


The Impact of a Yoga-Based Mindfulness Intervention versus Psycho-Educational Session for Older Adults with Mild Cognitive Impairment: The Protocol of a Randomized Controlled Trial
 , ,
, ,
Abstract
1. Background
- (1)
- To compare the change in cognitive function scores between older adults with MCI receiving a YBM intervention versus those receiving a PES intervention.
- (2)
- To compare the change in physical function scores between older adults with MCI receiving a YBM intervention versus those receiving a PES intervention.
- (3)
- To compare the change in well-being scores between older adults with MCI receiving a YBM intervention versus those receiving a PES intervention.
- (4)
- To compare the change in anxiety and depression scores between older adults with MCI receiving a YBM intervention versus those receiving a PES intervention.
- (5)
- To assess the correlation between cognitive function and physical function in older adults with MCI, controlling for psychological variables (depression, anxiety, well-being), and group (YBM intervention or participating in PES)
2. Method
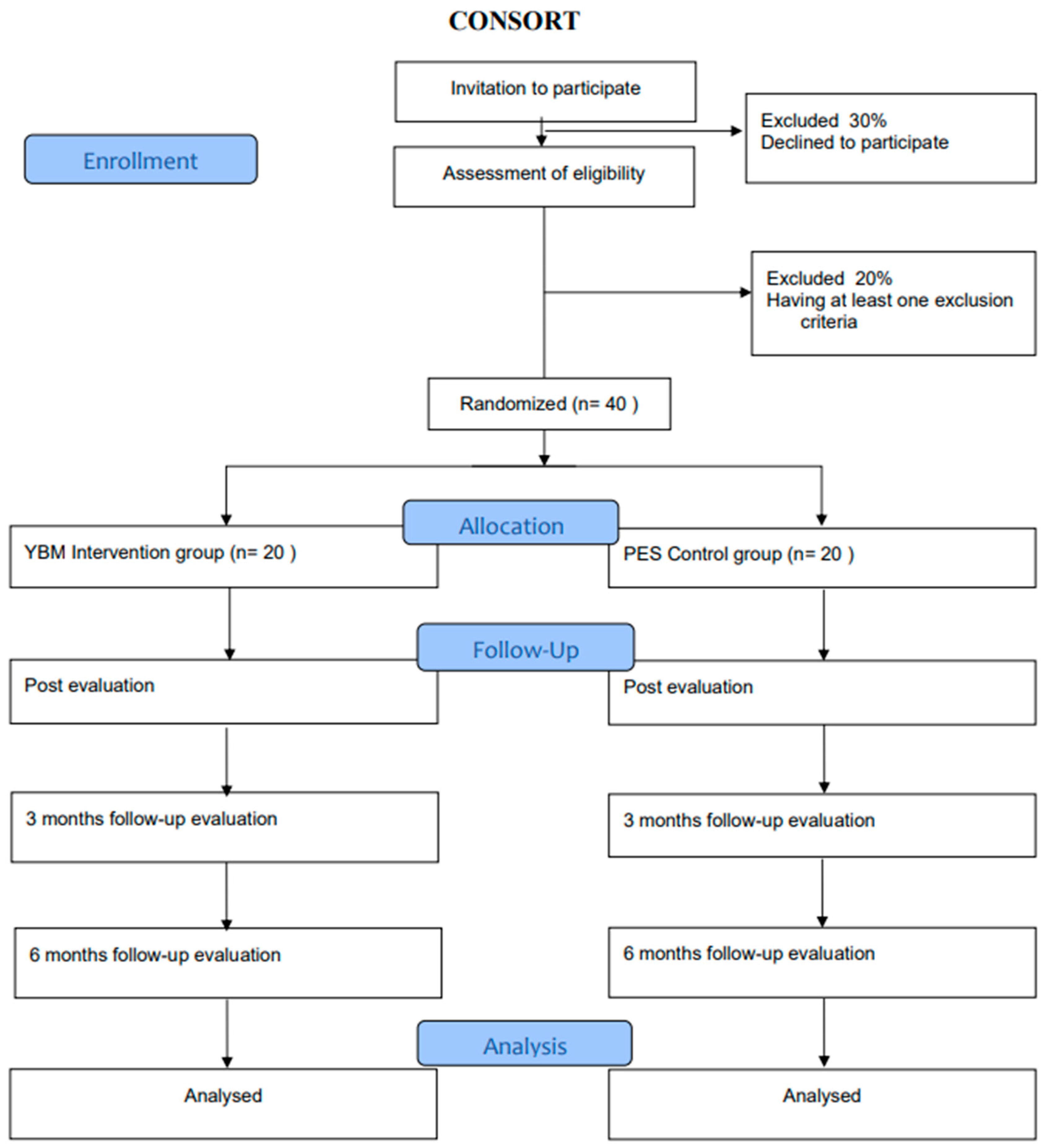
2.1. Trial Design
2.2. Study Setting
2.3. Participants
- Having 60 years and above,
- People who have MCI are diagnosed by three criteria:
- ➢
- by a neurologist and/or psychiatrist, and/or geriatrician, and/or neuropsychologist. through evaluation by saying that they had memory problems confirmed by an informant (in case they have a formal or informal caregiver or simply, their partner), (but without problems in their activities of daily living);
- ➢
- and with a score < 21 on the Montreal Cognitive Assessment (MoCA < 21).
- Without dementia, according to the criteria of the Clinical Dementia Rating Scale (CDR), a score of 0.05.
- People who performed yoga and/or mindfulness within the last 6 months
- The presence of a psychiatric clinical diagnosis; or neurological/cerebrovascular condition.
- Presence of a disabling physical illness or/and presence of a disability that limits and/or impede communication, such as major impairments in eyesight, and/ hearing or upper limb motor movements, and/or other health problem that would interfere with regular yoga and mindfulness practice.
2.4. Recruitment and Informed Consent Process
2.5. Randomization
2.6. Sample Size
3. Intervention Program
3.1. Procedures
3.2. Criteria for Stopping or Modifying Allocated Interventions
3.3. Plans to Improve Adherence to Intervention Protocols
3.4. Relevant Therapies and Interventions Allowedor Prohibited during the Trial
3.5. Participant Timeline
4. Outcomes
4.1. Primary Outcomes
4.2. Secondary Outcomes
5. Covariates
5.1. Strategies to Promote Participant Retention and Complete Follow-Up
5.2. Data Management and Confidentiality
6. Analysis
6.1. Plans to Give Access to the Full Protocol and Participant Level-Data
6.2. Patient and Public Involvement
6.3. Dissemination Plans
6.4. Composition of the Data Monitoring Committee, Its Role, and Reporting Structure
6.5. Adverse Event Reporting
6.6. Strategies for Communicating Important Protocol Amendments
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- United Nations Department of Economic and Social Affairs. World Population Prospects 2022: Summary of Results; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2022. [Google Scholar]
- Schmidt, I.; Wilson, M.; Nair, A.; Alam, M.; Carlson, A. Harnessing the Potential of Population Aging Insights and Opportunities for Development Finance. 2022. Available online: https://investinginpopulationaging.com/ (accessed on 20 August 2022).
- Ministerio de Planificacion. Encuesta de Caracterización Socioeconómica Nacional (CASEN); Ministerio de Planificacion: Ciudad La Paz, Bolivia, 2015; p. 250.
- United Nations. World Population Prospects; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Zheng, L.; Li, G.; Gao, D.; Wang, S.; Meng, X.; Wang, C.; Yuan, H.; Chen, L. Cognitive frailty as a predictor of dementia among older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2020, 87, 103997. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015-The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Lancet 2015, 1, 2112–2117. [Google Scholar]
- Ministerio de Salud de Chile. Encuesta Nacional de Salud ENS Chile 2009–2010: III Metodología; Ministerio de Salud de Chile: Santiago, Chile, 2010.
- Thumala, D.; Kennedy, B.K.; Calvo, E.; Gonzalez-Billault, C.; Zitko, P.; Lillo, P.; Villagra, R.; Ibáñez, A.; Assar, R.; Andrade, M.; et al. Aging and Health Policies in Chile: New Agendas for Research. Health Syst. Reform 2017, 3, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Geda, Y.E.; Topazian, H.M.; Lewis, R.A.; Roberts, R.O.; Knopman, D.S.; Pankratz, V.S.; Christianson, T.J.; Boeve, B.F.; Tangalos, E.G.; Ivnik, R.J.; et al. Engaging in Cognitive Activities, Aging and Mild Cognitive Impairment: A Population-Based Study. J. Neuropsychiatry Clin. Neurosci. 2011, 23, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.; Knopman, D.S. Classification and Epidemiology of MCI. Clin. Geriatr. Med. 2013, 29, 753–772. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud. Encuesta Nacional de Salud 2016–2017 Primeros Resultados; Ministerio de Salud: Santiago, Chile, 2017; p. 61.
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Heutz, R.A.M. Can Mindfulness Beat Alzheimer’s Disease? Maastricht J. Lib. Arts 2017, 9, 33–48. [Google Scholar] [CrossRef]
- Innes, K.E.; Selfe, T.K.; Khalsa, D.S.; Kandati, S. A randomized controlled trial of two simple mind-body programs, Kirtan Kriya meditation and music listening, for adults with subjective cognitive decline: Feasibility and acceptability. Complement. Ther. Med. 2016, 26, 98–107. [Google Scholar] [CrossRef]
- Orgeta, V.; Qazi, A.; Spector, A.; Orrell, M. Psychological treatments for depression and anxiety in dementia and mild cognitive impairment: Systematic review and meta-analysis. Br. J. Psychiatry 2015, 207, 293–298. [Google Scholar] [CrossRef]
- Mirza, S.S.; Wolters, F.J.; Swanson, S.A.; Koudstaal, P.J.; Hofman, A.; Tiemeier, H.; Ikram, M.A. 10-year trajectories of depressive symptoms and risk of dementia: A population-based study. Lancet Psychiatry 2016, 3, 628–635. [Google Scholar] [CrossRef]
- Solfrizzi, V.; D’Introno, A.; Colacicco, A.M.; Capurso, C.; Del Parigi, A.; Caselli, R.J.; Scapicchio, P.L.; Scafato, E.; Gandin, C.; Capurso, A.; et al. Incident occurrence of depressive symptoms among patients with mild cognitive impairment—The Italian longitudinal study on aging. Dement. Geriatr. Cogn. Disord. 2007, 24, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Nazar, G.; Ulloa, N.; Martínez-Sanguinetti, M.A.; Leiva, A.M.; Petermann-Rocha, F.; Martínez, X.D.; Lanuza, F.; Cigarroa, I.; Concha-Cisternas, Y.; Troncoso, C.; et al. Association between cognitive impairment and depression in Chilean older adults. Rev. Med. Chile 2020, 148, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Steenland, K.; Karnes, C.; Seals, R.; Carnevale, C.; Hermida, A.; Levey, A. Late-life depression as a risk factor for mild cognitive impairment or Alzheimer’s disease in 30 US Alzheimer’s disease centers. J. Alzheimers Dis. 2012, 31, 265–275. [Google Scholar] [CrossRef]
- Ma, L. Depression, Anxiety, and Apathy in Mild Cognitive Impairment: Current Perspectives. Front. Aging Neurosci. 2020, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Josman, N.; Abdallah, T.M.; Engel-Yeger, B. Using the LOTCA to measure cultural and sociodemographic effects on cognitive skills in two groups of children. Am. J. Occup. Ther. 2011, 65, 29–37. [Google Scholar] [CrossRef]
- Mallya, S.; Fiocco, A.J. Effects of Mindfulness Training on Cognition and Well-Being in Healthy Older Adults. Mindfulness 2016, 7, 453–465. [Google Scholar] [CrossRef]
- Albala, C.; Lera, L.; Sanchez, H.; Angel, B.; Márquez, C.; Arroyo, P.; Fuentes, P. Frequency of frailty and its association with cognitive status and survival in older Chileans. Clin. Interv. Aging 2017, 12, 995–1001. [Google Scholar] [CrossRef]
- Llewellyn, D.J.; Lang, I.A.; Langa, K.M.; Huppert, F.A. Cognitive function and psychological well-being: Findings from a population-based cohort. Age Ageing 2008, 37, 685–689. [Google Scholar] [CrossRef]
- Ribeiro, O.; Teixeira, L.; Araújo, L.; Rodríguez-Blázquez, C.; Calderón-Larrañaga, A.; Forjaz, M.J. Anxiety, Depression and Quality of Life in Older Adults: Trajectories of Influence across Age. Int. J. Environ. Res. Public Health 2020, 17, 9039. [Google Scholar] [CrossRef]
- Sanford, A. Mild Cognitive Impairment. Clin. Geriatr. Med. 2017, 55, 464–467. [Google Scholar] [CrossRef]
- Siu, M.; Lee, D.T.F. Effects of tai chi on cognition and instrumental activities of daily living in community dwelling older people with mild cognitive impairment. BMC Geriatr. 2018, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Farhang, M.; Miranda-Castillo, C.; Rubio, M.; Furtado, G. Impact of mind-body interventions in older adults with mild cognitive impairment: A systematic review. Int. Psychogeriatr. 2019, 31, 643–666. [Google Scholar] [CrossRef] [PubMed]
- Eyre, H.A.; Siddarth, P.; Acevedo, B.; Van Dyk, K.; Paholpak, P.; Ercoli, L.; Cyr, N.S.; Yang, H.; Khalsa, D.S.; Lavretsky, H. A randomized controlled trial of Kundalini yoga in mild cognitive impairment. Int. Psychogeriatr. 2017, 29, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Sungkarat, S.; Boripuntakul, S.; Chattipakorn, N.; Watcharasaksilp, K.; Lord, S.R. Effects of Tai Chi on Cognition and Fall Risk in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2017, 65, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.P.; Coles, J.; Chambers, R.; Wu, D.B.C.; Hassed, C. The Effects of Mindfulness on Older Adults with Mild Cognitive Impairment. J. Alzheimer Dis. Rep. 2017, 1, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A.; Michalsen, A.; Khalsa, S.B.S.; Telles, S.; Sherman, K.J. Effects of yoga on mental and physical health: A short summary of reviews. Evid. Based Complement. Altern. Med. 2012, 2012, 165410. [Google Scholar] [CrossRef]
- Lopes, K.T.; Costa, D.F.; Santos, L.F.; Castro, D.P.; Bastone, A.C. Prevalence of fear of falling among a population of older adults and its correlation with mobility, dynamic balance, risk and history of falls. Braz. J. Phys. Ther. 2009, 13, 223–229. [Google Scholar] [CrossRef]
- Cramer, H.; Schäfer, M.; Schöls, M.; Köcke, J.; Elsenbruch, S.; Lauche, R.; Engler, H.; Dobos, G.; Langhorst, J. Randomised clinical trial: Yoga vs. written self-care advice for ulcerative colitis. Aliment. Pharmacol. Ther. 2017, 45, 1379–1389. [Google Scholar] [CrossRef]
- Sengupta, P. Challenge of infertility: How protective the yoga therapy is? Anc. Sci. Life 2012, 32, 61–62. [Google Scholar] [CrossRef]
- Woodyard, C. Exploring the therapeutic effects of yoga and its ability to increase quality of life. Int. J. Yoga 2011, 4, 49–54. [Google Scholar] [CrossRef]
- Ni, M.; Mooney, K.; Signorile, J.F. Controlled pilot study of the effects of power yoga in Parkinson’s disease. Complement. Ther. Med. 2016, 25, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Nick, N.; Petramfar, P.; Ghodsbin, F.; Keshavarzi, S.; Jahanbin, I. The Effect of Yoga on Balance and Fear of Falling in Older Adults. PMR 2016, 1, 145–151. [Google Scholar]
- Bhattacharyya, K.K.; Andel, R.; Small, B.J. Effects of yoga-related mind-body therapies on cognitive function in older adults: A systematic review with meta-analysis. Arch. Gerontol. Geriatr. 2021, 93, 104319. [Google Scholar] [CrossRef] [PubMed]
- Tremont, G.; Davis, J.; Ott, B.R.; Uebelacker, L.; Kenney, L.; Gillette, T.; Britton, K.; Sanborn, V. Feasibility of a Yoga Intervention for Individuals with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Integr. Complement. Med. 2022, 28, 250–260. [Google Scholar] [CrossRef]
- Chobe, S.; Patra, S.K.; Chobe, M.; Metri, K. Efficacy of Integrated Yoga and Ayurveda Rasayana on cognitive functions in elderly with mild cognitive impairment: Non-randomized three-arm clinical trial. J. Ayurveda Integr. Med. 2022, 13, 100373. [Google Scholar] [CrossRef]
- Gothe, N.P.; Kramer, A.F.; McAuley, E. The effects of an 8-week hatha yoga intervention on executive function in older adults. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Baklouti, S.; Aloui, A.; Baklouti, H.; Jarraya, M. Effects of Hatha yoga on cognitive functions in the elderly: A cross-sectional study. Libyan J. Med. 2022, 17, 2080799. [Google Scholar] [CrossRef]
- Desai, R.; Tailor, A.; Bhatt, T. Effects of yoga on brain waves and structural activation: A review. Complement. Ther. Clin. Pract. 2015, 21, 112–118. [Google Scholar] [CrossRef]
- Marciniak, R.; Sheardova, K.; Čermáková, P.; Hudeček, D.; Šumec, R.; Hort, J. Effect of meditation on cognitive functions in context of aging and neurodegenerative diseases. Front. Behav. Neurosci. 2014, 8, 17. [Google Scholar] [CrossRef]
- Yang, H.; Leaver, A.M.; Siddarth, P.; Paholpak, P.; Ercoli, L.; St. Cyr, N.M.; Eyre, H.A.; Narr, K.L.; Khalsa, D.S.; Lavretsky, H. Neurochemical and neuroanatomical plasticity following memory training and yoga interventions in older adults with mild cognitive impairment. Front. Aging Neurosci. 2016, 8, 277. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Hanh, T.N. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; Delacorte: New York, NY, USA, 1990. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Wong, W.P.; Hassed, C.; Chambers, R.; Coles, J. The effects of mindfulness on persons with mild cognitive impairment: Protocol for a mixed-methods longitudinal study. Front. Aging Neurosci. 2016, 8, 156. [Google Scholar] [CrossRef] [PubMed]
- Larouche, E.; Hudona, C.; Gouleta, S. Potential benefits of mindfulness-based interventions in mild cognitive impairment and Alzheimer’s disease: An interdisciplinary perspective. Behav. Brain Res. 2015, 276, 199–212. [Google Scholar] [CrossRef]
- Marciniak, R.; Šumec, R.; Vyhnálek, M.; Bendíčková, K.; Lázničková, P.; Forte, G.; Jeleník, A.; Římalová, V.; Frič, J.; Hort, J.; et al. The Effect of Mindfulness-Based Stress Reduction (MBSR) on Depression, Cognition, and Immunity in Mild Cognitive Impairment: A Pilot Feasibility Study. Clin. Interv. Aging 2020, 15, 1365–1381. [Google Scholar] [CrossRef] [PubMed]
- Doshi, K.; Henderson, S.L.; Fan, Q.; Wong, K.F.; Lim, J. Mindfulness-Based Training Does Not Improve Neuropsychological Outcomes in Mild Cognitive Impairment More Than Spontaneous Reversion Rates: A Randomized Controlled Trial. J. Alzheimer Dis. 2021, 84, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Loprinzi, P.D.; Yeung, A.S.; Zeng, N.; Huang, T. The Beneficial Effects of Mind-Body Exercises for People With Mild Cognitive Impairment: A Systematic Review With Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 1556–1573. [Google Scholar] [CrossRef]
- Han, A. Mindfulness-Based Interventions for Older Adults with Dementia or Mild Cognitive Impairment: A Meta-Analysis. Clin. Gerontol. 2022, 45, 763–776. [Google Scholar] [CrossRef]
- Wells, R.E.; Yeh, G.Y.; Kerr, C.E.; Wolkin, J.; Davis, R.B.; Tan, Y.; Spaeth, R.; Wall, R.B.; Walsh, J.; Kaptchuk, T.J.; et al. Meditation’s impact on default mode network and hippocampus in mild cognitive impairment: Pilot study. Neurosci. Lett. 2013, 556, 15–19. [Google Scholar] [CrossRef]
- Shim, M.; Tilley, J.L.; Im, S.; Price, K.; Gonzalez, A. A Systematic Review of Mindfulness-Based Interventions for Patients with Mild Cognitive Impairment or Dementia and Caregivers. J. Geriatr. Psychiatry Neurol. 2020, 34, 528–554. [Google Scholar] [CrossRef]
- Kurth, F.; Cherbuin, N.; Luders, E. Promising links between meditation and reduced (brain) aging: An attempt to bridge some gaps between the alleged fountain of youth and the youth of the field. Front. Psychol. 2017, 8, 860. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Dickersin, K.; Moher, D. SPIRIT 2013: New guidance for content of clinical trial protocols. Lancet 2013, 381, 91–92. [Google Scholar] [CrossRef]
- Wong, G.K.C.; Mak, J.S.Y.; Wong, A.; Zheng, V.Z.Y.; Poon, W.S.; Abrigo, J.; Mok, V.C.T. Minimum Clinically Important Difference of Montreal Cognitive Assessment in aneurysmal subarachnoid hemorrhage patients. J. Clin. Neurosci. 2017, 46, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Chobe, S.; Chobe, M.; Metri, K.; Patra, S.K.; Nagaratna, R. Impact of Yoga on cognition and mental health among elderly: A systematic review. Complement. Ther. Med. 2020, 52, 102421. [Google Scholar] [CrossRef]
- Martens, N.L. Yoga Interventions Involving Older Adults: Integrative Review. J. Gerontol. Nurs. 2022, 48, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Krejčí, M.; Hill, M.; Kajzar, J.; Tichý, M.; Hošek, V. Yoga Exercise Intervention Improves Balance Control and Prevents Falls in Seniors Aged 65. Zdr. Varst. 2022, 61, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Delgado, C.; Araneda, A.; Behrens, M.I. Validación del instrumento Montreal Cognitive Assessment en español en adultos mayores de 60 años. Neurología 2019, 34, 376–385. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of dailyliving. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Hervás, G.; Vázquez, C. Construction and validation of a measure of integrative well-being in seven languages: The Pemberton Happiness Index. Health Qual. Life Outcomes 2013, 11, 66. [Google Scholar] [CrossRef]
- Martínez Zelaya, G.; Bilbao, M.; Costa, D.; da Costa, S. Latinoamericanos, Bienestar y su medida: Validación del Pemberton Happiness Index en 3 países. Rev. Latinoam. Psicol. Posit. 2018, 4, 125–140. [Google Scholar]
- Miranda-Castillo, C.; Contreras, D.; Garay, K.; Martínez, P.; León-Campos, M.O.; Farhang, M.; Morán, J.; Fernández-Fernández, V. Validation of the Geriatric Anxiety Inventory in Chilean older people. Arch. Gerontol. Geriatr. 2019, 83, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Yochim, B.; Mueller, A.; June, A.; Segal, D. Psychometric Properties of the Geriatric Anxiety Scale: Comparison to the Beck Anxiety Inventory and Geriatric Anxiety Inventory. Clin. Gerontol. 2011, 34, 21–33. [Google Scholar] [CrossRef]
- Trinidad, M.; Eduardo, V.; Pedro, P. The Geriatric Depression Scale (GDS). Rev. Med. 2002, 128. [Google Scholar] [CrossRef]
- Gómez-Angulo, C.; Campo-Arias, A. Escala de Yesavage para Depresión Geriátrica (GDS-15 y GDS-5): Estudio de la consistencia interna y estructura factorial. Univ. Psychol. 2014, 10, 735–743. [Google Scholar] [CrossRef]
- Li, L.; Wang, Y.; Yan, J.; Chen, Y.; Zhou, R.; Yi, X.; Shi, Q.; Zhou, H. Clinical predictors of cognitive decline in patients with mild cognitive impairment: The Chongqing aging study. J. Neurol. 2012, 259, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.L.; Qiu, C.X.; Wahlin, A.; Winblad, B.; Fratiglioni, L. Diabetes mellitus and risk of dementia in the Kungsholmen project: A 6-year follow-up study. Neurology 2004, 63, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.-Y.; Zhao, X.-D.; Zhu, B.-G.; Hu, C.-P. Demographic Factors and Cognitive Function Assessments Associated with Mild Cognitive Impairment Progression for the Elderly. Biomed. Res. Int. 2020, 2020, 3054373. [Google Scholar] [CrossRef]
- Rojas, G.; Martínez, P.; Guajardo, V.; Campos, S.; Herrera, P.; Vöhringer, P.A.; Gómez, V.; Szabo, W.; Araya, R. A collaborative, computer-assisted, psycho-educational intervention for depressed patients with chronic disease at primary care: Protocol for a cluster randomized controlled trial. BMC Psychiatry 2021, 21, 418. [Google Scholar] [CrossRef]
- Goel, M.K.; Khanna, P.; Kishore, J. Understanding survival analysis: Kaplan-Meier estimate. Int. J. Ayurveda Res. 2010, 1, 274–278. [Google Scholar] [CrossRef]
- Wang, H.; Li, T.; Barbarino, P.; Gauthier, S.; Brodaty, H.; Molinuevo, J.L.; Xie, H.; Sun, Y.; Yu, E.; Tang, Y.; et al. Dementia care during COVID-19. Lancet 2020, 395, 1190–1191. [Google Scholar] [CrossRef]
- Slachevsky, A.; Zitko, P.; Martínez-Pernía, D.; Forno, G.; Court, F.A.; Lillo, P.; Villagra, R.; Duran-Aniotz, C.; Parrao, T.; Assar, R.; et al. GERO Cohort Protocol, Chile, 2017–2022: Community-based Cohort of Functional Decline in Subjective Cognitive Complaint elderly. BMC Geriatr. 2020, 20, 505. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Wiels, W.A.; Wittens, M.M.J.; Zeeuws, D.; Baeken, C.; Engelborghs, S. Neuropsychiatric Symptoms in Mild Cognitive Impairment and Dementia Due to AD: Relation with Disease Stage and Cognitive Deficits. Front. Psychiatry 2021, 12, 707580. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Liu, C.; Yu, D.; Fawkes, S.; Ma, J.; Zhang, M.; Li, C. Prevalence of mild cognitive impairment in community-dwelling Chinese populations aged over 55 years: A meta-analysis and systematic review. BMC Geriatr. 2021, 21, 10. [Google Scholar] [CrossRef]
- Mone, P.; Pansini, A.; Frullone, S.; de Donato, A.; Buonincontri, V.; De Blasiis, P.; Marro, A.; Morgante, M.; De Luca, A.; Santulli, G. Physical decline and cognitive impairment in frail hypertensive elders during COVID-19. Eur. J. Intern. Med. 2022, 99, 89–92. [Google Scholar] [CrossRef]
- Pansini, A.; Lombardi, A.; Morgante, M.; Frullone, S.; Marro, A.; Rizzo, M.; Martinelli, G.; Boccalone, E.; De Luca, A.; Santulli, G.; et al. Hyperglycemia and Physical Impairment in Frail Hypertensive Older Adults. Front. Endocrinol. 2022, 13, 831556. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud Centro de Prensa. La Salud Mental y Los Adultos Mayores. Ginebra Suiza OMS. 2016, pp. 5–9. Available online: https://www.who.int/es/news-room/fact-sheets/detail/la-salud-mental-y-los-adultos-mayores (accessed on 20 August 2022).


{kind=link}
| Study Period | |||||||
|---|---|---|---|---|---|---|---|
| Enrolment | Allocation | Post-Allocation | Close-Out | ||||
| Timepoint ** | −t1 | 0 | t1 | t2 | t3 | t4 | t5 |
| Enrolment | Baseline | Intervention | Post | 3M | 6M | ||
| Eligibility screen | X | ||||||
| Informed consent | X | ||||||
| Allocation | X | ||||||
| Intervention | |||||||
| YBM Intervention | X | ||||||
| Control | |||||||
| PES | X | ||||||
| Assessments | |||||||
| MoCA | X | X | X | X | |||
| Demographic | X | ||||||
| BI | X | X | X | X | |||
| IADL | X | X | X | X | |||
| PHI | X | X | X | X | |||
| GAI | X | X | X | X | |||
| GDS-5 | X | X | X | X | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farhang, M.; Rojas, G.; Martínez, P.; Behrens, M.I.; Langer, Á.I.; Diaz, M.; Miranda-Castillo, C. The Impact of a Yoga-Based Mindfulness Intervention versus Psycho-Educational Session for Older Adults with Mild Cognitive Impairment: The Protocol of a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 15374. https://doi.org/10.3390/ijerph192215374
Farhang M, Rojas G, Martínez P, Behrens MI, Langer ÁI, Diaz M, Miranda-Castillo C. The Impact of a Yoga-Based Mindfulness Intervention versus Psycho-Educational Session for Older Adults with Mild Cognitive Impairment: The Protocol of a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(22):15374. https://doi.org/10.3390/ijerph192215374
Chicago/Turabian StyleFarhang, Maryam, Graciela Rojas, Pablo Martínez, Maria Isabel Behrens, Álvaro I. Langer, Marcela Diaz, and Claudia Miranda-Castillo. 2022. "The Impact of a Yoga-Based Mindfulness Intervention versus Psycho-Educational Session for Older Adults with Mild Cognitive Impairment: The Protocol of a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 22: 15374. https://doi.org/10.3390/ijerph192215374
APA StyleFarhang, M., Rojas, G., Martínez, P., Behrens, M. I., Langer, Á. I., Diaz, M., & Miranda-Castillo, C. (2022). The Impact of a Yoga-Based Mindfulness Intervention versus Psycho-Educational Session for Older Adults with Mild Cognitive Impairment: The Protocol of a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(22), 15374. https://doi.org/10.3390/ijerph192215374