
The “Our Voice” Method: Participatory Action Citizen Science Research to Advance Behavioral Health and Health Equity Outcomes

 , ,
, ,
Abstract
1. Introduction
2. The OV Method for Action-Focused Research
2.1. Theoretical Foundations
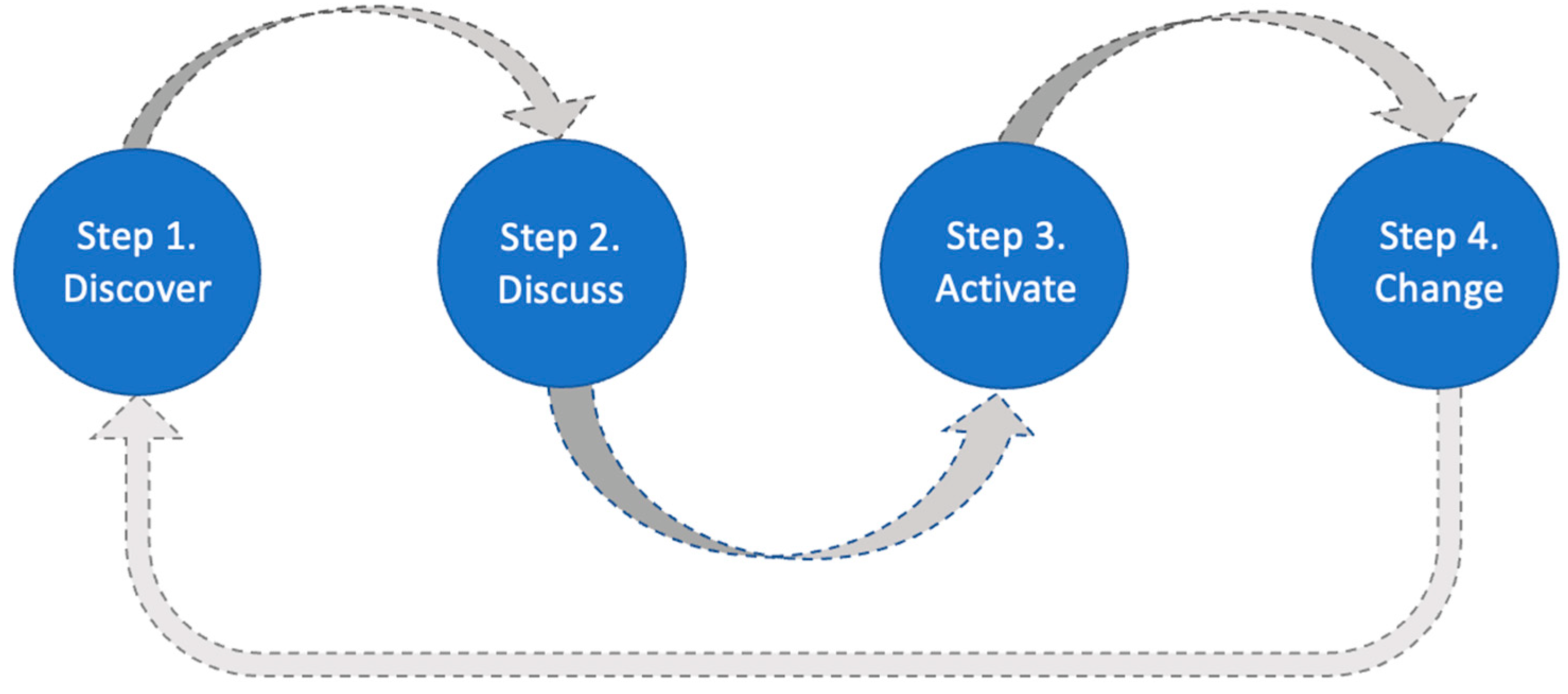
2.2. The OV Method
2.3. Applications
3. Research, Process, and Community Outcomes

{kind=link}
{kind=link}
| Study | Focus | Study Details | Outcomes by Category | ||||
|---|---|---|---|---|---|---|---|
| Location | Citizen Scientists | Metrics | Research (Building Knowledge) | Process (Building Capacity) | Community (Building Health) | ||
| Chrisinger et al. (2018) [23] | Healthy Corner Store Network | New Jersey, USA | 8 adult community members 18–40 years | Documenting resident perceptions of Healthy Corner Store Network access and food environments |
|
|
|
| Buman et al. (2015) [30] | Shoppers’ experiences in an urban famer’s market | Southwestern USA | 38 adult shoppers aged 18–35 | Factors that enhance or diminish the experience of shoppers in an urban farmer’s market |
| N/A |
|
| Sheats et al. (2017) [24] | Healthy food environments | California, USA | 23 older adults (aged 61–92 years) | Factors that impact accessibility, choice, and buying healthy food, and experiences of older adults while navigating food environments |
|
|
|
| Seguin et al. (2015) [32] | Barriers and facilitators to rural healthy eating and active living | New York, USA | 24 rural adults (mean age 69.4 years; SD 13.2) | Conducting environmental audits to identify factors that prevent or promote healthy eating and active living. |
|
|
|
3.1. Step 1. Discover
3.2. Step 2. Discuss
3.3. Step 3. Activate
3.4. Step 4. Change
4. Hallmark Features of the OV Method
4.1. Multifaceted Participatory Practices
4.2. Adaptability and Accessibility
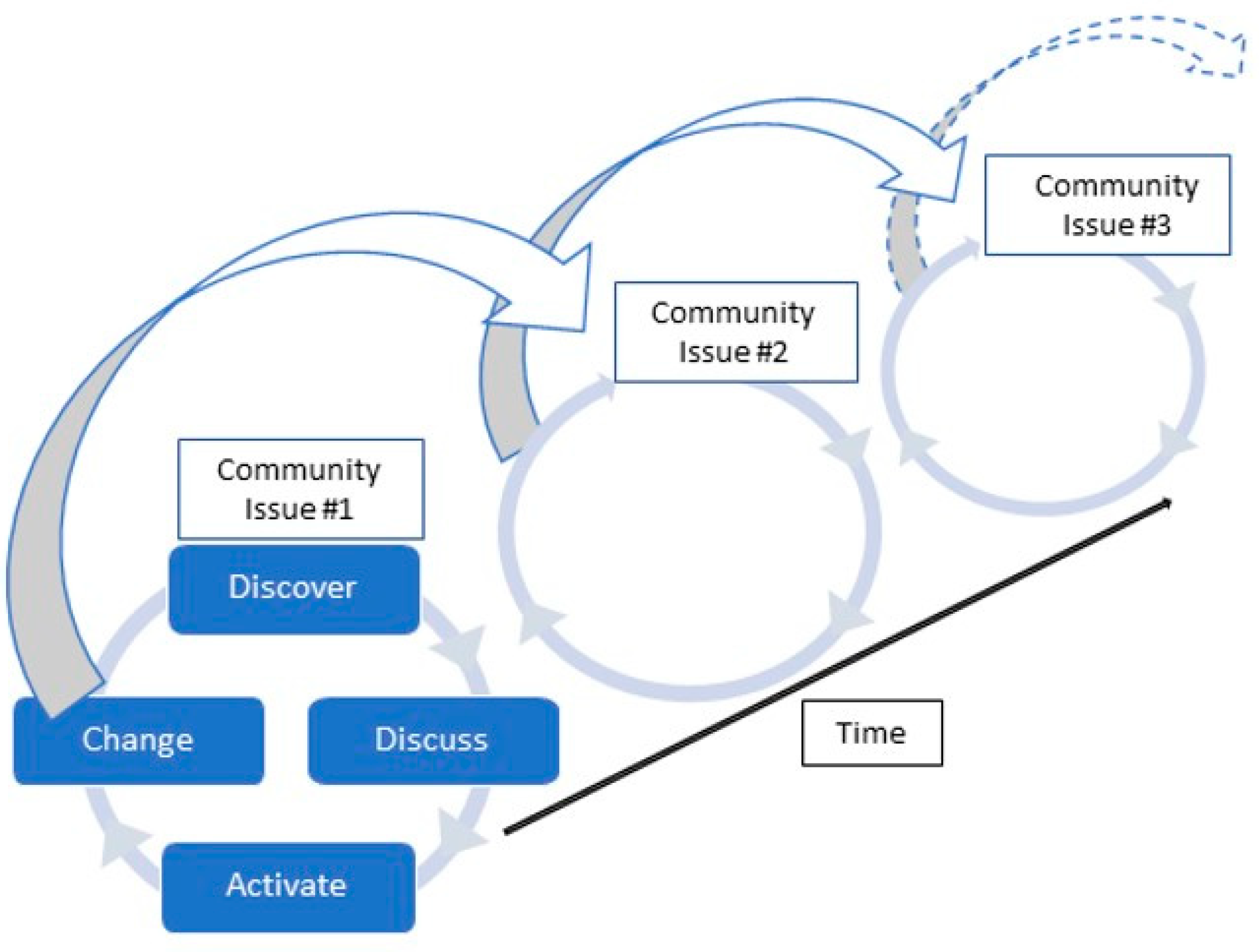
4.3. Iterative Process with Potential for Cumulative Results
5. Innovations in Current OV Projects
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization Heath Equity and Its Determinants. World Health Organization. 2021. Available online: https://www.who.int/publications/m/item/health-equity-and-its-determinants (accessed on 1 June 2022).
- Braveman, P.; Gruskin, S. Defining equity in health. J. Epidemiol. Community Health 2003, 57, 254–258. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef]
- Freire, P. Pedagogy of the Oppressed, 30th ed.; Bloomsbury Publishing Inc.: New York, NY, USA, 2012. [Google Scholar]
- Graham, I.D.; McCutcheon, C.; Kothari, A. Exploring the frontiers of research co-production: The Integrated Knowledge Translation Research Network concept papers. Health Res. Policy Syst. 2019, 17, 88. [Google Scholar] [CrossRef] [PubMed]
- Beckett, K.; Farr, M.; Kothari, A.; Wye, L.; Le May, A. Embracing complexity and uncertainty to create impact: Exploring the processes and transformative potential of co-produced research through development of a social impact model. Health Res. Policy Syst. 2018, 16, 118. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of community-based research: Assessing partnership approaches to improve public health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed]
- Jull, J.; Giles, A.; Graham, I.D. Community-based participatory research and integrated knowledge translation: Advancing the co-creation of knowledge. Implement. Sci. 2017, 12, 150. [Google Scholar] [CrossRef]
- Tolman, D.L.; Brydon-Miller, M. (Eds.) From Subjects to Subjectivities: A Handbook of Interpretive and Participatory Methods; New York University Press: New York, NY, USA, 2001. [Google Scholar]
- Irwin, A. Citizen Science: A Study of People, Expertise and Sustainable Development; Routledge: London, UK, 2002. [Google Scholar]
- European Citizen Science Association What Is Citizen Science? European Citizen Science Association. 2021. Available online: https://ecsa.citizen-science.net/#what-is-cs (accessed on 1 June 2022).
- Albert, A.; Balázs, B.; Butkevičienė, E.; Mayer, K.; Perelló, J. Citizen Social Science: New and Established Approaches to Participation in Social Research, Chapter 7; Vohland, K., Ed.; The Science of Citizen Science; Springer: Berlin/Heidelberg, Germany, 2021; pp. 119–138. [Google Scholar] [CrossRef]
- King, A.C.; Campero, M.I.; Garcia, D.; Blanco-Velazquez, I.; Banchoff, A.; Fierros, F.; Ahn, D.K. Testing the effectiveness of community-engaged citizen science to promote physical activity, foster healthier neighborhood environments, and advance health equity in vulnerable communities: The Steps for Change randomized controlled trial design and methods. Contemp. Clin. Trials 2021, 108, 106526. [Google Scholar]
- Wiggins, A.; Wilbanks, J. The rise of citizen science in health and biomedical research. Am. J. Bioeth. 2019, 19, 3–14. [Google Scholar] [CrossRef]
- Rosas, L.G.; Espinosa, P.R.; Jimenez, F.M.; King, A.C. The Role of Citizen Science in Promoting Health Equity. Annu. Rev. Public Health 2022, 43, 215. [Google Scholar] [CrossRef]
- King, A.C.; King, D.K.; Banchoff, A.; Solomonov, S.; Ben Natan, O.; Hua, J. Employing participatory citizen science methods to promote age-friendly environments worldwide. Int. J. Environ. Res. Public Health 2020, 17, 1541. [Google Scholar] [CrossRef]
- King, A.C.; Odunitan-Wayas, F.A.; Chaudhury, M.; Rubio, M.A.; Baiocchi, M.; Kolbe-Alexander, T.; Gardiner, P.A. Community-based approaches to reducing health inequities and fostering environmental justice through global youth-engaged citizen science. Int. J. Environ. Res. Public Health 2021, 18, 892. [Google Scholar] [CrossRef]
- Buman, M.P.; Winter, S.J.; Sheats, J.L.; Hekler, E.B.; Otten, J.J.; Grieco, L.A.; King, A.C. The Stanford Healthy Neighborhood Discovery Tool: A computerized tool to assess active living environments. Am. J. Prev. Med. 2013, 44, e41–e47. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N. ‘Ecological models of health behavior’. In Health Behavior: Theory, Research, and Practice, 5th ed.; Jossey-Bass/Wiley: Hoboken, NJ, USA, 2015; pp. 43–64. [Google Scholar]
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef]
- Zha, C.C.; Jansen, B.; Banchoff, A.; Fernes, P.; Chong, J.; Castro, V.; Vallez-Kelly, T.; Fenton, M.; Rogers, J.; King, A.C. Integrating Photovoice and Citizen Science: The Our Voice Initiative in Practice. Health Promot. Pract. 2022. [Google Scholar] [CrossRef]
- King, A.C.; Winter, S.J.; Chrisinger, B.W.; Hua, J.; Banchoff, A.W. Maximizing the promise of citizen science to advance health and prevent disease. Prev. Med. 2019, 119, 44. [Google Scholar] [CrossRef]
- Chrisinger, B.W.; Ramos, A.; Shaykis, F.; Martinez, T.; Banchoff, A.W.; Winter, S.J.; King, A.C. Leveraging citizen science for healthier food environments: A pilot study to evaluate corner stores in Camden, New Jersey. Front. Public Health 2018, 6, 89. [Google Scholar] [CrossRef]
- Sheats, J.L.; Winter, S.J.; Romero, P.P.; King, A.C. FEAST: Empowering community residents to use technology to assess and advocate for healthy food environments. J. Urban Health 2017, 94, 180–189. [Google Scholar] [CrossRef]
- Winter, S.J.; Rosas, L.G.; Romero, P.P.; Sheats, J.L.; Buman, M.P.; Baker, C.; King, A.C. Using citizen scientists to gather, analyze, and disseminate information about neighborhood features that affect active living. J. Immigr. Minor. Health 2016, 18, 1126–1138. [Google Scholar] [CrossRef]
- Rodriguez, N.M.; Arce, A.; Kawaguchi, A.; Hua, J.; Broderick, B.; Winter, S.J.; King, A.C. Enhancing safe routes to school programs through community-engaged citizen science: Two pilot investigations in lower density areas of Santa Clara County, California, USA. BMC Public Health 2019, 19, 256. [Google Scholar] [CrossRef]
- Graham, S.; Zha, C.C.; King, A.C.; Banchoff, A.W.; Sarnquist, C.; Dauber, M.; Baiocchi, M. A novel model for generating creative, community-responsive interventions to reduce gender-based violence on college campuses. Int. J. Environ. Res. Public Health 2021, 18, 7933. [Google Scholar] [CrossRef]
- O’Connor, A.; King, A.; Banchoff, A.; Eyler, A.; Reis, R.; Brownson, R.; Salvo, D. Harnessing citizen science to assess and improve utilization of metropolitan parks: The Park Activity, Recreation, and Community, Study (PARCS) in St. Louis, MO. J. Healthy Eat. Act. Living 2021, 1, 186–203. [Google Scholar] [CrossRef]
- Tuckett, A.G.; Freeman, A.; Hetherington, S.; Gardiner, P.A.; King, A.C.; Burnie Brae Citizen Scientists. Older Adults Using Our Voice Citizen Science to Create Change in Their Neighborhood Environment. Int. J. Environ. Res. Public Health 2018, 15, 2685. [Google Scholar] [CrossRef] [PubMed]
- Buman, M.P.; Bertmann, F.; Hekler, E.B.; Winter, S.J.; Sheats, J.L.; King, A.C.; Wharton, C.M. A qualitative study of shopper experiences at an urban farmers’ market using the Stanford Healthy Neighborhood Discovery Tool. Public Health Nutr. 2015, 18, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- González, S.A.; Rubio, M.A.; Triana, C.A.; King, A.C.; Banchoff, A.W.; Sarmiento, O.L. Building healthy schools through technology-enabled citizen science: The case of the our voice participatory action model in schools from Bogotá, Colombia. Glob. Public Health 2022, 17, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.A.; Morgan, E.H.; Connor, L.M.; Garner, J.A.; King, A.C.; Sheats, J.L.; Winter, S.J.; Buman, M.P. Rural Food and Physical Activity Assessment Using an Electronic Tablet-Based Application, New York, 2013-2014. Prev. Chronic Dis. 2015, 12, E102. [Google Scholar] [CrossRef]
- Odunitan-Wayas, F.A.; Hamann, N.; Sinyanya, N.A.; King, A.C.; Banchoff, A.; Winter, S.J.; Lambert, E.V. A citizen science approach to determine perceived barriers and promoters of physical activity in a low-income South African community. Glob. Public Health 2020, 15, 749–762. [Google Scholar] [CrossRef]
- Buman, M.P.; Winter, S.J.; Baker, C.; Hekler, E.B.; Otten, J.J.; King, A.C. Neighborhood Eating and Activity Advocacy Teams (NEAAT): Engaging older adults in policy activities to improve food and physical environments. Transl. Behav. Med. 2012, 2, 249–253. [Google Scholar] [CrossRef]
- Winter, S.J.; Buman, M.P.; Sheats, J.L.; Hekler, E.B.; Otten, J.J.; Baker, C.; Cohen, D.; Butler, B.A.; King, A.C. Harnessing the potential of older adults to measure and modify their environments: Long-term successes of the Neighborhood Eating and Activity Advocacy Team (NEAAT) study. TBM 2014, 4, 226–227. [Google Scholar] [CrossRef]
- Rubio, M.A.; Triana, C.; King, A.C.; Rosas, L.G.; Banchoff, A.W.; Rubiano, O.; Sarmiento, O.L. Engaging citizen scientists to build healthy park environments in Colombia. Health Promot. Int. 2021, 36, 223–234. [Google Scholar] [CrossRef]
- Welborn, R.; Downey, L.; Dyk, P.H.; Monroe, P.A.; Tayler-Mackey, C.; Worth, S.L. Turning the tide on poverty: Documenting impacts through ripple effect mapping. Community Dev. 2016, 47, 385–402. [Google Scholar] [CrossRef]
- Kusenbach, M. Street Phenomenology: The Go-Along as Ethnographic Research Tool. Ethnography 2003, 4, 455–485. [Google Scholar] [CrossRef]
- Carpiano, R.M. Come take a walk with me: The “Go-Along” interview as a novel method for studying the implications of place for health and well-being. Health Place 2009, 15, 263–272. [Google Scholar] [CrossRef]
- Evans, J.; Jones, P. The walking interview: Methodology, mobility and place. Appl. Geogr. 2011, 31, 849–858. [Google Scholar] [CrossRef]
- Springgay, S.; Truman, S.E. Walking Methodologies in a More-Than-Human World: WalkingLab; Milton Park: Abingdon, UK; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Peluso, N.L. Whose Woods Are These? Counter-Mapping Forest Territories in Kalimantan, Indonesia. Antipode 1995, 27, 383–406. [Google Scholar] [CrossRef]
- Kitzinger, J. The methodology of focus groups: The importance of interaction between research participants. Sociol. Health Illn. 1994, 16, 103–121. [Google Scholar] [CrossRef]
- Leavy, P. The practice of feminist oral history and focus group interviews. In S. N. Hesse-Biber, & P. L. Leavy Feminist Research Practice; SAGE Publications, Inc.: Newbury Park, CA, USA, 2007; pp. 149–186. [Google Scholar]
- Center for Community Health and Development (n.d.). Chapter 3, Section 3: Conducting Public Forums and Listening Sessions. University of Kansas. The Community Tool Box. Available online: https://ctb.ku.edu/en/table-of-contents/assessment/assessing-community-needs-and-resources/conduct-public-forums/main (accessed on 9 August 2022).
- Lykes, M.B.; Coquillon, E. Participatory and action research and feminisms: Towards transformative praxis. In S.N. Hesse-Biber Handbook of Feminist Research: Theory and Praxis; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2007; pp. 297–326. [Google Scholar]
- Massey, D.B. For Space; SAGE: London, UK; Thousand Oaks, CA, USA, 2005; 222p. [Google Scholar]
- Chrisinger, B.W.; King, A.C. Stress experiences in neighborhood and social environments (SENSE): A pilot study to integrate the quantified self with citizen science to improve the built environment and health. Int. J. Health Geogr. 2018, 17, 17. [Google Scholar] [CrossRef]
- Haraway, D.J. Simians, Cyborgs, and Women: The Reinvention of Nature; Routledge: London, UK, 1991. [Google Scholar]
- Corburn, J. Bringing Local Knowledge into Environmental Decision Making: Improving Urban Planning for Communities at Risk. J. Plan. Educ. Res. 2003, 22, 420–433. [Google Scholar] [CrossRef]
- Sarmiento, O.L.; Higuera-Mendieta, D.; Wilches-Mogollon, M.A.; Guzman, L.A.; Rodríguez, D.A.; Morales, R.; Diez Roux, A.V. Urban transformations and health: Methods for TrUST—A natural experiment evaluating the impacts of a mass transit cable car in Bogotá, Colombia. Front. Public Health 2020, 8, 64. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B.; Minkler, M.; Foley, K. Developing and Maintaining Partnerships with Communities. In Methods in Community-Based Participatory Research for Health; Israel, B., Eng, E., Schulz, A., Parker, Eds.; Jossey-Bass: San Francisco, CA, USA, 2005; pp. 31–51. [Google Scholar]


| Our Voice Method Steps | Outcome Category | ||
|---|---|---|---|
| Research (Building Knowledge) | Process (Building Capacity) | Community (Building Health) | |
| Step 1: Discover | Co-produce individual citizen scientist understanding and embodied experiences in selected settings | Establish equitable distribution of power across partnership as citizen scientists control data collection | Assemble a resource of citizen scientist collected data that can be used in further advocacy efforts |
| Understand acceptability of technology-based methods and citizen science approach in different populations | Enhance awareness among citizen scientists about influence of environment on health | Experience benefits of data gathering, e.g., collective engagement and contributions to science and the community | |
| Help to build self-efficacy for using digital tools | Experience therapeutic benefits of participating in a research walk, e.g., improved mental and/or physical health | ||
| Step 2: Discuss | Co-generate understanding of group perspectives and interpretations of one’s own experiences in selected setting | Facilitate awareness of collective issues in selected setting | Catalyze new relationships across citizen scientists and community stakeholders |
| Identify needs or barriers and sources of strength for health-focused topic | Foster trust across partners through transparent research process Strengthen social connections across community members | Assign priority for action based on community values | |
| Characterize points of consensus and tension for health-focused topic | Generate collective solution-building using diverse, inclusive process | ||
| Build group momentum for action toward change | |||
| Identify trusted leaders/stakeholders within the community | |||
| Step 3: Activate | Identify appropriate research directions to match community priorities for inquiry and improvement | Initiate open lines for equitable communication within partnership about change, who can contribute, and how | Encourage exchange of local knowledge and desired actions between service users, providers and community members |
| Deliver advocacy training to citizen scientists to learn new skills and cultivate empowerment | Foster use of data-driven decisions among community stakeholders | ||
| Reinforce support for or inform changes to existing plans, programs, or policies | |||
| Step 4: Change | Complete short- and long-term improvements in social and/or environmental conditions, which impact health indicators | Further train citizen scientists in topics such as strategic communication, additional advocacy strategies, and ripple effects activities | Disseminate findings by citizen scientists across local networks |
| Intended and unintended impacts across time (ripple effects) | Extend partnership timeline to address long-term issues | Form groups to advocate change to decision-makers | |
| Bolster or sustain existing programming | |||
| Form coalitions across citizen scientists and stakeholders to sustain change | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedersen, M.; Wood, G.E.R.; Fernes, P.K.; Goldman Rosas, L.; Banchoff, A.; King, A.C. The “Our Voice” Method: Participatory Action Citizen Science Research to Advance Behavioral Health and Health Equity Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 14773. https://doi.org/10.3390/ijerph192214773
Pedersen M, Wood GER, Fernes PK, Goldman Rosas L, Banchoff A, King AC. The “Our Voice” Method: Participatory Action Citizen Science Research to Advance Behavioral Health and Health Equity Outcomes. International Journal of Environmental Research and Public Health. 2022; 19(22):14773. https://doi.org/10.3390/ijerph192214773
Chicago/Turabian StylePedersen, Maja, Grace E. R. Wood, Praveena K. Fernes, Lisa Goldman Rosas, Ann Banchoff, and Abby C. King. 2022. "The “Our Voice” Method: Participatory Action Citizen Science Research to Advance Behavioral Health and Health Equity Outcomes" International Journal of Environmental Research and Public Health 19, no. 22: 14773. https://doi.org/10.3390/ijerph192214773
APA StylePedersen, M., Wood, G. E. R., Fernes, P. K., Goldman Rosas, L., Banchoff, A., & King, A. C. (2022). The “Our Voice” Method: Participatory Action Citizen Science Research to Advance Behavioral Health and Health Equity Outcomes. International Journal of Environmental Research and Public Health, 19(22), 14773. https://doi.org/10.3390/ijerph192214773