
Working Time Control and Variability in Europe Revisited: Correlations with Health, Sleep, and Well-Being
Abstract
1. Introduction
1.1. Working Time Control (WTC)
1.2. Working Time Variability (WTV)
- whether the duration of daily or weekly working hours is stable (low WTV) or fluctuates (high WTV),
- whether the number of working days per week is stable (low WTV) or varies (high WTV), and
- whether daily start and end times are identical (low WTV) or variable (high WTV).
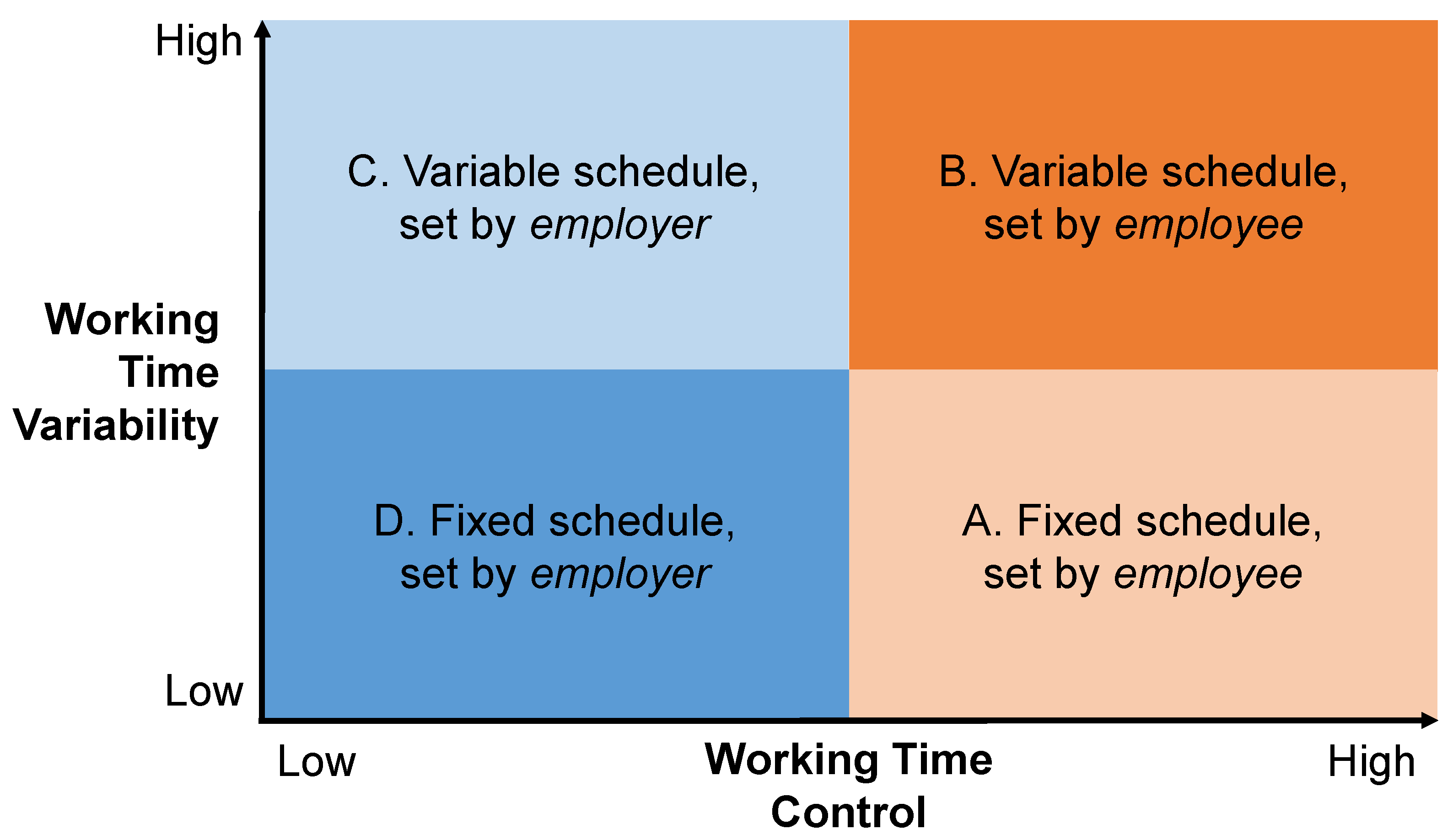
1.3. Working Time Control and Working Time Variability Combined: A Typology
1.4. Research Questions
2. Materials and Methods
2.1. Independent Variables
2.2. Dependent Variables
2.3. Control Variables
2.4. Data Analysis
3. Results
3.1. Descriptive Results
3.2. Multi-Level Results
3.3. Robustness Checks
3.4. Occupational Sectors
4. Discussion
4.1. Theoretical Implications
4.2. Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Sample | Working Time Arrangement Set by… | ||||||
|---|---|---|---|---|---|---|---|
| Employer | Employee | ||||||
| % (Column) | N | Fixed | Variable | Fixed | Variable | ||
| % (Row) | % (Row) | % (Row) | % (Row) | ||||
| Anglo-Saxon countries | Ireland | 3 | 816 | 39 | 38 | 5 | 18 |
| UK | 5 | 1287 | 36 | 34 | 10 | 20 | |
| Total | 15 | 4242 | 36 | 34 | 9 | 20 | |
| Baltic countries | Estonia | 3 | 783 | 40 | 31 | 8 | 22 |
| Latvia | 3 | 710 | 56 | 27 | 3 | 14 | |
| Lithuania | 3 | 806 | 56 | 37 | 1 | 6 | |
| Total | 1 | 356 | 52 | 33 | 4 | 12 | |
| Central-Eastern countries | Bulgaria | 3 | 857 | 73 | 23 | 1 | 3 |
| Croatia | 3 | 785 | 57 | 33 | 3 | 6 | |
| Czech Rep. | 3 | 792 | 46 | 37 | 3 | 15 | |
| Hungary | 3 | 786 | 53 | 33 | 3 | 11 | |
| Poland | 3 | 795 | 52 | 30 | 6 | 11 | |
| Romania | 3 | 811 | 59 | 33 | 2 | 6 | |
| Slovenia | 4 | 1263 | 41 | 34 | 6 | 19 | |
| Slovakia | 3 | 770 | 51 | 40 | 2 | 7 | |
| Total | 18 | 4963 | 54 | 32 | 4 | 10 | |
| Continental countries | Austria | 3 | 859 | 27 | 40 | 6 | 27 |
| Belgium | 8 | 2121 | 34 | 32 | 8 | 26 | |
| France | 5 | 1345 | 28 | 40 | 7 | 25 | |
| Germany | 6 | 1759 | 36 | 37 | 7 | 20 | |
| Luxembourg | 3 | 886 | 38 | 29 | 9 | 24 | |
| Netherlands | 3 | 830 | 22 | 33 | 11 | 34 | |
| Total | 41 | 11,532 | 32 | 37 | 8 | 23 | |
| Northern countries | Denmark | 3 | 888 | 10 | 37 | 8 | 45 |
| Finland | 3 | 792 | 23 | 32 | 10 | 35 | |
| Sweden | 3 | 888 | 16 | 30 | 12 | 42 | |
| Total | 5 | 1402 | 16 | 32 | 11 | 41 | |
| Southern countries | Cyprus | 3 | 772 | 58 | 35 | 3 | 4 |
| Greece | 2 | 607 | 62 | 30 | 1 | 7 | |
| Italy | 3 | 900 | 56 | 29 | 5 | 10 | |
| Malta | 3 | 865 | 55 | 32 | 6 | 8 | |
| Portugal | 3 | 740 | 61 | 29 | 3 | 7 | |
| Spain | 9 | 2642 | 54 | 31 | 6 | 9 | |
| Total | 20 | 5560 | 56 | 30 | 5 | 9 | |
Appendix B
| Robustness Checks | ||||||||
|---|---|---|---|---|---|---|---|---|
| (1) ICT Use at Least 50% of the Time (Subset) | (2) Control for Autonomy at Work | |||||||
| Independent variables | Dependent variables (all scaled 0–100 per cent) | |||||||
| S-RH | PHC | SP | W-B | S-RH | PHC | SP | W-B | |
| WTC: high WTC 1 | −0.08 (0.598) | 0.39 (0.669) | 0.09 (0.840) | −0.26 (0.665) | 0.19 (0.467) | 0.06 (0.528) | −0.05 (0.649) | −0.23 (0.520) |
| WTV: high WTV 2 | −1.92 *** (0.416) | 5.26 *** (0.465) | 5.36 *** (0.584) | −4.17 *** (0.463) | −1.94 *** (0.258) | 4.54 *** (0.293) | 4.30 *** (0.360) | −3.87 *** (0.288) |
| Interaction: high WTC × high WTV | 1.47 * (0.720) | −1.63 * (0.805) | −1.85 * (1.011) | 1.42 (0.801) | 1.11 * (0.550) | −1.30 * (0.623) | −0.84 (0.766) | 0.64 (0.613) |
| Control variables | See Table 2 | See Table 2 and Section 3.3 | ||||||
| ICC (country level) | 0.05 | 0.06 | 0.05 | 0.02 | 0.06 | 0.06 | 0.05 | 0.02 |
| χ2 (df = 3) | 23.06 | 153.06 | 97.51 | 95.34 | 61.65 | 267.49 | 164.85 | 215.46 |
| N | 12,605 | 12,605 | 12,605 | 12,605 | 27,511 | 27,511 | 27,511 | 27,511 |
| Robustness Checks | ||||||||
|---|---|---|---|---|---|---|---|---|
| (3) Control for Organizational Factors 3 | (4) Shift Workers Only | |||||||
| Independent variables | Dependent variables (all scaled 0–100 per cent) | |||||||
| S-RH | PHC | SP | W-B | S-RH | PHC | SP | W-B | |
| WTC: high WTC 1 | 0.32 (0.467) | 0.10 (0.528) | −0.20 (0.650) | 0.10 (0.520) | 1.24 (1.466) | −1.41 (1.712) | −2.15 (2.096) | 4.07 * (1.17) |
| WTV: high WTV 2 | −1.94 *** (0.259) | 4.54 *** (0.294) | 4.28 (0.361) | −3.85 *** (0.289) | −2.15 *** (0.488) | 4.67 *** (0.570) | 3.83 *** (0.697) | −3.34 *** (0.554) |
| Interaction: high WTC × high WTV | 1.05 (0.551) | −1.28 * (0.624) | −0.76 (0.768) | 0.62 (0.615) | −0.73 (1.670) | 2.43 (1.950) | 1.95 (2.386) | −4.36 * (1.898) |
| Control variables | See Table 2 and Section 3.3 | See Table 2 (shift work excluded) | ||||||
| ICC (country level) | 0.06 | 0.06 | 0.05 | 0.02 | 0.05 | 0.06 | 0.06 | 0.03 |
| χ2 (df = 3) | 62.25 | 266.04 | 162.64 | 207.55 | 22.42 | 80.18 | 35.36 | 52.25 |
| N | 27,302 | 27,302 | 27,302 | 27,302 | 6625 | 6625 | 6625 | 6625 |
Appendix C
| Occupational Sectors | ||||||||
|---|---|---|---|---|---|---|---|---|
| Hospitality | Retail | |||||||
| Independent variables | Dependent variables (all scaled 0–100 per cent) | |||||||
| S-RH | PHC | SP | W-B | S-RH | PHC | SP | W-B | |
| WTC: high WTC 1 | −2.65 (2.570) | 5.16 (2.970) | −2.56 (3.660) | 6.74 * (2.955) | 0.13 (1.534) | −2.60 (1.015) | −2.05 (2.083) | 0.085 (1.760) |
| WTV: high WTV 2 | −3.55 *** (1.026) | 5.62 *** (1.188) | 4.32 ** (1.465) | −3.51 ** (1.171) | −2.31 ** (0.747) | 5.13 *** (0.844) | 2.682 ** (1.015) | −5.12 *** (0.085) |
| Interaction: high WTC × high WTV | 2.87 (2.947) | −4.18 (3.409) | 4.16 (4.201) | −6.94 * (3.385) | 0.650 (1.882) | −0.233 (2.122) | −0.84 (0.766) | 1.87 (2.158) |
| Control variables | See Table 2 (except economic sector) | |||||||
| ICC (country level) | 0.04 | 0.07 | 0.08 | 0.03 | 0.06 | 0.06 | 0.05 | 0.02 |
| χ2 (df = 3) | 12.64 | 23.09 | 13.45 | 19.19 | 10.27 | 44.78 | 11.34 | 15.96 |
| N | 1480 | 1480 | 1480 | 1480 | 2697 | 2697 | 2697 | 2697 |
| Occupational Sectors | ||||
|---|---|---|---|---|
| Health and Social Care | ||||
| Dependent variables (all scaled 0–100 per cent) | ||||
| S-RH | PHC | SP | W-B | |
| WTC: high WTC 1 | 1.73 (1.612) | −1.67 (1.809) | 3.55 (2.254) | 1.00 (1.778) |
| WTV: high WTV 2 | −1.95 * (0.801) | 4.31 *** (0.899) | 5.33 *** (1.120) | −3.60 *** (0.851) |
| Interaction: high WTC × high WTV | −1.47 (1.821) | 1.59 (2.044) | −3.30 (2.548) | −1.31 (2.016) |
| Control variables | See Table 2 (except economic sector) | |||
| ICC (country level) | 0.07 | 0.06 | 0.04 | 0.02 |
| χ2 (df = 3) | 9.72 | 31.73 | 25.73 | 23.51 |
| N | 3182 | 3182 | 3182 | 3182 |
References
- Uglanova, E.; Dettmers, J. Sustained Effects of Flexible Working Time Arrangements on Subjective Well-Being. J. Happiness Stud. 2018, 19, 1727–1748. [Google Scholar] [CrossRef]
- Anttila, T.; Härmä, M.; Oinas, T. Working hours—Tracking the current and future trends. Ind. Health 2021, 59, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Anttila, T.; Oinas, T. 24/7 society—The new timing of work? In Family, Work and Well-Being: Emergence of New Issues; Tammelin, M., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 63–76. [Google Scholar]
- Eurofound; ILO. Working Anytime, Anywhere: The Effects on the World of Work; Publications Office of the European Union: Luxembourg; International Labour Office: Geneva, Switzerland, 2017.
- Katsabian, T. It’s the End of Working Time as We Know It—New Challenges to the Concept of Working Time in the Digital Reality. McGill Law J. 2020, 65, 379–419. [Google Scholar] [CrossRef]
- Lee, D.-J.; Sirgy, J.M. Work-Life Balance in the Digital Workplace: The Impact of Schedule Flexibility and Telecommuting on Work-Life Balance and Overall Life Satisfaction. In Thriving in Digital Workspaces: Emerging Issues for Research and Practice; Coetzee, M., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 355–384. [Google Scholar]
- Costa, G.; Sartori, S.; Åkerstedt, T. Influence of Flexibility and Variability of Working Hours on Health and Well-Being. Chronobiol. Int. 2006, 23, 1125–1137. [Google Scholar] [CrossRef]
- Anxo, D.; Franz, C.; Kümmerling, A. Working time distribution and preferences across the life course: A european perspective. Econ. Lav. 2013, 47, 77–106. [Google Scholar]
- De Spiegeleare, S.; Piasna, A. The Why and How of Working Time Reduction; EuropeanTrade Union Institute: Brussels, Belgium, 2017. [Google Scholar]
- Costa, G.; Åkerstedt, T.; Nachreiner, F.; Baltieri, F.; Carvalhais, J.; Folkard, S.; Dresen, M.F.; Gadbois, C.; Gartner, J.; Sukalo, H.G.; et al. Flexible Working Hours, Health, and Well-Being in Europe: Some Considerations from a SALTSA Project. Chronobiol. Int. 2004, 21, 831–844. [Google Scholar] [CrossRef]
- Karhula, K.; Salo, P.; Koskinen, A.; Ojajärvi, A.; Oksanen, T.; Puttonen, S.; Kivimäki, M.; Härmä, M. Employee control over scheduling of shifts and objectively measured working hour characteristics: A cross-sectional analysis of linked register and survey data. Chronobiol. Int. 2019, 36, 85–95. [Google Scholar] [CrossRef]
- Nijp, H.H.; Beckers, D.G.J.; Geurts, S.A.E.; Tucker, P.; Kompier, M.A.J. Systematic review on the association between employee worktime control and work-non-work balance, health and well-being, and job-related outcomes. Scandinavian J. Work Environ. Health 2012, 38, 299–313. [Google Scholar] [CrossRef]
- Bohle, P.; Willaby, H.; Quinlan, M.; McNamara, M. Flexible work in call centres: Working hours, work-life conflict & health. Appl. Ergon. 2011, 42, 219–224. [Google Scholar]
- Hughes, E.L.; Parkes, K.R. Work hours and well-being: The roles of work-time control and work–family interference. Work Stress 2007, 21, 264–278. [Google Scholar] [CrossRef]
- Ala-Mursula, L.; Vahtera, J.; Kouvonen, A.; Väänänen, A.; Linna, A.; Pentti, J.; Kivimäki, M. Long hours in paid and domestic work and subsequent sickness absence: Does control over daily working hours matter? Occup. Environ. Med. 2006, 63, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Parent-Thirion, A.; Biletta, I.; Cabrita, J.; Llave, O.V.; Vermeylen, G.; Wilczynska, A.; Wilkens, M. 6th European Working Conditions Survey: 2017 Update; Publications Office of the European Union: Luxembourg, 2017.
- Artazcoz, L.; Cortès-Franch, I.; Escribà-Agüir, V.; López, M.; Benavides, F.G. Long working hours and job quality in Europe: Gender and welfare state differences. Int. J. Environ. Res. Public Health 2018, 15, 2592. [Google Scholar] [CrossRef] [PubMed]
- Lunau, T.; Bambra, C.L.; Eikemo, T.A.; van der Wel, K.A.; Dragano, N. A balancing act? Work–life balance, health and well-being in European welfare states. Eur. J. Public Health 2014, 24, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Arlinghaus, A.; Bohle, P.; Iskra-Golec, I.; Jansen, N.; Jay, S.; Rotenberg, L. Working Time Society consensus statements: Evidence-based effects of shift work and non-standard working hours on workers, family and community. Ind. Health 2019, 57, 184–200. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.; Tijdens, K. Working time flexibility components and working time regimes in Europe: Using company-level data across 21 countries. Int. J. Hum. Resour. Manag. 2013, 24, 1418–1434. [Google Scholar] [CrossRef]
- Beckers, D.G.J.; Kompier, M.A.J.; Kecklund, G.; Härmä, M. Worktime control: Theoretical conceptualization, current empirical knowledge, and research agenda. Scand. J. Work Environ. Health 2012, 38, 291–297. [Google Scholar] [CrossRef]
- Schneider, D.; Harknett, K. Consequences of Routine Work-Schedule Instability for Worker Health and Well-Being. Am. Sociol. Rev. 2019, 84, 82–114. [Google Scholar] [CrossRef]
- Bohle, P.; Quinlan, M.; Kennedy, D.; Williamson, A. Working hours, work-life conflict and health in precarious and “permanent” employment. Rev. De Saúde Pública 2004, 38 (Suppl.), 19–25. [Google Scholar] [CrossRef]
- Henly, J.R.; Lambert, S.J. Unpredictable Work Timing in Retail Jobs: Implications for Employee Work–Life Conflict. ILR Rev. 2014, 67, 986–1016. [Google Scholar] [CrossRef]
- Dembe, A.E.; Erickson, J.B.; Delbos, R.G.; Banks, S.M. The impact of overtime and long work hours on occupational injuries and illnesses: New evidence from the United States. Occup. Environ. Med. 2005, 62, 588. [Google Scholar] [CrossRef]
- Marchand, A.; Demers, A.; Durand, P. Does work really cause distress? The contribution of occupational structure and work organization to the experience of psychological distress. Soc. Sci. Med. 2005, 61, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Vahle-Hinz, T.; Kirschner, K.; Thomson, M. Employment-related Demands and Resources—New Ways of Researching Stress in Flexible Work Arrangements. Manag. Rev. 2013, 24, 199–221. [Google Scholar] [CrossRef]
- Berg, P.; Bosch, G.; Charest, J. Working-time configurations: A framework for analyzing diversity across countries. ILR Rev. 2014, 67, 805–837. [Google Scholar] [CrossRef]
- Virtanen, M.; Kivimäki, M.; Joensuu, M.; Virtanen, P.; Elovainio, M.; Vahtera, J. Temporary employment and health: A review. Int. J. Epidemiol. 2005, 34, 610–622. [Google Scholar] [CrossRef]
- Harknett, K.; Schneider, D.; Irwin, V. Improving health and economic security by reducing work schedule uncertainty. Proc. Natl. Acad. Sci. USA 2021, 118, e2107828118. [Google Scholar] [CrossRef]
- Cavallari, J.M.; Garza, J.L.; Ferguson, J.M.; Laguerre, R.A.; Decker, R.E.; Suleiman, A.O.; Dugan, A.G. Working Time Characteristics and Mental Health among Corrections and Transportation Workers. Ann. Work Expo. Health 2021, 65, 432–445. [Google Scholar] [CrossRef]
- Magnusson, C. Flexible time—But is the time owned? Family friendly and family unfriendly work arrangements, occupational gender composition and wages: A test of the mother-friendly job hypothesis in Sweden. Community Work Fam. 2021, 24, 291–314. [Google Scholar] [CrossRef]
- Wöhrmann, A.M.; Dilchert, N.; Michel, A. Working time flexibility and work-life balance. Z. Für Arb. 2021, 75, 74–85. [Google Scholar] [CrossRef]
- Garde, A.H.; Albertsen, K.; Nabe-Nielsen, K.; Carneiro, I.G.; Skotte, J.; Hansen, S.M.; Lund, H.; Hvid, H.; Hansen, Å.M. Implementation of self-rostering (the PRIO-project): Effects on working hours, recovery, and health. Scand. J. Work Environ. Health 2012, 38, 314–326. [Google Scholar] [CrossRef]
- Shin, M.-G.; Kim, Y.-J.; Kim, T.-K.; Kang, D. Effects of Long Working Hours and Night Work on Subjective Well-Being Depending on Work Creativity and Task Variety, and Occupation: The Role of Working-Time Mismatch, Variability, Shift Work, and Autonomy. Int. J. Environ. Res. Public Health 2021, 18, 6371. [Google Scholar] [CrossRef]
- Eurofound. Work on Demand: Recurrence, Effects and Challenges; Publications Office of the European Union: Luxemburg, 2018.
- Valcour, M. Work-based resources as moderators of the relationship between work hours and satisfaction with work-family balance. J. Appl. Psychol. 2007, 92, 1512–1523. [Google Scholar] [CrossRef]
- Soga, L.R.; Bolade-Ogunfodun, Y.; Mariani, M.; Nasr, R.; Laker, B. Unmasking the other face of flexible working practices: A systematic literature review. J. Bus. Res. 2022, 142, 648–662. [Google Scholar] [CrossRef]
- Backhaus, N.; Steidelmüller, C. How Leadership Can Help to Mitigate the Dark Side of Autonomy: Results Based on the German Sample of the European Working Conditions Survey. Manag. Rev. 2021, 32, 182–218. [Google Scholar]
- Kubicek, B.; Paškvan, M.; Bunner, J. The Bright and Dark Sides of Job Autonomy. In Job Demands in a Changing World of Work: Impact on Workers’ Health and Performance and Implications for Research and Practice; Korunka, C., Kubicek, B., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 45–63. [Google Scholar]
- Väänänen, A.; Toivanen, M. The challenge of tied autonomy for traditional work stress models. Work Stress 2018, 32, 1–5. [Google Scholar] [CrossRef]
- Väänänen, A.; Toivanen, M.; Lallukka, T. Lost in Autonomy—Temporal Structures and Their Implications for Employees’ Autonomy and Well-Being among Knowledge Workers. Occup. Health Sci. 2020, 4, 83–101. [Google Scholar] [CrossRef]
- Gerdenitsch, C.; Kubicek, B.; Korunka, C. Control in flexible working arrangements: When freedom becomes duty. J. Pers. Psychol. 2015, 14, 61. [Google Scholar] [CrossRef]
- Kubicek, B.; Korunka, C.; Tement, S. Too much job control? Two studies on curvilinear relations between job control and eldercare workers’ well-being. Int. J. Nurs. Stud. 2014, 51, 1644–1653. [Google Scholar] [CrossRef]
- Mazmanian, M.; Orlikowski, W.J.; Yates, J. The Autonomy Paradox: The Implications of Mobile Email Devices for Knowledge Professionals. Organ. Sci. 2013, 24, 1337–1357. [Google Scholar] [CrossRef]
- Eurofound. Telework and ICT-Based Mobile Work: Flexible Working in the Digital Age; Publications Office of the European Union: Luxemburg, 2020.
- Pérez-Zapata, O.; Serrano Pascual, A.; Álvarez-Hernández, G.; Castaño Collado, C. Knowledge work intensification and self-management: The autonomy paradox. Work. Organ. Labour Glob. 2016, 10, 27–49. [Google Scholar] [CrossRef]
- Sewell, G.; Taskin, L. Out of Sight, Out of Mind in a New World of Work? Autonomy, Control, and Spatiotemporal Scaling in Telework. Organ. Stud. 2015, 36, 1507–1529. [Google Scholar] [CrossRef]
- Steidelmüller, C.; Meyer, S.-C.; Müller, G. Home-Based Telework and Presenteeism Across Europe. J. Occup. Environ. Med. 2020, 62, 998–1005. [Google Scholar] [CrossRef]
- Gerdenitsch, C. New Ways of Working and Satisfaction of Psychological Needs. In Job Demands in a Changing World of Work: Impact on Workers’ Health and Performance and Implications for Research and Practice; Korunka, C., Kubicek, B., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 91–109. [Google Scholar]
- McCrate, E. Unstable and on-Call Work Schedules in the United States and Canada; International Labour Organization: Genf, Switzerland, 2018. [Google Scholar]
- Härmä, M.; Ropponen, A.; Hakola, T.; Koskinen, A.; Vanttola, P.; Puttonen, S.; Sallinen, M.; Salo, P.; Oksanen, T.; Pentti, J.; et al. Developing register-based measures for assessment of working time patterns for epidemiologic studies. Scand. J. Work. Environ. Health 2015, 41, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Greubel, J.; Arlinghaus, A.; Nachreiner, F. Arbeitszeitflexibilität auf Kosten der Sicherheit?—Zum Zusammenhang zwischen der Variabilität der Arbeitszeit und der Häufigkeit von Arbeitsunfällen. Z. Für Arb. 2014, 68, 89–95. [Google Scholar]
- Kubo, T.; Takahashi, M.; Togo, F.; Liu, X.; Shimazu, A.; Tanaka, K.; Takaya, M. Effects on employees of controlling working hours and working schedules. Occup. Med. 2013, 63, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Amlinger-Chatterjee, M. Psychische Gesundheit in der Arbeitswelt: Atypische Arbeitszeiten; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Dortmund/Berlin/Dresden, Germany, 2016. [Google Scholar]
- Kleiner, S.; Pavalko, E.K. Clocking In: The Organization of Work Time and Health in the United States. Soc. Forces 2010, 88, 1463–1486. [Google Scholar] [CrossRef]
- Norlund, S.; Reuterwall, C.; Höög, J.; Lindahl, B.; Janlert, U.; Birgander, L.S. Burnout, working conditions and gender-results from the northern Sweden MONICA Study. BMC Public Health 2010, 10, 326. [Google Scholar] [CrossRef]
- Golden, L. Irregular Work Scheduling and Its Consequences; Economic Policy Institute: Washington, DC, USA, 2015; p. 394. [Google Scholar]
- Eriksen, C.A.; Kecklund, G. Sleep, Sleepiness and Health Complaints in Police Officers: The Effects of a Flexible Shift System. Ind. Health 2007, 45, 279–288. [Google Scholar] [CrossRef]
- Olsen, K.M.; Dahl, S.-Å. Working time: Implications for sickness absence and the work–family balance. Int. J. Soc. Welf. 2010, 19, 45–53. [Google Scholar] [CrossRef]
- Janssen, D.; Nachreiner, F. Flexible Arbeitszeiten; Wirtschaftsverlag NW Verlag für neue Wissenschaft GmbH: Bremerhaven, Germany, 2004. [Google Scholar]
- Zeytinoglu, I.; Lillevik, W.; Seaton, B.; Moruz, J. Part-Time and Casual Work in Retail Trade: Stress and other Factors Affecting the Workplace. Relat. Ind. 2004, 59, 516–544. [Google Scholar]
- Karhula, K.; Wöhrmann, A.M.; Brauner, C.; Härmä, M.; Kivimäki, M.; Michel, A.; Oksanen, T. Working time dimensions and well-being: A cross-national study of Finnish and German health care employees. Chronobiol. Int. 2020, 37, 1312–1324. [Google Scholar] [CrossRef]
- Larsen, A.D.; Ropponen, A.; Hansen, J.; Hansen, Å.M.; Kolstad, H.A.; Koskinen, A.; Härmä, M.I.; Garde, A.H. Working time characteristics and long-term sickness absence among Danish and Finnish nurses: A register-based study. Int. J. Nurs. Stud. 2020, 112, 103639. [Google Scholar] [CrossRef] [PubMed]
- Rosenström, T.; Härmä, M.; Kivimäki, M.; Ervasti, J.; Virtanen, M.; Hakola, T.; Koskinen, A.; Ropponen, A. Patterns of working hour characteristics and risk of sickness absence among shift-working hospital employees: A data-mining cohort study. Scand. J. Work. Environ. Health 2021, 47, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Kaduk, A.; Genadek, K.; Kelly, E.L.; Moen, P. Involuntary vs. voluntary flexible work: Insights for scholars and stakeholders. Community Work Fam. 2019, 22, 412–442. [Google Scholar] [CrossRef] [PubMed]
- Allen, T.D.; Johnson, R.C.; Kiburz, K.M.; Shockley, K.M. Work–family conflict and flexible work arrangements: Deconstructing flexibility. Pers. Psychol. 2013, 66, 345–376. [Google Scholar] [CrossRef]
- Geurts, S.A.E.; Beckers, D.G.J.; Taris, T.W.; Kompier, M.A.J.; Smulders, P.G.W. Worktime Demands and Work-Family Interference: Does Worktime Control Buffer the Adverse Effects of High Demands? J. Bus. Ethics 2009, 84, 229–241. [Google Scholar] [CrossRef]
- Anttila, T.; Oinas, T.; Tammelin, M.; Nätti, J. Working-time regimes and work-life balance in Europe. Eur. Sociol. Rev. 2015, 31, 713–724. [Google Scholar] [CrossRef]
- ILO; Eurofound. Working Conditions in a Global Perspective; Publications Office of the European Union: Luxembourg; International Labour Organization: Geneva, Switzerland, 2019.
- Franke, F. Is Work Intensification Extra Stress? J. Pers. Psychol. 2015, 14, 17–27. [Google Scholar] [CrossRef]
- Müller, G.; Tisch, A.; Wöhrmann, A.M. The impact of long working hours on the health of German employees. Ger. J. Hum. Resour. Manag. 2018, 32, 217–235. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Luke, S.G. Evaluating significance in linear mixed-effects models in R. Behav. Res. Methods 2017, 49, 1494–1502. [Google Scholar] [CrossRef]
- Lott, Y. Working-time flexibility and autonomy: A European perspective on time adequacy. Eur. J. Ind. Relat. 2015, 21, 259–274. [Google Scholar] [CrossRef]
- Eurofound. Working Time Developments in the 21st Century: Work Duration and Its Regulation in the EU; Publications Office of the European Union: Luxemburg, 2016.
- Rigó, M.; Dragano, N.; Wahrendorf, M.; Siegrist, J.; Lunau, T. Work stress on rise? Comparative analysis of trends in work stressors using the European working conditions survey. Int. Arch. Occup. Environ. Health 2021, 94, 459–474. [Google Scholar] [CrossRef] [PubMed]
- Giebel, O.; Janßen, D.; Schomann, C.; Nachreiner, F. A New Approach for Evaluating Flexible Working Hours. Chronobiol. Int. 2004, 21, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Janssen, D.; Nachreiner, F. Health and psychosocial effects of flexible working hours. Rev. De Saúde Pública 2004, 38 (Suppl.), 11–18. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fenwick, R.; Tausig, M. Scheduling Stress: Family and Health Outcomes of Shift Work and Schedule Control. Am. Behav. Sci. 2001, 44, 1179–1198. [Google Scholar] [CrossRef]
- Shiri, R.; Karhula, K.; Turunen, J.; Koskinen, A.; Ropponen, A.; Ervasti, J.; Kivimäki, M.; Härmä, M. The Effect of Using Participatory Working Time Scheduling Software on Employee Well-Being and Workability: A Cohort Study Analysed as a Pseudo-Experiment. Healthcare 2021, 9, 1385. [Google Scholar] [CrossRef]
- Turunen, J.; Karhula, K.; Ropponen, A.; Koskinen, A.; Hakola, T.; Puttonen, S.; Hämäläinen, K.; Pehkonen, J.; Härmä, M. The effects of using participatory working time scheduling software on sickness absence: A difference-in-differences study. Int. J. Nurs. Stud. 2020, 112, 103716. [Google Scholar] [CrossRef]
- Hulsegge, G.; van Mechelen, W.; Proper, K.I.; Paagman, H.; Anema, J.R. Shift work, and burnout and distress among 7798 blue-collar workers. Int. Arch. Occup. Environ. Health 2020, 93, 955–963. [Google Scholar] [CrossRef]
- Eurofound. Overtime in Europe: Regulation and Practice; Publications Office of the European Union: Luxemburg, 2022.
- Eurofound. Living, Working and COVID-19; Publications Office of the European Union: Luxemburg, 2020.
- Milasi, S.; Bisello, M.; Hurley, J.; Sostero, M.; Fernández-Macías, E. The Potential for Teleworking in Europe and the Risk of a New Digital Divide. Available online: https://voxeu.org/article/potential-teleworking-europe-and-risk-new-digital-divide (accessed on 31 August 2020).
- Sostero, M.; Milasi, S.; Hurley, J.; Macias, E.F.; Bisello, M. Teleworkability and the COVID-19 Crisis: A New Digital Divide? May 2020; Joint Research Centre (JRC), European Commission: Seville, Spain, 2020.
- Dörflinger, N. Social interactions at work: Why interactive work should be an analytical category in its own right. Empl. Relat. Int. J. 2022, 44, 81–95. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]



| Sample | WTC | ||||||
|---|---|---|---|---|---|---|---|
| WTC Low | WTC High | ||||||
| % (Column) | N (Unweighted) | WTV Low | WTV High | WTV Low | WTV High | ||
| % (Row) | % (Row) | % (Row) | % (Row) | ||||
| (1) Individual characteristics | |||||||
| Sex | Male | 50 | 14,005 | 39 | 35 | 6 | 20 |
| Female | 50 | 14,051 | 42 | 33 | 7 | 17 | |
| Age (in years) | 15–29 | 19 | 5438 | 38 | 38 | 6 | 18 |
| 30–44 | 38 | 10,587 | 42 | 34 | 7 | 17 | |
| 45–54 | 27 | 7631 | 41 | 34 | 7 | 19 | |
| 55–65 | 16 | 4400 | 41 | 30 | 9 | 20 | |
| Education (ISCED) | Low | 16 | 4387 | 51 | 33 | 5 | 11 |
| Medium | 52 | 14,634 | 44 | 35 | 6 | 14 | |
| High | 32 | 9036 | 30 | 33 | 9 | 28 | |
| Spouse/partner in household | Yes | 32 | 8941 | 41 | 36 | 5 | 18 |
| No | 68 | 19,115 | 40 | 33 | 8 | 19 | |
| Age youngest child (<18) in household (in years) | No child | 64 | 18,055 | 41 | 35 | 7 | 17 |
| <7 | 16 | 4490 | 37 | 35 | 8 | 19 | |
| 7–12 | 11 | 3148 | 42 | 31 | 7 | 21 | |
| 13–17 | 8 | 2364 | 39 | 34 | 7 | 21 | |
| Household size (no. of individuals) | 1 | 13 | 3754 | 39 | 35 | 6 | 20 |
| 2 | 30 | 8551 | 40 | 34 | 8 | 18 | |
| 3 | 24 | 6829 | 43 | 34 | 6 | 17 | |
| 4 | 23 | 6408 | 40 | 34 | 7 | 19 | |
| 5 | 7 | 1843 | 40 | 32 | 8 | 20 | |
| 6 or more | 2 | 672 | 47 | 30 | 7 | 16 | |
| (2) Working time characteristics | |||||||
| Shift work | No | 76 | 21,303 | 42 | 28 | 8 | 22 |
| Yes | 24 | 6754 | 36 | 53 | 3 | 8 | |
| Actual working time (hours/week) | 1–19 | 9 | 2483 | 31 | 36 | 7 | 26 |
| 20–34 | 18 | 5037 | 37 | 38 | 8 | 16 | |
| 35–39 | 22 | 6300 | 40 | 34 | 9 | 17 | |
| 40–47 | 40 | 11,200 | 50 | 29 | 6 | 15 | |
| 48–59 | 9 | 2395 | 24 | 43 | 4 | 29 | |
| 60+ | 2 | 642 | 16 | 46 | 3 | 35 | |
| (3) Working time control (WTC) and working time variability (WTV) | |||||||
| WTC | Low | 75 | 20,976 | 54 | 46 | – | – |
| High | 25 | 7081 | – | – | 27 | 73 | |
| WTV | Low | 48 | 13,333 | 86 | – | 14 | – |
| High | 52 | 14,723 | – | 65 | – | 35 | |
| N | 100 | 28,056 | 41 | 34 | 7 | 18 | |
| N (unweighted) | 100 | 27,706 | 43 | 33 | 6 | 18 | |
| Independent Variables | Dependent Variables (All Scaled 0–100 per Cent) | |||
|---|---|---|---|---|
| Self-Rated Health (0 Very Bad, 100 Very Good) | Psychosomatic Health Complaints (0 No Complaints, 100 All Complaints) | Sleep Problems (0 None, 100 All Problems) | Well-Being (WHO-5-Scale) (0 Very Low, 100 Very High) | |
| WTC: high WTC 1 | 0.32 (0.465) | 0.14 (0.526) | −0.14 (0.647) | 0.15 (0.519) |
| WTV: high WTV 2 | −1.92 *** (0.258) | 4.53 *** (0.292) | 4.30 *** (0.359) | −3.85 *** (0.288) |
| Interaction: high WTC × high WTV | 1.03 (0.549) | −1.29 * (0.621) | −0.80 (0.765) | 0.52 (0.613) |
| Control variables for all dependent variables | EU28 countries (random intercept), individual characteristics (gender, age, education level, marital status, age of youngest child ≤18 years in household, household size), occupation, economic sector, working time characteristics (actual working time duration and shift work), see Table 1 | |||
| ICC (EU 28 country level) | 0.06 | 0.06 | 0.05 | 0.02 |
| χ2 (df = 3) | 62.0 *** | 268.7 *** | 165.76 *** | 210.8 *** |
| N | 27,706 | 27,706 | 27,706 | 27,706 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Backhaus, N. Working Time Control and Variability in Europe Revisited: Correlations with Health, Sleep, and Well-Being. Int. J. Environ. Res. Public Health 2022, 19, 14778. https://doi.org/10.3390/ijerph192214778
Backhaus N. Working Time Control and Variability in Europe Revisited: Correlations with Health, Sleep, and Well-Being. International Journal of Environmental Research and Public Health. 2022; 19(22):14778. https://doi.org/10.3390/ijerph192214778
Chicago/Turabian StyleBackhaus, Nils. 2022. "Working Time Control and Variability in Europe Revisited: Correlations with Health, Sleep, and Well-Being" International Journal of Environmental Research and Public Health 19, no. 22: 14778. https://doi.org/10.3390/ijerph192214778
APA StyleBackhaus, N. (2022). Working Time Control and Variability in Europe Revisited: Correlations with Health, Sleep, and Well-Being. International Journal of Environmental Research and Public Health, 19(22), 14778. https://doi.org/10.3390/ijerph192214778