J. Telemed. Telecare 2015, 21, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.K.; Esquenazi, A.; Flanagan, S. The Transformation of the Rehabilitation Paradigm Across the Continuum of Care. Pm R 2018, 10 (9 Suppl 2), S264–S271. [Google Scholar] [CrossRef] [Green Version]
- Whitson, H.E.; Hastings, S.N.; Lekan, D.A.; Sloane, R.; White, H.K.; McConnell, E.S. A quality improvement program to enhance after-hours telephone communication between nurses and physicians in a long-term care facility. J. Am. Geriatr. Soc. 2008, 56, 1080–1086. [Google Scholar] [CrossRef]
- Wilmink, G.; Dupey, K.; Alkire, S.; Grote, J.; Zobel, G.; Fillit, H.M.; Movva, S. Artificial Intelligence-Powered Digital Health Platform and Wearable Devices Improve Outcomes for Older Adults in Assisted Living Communities: Pilot Intervention Study. JMIR Aging 2020, 3, e19554. [Google Scholar] [CrossRef]
- Yoon, J.; Chang, E.; Rubenstein, L.V.; Park, A.; Zulman, D.M.; Stockdale, S.; Ong, M.K.; Atkins, D.; Schectman, G.; Asch, S.M. Impact of Primary Care Intensive Management on High-Risk Veterans’ Costs and Utilization A Randomized Quality Improvement Trial. Ann. Intern. Med. 2018, 168, 846–854. [Google Scholar] [CrossRef]
- Zubeltzu, B.; Mitxelena, A.; Alberdi, A.; Elola, M.; Errasti, U.; Berroeta, A.; Vaquero, M.; Fuertes, A.; Perez, N.; Echegaray, M.; et al. Multipronged management strategy for patients with complex needs using an integrated organizational model. Int. J. Integr. Care (IJIC) 2018, 18, 14. [Google Scholar] [CrossRef]
- Du Prel, J.-B.; Röhrig, B.; Blettner, M. Critical Appraisal of Scientific Articles. Dtsch. Arztebl. Int. 2009, 106, 100–105. [Google Scholar] [CrossRef]
- Newbould, L.; Mountain, G.; Hawley, M.S.; Ariss, S. Videoconferencing for Health Care Provision for Older Adults in Care Homes: A Review of the Research Evidence. Int. J. Telemed. Appl. 2017, 2017, 5785613. [Google Scholar] [CrossRef]
- Chess, D.; Whitman, J.J.; Croll, D.; Stefanacci, R. Impact of after-hours telemedicine on hospitalizations in a skilled nursing facility. Am. J. Manag. Care 2018, 24, 385–388. [Google Scholar] [PubMed]
- Dadosky, A.; Overbeck, H.; Barbetta, L.; Bertke, K.; Corl, M.; Daly, K.; Hiles, N.; Rector, N.; Chung, E.; Menon, S. Telemanagement of Heart Failure Patients Across the Post-Acute Care Continuum. Telemed. J. E Health 2018, 24, 360–366. [Google Scholar] [CrossRef] [PubMed]
- De Luca, R.; Bramanti, A.; De Cola, M.C.; Trifiletti, A.; Tomasello, P.; Torrisi, M.; Reitano, S.; Leo, A.; Bramanti, P.; Calabrò, R.S. Tele-health-care in the elderly living in nursing home: The first Sicilian multimodal approach. Aging Clin. Exp. Res. 2016, 28, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyer, J.; Leider, J.P.; Satorius, J.; Tanenbaum, E.; Basel, D.; Knudson, A. Implementation of Telemedicine Consultation to Assess Unplanned Transfers in Rural Long-Term Care Facilities, 2012–2015: A Pilot Study. J. Am. Med. Dir. Assoc. 2016, 17, 1006–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, J.W.; Kennedy, M.; Nathanson, L.A.; Wardlow, L.; Crowley, C.; Stuck, A. Reducing Emergency Department Transfers from Skilled Nursing Facilities Through an Emergency Physician Telemedicine Service. West. J. Emerg. Med. 2020, 21, 205–209. [Google Scholar] [CrossRef]
- Kane-Gill, S.L.; Wong, A.; Culley, C.M.; Perera, S.; Reynolds, M.D.; Handler, S.M.; Kellum, J.A.; Aspinall, M.B.; Pellett, M.E.; Long, K.E.; et al. Transforming the Medication Regimen Review Process Using Telemedicine to Prevent Adverse Events. J. Am. Geriatr. Soc. 2021, 69, 530–538. [Google Scholar] [CrossRef]
- Li, S.E.; Hossain, M.; Gilman, B.; Forrow, L.V.; Lee, K.M.; Brown, R. Effects of a Nursing Home Telehealth Program on Spending and Utilization for Medicare Residents. Health Serv. Res. 2022, 57, 1191–1200. [Google Scholar] [CrossRef]
- Low, J.A.; Jin, T.H.; Chin, L.T.L.; Agarwal, N.; Huat, G.K.; Yeow, A.; Soh, C. Cost analysis of implementing a telegeriatrics ecosystem with nursing homes: Panel data analysis. Health Syst. 2019, 9, 285–292. [Google Scholar] [CrossRef]
- Tynan, A.; Deeth, L.; McKenzie, D.; Bourke, C.; Stenhouse, S.; Pitt, J.; Linneman, H. Integrated approach to oral health in aged care facilities using oral health practitioners and teledentistry in rural Queensland. Aust. J. Rural Health 2018, 26, 290–294. [Google Scholar] [CrossRef]
- Baxter, K.E.; Kochar, S.; Williams, C.; Blackman, C.; Himmelvo, J. Development of a Palliative Telehealth Pilot to Meet the Needs of the Nursing Home Population. J. Hosp. Palliat. Nurs. 2021, 23, 478–483. [Google Scholar] [CrossRef]
- Stern, A.; Mitsakakis, N.; Paulden, M.; Alibhai, S.; Wong, J.; Tomlinson, G.; Brooker, A.-S.; Krahn, M.; Zwarenstein, M. Pressure ulcer multidisciplinary teams via telemedicine: A pragmatic cluster randomized stepped wedge trial in long term care. BMC Health Serv. Res. 2014, 14, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catic, A.G.; Mattison, M.L.; Bakaev, I.; Morgan, M.; Monti, S.M.; Lipsitz, L. ECHO-AGE: An Innovative Model of Geriatric Care for Long-Term Care Residents with Dementia and Behavioral Issues. J. Am. Med. Dir. Assoc. 2014, 15, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, D.C.; O’Malley, A.J. Use of Telemedicine Can Reduce Hospitalizations of Nursing Home Residents and Generate Savings for Medicare. Health Aff. 2014, 33, 244–250. [Google Scholar] [CrossRef] [Green Version]
- Hui, E.; Woo, J.; Hjelm, M.; Zhang, Y.; Tsui, H. Telemedicine: A Pilot Study in Nursing Home Residents. Gerontology 2001, 47, 82–87. [Google Scholar] [CrossRef]
- Lyketsos, C.G.; Roques, C.; Hovanec, L.; Jones, B.N. 3rd Telemedicine use and the reduction of psychiatric admissions from a long-term care facility. J. Geriatr. Psychiatry Neurol. 2001, 14, 76–79. [Google Scholar] [CrossRef]
- Yeow, A.; Goh, K.H. Work Harder or Work Smarter? Information Technology and Resource Allocation in Healthcare Pro-cesses. MIS Q. 2015, 39, 763–786. [Google Scholar] [CrossRef]
- Gillespie, S.M.; Wasserman, E.B.; Wood, N.E.; Wang, H.; Dozier, A.; Nelson, D.; McConnochie, K.M.; Shah, M.N. High-Intensity Telemedicine Reduces Emergency Department Use by Older Adults with Dementia in Senior Living Communities. J. Am. Med. Dir. Assoc. 2019, 20, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.; Garnvwa, H.; Oppong, R. Critical Appraisal of Published Systematic Reviews Assessing the Cost-Effectiveness of Telemedicine Studies. Telemed. J. E-Health 2014, 20, 609–618. [Google Scholar] [CrossRef]
- Alexander, G.L.; Powell, K.R.; Deroche, C.B. An evaluation of telehealth expansion in U.S. nursing homes. J. Am. Med. Inform. Assoc. 2021, 28, 342–348. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services. Skilled Nursing Facility 30-Day All-Cause Readmission Measure (SNFRM) NQF #2510: All-Cause Risk-Standardized Readmission Measure. Technical Report Supplement—2019 Update. Available online: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/SNF-VBP/Downloads/SNFRM-TechReportSupp-2019-.pdf (accessed on 22 March 2022).
- Centers for Medicare and Medicaid Services. Hospital Readmissions Reduction Program (HRRP). Available online: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/HRRP/Hospital-Readmission-Reduction-Program (accessed on 22 March 2022).
- Rezvan, A. Telephone Communication with the Primary Physician by Staff of a Long-Term Care Facility. J. Am. Geriatr. Soc. 1989, 37, 289–290. [Google Scholar] [CrossRef]
- Kümpel, C.; Schneider, U. Additional reimbursement for outpatient physicians treating nursing home residents reduces avoidable hospital admissions: Results of a reimbursement change in Germany. Health Policy 2020, 124, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Stephens, C.E.; Halifax, E.; David, D.; Bui, N.; Lee, S.J.; Shim, J.; Ritchie, C.S. “They Don’t Trust Us”: The Influence of Perceptions of Inadequate Nursing Home Care on Emergency Department Transfers and the Potential Role for Telehealth. Clin. Nurs. Res. 2020, 29, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Georgeton, E.; Aubert, L.; Pierrard, N.; Gaborieau, G.; Berrut, G.; de Decker, L. General practitioners adherence to recommendations from geriatric assessments made during teleconsultations for the elderly living in nursing homes. Maturitas 2015, 82, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Cryer, L.; Shannon, S.B.; Van Amsterdam, M.; Leff, B. Costs for ‘Hospital at Home’ Patients Were 19 Percent Lower, with Equal or Better Outcomes Compared to Similar Inpatients. Health Aff. 2012, 31, 1237–1243. [Google Scholar] [CrossRef]
- Leff, B.; Montalto, M. Home hospital—Toward a tighter definition. J. Am. Geriatr. Soc. 2004, 52, 2141. [Google Scholar] [CrossRef]
- Levine, D.M.; Ouchi, K.; Blanchfield, B.; Diamond, K.; Licurse, A.; Pu, C.T.; Schnipper, J.L. Hospital-Level Care at Home for Acutely Ill Adults: A Pilot Randomized Controlled Trial. J. Gen. Intern. Med. 2018, 33, 729–736. [Google Scholar] [CrossRef] [Green Version]
- Levine, D.M.; Pian, J.; Mahendrakumar, K.; Patel, A.; Saenz, A.; Schnipper, J.L. Hospital-Level Care at Home for Acutely Ill Adults: A Qualitative Evaluation of a Randomized Controlled Trial. J. Gen. Intern. Med. 2021, 36, 1965–1973. [Google Scholar] [CrossRef]
- Federman, A.D.; Soones, T.; DeCherrie, L.V.; Leff, B.; Siu, A.L. Association of a Bundled Hospital-at-Home and 30-Day Postacute Transitional Care Program with Clinical Outcomes and Patient Experiences. JAMA Intern. Med. 2018, 178, 1033–1040. [Google Scholar] [CrossRef]
- Güler, N.F.; Übeyli, E.D. Theory and Applications of Telemedicine. J. Med. Syst. 2004, 26, 199–220. [Google Scholar] [CrossRef]
- Esterle, L.; Mathieu-Fritz, A. Teleconsultation in geriatrics: Impact on professional practice. Int. J. Med. Inform. 2013, 82, 684–695. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, 834–840. [Google Scholar] [CrossRef] [PubMed]
- The CONSORT Group. Consolidated Standards of Reporting Trials. Available online: http://www.consort-statement.org/ (accessed on 8 October 2022).



{kind=link}
{kind=link}
| Database | PubMed: 4 Search Strings Combined with Boolean Operator |
|---|---|
| For nursing home | (((((nursing home[MeSH Terms] OR “nursing home”[Title/Abstract] OR “nursing homes”[Title/Abstract] OR “nursing facility”[Title/Abstract] OR “nursing facilities”[Title/Abstract] OR “long-term care”[Title/Abstract] OR “long-term care facility”[Title/Abstract] OR “long-term care facilities”[Title/Abstract] OR “aged care”[Title/Abstract] OR “care home”[Title/Abstract] OR “care homes”[Title/Abstract] OR “home for the aged”[Title/Abstract] OR “homes for the aged”[Title/Abstract] OR “institutional care”[Title/Abstract] OR “residential care”[Title/Abstract]))) AND |
| For telemedicine | (((((((((((((((((((telemedicine[MeSH Terms]) OR (telemedicine[Title/Abstract])) OR (telehealth[Title/Abstract])) OR (Telemedicine[Title/Abstract])) OR (distance based treatment[Title/Abstract])) OR (teleconsultation[Title/Abstract])) OR (information communication technology[Title/Abstract])) OR (ICT[Title/Abstract])) OR (health information technology[Title/Abstract])) OR (external clinical support[Title/Abstract])) OR (ICT-based intervention[Title/Abstract]))) OR (mobile health[Title/Abstract])) OR (mHealth[Title/Abstract])) OR (digital health[Title/Abstract])) OR (virtual care[Title/Abstract])) OR (telemonitor*[Title/Abstract])) OR (telerehabilitation[Title/Abstract]))))) AND |
| For hospitalization | ((((hospitalization[MeSH Terms]) OR (hospitaliz*[Title/Abstract] OR hospitalis*[Title/Abstract])) OR (((hospital[Title/Abstract] OR hospitals[Title/Abstract])) AND (admit*[Title/Abstract] OR admis*[Title/Abstract] OR transfer*[Title/Abstract] OR refer*[Title/Abstract] OR transition[Title/Abstract])) OR ((“acute care”[Title/Abstract]) AND (admit*[Title/Abstract] OR admis*[Title/Abstract] OR transfer*[Title/Abstract] OR refer*[Title/Abstract] OR transition[Title/Abstract])) OR ((emergency[Title/Abstract]) AND (admit*[Title/Abstract] OR admis*[Title/Abstract] OR transfer*[Title/Abstract] OR refer*[Title/Abstract] OR transition[Title/Abstract])))) |
| Source | Baxter et al. 2021 [128] | Catic et al. 2014 [130] | Chess et al. 2018 [119] | Dadosky et al. 2018 [120] | De Luca et al. 2016 [121] | Grabowski et al. 2014 [131] | Hofmeyer et al. 2016 [122] | Hui et al. 2001 [132] | Joseph et al. 2020 [123] | Kane-Gill et al. 2021 [124] | Li et al. 2022 [125] | Low et al. 2019 [126] | Lyketsos et al. 2001 [133] | Stern et al. 2014 [129] | Tynan et al. 2018 [127] | Yeow et al. 2015 [134] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Data Charting Results | |||||||||||||||||
| Evidence Level | |||||||||||||||||
| Higher | X | X | X | X | X | X | X | ||||||||||
| Lower | X | X | X | X | X | X | X | X | X | ||||||||
| Population Density | |||||||||||||||||
| High | X | X | X | X | X | X | X | X | X | X | X | X | |||||
| Low | X | X | X | X | |||||||||||||
| Telemedicine Intervention | |||||||||||||||||
| Specific Health Care Model | X | X | X | X | X | ||||||||||||
| Intermediate Telemedicine service | X | X | X | X | X | X | X | ||||||||||
| Direct Contact between Communicating Parties | X | X | X | X | X | X | X | X | X | ||||||||
| Audio | X | X | X | X | X | X | X | X | X ° | X | X | X | X | X | X | X | |
| Video | X | X | X | X | X | X | X | X | X ° | X | X | X | X | X | X | X | |
| Medical Diagnostic/ Monitoring Technology | X | X | X | X | X | X | X | X | X | X | |||||||
| (Electronic) Health Record on NHR | X | X | X | X | X | X | X | X | X | ||||||||
| Telemedicine Training/ Instruction of Caregivers | X | X | X | X | X | X | X | X | X | X | X | X | |||||
| Involved Health Professionals | |||||||||||||||||
| Specialist | X | X | X | X | X | X | X | X | X | ||||||||
| Physician | X | X | X | X | X | X | X | ||||||||||
| Specialized Nursing Staff at Consulted Health Care site | X | X | X | X | X | X | X | ||||||||||
| Specialized Nursing staff at the NH/SNF/LTC | X | X | X | X | X | X | |||||||||||
| Nursing Staff at the NH/SNF/LTC | X | X | X | X | X | X | X | X | X | X | X | ||||||
| Other | 1 | 1 | 1 | 1,2,3 | 4 | 3 | 1,2 | 1,4 | 4 | 4 | |||||||
| Intervention Properties | |||||||||||||||||
| Diagnostic | X | X | X | X | X | X | X | X | |||||||||
| Therapeutic | X | X | X | X | X | X | X | ||||||||||
| Monitoring | X | X | X | X | X | X | X | X | |||||||||
| Review Question 1 | |||||||||||||||||
| ED Visits | ↓* | ↓* | ↓ | ↓ | ↓ | ↓ | = | ↓ | ↓ | ||||||||
| Hospitalization Rate | ↓ | ↓ | ↓ | ↓ | ↓* | =/↓ | ↓* | ↓ | ↓ | = | =/↓ | ↓ | ↓ | = | ↓ | ||
| Mortality Rate | ↓ | ||||||||||||||||
| Review Question 2 | |||||||||||||||||
| Cost-Effectiveness | ↑ | ↑ | ↑ | ↑ | ↑ | =/↑ | ↑ | ↑ | ↑ | ↑? | ↑/↓ | ||||||
| Satisfaction/Well-Being of Health Care Professionals | ↑ | ↑ | ↑ | ↑ | ↑ | ↑ | |||||||||||
| Duty Hours in Telemedicine | |||||||||||||||||
| Weekdays | X | X | X | n. i. | X | X | X | ||||||||||
| After Hours/Weekends | X | X | n. i. | ||||||||||||||
| 24/7 | X | X | X | X | X | X | n. i. | X | |||||||||
| Regarding the 16 Included Studies [119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134]: | Number of Studies | References | |
|---|---|---|---|
| Study design | Higher evidence level ^ | 7 | [121,123,124,125,129,130,131] |
| Lower evidence level ° | 9 | [119,120,122,126,127,128,132,133,134] | |
| Facility | Nursing home (NH) | 7 | [121,126,127,128,131,132,134] |
| Long-term care facility (LTC) | 3 | [122,129,130] | |
| Skilled nursing facility (SNF) | 4 | [119,120,123,133] | |
| LTC and SNF | 2 | [124,125] | |
| Purpose of telemedicine | Diagnosis | 5 | [119,122,123,127,131] |
| Therapy | 2 | [128,130] | |
| Monitoring | 3 | [120,121,124] | |
| Combination of purposes | 6 | [125,126,129,132,133,134] | |
| Establishing contact between communicating parties via telemedicine | Directly by hospital or nursing home itself | 9 | [120,123,126,127,129,130,132,133,134] |
| By an intermediate service | 7 | [119,121,122,124,125,128,131] | |
| Consultation by | Specialist | 9 | [120,121,122,126,127,129,130,132,134] |
| Physician | 7 | [119,123,124,125,128,131,133] | |
| Nursing staff | Specialized nursing staff at telemedicine consultant site | 5 | [122,125,128,131,132] |
| Specialized nursing staff at NH | 4 | [119,120,123,126] | |
| No specialized nursing staff | 5 | [121,124,127,130,134] | |
| Specialized staff at both telemedicine consultant site as well as NH | 2 | [129,133] | |
| Consultation between | Specialist/physician and specialized NH nursing staff | 6 | [119,120,123,126,129,133] |
| Specialist/physician and NH nursing staff | 10 | [121,122,124,125,127,128,130,131,132,134] | |
| Telemedicine service offered on ^^ | Weekdays | 6 | [121,124,127,129,132,133] |
| Both weekdays and after hours | 7 | [120,122,123,125,128,130,134] | |
| After hours | 2 | [119,131] | |
| Use of medical/monitoring diagnostic technology | Yes | 10 | [119,120,121,122,123,125,127,129,132,133] |
| No | 6 | [124,126,128,130,131,134] | |
| Use of (electronic) health record | Yes | 9 | [119,120,121,123,124,125,129,130,133] |
| No | 7 | [122,126,127,128,131,132,134] | |
| Reduction in Emergency Department Visits, Hospitalization, and/or Mortality | Total Number of Studies | |||
|---|---|---|---|---|
| Yes | No | |||
| Level of evidence (credibility) according to study design | higher | 3 [121,123,130] | 4 * [124,125,129,131] | 7 |
| lower | 9 [119,120,122,126,127,128,132,133,134] | 0 | 9 | |
| Total number of studies | 12 | 4 * | 16 | |
| Cost Savings | Total Number of Studies | |||
|---|---|---|---|---|
| Yes | Inconclusive/No | |||
| Level of evidence (credibility) according to study design | higher | 3 [123,129,131] | 1 * [125] | 4 |
| lower | 5 [119,120,126,132,133] | 2 [127,134] | 7 | |
| Total number of studies | 8 | 3 | 11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valk-Draad, M.P.; Bohnet-Joschko, S. Nursing Home-Sensitive Hospitalizations and the Relevance of Telemedicine: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 12944. https://doi.org/10.3390/ijerph191912944
Valk-Draad MP, Bohnet-Joschko S. Nursing Home-Sensitive Hospitalizations and the Relevance of Telemedicine: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12944. https://doi.org/10.3390/ijerph191912944
Chicago/Turabian StyleValk-Draad, Maria Paula, and Sabine Bohnet-Joschko. 2022. "Nursing Home-Sensitive Hospitalizations and the Relevance of Telemedicine: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 19: 12944. https://doi.org/10.3390/ijerph191912944
APA StyleValk-Draad, M. P., & Bohnet-Joschko, S. (2022). Nursing Home-Sensitive Hospitalizations and the Relevance of Telemedicine: A Scoping Review. International Journal of Environmental Research and Public Health, 19(19), 12944. https://doi.org/10.3390/ijerph191912944