
A Cross-Sectional Analysis of Paternal Intimacy Problems, Stress Levels, and Satisfaction from Families with Children Born with Mucoviscidosis

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Instruments
2.3. Statistical Analysis
3. Results
3.1. Patients’ Background
3.2. Unstandardized Survey Questions
3.3. Analysis of Standardized Questionnaires
4. Discussion
4.1. Literature Analysis
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanders, D.B.; Fink, A.K. Background and Epidemiology. Pediatr. Clin. N. Am. 2016, 63, 567–584. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Shen, Y.; Zheng, J. A review of cystic fibrosis: Basic and clinical aspects. Anim. Models Exp. Med. 2021, 4, 220–232. [Google Scholar] [CrossRef] [PubMed]
- McBennett, K.A.; Davis, P.B.; Konstan, M.W. Increasing life expectancy in cystic fibrosis: Advances and challenges. Pediatr. Pulmonol. 2022, 57 (Suppl. S1), S5–S12. [Google Scholar] [CrossRef] [PubMed]
- Keogh, R.H.; Szczesniak, R.; Taylor-Robinson, D.; Bilton, D. Up-to-date and projected estimates of survival for people with cystic fibrosis using baseline characteristics: A longitudinal study using UK patient registry data. J. Cyst. Fibros. 2018, 17, 218–227. [Google Scholar] [CrossRef]
- Durda-Masny, M.; Goździk-Spychalska, J.; John, A.; Czaiński, W.; Stróżewska, W.; Pawłowska, N.; Wlizło, J.; Batura-Gabryel, H.; Szwed, A. The determinants of survival among adults with cystic fibrosis-a cohort study. J. Physiol. Anthropol. 2021, 40, 19. [Google Scholar] [CrossRef]
- Yamaoka, Y.; Tamiya, N.; Moriyama, Y.; Sandoval Garrido, F.A.; Sumazaki, R.; Noguchi, H. Mental Health of Parents as Caregivers of Children with Disabilities: Based on Japanese Nationwide Survey. PLoS ONE. 2015, 10, e0145200. [Google Scholar] [CrossRef]
- Gurtovenko, K.; Fladeboe, K.M.; Galtieri, L.R.; King, K.; Friedman, D.; Compas, B.; Breiger, D.; Lengua, L.; Keim, M.; Kawamura, J.; et al. Stress and psychological adjustment in caregivers of children with cancer. Health Psychol. 2021, 40, 295–304. [Google Scholar] [CrossRef]
- Continisio, G.I.; Serra, N.; Guillari, A.; Civitella, M.T.; Sepe, A.; Simeone, S.; Gargiulo, G.; Toscano, S.; Esposito, M.R.; Raia, V.; et al. An investigation on parenting stress of children with cystic fibrosis. Ital. J. Pediatr. 2020, 46, 33. [Google Scholar] [CrossRef]
- Deffaa, M.; Weis, M.; Trommsdorff, G. The Role of Maternal Parenting for Children’s Behavior Regulation in Environments of Risk. Front. Psychol. 2020, 11, 2159. [Google Scholar] [CrossRef]
- Sheidow, A.J.; Henry, D.B.; Tolan, P.H.; Strachan, M.K. The Role of Stress Exposure and Family Functioning in Internalizing Outcomes of Urban Families. J. Child Fam. Stud. 2014, 23, 1351–1365. [Google Scholar] [CrossRef]
- Lee, D.; McLanahan, S. Family Structure Transitions and Child Development: Instability, Selection, and Population Heterogeneity. Am. Sociol. Rev. 2015, 80, 738–763. [Google Scholar] [CrossRef] [PubMed]
- Jessee, V.; Adamsons, K. Father Involvement and Father-Child Relationship Quality: An Intergenerational Perspective. Parent. Sci. Pract. 2018, 18, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Dong, Q.; Chen, H.; Yang, S. Mother’s Parenting Stress and Marital Satisfaction During the Parenting Period: Examining the Role of Depression, Solitude, and Time Alone. Front. Psychol. 2022, 13, 847419. [Google Scholar] [CrossRef] [PubMed]
- Farrell, P.M. The prevalence of cystic fibrosis in the European Union. J. Cyst. Fibros. 2008, 7, 450–453. [Google Scholar] [CrossRef]
- Endler, N.S.; Parker, J.D. State and trait anxiety, depression and coping styles. Aust. J. Psychol. 1990, 42, 207–220. [Google Scholar] [CrossRef]
- Spratt, E.G.; Friedenberg, S.L.; Swenson, C.C.; Larosa, A.; De Bellis, M.D.; Macias, M.M.; Summer, A.P.; Hulsey, T.C.; Runyan, D.K.; Brady, K.T. The Effects of Early Neglect on Cognitive, Language, and Behavioral Functioning in Childhood. Psychology 2012, 3, 175–182. [Google Scholar] [CrossRef]
- LoPiccolo, J.; Steger, J.C. The sexual interaction inventory: A new instrument for assessment of sexual dysfunction. Arch. Sex. Behav. 1974, 3, 585–595. [Google Scholar] [CrossRef]
- Catania, J.A. Dyadic sexual communication scale. In Handbook of Sexuality-Related Measures; Routledge: London, UK, 1998; pp. 129–131. [Google Scholar] [CrossRef]
- van den Broucke, S.; Vandereycken, W.; Vertommen, H. Marital intimacy: Conceptualization and assessment. Clin. Psychol. Rev. 1995, 15, 217–233. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0, Released 2020; IBM Corp: Armonk, NY, USA, 2020.
- Microsoft Corporation. Microsoft Excel. 2018. Available online: https://office.microsoft.com/excel (accessed on 30 August 2022).
- Raju, S.V.; Jackson, P.L.; Courville, C.A.; McNicholas, C.M.; Sloane, P.A.; Sabbatini, G.; Tidwell, S.; Tang, L.P.; Liu, B.; Fortenberry, J.A.; et al. Cigarette smoke induces systemic defects in cystic fibrosis transmembrane conductance regulator function. Am. J. Respir. Crit. Care Med. 2013, 188, 1321–1330. [Google Scholar] [CrossRef]
- Darling, C.A.; Senatore, N.; Strachan, J. Fathers of children with disabilities: Stress and life satisfaction. Stress Health 2012, 28, 269–278. [Google Scholar] [CrossRef]
- Siracusano, M.; Riccioni, A.; Gialloreti, L.E.; Segatori, E.; Arturi, L.; Vasta, M.; Porfirio, M.C.; Terribili, M.; Galasso, C.; Mazzone, L. Parental Stress and Disability in Offspring: A Snapshot during the COVID-19 Pandemic. Brain Sci. 2021, 11, 1040. [Google Scholar] [CrossRef] [PubMed]
- Sarimski, K. Erlebte Belastung von Müttern von Kindern mit Down-Syndrom im Vorschulalter [Parenting Stress in Mothers of Children with Down Syndrome in Preschool Age]. Prax. Kinderpsychol. Kinderpsychiatr. 2017, 66, 672–686. (In German) [Google Scholar] [CrossRef] [PubMed]
- Kiernan, J.; Mitchell, D.; Stansfield, J.; Taylor, C. Mothers’ perspectives on the lived experience of children with intellectual disability and challenging behaviour. J. Intellect. Disabil. 2019, 23, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Duchovic, C.A.; Gerkensmeyer, J.E.; Wu, J. Factors associated with parental distress. J. Child Adolesc. Psychiatr. Nurs. 2009, 22, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Saloviita, T.; Itälinna, M.; Leinonen, E. Explaining the parental stress of fathers and mothers caring for a child with intellectual disability: A Double ABCX Model. J. Intellect. Disabil. Res. 2003, 47, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Fucà, E.; Costanzo, F.; Ursumando, L.; Vicari, S. Parenting Stress in Mothers of Children and Adolescents with Down Syndrome. J. Clin. Med. 2022, 11, 1188. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.P.; Lee, S.J. Mothers’ and Fathers’ Parenting Stress, Responsiveness, and Child Wellbeing Among Low-Income Families. Child Youth Serv. Rev. 2020, 116, 105218. [Google Scholar] [CrossRef]
- Vernhet, C.; Dellapiazza, F.; Blanc, N.; Cousson-Gélie, F.; Miot, S.; Roeyers, H.; Baghdadli, A. Coping strategies of parents of children with autism spectrum disorder: A systematic review. Eur. Child Adolesc. Psychiatry 2019, 28, 747–758. [Google Scholar] [CrossRef]
- Shokoohi-Yekta, M.; Ghobary-Bonab, B.; Malayeri, S.A.; Zamani, N.; Pourkarimi, J. The relationship between anger and coping strategies of mothers of children with special needs. Procedia-Soc. Behav. Sci. 2015, 205, 140–144. [Google Scholar] [CrossRef][Green Version]
- Bujnowska, A.M.; Rodríguez, C.; García, T.; Areces, D.; Marsh, N.V. Coping with stress in parents of children with developmental disabilities. Int. J. Clin. Health Psychol. 2021, 21, 100254. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Cases (n = 107) | Controls (n = 124) | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 35.9 ± 9.4 | 34.6 ± 9.0 | 0.284 |
| Age range (years) | 0.620 | ||
| <25 | 12 (11.2%) | 17 (13.7%) | |
| 25–35 | 40 (37.4%) | 51 (41.4%) | |
| >35 | 55 (51.4%) | 56 (45.2%) | |
| Area of Residence (urban) | 66 (61.7%) | 63 (50.8%) | 0.096 |
| Relationship Status | 0.569 | ||
| Married/Concubinage | 98 (91.6%) | 116 (93.5%) | |
| Single/Divorced/Widowed | 9 (8.4%) | 8 (6.5%) | |
| Income (medium and high) | 71 (66.4%) | 90 (72.6%) | 0.304 |
| Education (university degree) | 39 (36.4%) | 47 (37.9%) | 0.819 |
| Religion | 0.737 | ||
| Orthodox | 86 (80.4%) | 98 (79.0%) | |
| Catholic | 6 (5.6%) | 5 (4.0%) | |
| Protestant | 7 (6.5%) | 7 (5.6%) | |
| Not specified | 8 (7.5%) | 14 (11.3%) | |
| Practicing religion (yes) | 53 (49.5%) | 47 (37.9%) | 0.075 |
| Occupation (employed or self-employed) | 72 (67.3%) | 95 (76.6%) | 0.114 |
| Sexual activity | 0.021 | ||
| Weekly or more | 24 (22.4%) | 37 (29.8%) | |
| 1–3 times per month | 43 (40.2%) | 61 (49.2%) | |
| Less than 1–3 times per month | 40 (37.4%) | 26 (21.0%) | |
| Substance use behavior | |||
| Frequent alcohol consumption | 9 (8.4%) | 5 (4.0%) | 0.164 |
| Frequent smoker | 37 (34.6%) | 28 (22.6%) | 0.043 |
| Drug user | 3 (2.8%) | 3 (2.4%) | 0.854 |
| Variables | Cases (n = 107) | Controls (n = 124) | p-Value |
|---|---|---|---|
| Number of children | <0.001 | ||
| 1 | 95 (88.8%) | 76 (61.3%) | |
| ≥2 | 12 (11.2%) | 48 (38.7%) | |
| Age of children | 0.019 | ||
| Infancy | 59 (55.1%) | 61 (49.2%) | |
| Childhood | 37 (34.6%) | 33 (26.6%) | |
| Adolescence | 11 (10.3%) | 30 (24.2%) | |
| Psychiatric disease (yes) | 11 (10.3%) | 7 (5.6%) | 0.190 |
| Marital distress (yes) | 16 (15.0%) | 8 (6.5%) | 0.034 |
| Attending psychotherapy (yes) | 5 (4.7%) | 1 (0.8%) | 0.065 |
| Attending couple therapy (yes) | 7 (6.5%) | 3 (2.4%) | 0.124 |
| Taking psychiatric medication (yes) | 8 (7.5%) | 2 (1.6%) | 0.028 |
| Comorbid conditions | 23 (18.7%) | 29 (23.4%) | 0.384 |
| Reproductive problems | |||
| Erectile dysfunction | 13 (12.1%) | 10 (8.1%) | 0.301 |
| Ejaculation problems | 9 (8.4%) | 11 (8.9%) | 0.901 |
| Inhibited sexual desire | 26 (24.3%) | 17 (13.7%) | 0.039 |
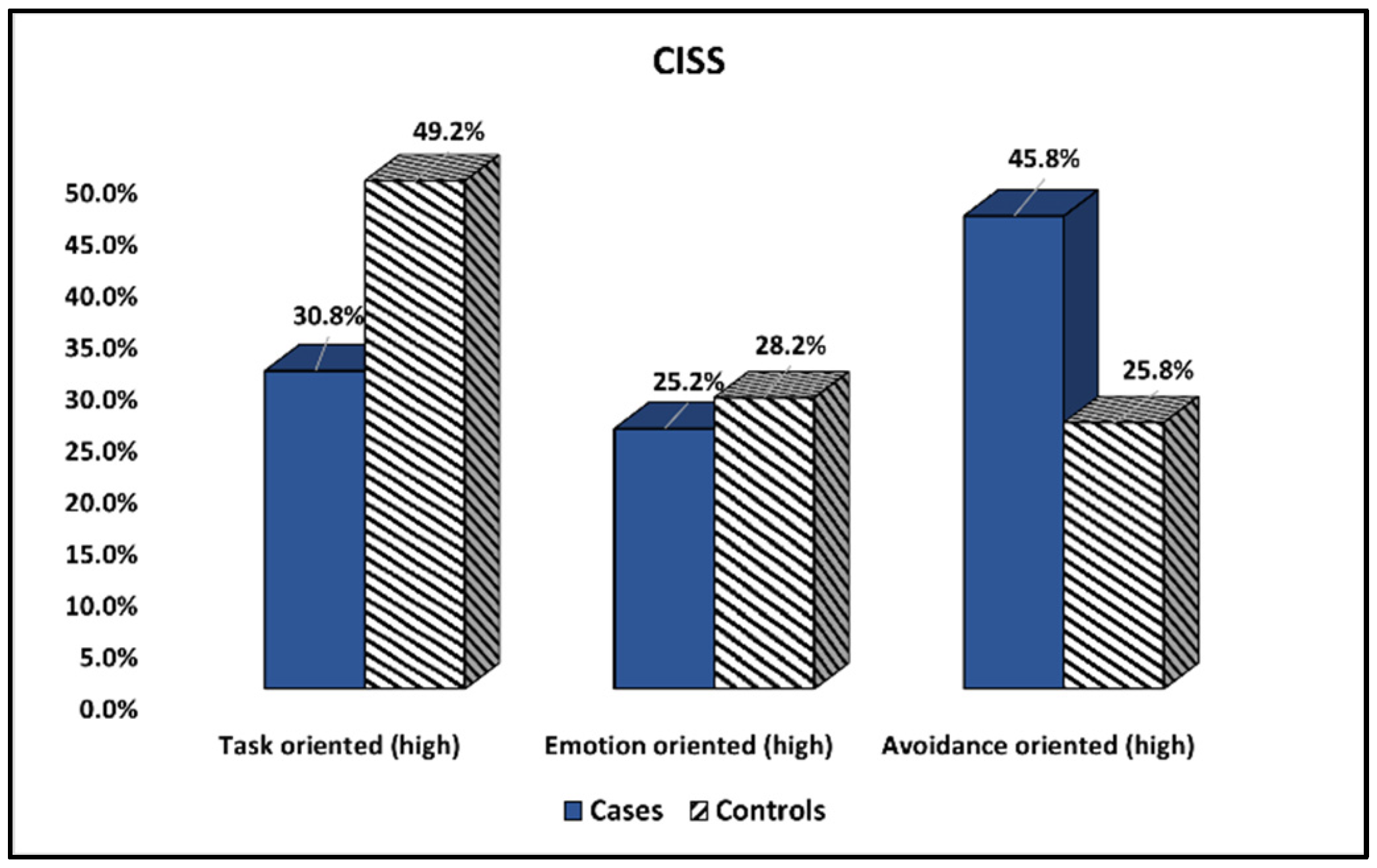
| Items (Score Range) | Cases (n = 107) | Controls (n = 124) | p-Value |
|---|---|---|---|
| Task-oriented (high) | 33 (30.8%) | 61 (49.2%) | 0.004 |
| Emotion-oriented (high) | 27 (25.2%) | 35 (28.2%) | 0.608 |
| Avoidance-oriented (high) | 49 (45.8%) | 32 (25.8%) | 0.002 |
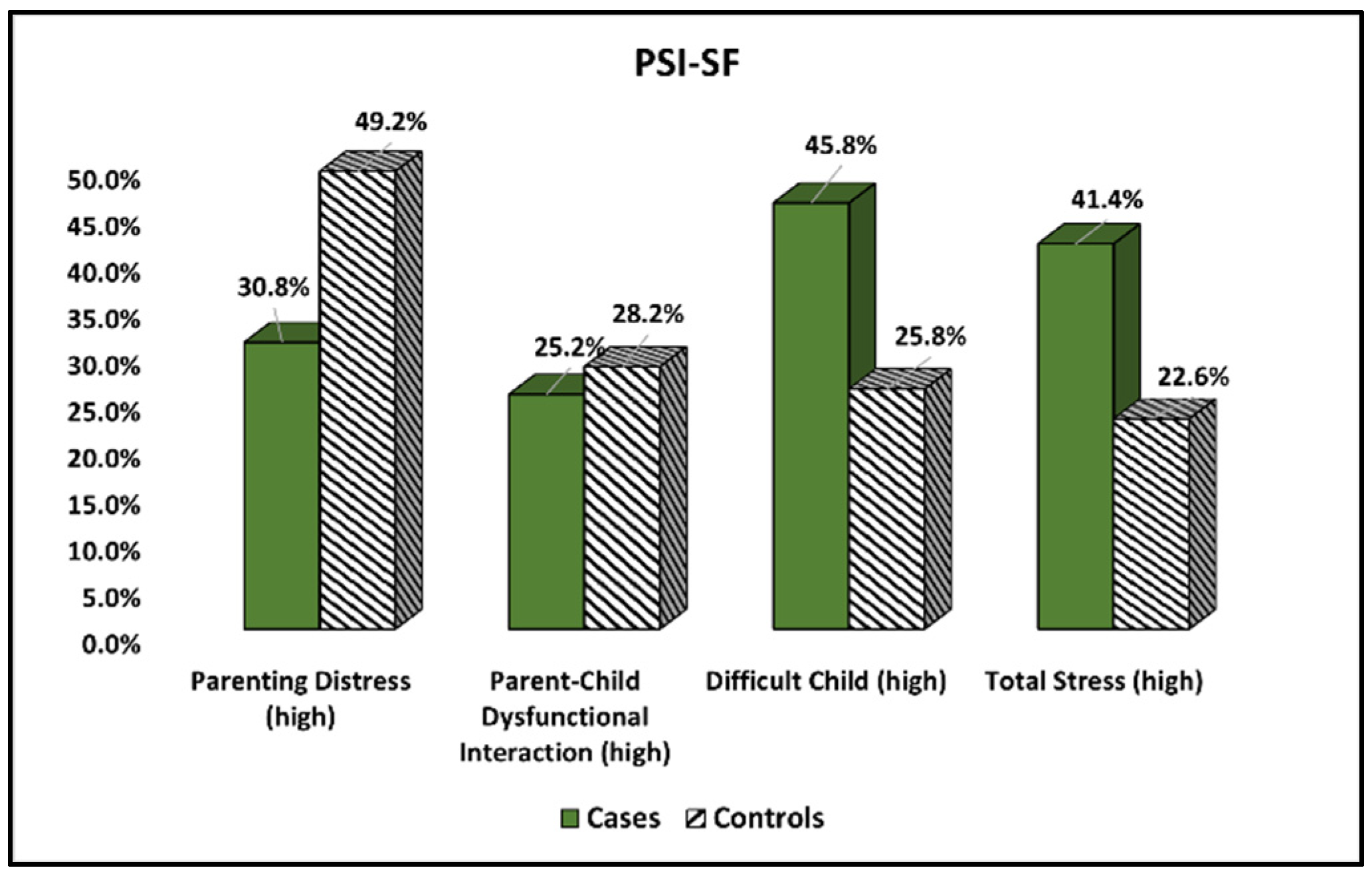
| Components | Cases (n = 107) | Controls (n = 124) | p-Value |
|---|---|---|---|
| Parenting Distress (high) | 46 (43.0%) | 33 (26.6%) | 0.008 |
| Parent–Child Dysfunctional Interaction (high) | 29 (27.1%) | 30 (24.2%) | 0.613 |
| Difficult Child (high) | 37 (34.6%) | 23 (18.5%) | 0.005 |
| Total Stress (high) | 44 (41.4%) | 28 (22.6%) | 0.002 |
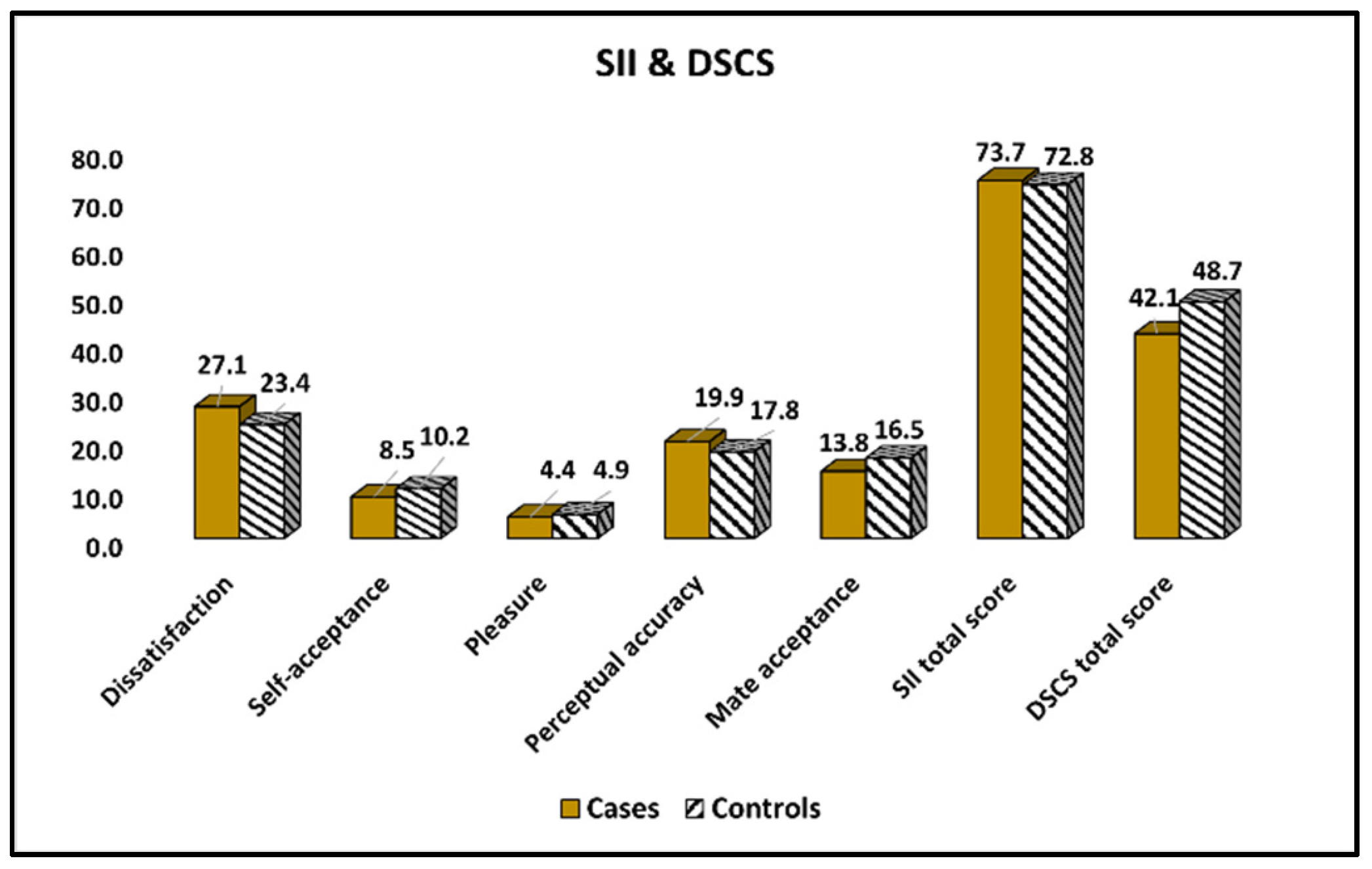
| Items | Cases (n = 107) | Controls (n = 124) | p-Value |
|---|---|---|---|
| Dissatisfaction | 27.1 ± 2.6 | 23.4 ± 3.0 | <0.001 |
| Self-acceptance | 8.5 ± 2.9 | 10.2 ± 3.3 | <0.001 |
| Pleasure | 4.4 ± 2.7 | 4.9 ± 3.1 | 0.195 |
| Perceptual accuracy | 19.9 ± 4.3 | 17.8 ± 5.5 | 0.002 |
| Mate acceptance (marital quality) | 13.8 ± 1.9 | 16.5 ± 2.2 | <0.001 |
| SII total score | 73.7 ± 14.4 | 72.8 ± 17.1 | 0.668 |
| DSCS total score | 42.1 ± 11.6 | 48.7 ± 9.9 | <0.001 |
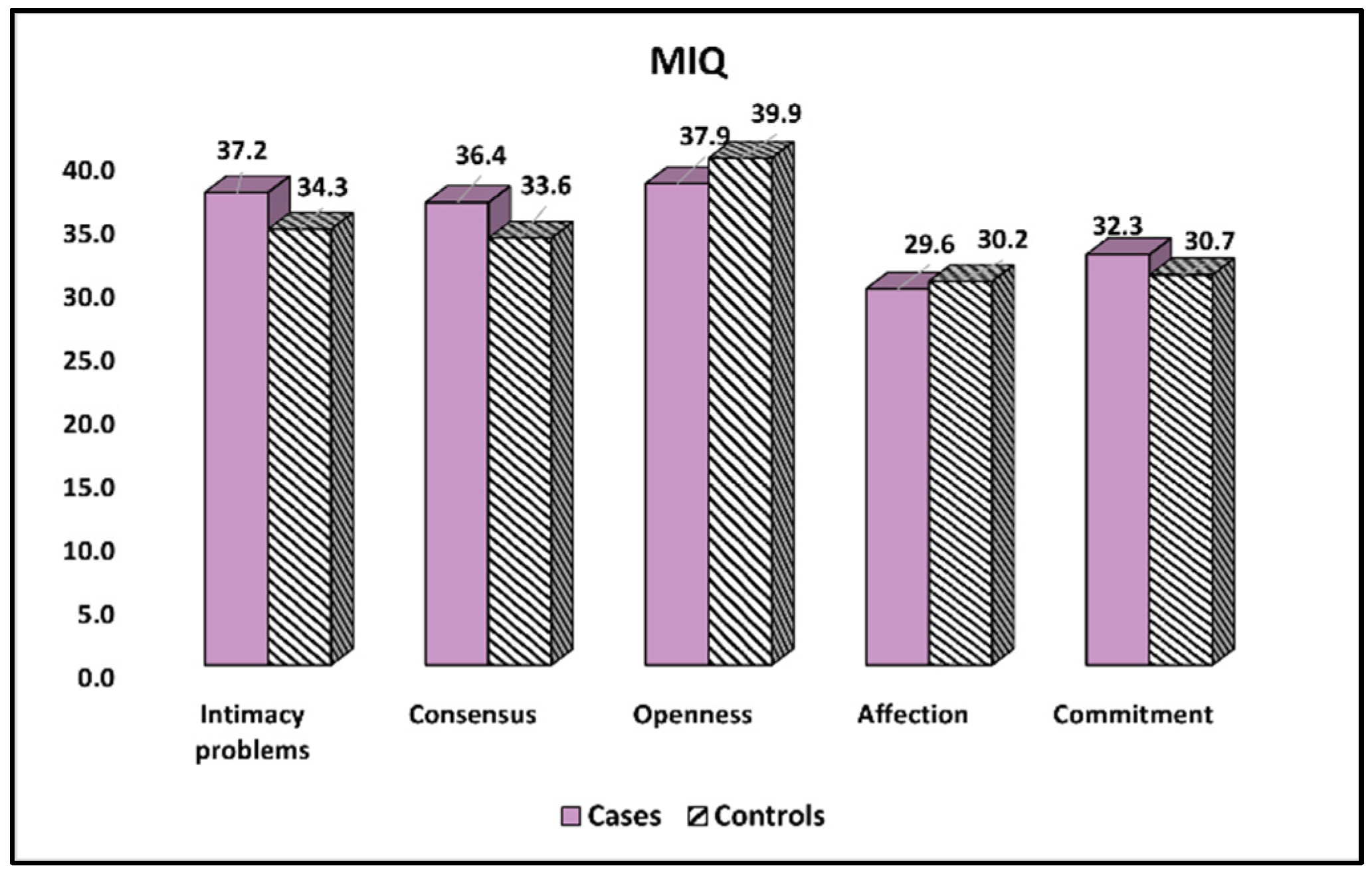
| Items | Cases (n = 107) | Controls (n = 124) | p-Value |
|---|---|---|---|
| Intimacy problems | 37.2 ± 10.4 | 34.3 ± 8.6 | 0.021 |
| Consensus | 36.4 ± 7.7 | 33.6 ± 7.0 | 0.004 |
| Openness | 37.9 ± 7.0 | 39.9 ± 8.5 | 0.054 |
| Affection | 29.6 ± 5.8 | 30.2 ± 6.1 | 0.446 |
| Commitment | 32.3 ± 6.5 | 30.7 ± 5.7 | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popa, Z.L.; Margan, M.-M.; Bernad, E.; Stelea, L.; Craina, M.; Ciuca, I.M.; Bina, A.M. A Cross-Sectional Analysis of Paternal Intimacy Problems, Stress Levels, and Satisfaction from Families with Children Born with Mucoviscidosis. Int. J. Environ. Res. Public Health 2022, 19, 15055. https://doi.org/10.3390/ijerph192215055
Popa ZL, Margan M-M, Bernad E, Stelea L, Craina M, Ciuca IM, Bina AM. A Cross-Sectional Analysis of Paternal Intimacy Problems, Stress Levels, and Satisfaction from Families with Children Born with Mucoviscidosis. International Journal of Environmental Research and Public Health. 2022; 19(22):15055. https://doi.org/10.3390/ijerph192215055
Chicago/Turabian StylePopa, Zoran Laurentiu, Madalin-Marius Margan, Elena Bernad, Lavinia Stelea, Marius Craina, Ioana Mihaela Ciuca, and Anca Mihaela Bina. 2022. "A Cross-Sectional Analysis of Paternal Intimacy Problems, Stress Levels, and Satisfaction from Families with Children Born with Mucoviscidosis" International Journal of Environmental Research and Public Health 19, no. 22: 15055. https://doi.org/10.3390/ijerph192215055
APA StylePopa, Z. L., Margan, M.-M., Bernad, E., Stelea, L., Craina, M., Ciuca, I. M., & Bina, A. M. (2022). A Cross-Sectional Analysis of Paternal Intimacy Problems, Stress Levels, and Satisfaction from Families with Children Born with Mucoviscidosis. International Journal of Environmental Research and Public Health, 19(22), 15055. https://doi.org/10.3390/ijerph192215055