
Disaster Evacuation for Home-Based Patients with Special Healthcare Needs: A Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Terms Used in Study
2.1.1. Public Shelter
2.1.2. Welfare Shelter
2.1.3. Pediatric Patients Receiving Home Medical Care
2.2. Data Collection
2.3. Survey Content
2.3.1. Background Information about Pediatric Patients Requiring Home Medical Care
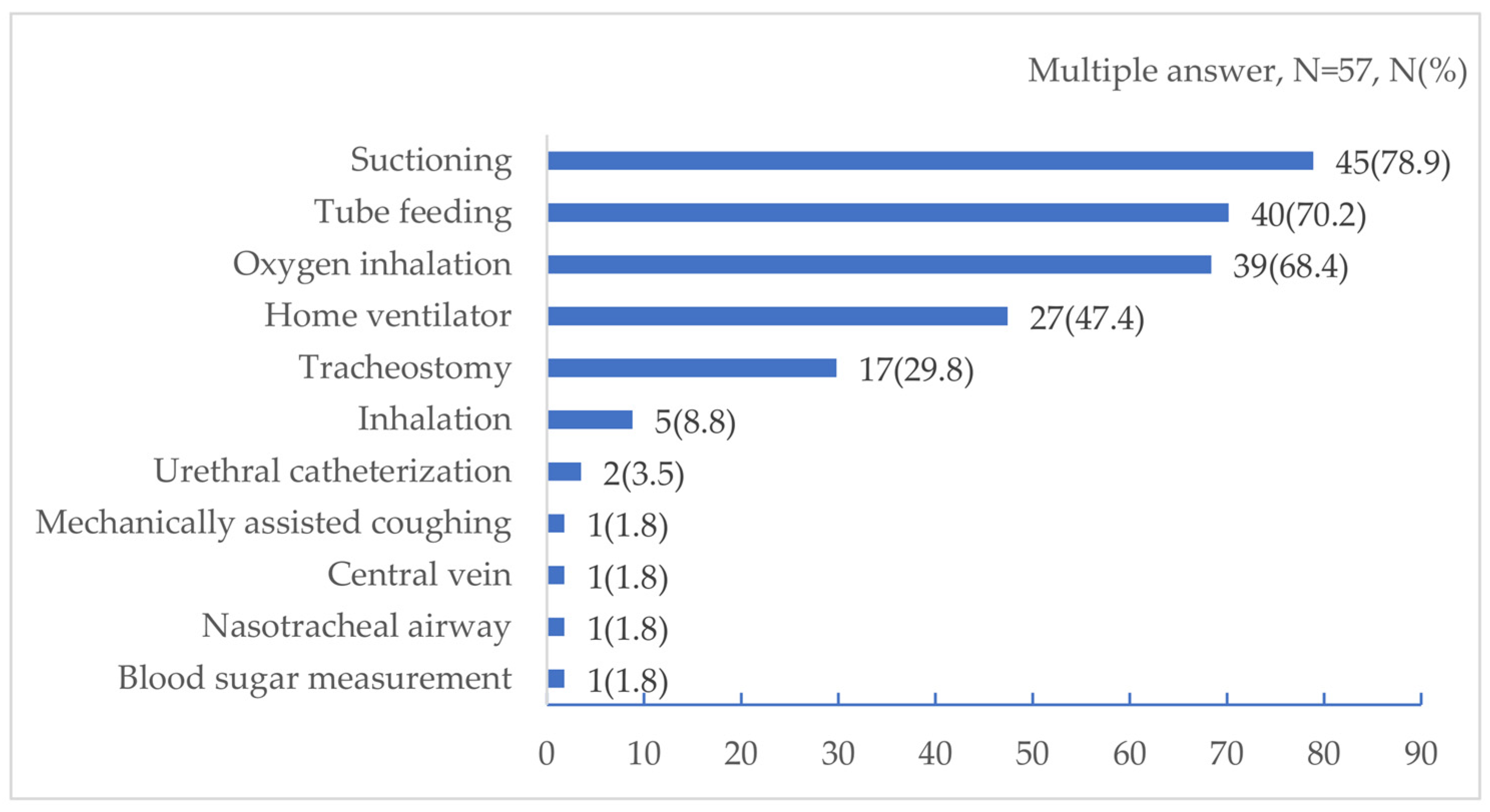
2.3.2. Medical Devices and Procedures
2.3.3. Family Caregiver Background
2.3.4. Preparation in the Event of a Disaster
2.3.5. Destination of, Preparation for, and Intention to Evacuate
2.3.6. Knowledge of Welfare Shelters, Decentralized Evacuation
2.3.7. Disaster Risk in Residential Areas
2.4. Analytical Methods
2.5. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamada, Y.; Satoh, M.; Sugi, M.; Kodama, C.; Noda, A.T.; Nakano, M.; Nasuno, T. Response of Tropical Cyclone Activity and Structure to Global Warming in a High-Resolution Global Nonhydrostatic Model. J. Clim. 2017, 30, 9703–9724. [Google Scholar] [CrossRef]
- Kato, T. Quasi-Stationary Band-Shaped Precipitation Systems, Named “Senjo-Kousuitai”, Causing Localized Heavy Rainfall in Japan. J. Meteorol. Soc. Jpn. Ser. II 2020, 98, 485–509. [Google Scholar] [CrossRef]
- Japan Meteorological Agency Commentary on “Senjo-Kousuitai”. Available online: https://www.jma.go.jp/jma/kishou/know/bosai/kishojoho_senjoukousuitai.html (accessed on 8 August 2022). (In Japanese).
- Hirockawa, Y.; Kato, T.; Tsuguti, H.; Seino, N. Identification and Classification of Heavy Rainfall Areas and Their Characteristic Features in Japan. J. Meteorol. Soc. Jpn. Ser. II 2020, 98, 835–857. [Google Scholar] [CrossRef]
- Takasaki, Y.; Yoshizaki, M.; Suzuki-Parker, A.; Watarai, Y. Sensitivity of Quasi-Stationary Band-Shaped Precipitation System to Topography: A Case Study for 28 August 2008 Okazaki Heavy Rainfall Event. J. Meteorol. Soc. Jpn. Ser. II 2019, 97, 453–466. [Google Scholar] [CrossRef]
- Kyushu Electric Power Co., Inc. Results of Response to Disasters. Available online: https://www.kyuden.co.jp/company_history_energy_disaster_disaster.html (accessed on 9 August 2022). (In Japanese).
- Dugan, J.; Byles, D.; Mohagheghi, S. Social Vulnerability to Long-Duration Power Outages. 2022. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4172862 (accessed on 12 September 2022).
- Stanberry, L.R.; Thomson, M.C.; James, W. Prioritizing the Needs of Children in a Changing Climate. PLOS Med. 2018, 15, e1002627. [Google Scholar] [CrossRef]
- Anderko, L.; Chalupka, S.; Du, M.; Hauptman, M. Climate Changes Reproductive and Children’s Health: A Review of Risks, Exposures, and Impacts. Pediatr. Res. 2020, 87, 414–419. [Google Scholar] [CrossRef]
- Barfield, W.D.; Krug, S.E.; Watterberg, K.L.; Aucott, S.W.; Benitz, W.E.; Eichenwald, E.C.; Goldsmith, J.P.; Hand, I.L.; Committee on Fetus and Newborn; Disaster Preparedness Advisory Council; et al. Disaster Preparedness in Neonatal Intensive Care Units. Pediatrics 2017, 139, e20170507. [Google Scholar] [CrossRef]
- Nakayama, T.; Tanaka, S.; Uematsu, M.; Kikuchi, A.; Hino-Fukuyo, N.; Morimoto, T.; Sakamoto, O.; Tsuchiya, S.; Kure, S. Effect of a Blackout in Pediatric Patients with Home Medical Devices during the 2011 Eastern Japan Earthquake. Brain Dev. 2014, 36, 143–147. [Google Scholar] [CrossRef]
- Runkle, J.D.; Brock-Martin, A.; Karmaus, W.; Svendsen, E.R. Secondary Surge Capacity: A Framework for Understanding Long-Term Access to Primary Care for Medically Vulnerable Populations in Disaster Recovery. Am. J. Public Health 2012, 102, e24–e32. [Google Scholar] [CrossRef]
- Lazo, J.K.; Bostrom, A.; Morss, R.E.; Demuth, J.L.; Lazrus, H. Factors Affecting Hurricane Evacuation Intentions. Risk Anal. 2015, 35, 1837–1857. [Google Scholar] [CrossRef]
- Trumbo, C.; Meyer, M.A.; Marlatt, H.; Peek, L.; Morrissey, B. An Assessment of Change in Risk Perception and Optimistic Bias for Hurricanes Among Gulf Coast Residents. Risk Anal. 2014, 34, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Bateman, J.M.; Edwards, B. Gender and Evacuation: A Closer Look at Why Women Are More Likely to Evacuate for Hurricanes. Nat. Hazards Rev. 2002, 3, 107–117. [Google Scholar] [CrossRef]
- Brodar, K.E.; La Greca, A.M.; Tarlow, N.; Comer, J.S. “My Kids Are My Priority”: Mothers’ Decisions to Evacuate for Hurricane Irma and Evacuation Intentions for Future Hurricanes. J. Fam. Issues 2020, 41, 2251–2274. [Google Scholar] [CrossRef]
- Collins, J.; Ersing, R.; Polen, A. Evacuation Decision-Making during Hurricane Matthew: An Assessment of the Effects of Social Connections. Weather Clim. Soc. 2017, 9, 769–776. [Google Scholar] [CrossRef]
- Dash, N.; Gladwin, H. Evacuation Decision Making and Behavioral Responses: Individual and Household. Nat. Hazards Rev. 2007, 8, 69–77. [Google Scholar] [CrossRef]
- Peek, L.; Stough, L.M. Children with Disabilities in the Context of Disaster: A Social Vulnerability Perspective. Child Dev. 2010, 81, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Kailes, J.I.; Enders, A. Moving Beyond “Special Needs”: A Function-Based Framework for Emergency Management and Planning. J. Disabil. Policy Stud. 2007, 17, 230–237. [Google Scholar] [CrossRef]
- Na, H.S.; Grace, R. Influence of Social Networks and Opportunities for Social Support on Evacuation Destination Decision-Making. Saf. Sci. 2022, 147, 105564. [Google Scholar] [CrossRef]
- Whytlaw, J.L.; Hutton, N.; Yusuf, J.-E.; Richardson, T.; Hill, S.; Olanrewaju-Lasisi, T.; Antwi-Nimarko, P.; Landaeta, E.; Diaz, R. Changing Vulnerability for Hurricane Evacuation during a Pandemic: Issues and Anticipated Responses in the Early Days of the COVID-19 Pandemic. Int. J. Disaster Risk Reduct. 2021, 61, 102386. [Google Scholar] [CrossRef]
- Renne, J.L.; Mayorga, E. What Has America Learned Since Hurricane Katrina? Evaluating Evacuation Plans for Carless and Vulnerable Populations in 50 Large Cities across the United States. Int. J. Disaster Risk Reduct. 2022, 80, 103226. [Google Scholar] [CrossRef]
- Cabinet Office Measures for People Vulnerable to Disasters. Available online: https://www.bousai.go.jp/taisaku/hisaisyagyousei/youengosya/index.html (accessed on 12 September 2022). (In Japanese).
- Japan Meteorological Agency Correspondence between Weather Information and Warning Levels. Available online: https://www.jma.go.jp/jma/kishou/know/bosai/alertlevel.html (accessed on 12 September 2022). (In Japanese).
- Takaoka, S.; Kawata, Y.; Kai, T. A Study of Issues Related to the Operation of Evacuation Shelters in a Corona-Endemic Society—Through the Guidelines and Training of Shiga Prefecture in Japan. J. Disaster Res. 2021, 16, 40–47. [Google Scholar] [CrossRef]
- Cabinet Office 2021 White Paper on Disaster Prevention, Measures for Shelters Based on the Infection Status of COVID-19. Available online: https://www.bousai.go.jp/kaigirep/hakusho/r03/honbun/0b_1s_01_01.html (accessed on 12 September 2022). (In Japanese).
- Old Dominion University Life in Hampton Roads Survey: Hurricanes and COVID-19. Available online: http://www.odu.edu/news/2020/8/lihr_hurricanes_and_ (accessed on 12 September 2022).
- Ministry of Health, Labour and Welfare. Trends in Policies for Special Healthcare Needs Children. Available online: https://www.mhlw.go.jp/content/10800000/000584473.pdf (accessed on 12 September 2022). (In Japanese)
- Karaye, I.M.; Thompson, C.; Horney, J.A. Evacuation Shelter Deficits for Socially Vulnerable Texas Residents During Hurricane Harvey. Health Serv. Res. Manag. Epidemiol. 2019, 6, 2333392819848885. [Google Scholar] [CrossRef]
- Kako, M.; Steenkamp, M.; Ryan, B.; Arbon, P.; Takada, Y. Best Practice for Evacuation Centres Accommodating Vulnerable Populations: A Literature Review. Int. J. Disaster Risk Reduct. 2020, 46, 101497. [Google Scholar] [CrossRef]
- Fukuoka City List of Evacuation Sites and Public Shelters. Available online: https://www.city.fukuoka.lg.jp/bousai/shiteihinannbasyooyobishiteihinannjyoitirann.html (accessed on 15 October 2022). (In Japanese).
- Cabinet Office 2015 Disaster Prevention White Paper, Evacuation Site/Public Shelter. Available online: https://www.bousai.go.jp/kaigirep/hakusho/h27/honbun/1b_1s_02_02.html (accessed on 8 August 2022). (In Japanese).
- Ministry of Education, Culture, Sports, Science and Technology Investigation on Disaster Prevention Functions of Public Schools That Serve as Evacuation Shelters, as of 1 April 2017. Available online: https://www.mext.go.jp/a_menu/shisetu/bousai/1394437.htm (accessed on 12 September 2022). (In Japanese).
- Cabinet Office Revision of Guidelines for Securing and Operating Welfare Shelters, May 2021. Available online: https://www.bousai.go.jp/taisaku/hinanjo/r3_guideline.html (accessed on 11 September 2022).
- Schmidt, A.; Ilango, S.M.; McManus, M.A.; Rogers, K.K.; White, P.H. Outcomes of Pediatric to Adult Health Care Transition Interventions: An Updated Systematic Review. J. Pediatr. Nurs. 2020, 51, 92–107. [Google Scholar] [CrossRef]
- Japan Pediatric Society Recommendations for Transitional Care for Patients with Childhood-Onset Diseases, Japan Pediatric Society. Available online: http://www.jpeds.or.jp/modules/guidelines/index.php?content_id=54 (accessed on 18 September 2022). (In Japanese).
- White, P.H.; Cooley, W.C.; Boudreau, A.D.A.; Cyr, M.; Davis, B.E.; Dreyfus, D.E.; Forlenza, E.; Friedland, A.; Greenlee, C.; Mann, M.; et al. Supporting the Health Care Transition from Adolescence to Adulthood in the Medical Home. Pediatrics 2018, 142, e20182587. [Google Scholar] [CrossRef]
- General Perinatal Maternal and Child Medical Care Center, F.U.H. General Perinatal Maternal and Child Medical Care Center, Fukuoka University Hospital. Available online: https://www.hop.fukuoka-u.ac.jp/center/04/ (accessed on 15 October 2022). (In Japanese).
- Fukuoka University Hospital. Available online: https://www.hop.fukuoka-u.ac.jp/eng/ (accessed on 31 August 2022). (In Japanese).
- Tanaka, S. Severe mental and physical disability medical care at the time of disaster—Problems and countermeasures in the event of a disaster, preparation in advance. Jpn. J. Pediatr. Med. 2015, 47, 1894–1898. (In Japanese) [Google Scholar]
- Nakagawa, K.; Yamamoto, M.; Kitamura, Y.; Yoneyama, A.; Kato, K. Awareness of disaster prevention among families of children with severe physical and mental disabilities living in the Tokyo metropolitan area—Degree of recognition of welfare shelter, intention to evacuate, demands to live in an evacuation shelter. J. Child Health 2016, 75, 621–628. (In Japanese) [Google Scholar]
- Ministry of Health, Labour and Welfare. Regarding pediatric medical care. In Proceedings of the 17th Meeting on the Review of Medical Plans; Available online: https://www.mhlw.go.jp/content/10800000/000584472.pdf (accessed on 31 August 2022). (In Japanese).
- Ministry of Internal Affairs and Communications. Japan Summary of 2020 Census Population Results. Available online: https://www.stat.go.jp/data/kokusei/2020/kekka/pdf/outline_01.pdf (accessed on 15 October 2021). (In Japanese)
- Vásquez, W.F.; Murray, T.J.; Mozumder, P. Understanding Hurricane Evacuation Planning in the Northeastern and Mid-Atlantic United States. Nat. Hazards Rev. 2016, 17, 04015018. [Google Scholar] [CrossRef]
- Bloom, S.R.; Kuhlthau, K.; Van Cleave, J.; Knapp, A.A.; Newacheck, P.; Perrin, J.M. Health Care Transition for Youth with Special Health Care Needs. J. Adolesc. Health 2012, 51, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Kato, H. Childhood Chronic Specified Disease Child Adult Transitional Medical Support Model Project (Document 2). Available online: https://www.mhlw.go.jp/file/05-Shingikai-12601000-Seisakutoukatsukan-Sanjikanshitsu_Shakaihoshoutantou/0000170303.pdf (accessed on 20 September 2022). (In Japanese).
- Kumode, M.; Hoshino, R.; Sato, S.; Matsubasa, T.; Nagae, A.; Fujita, Y. Fact-Finding Survey of Children with Advanced Special Healthcare Needs. J. Jpn. Soc. Pediatr. Surg. 2018, 22, 1519–1526. (In Japanese) [Google Scholar]
- Araki, S.; Nakamura, K.; Kashiwabara, Y.; Eguchi, H.; Shimono, M. A Field Survey of Working Conditions of Parents with Children Requiring Medical Care. J. UOEH 2019, 41, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. Report of a Survey on the Actual Situation Regarding the Lives of Patients with Special Healthcare Needs and Family Caregivers at Home. Available online: https://www.mhlw.go.jp/content/12200000/000653544.pdf (accessed on 20 September 2022). (In Japanese)
- Nakai, H.; Tsukasaki, K.; Kyota, K.; Itatani, T.; Nihonyanagi, R.; Shinmei, Y.; Yasuoka, S. Factors Related to Evacuation Intentions of Power-Dependent Home Care Patients in Japan. J. Community Health Nurs. 2016, 33, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Takada, S. Post-Traumatic Stress Disorders and Mental Health Care (Lessons Learned from the Hanshin-Awaji Earthquake, Kobe, 1995). Brain Dev. 2013, 35, 214–219. [Google Scholar] [CrossRef]
- Tanaka, S. Issues in the Support and Disaster Preparedness of Severely Disabled Children in Affected Areas. Brain Dev. 2013, 35, 209–213. [Google Scholar] [CrossRef]
- Takasugi, T.; Umeyama, G.; Shimazaki, K.; Yokoyama, Y.; Haraoka, T.; Ikeda, M.; Okada, E.; Ojima, T. Issues and Countermeasures Regarding Disaster Response in the Healthcare and Welfare Fields for Persons Requiring Special Care and Consideration in the Kumamoto Earthquake: Through Qualitative Research. J. Natl. Inst. Public Health 2020, 69, 296–305. (In Japanese) [Google Scholar] [CrossRef]
- Kanai, J.; Nakano, S. Survey on Theactual Conditons of Welfare Evacuation Shelthers in the Kumamoto Earthquake. J. Geol. Eng. F6 2018, 74, I_131–I_136. (In Japanese) [Google Scholar] [CrossRef]
- Knai, J.; Nakano, S.; Nonomura, A.; Uno, K. Conduct Survey about Evacuation Center for Vulnerable People in Shikoku Area. J. Geol. Eng. F6 2016, 72, I_145–I_150. (In Japanese) [Google Scholar] [CrossRef]


{kind=link}
| Item | Category | Total | Invention to Evacuate to Public Shelter | p-Value | ||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| N (%) | N (%) | N (%) | ||||
| Patients with home medical care background | ||||||
| Age (median [rang]) | 7.0 (0–46) | |||||
| Number of cohabitants (Mean [Standard deviation]) | 3.9 (0.9) | |||||
| Age group | Younger than 15 years | 48 (84.2) | 21 (43.8) | 27 (56.3) | 0.969 a | |
| 15 years or older | 9 (15.8) | 4 (44.4) | 5 (55.6) | |||
| Sex | Men | 29 (50.9) | 12 (41.4) | 17 (58.6) | 0.701 a | |
| Women | 28 (49.1) | 13 (46.4) | 15 (53.6) | |||
| Number of cohabitants | Less than 4 | 16 (28.1) | 11 (68.8) | 5 (31.3) | 0.018 a | |
| 4 or more | 41 (71.9) | 14 (34.1) | 27 (65.9) | |||
| Necessary medical devices and procedures | ||||||
| Home ventilator | Yes | 27 (47.4) | 8 (29.6) | 19 (70.4) | 0.040 a | |
| No | 30 (52.6) | 17 (56.7) | 13 (43.3) | |||
| Tracheostomy | Yes | 17 (29.8) | 8 (47.1) | 9 (52.9) | 0.751 a | |
| No | 40 (70.2) | 17 (42.5) | 23 (57.5) | |||
| Oxygen inhalation | Yes | 39 (68.4) | 16 (41.0) | 23 (59.0) | 0.526 a | |
| No | 18 (31.6) | 9 (50.0) | 9 (50.0) | |||
| Suctioning | Yes | 45 (78.9) | 18 (40.0) | 27 (60.0) | 0.255 a | |
| No | 12 (21.1) | 7 (58.3) | 5 (41.7) | |||
| Tube feeding | Yes | 40 (70.2) | 20 (50.0) | 20 (50.0) | 0.152 a | |
| No | 17 (29.8) | 5 (29.4) | 12 (70.6) | |||
| Urethral catheterization | Yes | 2 (3.5) | 2 (100) | 0 (0.0) | 0.188 b | |
| No | 55 (96.5) | 23 (41.8) | 32 (58.2) | |||
| Blood sugar measurement | Yes | 1 (1.8) | 0 (0.0) | 1 (100) | 0.439 b | |
| No | 56 (98.2) | 24 (42.9) | 32 (57.1) | |||
| Nasotracheal airway | Yes | 1 (1.8) | 0 (0.0) | 1 (100) | 0.000 b | |
| No | 56 (98.2) | 25 (44.6) | 31 (55.4) | |||
| Central parenteral nutrition | Yes | 1 (1.8) | 0 (0.0) | 1 (100) | 0.000 b | |
| No | 56 (98.2) | 25 (44.6) | 31 (55.4) | |||
| Inhalation | Yes | 5 (8.8) | 4 (80.0) | 1 (20.0) | 0.157 b | |
| No | 52 (91.2) | 21 (40.4) | 31 (59.6) | |||
| Mechanically assisted coughing | Yes | 1 (1.8) | 0 (0.0) | 1 (100) | 1.00 b | |
| No | 56 (98.2) | 25 (44.6) | 31 (55.4) | |||
| Background of Family Caregivers | ||||||
| Age | 20s | 3 (5.3) | 1 (33.3) | 2 (66.7) | 1.00 b | |
| 30s and older | 54 (94.7) | 24 (44.4) | 30 (52.6) | |||
| Sex | Men | 1 (1.8) | 0 (0.0) | 1 (100) | 1.00 b | |
| Women | 56 (98.2) | 25 (44.6) | 31 (55.4) | |||
| Employment | Yes | 20 (35.1) | 5 (25.0) | 15 (75.0) | 0.035 a | |
| No | 37 (64.9) | 20 (54.1) | 17 (45.9) | |||
| Regular employment | Yes | 9 (15.8) | 2 (22.2) | 7 (77.8) | ||
| Non-regular employment | Yes | 11 (19.3) | 3 (27.3) | 8 (72.7) | ||
| Previous experience with evacuation from a disaster | Yes | 5 (8.8) | 4 (80.0) | 1 (20.0) | 0.157 b | |
| No | 52 (91.2) | 21 (40.4) | 31 (59.6) | |||
| Preparation for a disaster | ||||||
| Prepared for a disaster | Yes | 14 (24.6) | 4 (28.6) | 10 (71.4) | 0.184 a | |
| No | 43 (75.4) | 21 (48.8) | 22 (51.2) | |||
| Prepared children’s clothes | Yes | 11 (19.3) | 4 (36.4) | 7 (63.6) | 0.739 b | |
| No | 46 (80.7) | 21 (45.7) | 25 (54.3) | |||
| Prepared food for the Patient with Home Medical Care (PHMC) | Yes | 18 (31.6) | 7 (38.9) | 11 (61.1) | 0.607 a | |
| No | 39 (68.4) | 18 (46.2) | 21 (53.8) | |||
| Equipped with medical hygiene materials for the PHMC | Yes | 16 (28.1) | 6 (37.5) | 10 (62.5) | 0.546 a | |
| No | 41 (71.9) | 19 (46.3) | 22 (53.7) | |||
| Prepared children’s medicine | Yes | 7 (12.3) | 4 (57.1) | 3 (42.9) | 0.687 b | |
| No | 50 (87.7) | 21 (42.0) | 29 (58.0) | |||
| Secured a power source for continued use of medical devices during power outages | Yes | 35 (61.4) | 12 (34.3) | 23 (65.7) | 0.066 a | |
| No | 22 (38.6) | 13 (59.1) | 9 (40.9) | |||
| Destination, preparation and intention of evacuation | ||||||
| Secured shelter other than public shelter | Yes | 20 (35.1) | 5 (25.0) | 15 (75.0) | 0.035 a | |
| No | 37 (64.9) | 20 (54.1) | 17 (45.9) | |||
| Will evacuate to welfare shelter | Yes | 47 (82.5) | 23 (48.9) | 24 (51.1) | 0.160 b | |
| No | 10 (17.5) | 2 (20.0) | 8 (80.0) | |||
| Have simulated and prepared for life during evacuation | Yes | 9 (15.8) | 6 (66.7) | 3 (33.3) | 0.161 b | |
| No | 48 (84.2) | 19 (39.6) | 29 (60.4) | |||
| Have asked others to help our evacuation | Yes | 19 (33.3) | 6 (31.6) | 13 (68.4) | 0.186 a | |
| No | 38 (66.7) | 19 (50.0) | 19 (50.0) | |||
| Registered to the local government emergency evacuation assistance registry | Yes | 25 (43.9) | 11 (44.0) | 14 (56.0) | 0.985 a | |
| No | 32 (56.1) | 14 (43.8) | 18 (56.3) | |||
| Knowledge of public shelter and decentralized evacuation | ||||||
| I know where the public shelter is | Yes | 51 (89.5) | 20 (39.2) | 31 (60.8) | 0.077 b | |
| No | 6 (10.5) | 5 (83.3) | 1 (16.7) | |||
| I know where the welfare shelter is | Yes | 11 (19.3) | 2 (18.2) | 9 (81.8) | 0.090 b | |
| No | 46 (80.7) | 23 (50.0) | 23 (50.0) | |||
| I know where the welfare shelter is | Yes | 2 (3.5) | 0 (0.0) | 2 (100) | 0.499 b | |
| No | 55 (96.5) | 25 (45.5) | 30 (54.5) | |||
| I know that the government is calling for decentralized evacuation to prevent COVID-19 transmission | Yes | 21 (36.8) | 9 (42.9) | 12 (57.1) | 0.907 a | |
| No | 36 (63.2) | 16 (44.4) | 20 (55.6) | |||
| Disaster risk in the dwelling | ||||||
| I know the risk of river flooding in the area of my dwelling | Yes | 46 (80.7) | 19 (41.3) | 27 (58.7) | 0.508 b | |
| No | 11 (19.3) | 6 (54.5) | 5 (45.5) | |||
| I know the risk of landslides in the area of my dwelling | Yes | 42 (73.7) | 18 (42.9) | 24 (57.1) | 0.799 a | |
| No | 15 (26.3) | 7 (46.7) | 8 (53.3) | |||
| I know the risk of inundation by tsunami in the area of my dwelling | Yes | 42 (73.7) | 17 (40.5) | 25 (59.5) | 0.389 a | |
| No | 15 (26.3) | 8 (53.3) | 7 (46.7) | |||
| Item | Category | OR | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||
| Age | Less than 15 years/15 years or older | 1.27 | 0.26 | 6.29 | 0.774 |
| Parents’ Evacuation Experience | Yes/No | 11.51 | 0.77 | 171.78 | 0.077 |
| Use of a home ventilator | No/Yes | 3.99 | 1.13 | 14.03 | 0.031 |
| Ensure evacuation destinations other than designated evacuation centers | No/Yes | 7.29 | 1.62 | 32.88 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, Y.; Nakai, H.; Koga, Y.; Hasegawa, T.; Miyagi, Y. Disaster Evacuation for Home-Based Patients with Special Healthcare Needs: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 15356. https://doi.org/10.3390/ijerph192215356
Matsumoto Y, Nakai H, Koga Y, Hasegawa T, Miyagi Y. Disaster Evacuation for Home-Based Patients with Special Healthcare Needs: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(22):15356. https://doi.org/10.3390/ijerph192215356
Chicago/Turabian StyleMatsumoto, Yukari, Hisao Nakai, Yumi Koga, Tamayo Hasegawa, and Yumiko Miyagi. 2022. "Disaster Evacuation for Home-Based Patients with Special Healthcare Needs: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 22: 15356. https://doi.org/10.3390/ijerph192215356
APA StyleMatsumoto, Y., Nakai, H., Koga, Y., Hasegawa, T., & Miyagi, Y. (2022). Disaster Evacuation for Home-Based Patients with Special Healthcare Needs: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(22), 15356. https://doi.org/10.3390/ijerph192215356