
Understanding Physicians’ Motivation to Provide Healthcare Service Online in the Digital Age



Abstract
1. Introduction
2. Literature Review and Hypothesis Development
2.1. Physicians’ Participation in Online Healthcare Service
2.2. Theoretical Foundations
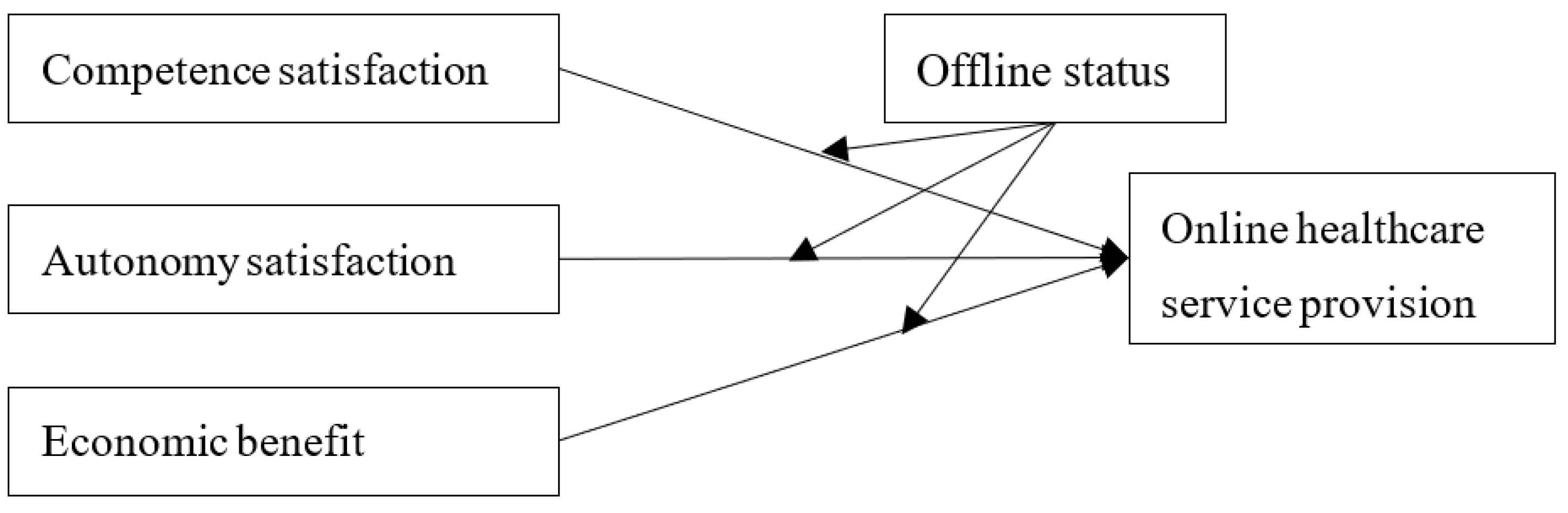
2.3. The Motivation of Healthcare Service Provision
2.4. The Moderating Effects of Offline Status
3. Methodology
3.1. Data Collection
3.2. Empirical Model
4. Results
4.1. Correlations
4.2. Empirical Results
4.3. Robustness Check
5. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
|---|---|---|---|---|---|---|
| Constant | −2.525 ** (0.619) | −1.120 (0.745) | 0.965 (0.662) | −1.246 (0.775) | 0.539 (0.698) | 0.500 (0.691) |
| Hospital level 1 | −0.569 (0.961) | −2.169 ** (0.701) | −0.337 (0.701) | −2.143 ** (0.774) | −0.245 (0.689) | −1.284 (0.716) |
| Hospital level 2 | 0.263 (0.578) | −0.267 (0.641) | 0.527 (0.479) | −0.378 (0.714) | 0.622 (0.494) | 0.065 (0.571) |
| Hospital level 3 | 1.085 * (0.521) | 0.162 (0.601) | 0.979 * (0.400) | −0.104 (0.676) | 0.888 * (0.406) | 0.095 (0.521) |
| ln(Visits + 1) | 0.295 ** (0.028) | 0.126 ** (0.039) | −0.159 * (0.062) | 0.109 ** (0.042) | −0.211 ** (0.059) | −0.160 ** (0.049) |
| Competence | 0.958 ** (0.037) | 1.394 ** (0.159) | 1.312 ** (1.196) | |||
| Autonomy | 0.275 ** (0.051) | 0.094 (0.183) | −0.176 (0.204) | |||
| Economic | 0.681 ** (0.100) | 0.858 ** (0.165) | 0.614 ** (0.187) | |||
| Status | 0.181 (0.115) | 0.324 (0.120) | 0.221 * (1.110) | |||
| Competence * Status | −0.133 ** (0.046) | −0.148 ** (0.054) | ||||
| Autonomy * Status | 0.053 (0.053) | 0.129 * (0.062) | ||||
| Economic * Status | −0.045 (0.037) | −0.048 (0.050) | ||||
| Log pseudolikelihood | −6103.155 | −5728.112 | −5943.303 | −5713.740 | −5932.858 | −5632.623 |
| Wald chi2 | 149.08 | 903.84 | 161.97 | 1031.07 | 177.92 | 1018.36 |
| Prob > chi2 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Pseudo R2 | 0.021 | 0.081 | 0.046 | 0.083 | 0.048 | 0.096 |
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
|---|---|---|---|---|---|---|
| Constant | −2.281 ** (0.548) | −1.094 (0.585) | 1.896 ** (0.632) | −1.379 * (0.576) | 2.275 ** (0.660) | 1.088 (0.586) |
| Hospital level 1 | 0.502 (0.888) | −0.781 (0.626) | 1.294 (0.682) | −0.799 (0.633) | 1.204 (0.676) | 0.030 (0.703) |
| Hospital level 2 | 0.934 (0.642) | 0.596 (0.778) | 1.333 * (0.524) | 0.580 (0.764) | 1.282 * (0.544) | 0.781 (0.636) |
| Hospital level 3 | 1.109 * (0.440) | 0.480 (0.492) | 1.203 ** (0.318) | 0.453 (0.481) | 1.167 ** (0.342) | 0.609 (0.374) |
| ln(Visits + 1) | 0.268 ** (0.026) | 0.100 ** (0.030) | −0.299 ** (0.062) | 0.095 ** (0.035) | −0.292 ** (0.065) | −0.217 ** (0.047) |
| Competence | 0.944 ** (0.035) | 1.226 ** (0.154) | 1.096 ** (0.191) | |||
| Autonomy | 0.239 ** (0.042) | 0.326 * (0.151) | 0.529 * (0.209) | |||
| Economic | 0.834 ** (0.089) | 0.638 ** (0.174) | 0.290 (0.191) | |||
| Status | 0.116 (0.101) | −0.135 (0.121) | 0.044 (0.096) | |||
| Competence * Status | −0.089 * (0.044) | −0.089 (0.053) | ||||
| Autonomy * Status | −0.026 (0.042) | −0.112 * (0.057) | ||||
| Economic * Status | 0.060 (0041) | 0.079 (0.054) | ||||
| Log pseudolikelihood | −6546.115 | −6159.308 | −6329.268 | −6156.702 | −6327.057 | −6047.847 |
| Wald chi2 | 110.26 | 1030.53 | 171.18 | 1366.31 | 180.68 | 1220.69 |
| Prob > chi2 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Pseudo R2 | 0.015 | 0.074 | 0.048 | 0.074 | 0.048 | 0.090 |
References
- Guo, S.; Guo, X.; Fang, Y.; Vogel, D. How doctors gain social and economic returns in online health-care communities: A professional capital perspective. J. Manag. Inf. Syst. 2017, 34, 487–519. [Google Scholar] [CrossRef]
- Yang, H.; Ju, X. Investigating the influences of motivators on physician contribution behaviors in online health community: Offline status as a moderator. In Proceedings of the 20th Pacific Asia Conference on Information Systems, Chiayi, Taiwan, 27 June–1 July 2016. [Google Scholar]
- Cao, X.; Wang, D. The role of online communities in reducing urban–rural health disparities in China. J. Assoc. Inf. Sci. Technol. 2018, 69, 890–899. [Google Scholar] [CrossRef]
- Goh, J.M.; Gao, G.; Agarwal, R. The creation of social value: Can an online health community reduce rural-urban health disparities? MIS Q. 2016, 40, 247–263. [Google Scholar] [CrossRef]
- Hwang, E.H.; Guo, X.; Tan, Y.; Dang, Y. Delivering Healthcare Through Teleconsultations: Implications for Offline Healthcare Disparity. Inf. Syst. Res. 2022, 33, 515–539. [Google Scholar] [CrossRef]
- Liu, Q.B.; Liu, X.; Guo, X. The effects of participating in a physician-driven online health community in managing chronic disease: Evidence from two natural experiments. MIS Q. 2020, 44, 391–419. [Google Scholar] [CrossRef]
- Farnan, J.M.; Sulmasy, L.S.; Worster, B.K.; Chaudhry, H.J.; Rhyne, J.A.; Arora, V.M. Online Medical Professionalism: Patient and public relationships: Policy statement from the American College of Physicians and the Federation of State Medical Boards. Ann. Intern. Med. 2013, 158, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Cao, B.; Yang, G.; Luo, N.; Chao, N. Turn to the Internet first? Using online medical behavioral data to forecast COVID-19 epidemic trend. Inf. Process. Manag. 2021, 58, 102486. [Google Scholar] [CrossRef]
- The State Information Center of China. The Annual Report on the Development of Sharing Economy in China; The State Information Center of China: Beijing, China, 2022. [Google Scholar]
- Green, E.P. Payment systems in the healthcare industry: An experimental study of physician incentives. J. Econ. Behav. Organ. 2014, 106, 367–378. [Google Scholar] [CrossRef]
- Yang, H.; Guo, X.; Wu, T.; Ju, X. Exploring the effects of patient-generated and system-generated information on patients’ online search, evaluation and decision. Electron. Commer. Res. Appl. 2015, 14, 192–203. [Google Scholar] [CrossRef]
- Wang, J.N.; Chiu, Y.L.; Yu, H.; Hsu, Y.T. Understanding a nonlinear causal relationship between rewards and physicians’ contributions in online health care communities: Longitudinal study. J. Med. Internet Res. 2017, 19, e427. [Google Scholar] [CrossRef]
- Wang, L.; Yan, L.L.; Zhou, T.; Guo, X.; Heim, G.R. Understanding Physicians’ Online-Offline Behavior Dynamics: An Empirical Study. Inf. Syst. Res. 2020, 32, 537–555. [Google Scholar] [CrossRef]
- Wennberg, J.E. Time to tackle unwarranted variations in practice. BMJ Br. Med. J. 2011, 342, 687–690. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, N.; Pick, D.; Kenning, P. To share or not to share? Explaining willingness to share in the context of social distance. J. Consum. Behav. 2018, 17, 366–378. [Google Scholar] [CrossRef]
- Xu, D.; Zhan, J.; Cheng, T.; Fu, H.; Yip, W. Understanding online dual practice of public hospital doctors in China: A mixed-methods study. Health Policy Plan. 2022, 37, 440–451. [Google Scholar] [CrossRef]
- Hsu, Y.-T.; Duan, R.; Chiu, Y.-L.; Wang, J.-N. Understanding the Inequality of Web Traffic and Engagement in Online Healthcare Communities. Front. Public Health 2022, 10, 917522. [Google Scholar] [CrossRef]
- Huang, E. Use and gratification in e-consumers. Internet Res. 2008, 18, 405–426. [Google Scholar] [CrossRef]
- Yaoyuneyong, G.; Foster, J.; Flynn, L.R. Factors impacting the efficacy of augmented reality virtual dressing room technology as a tool for online visual merchandising. J. Glob. Fash. Mark. 2014, 5, 283–296. [Google Scholar] [CrossRef]
- Upreti, A.; Musalay, P. (Eds.) Fear of Missing Out, Mobile Phone Dependency and Entrapment in Undergarduate Students; Springer: Singapore, 2018. [Google Scholar]
- Hsu, M.-H.; Chang, C.-M.; Lin, H.-C.; Lin, Y.-W. Determinants of continued use of social media: The perspectives of uses and gratifications theory and perceived interactivity. Inf. Res. 2015, 20. [Google Scholar]
- Wu, H.; Deng, Z.; Wang, B.; Wang, H. How online health community participation affects physicians’ performance in hospitals: Empirical evidence from China. Inf. Manag. 2021, 58, 103443. [Google Scholar] [CrossRef]
- Sampat, B.; Krishnamoorthy, B. Motivations for social network site (SNS) gaming: A uses and gratification & flow perspective. J. Int. Technol. Inf. Manag. 2016, 25, 75–98. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory. In Handbook of Theories of Social Psychology; Van Lange, P.A.M., Kruglanski, A.W., Higgins, E.T., Eds.; Sage Publications: Los Angeles, CA, USA, 2012; Volume 1, pp. 416–437. [Google Scholar]
- Vansteenkiste, M.; Lens, W.; Deci, E.L. Intrinsic versus extrinsic goal contents in self-determination theory: Another look at the quality of academic motivation. Educ. Psychol. 2006, 41, 19–31. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Gunz, A. Psychological needs as basic motives, not just experiential requirements. J. Personal. 2009, 77, 1467–1492. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, V.; Nerur, S.; Teng, J.T.C. (Eds.) Interactivity Redefined for the Social Web; Idea Group Inc. (IGI): Calgary, AB, USA, 2009. [Google Scholar]
- Zhang, X.; Liu, S.; Deng, Z.H.; Chen, X. Knowledge sharing motivations in online health communities: A comparative study of health professionals and normal users. Comput. Hum. Behav. 2017, 75, 797–810. [Google Scholar] [CrossRef]
- Liu, X.; Guo, X.; Wu, H.; Wu, T. The impact of individual and organizational reputation on physicians’ appointments online. Int. J. Electron. Commer. 2016, 20, 551–577. [Google Scholar] [CrossRef]
- Wu, H.; Lu, N. How your colleagues’ reputation impact your patients’ odds of posting experiences: Evidence from an online health community. Electron. Commer. Res. Appl. 2016, 16, 7–17. [Google Scholar] [CrossRef]
- Huang, N.; Yan, Z.; Yin, H. Effects of Online–Offline Service Integration on e-Healthcare Providers: A Quasi-Natural Experiment. Prod. Oper. Manag. 2021, 30, 2359–2378. [Google Scholar] [CrossRef]
- Li, Y.; Ma, X.; Song, J.; Yang, Y.; Ju, X. Exploring the effects of online rating and the activeness of physicians on the number of patients in an online health community. Telemed. E-Health 2019, 25, 1090–1098. [Google Scholar] [CrossRef]
- Hsu, Y.-T.; Chiu, Y.-L.; Wang, J.-N.; Liu, H.-C. Impacts of physician promotion on the online healthcare community: Using a difference-in-difference approac. Digit. Health 2022, 8, 20552076221106319. [Google Scholar] [CrossRef]
- Liu, F.; Guo, X.; Ju, X.; Han, X. Exploring the effects of different incentives on doctors’ contribution behaviors in online health communities. In International Conference on Smart Health; Springer: Cham, Switzerland, 2018; pp. 90–95. [Google Scholar]
- Sun, W.; Dang, Y.; Guo, X. The Impact of a New App Channel on Physicians’ Performance: Evidence From Online Healthcare Natural Experiment. In Proceedings of the 52nd Hawaii International Conference on System Sciences, Grand Wailea, HI, USA, 8 January–11 January 2019. [Google Scholar]
- Shah, A.M.; Ali, M.; Qayyum, A.; Begum, A.; Han, H.; Ariza-Montes, A.; Araya-Castillo, L. Exploring the Impact of Linguistic Signals Transmission on Patients’ Health Consultation Choice: Web Mining of Online Reviews. Int. J. Environ. Res. Public Health 2021, 18, 9969. [Google Scholar] [CrossRef]
- Yang, H.; Guo, X.; Wu, T. Exploring the influence of the online physician service delivery process on patient satisfaction. Decis. Support Syst. 2015, 78, 113–121. [Google Scholar] [CrossRef]
- Luo, P.; Chen, K.; Wu, C.; Li, Y. Exploring the Social Influence of Multichannel Access in an Online Health Community. J. Assoc. Inf. Sci. Technol. 2018, 69, 98–109. [Google Scholar] [CrossRef]
- Zhang, T.; Yan, X.; Wang, W.Y.C.; Chen, Q. Unveiling physicians’ personal branding strategies in online healthcare service platforms. Technol. Forecast. Soc. Chang. 2021, 171, 120964. [Google Scholar] [CrossRef]
- Yang, H.; Du, H.S.; He, W.; Qiao, H. Understanding the motivators affecting doctors’ contributions in online healthcare communities: Professional status as a moderator. Behav. Inf. Technol. 2021, 40, 146–160. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, F.; Xu, T.; Li, Y. What motivates physicians to share free health information on online health platforms? Inf. Process. Manag. 2020, 57, 102166. [Google Scholar] [CrossRef]
- Chuang, D. An empirical analysis of hospital hierarchical management system in china. Soc. Sci. Front 2018, 4, 84–94. [Google Scholar]
- Jin, J.; Yan, X.; Li, Y.; Li, Y. How users adopt healthcare information: An empirical study of an online Q&A community. Int. J. Med. Inform. 2016, 86, 91–103. [Google Scholar]
- Gardner, W.; Mulvey, E.P.; Shaw, E.C. Regression analyses of counts and rates: Poisson, overdispersed poisson, and negative binomial models. Psychol. Bull. 1995, 118, 392–404. [Google Scholar] [CrossRef]

| Variable | Description | Proxy | |
|---|---|---|---|
| Dependent variable | Online healthcare service provision | Total number of times of a physician providing online healthcare service | The total number of patients on the platform |
| Independent variables | Competence satisfaction | The level of a physician’s patients’ satisfaction with the physician’s online healthcare service | A physician’s online rating |
| Autonomy satisfaction | The level of a physician’s voluntary contribution to the platform other than providing online healthcare service | The total number of articles published on the platform | |
| Economic benefit | The monetary returns a physician obtained online consultation | The total number of gifts received from patients | |
| Moderator | Offline status | A physician’s offline social standing, which reflects his/her professional ranking and medical capacities | A physician’s offline medical title |
| Control variables | Hospital level | The level of the hospital where a physician registered with and working for offline | One of the three levels of hospital |
| Visits | The level of attention from potential patients on the platform | The total number of visits of a physician’s homepage on the platform | |
| Variable | Min | Max | Mean | Std. Dev. |
|---|---|---|---|---|
| Hospital level 1 | 0 | 1 | 0.004 | 0.064 |
| Hospital level 2 | 0 | 1 | 0.058 | 0.233 |
| Hospital level 3 | 0 | 1 | 0.921 | 0.270 |
| Visits | 17 | 5.32 × 107 | 448,430.200 | 1,625,244 |
| Consultation service | 0 | 389 | 8.137 | 26.282 |
| Competence satisfaction | 0 | 5 | 0.402 | 0.922 |
| Autonomy satisfaction | 0 | 1351 | 11.733 | 57.597 |
| Economic benefit | 0 | 4145 | 43.411 | 165.841 |
| Offline status | 0 | 4 | 3.038 | 0.912 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Hospital level 1 | 1 | |||||||
| Hospital level 2 | −0.016 | 1 | ||||||
| Hospital level 3 | −0.218 ** | −0.842 ** | 1 | |||||
| ln(Visits + 1) | −0.006 | −0.039 * | 0.026 | 1 | ||||
| Competence satisfaction | −0.009 | −0.073 ** | 0.084 ** | 0.193 ** | 1 | |||
| Autonomy satisfaction | 0.028 | 0.002 | −0.019 | 0.257 ** | 0.109 ** | 1 | ||
| Economic benefit | −0.013 | −0.053 ** | 0.048 * | 0.634 ** | 0.368 ** | 0.143 ** | 1 | |
| Offline status | −0.054 ** | −0.127 ** | 0.125 ** | 0.136 ** | 0.034 | 0.073 ** | 0.109 ** | 1 |
| Hypothesis | Results | Tested in |
|---|---|---|
| Hypothesis 1: Physicians who have a higher level of competence satisfaction has higher totals of service provision on healthcare service platforms. | Supported | Model 2 |
| Hypothesis 2: Physicians who have a higher level of autonomy satisfaction has higher totals of service provision on healthcare service platforms. | Supported | Model 2 |
| Hypothesis 3: Physicians who wish to gain higher economic benefits has higher totals of service provision on healthcare service platforms. | Supported | Model 3 |
| Hypothesis 4(1): A physician’s offline status negatively moderates the relationship between competence satisfaction and service provision. | Supported | Model 4 |
| Hypothesis 4(2): A physician’s offline status negatively moderates the relationship between autonomy satisfaction and service provision. | Not supported | Model 4 |
| Hypothesis 4(3): A physician’s offline status negatively moderates the relationship between economic benefit and service provision. | Not supported | Model 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, T.; Chen, Q.; Wang, W.Y.C.; Wei, Y. Understanding Physicians’ Motivation to Provide Healthcare Service Online in the Digital Age. Int. J. Environ. Res. Public Health 2022, 19, 15135. https://doi.org/10.3390/ijerph192215135
Zhang T, Chen Q, Wang WYC, Wei Y. Understanding Physicians’ Motivation to Provide Healthcare Service Online in the Digital Age. International Journal of Environmental Research and Public Health. 2022; 19(22):15135. https://doi.org/10.3390/ijerph192215135
Chicago/Turabian StyleZhang, Tingting, Qin Chen, William Yu Chung Wang, and Yuhan Wei. 2022. "Understanding Physicians’ Motivation to Provide Healthcare Service Online in the Digital Age" International Journal of Environmental Research and Public Health 19, no. 22: 15135. https://doi.org/10.3390/ijerph192215135
APA StyleZhang, T., Chen, Q., Wang, W. Y. C., & Wei, Y. (2022). Understanding Physicians’ Motivation to Provide Healthcare Service Online in the Digital Age. International Journal of Environmental Research and Public Health, 19(22), 15135. https://doi.org/10.3390/ijerph192215135