

BOAM: A Visual, Explanatory Diagnostic and Psychoeducation System Used in Collaboration with Families—Feasibility and Acceptability for Children Who Are Non-Responsive to Treatment as Usual

Abstract
1. Introduction
1.1. Literature Review
1.2. The BOAM Diagnostic Process
1.2.1. Step 1 of the BOAM Diagnostic Process: Understanding Psychological Functioning Using the BOAM Basic Model
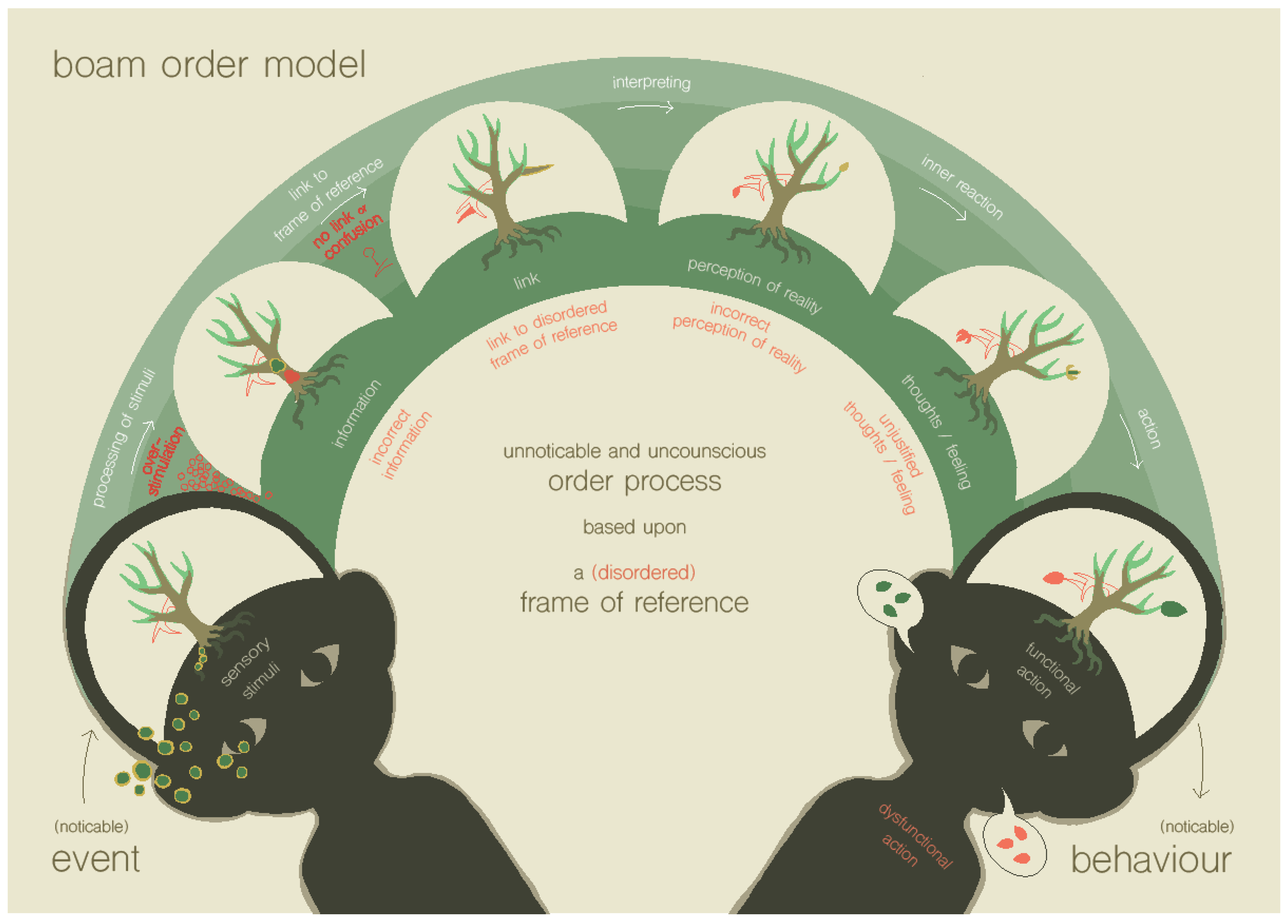
1.2.2. Step 2 of the BOAM Diagnostic Process: Recognizing the Disrupted Ordering Processes Using the BOAM Order Model
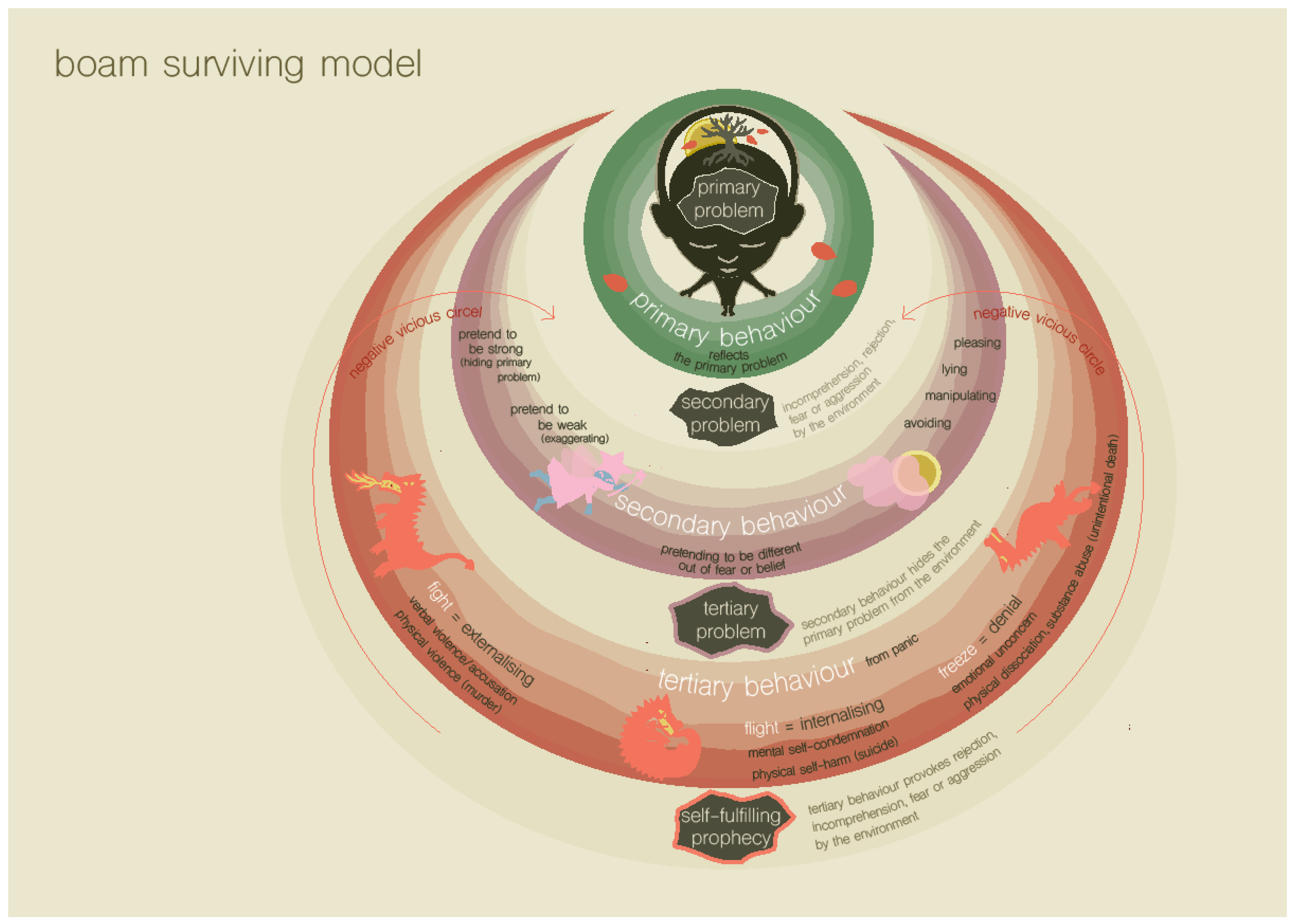
1.2.3. Step 3 of the BOAM Diagnostic Process: Recognizing the Survival Strategies and Core Needs behind Emotional and Behavioral Problems Using the BOAM Surviving Model
1.2.4. The BOAM Trajectory in a Broader Context
1.2.5. Possible Transdiagnostic Mechanisms
1.3. The Current Study
2. Methods
2.1. Participants
2.2. Procedure
2.3. Intervention
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Research Drop-Out Analysis
3.2. Feasibility and Acceptability of the BOAM Diagnostic Trajectory and Subsequent Treatment
3.3. Feasibility of Outcome Measures
3.4. Power Calculation for Future Studies
3.5. Correlations between the Outcome Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hansen, B.H.; Oerbeck, B.; Skirbekk, B.; Petrovski, B.É.; Kristensen, H. Neurodevelopmental disorders: Prevalence and comorbidity in children referred to mental health services. Nord. J. Psychiatry 2018, 72, 285–291. [Google Scholar] [CrossRef]
- O’Connor, C.; Downs, J.; Shetty, H.; McNicholas, F. Diagnostic trajectories in child and adolescent mental health services: Exploring the prevalence and patterns of diagnostic adjustments in an electronic mental health case register. Eur. Child Adolesc. Psychiatry 2020, 2, 1111–1123. [Google Scholar] [CrossRef] [PubMed]
- Barziay, R.; Calkins, M.E.; Moore, T.M.; Wolf, D.H.; Satterthwaite, T.D.; Scott, J.C.; Gur, R.E. Association between traumatic stress load, psychopathology, and cognition in the Philadelphia Neurodevelopmental Cohort. Psychol. Med. 2019, 49, 325–334. [Google Scholar] [CrossRef]
- Weems, C.F.; Russell, J.D.; Neill, E.L.; McCurdy, B. Annual research review: Pediatric posttraumatic stress disorder from a neurodevelopmental network perspective. J. Child Psychol. 2019, 60, 395–408. [Google Scholar] [CrossRef]
- Doyle, A.E.; Vuijk, P.J.; Doty, N.D.; McGrath, L.M.; Willoughby, B.L.; O’Donnell, E.H.; Wilson, H.K.; Colvin, M.K.; Toner, D.C.; Hudson, K.E.; et al. Cross-disorder cognitive impairments in youth referred for neuropsychiatric evaluation. J. Int. Neuropsychol. Soc. 2018, 24, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Abramovitch, A.; Short, T.; Schweiger, A. The C Factor: Cognitive dysfunction as a transdiagnostic dimension in psychopathology. Clin. Psychol. Rev. 2021, 86, 102007. [Google Scholar] [CrossRef]
- Caspi, A.; Houts, R.; Belsky, D.; Goldman-Mellor, S.J.; Harrington, H.; Israel, S.; Meier, M.; Ramrakha, S.; Shalev, I.; Poulton, R.; et al. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. 2014, 2, 119–137. [Google Scholar] [CrossRef] [PubMed]
- Brislin, S.J.; Martz, M.E.; Joshi, S.; Duval, E.R.; Gard, A.; Clark, D.A.; Hyde, L.W.; Hicks, B.M.; Taxali, A.; Angstadt, M.; et al. Differentiated nomological networks of internalizing, externalizing, and the general factor of psychopathology (‘p factor’) in emerging adolescence in the ABCD study. Psychol. Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Polek, E.; Neufeld, S.A.; Wilkinson, P.; Goodyer, I.; St Clair, M.; Prabhu, G.; Jones, P.B. How do the prevalence and relative risk of non-suicidal self-injury and suicidal thoughts vary across the population distribution of common mental distress (the p factor)? Observational analyses replicated in two independent UK cohorts of young people. BMJ Open 2020, 10, e032494. [Google Scholar] [CrossRef]
- Stochl, J.; Khandaker, G.M.; Lewis, G.; Perez, J.; Goodyer, I.M.; Zammit, S.; Jones, P.B. Mood, anxiety and psychotic phenomena measure a common psychopathological factor. Psychol. Med. 2015, 45, 1483–1493. [Google Scholar] [CrossRef]
- Shields, A.N.; Reardon, K.W.; Brandes, C.M.; Tackett, J.L. The p factor in children: Relationships with executive functions and effortful control. J. Res. Pers. 2019, 82, 103853. [Google Scholar] [CrossRef]
- Vanes, L.D.; Moutoussis, M.; Ziegler, G.; Goodyer, I.M.; Fonagy, P.; Jones, P.B.; Dolan, R.J. White matter tract myelin matura-tion and its association with general psychopathology in adolescence and early adulthood. Hum. Brain Mapp. 2020, 4, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Ho, B.P.; Stephenson, J.; Carter, M. Cognitive-behavioral approaches for children with autism spectrum disorder: A trend analysis. Res. Autism. Spectr. Disord. 2018, 45, 27–41. [Google Scholar] [CrossRef]
- Craig, F.; Operto, F.F.; De Giacomo, A.; Margari, L.; Frolli, A.; Conson, M.; Margari, F. Parenting stress among parents of children with neurodevelopmental disorders. Psychiatry Res. 2016, 242, 121–129. [Google Scholar] [CrossRef]
- Corbett, B.A.; Muscatello, R.A.; Klemencic, M.E.; Schwartzman, J.M. The impact of COVID-19 on stress, anxiety, and coping in youth with and without autism and their parents. Autism. Res. 2021, 14, 1496–1511. [Google Scholar] [CrossRef]
- James, A.C.; Reardon, T.; Soler, A.; James, G.; Creswell, C. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst. Rev. 2020, 2020, CD013162. [Google Scholar] [CrossRef]
- Vanheule, S. Psychiatric Diagnosis Revisited; Palgrave Macmillan: London, UK, 2017. [Google Scholar]
- Kendler, K.S. DSM issues: Incorporation of biological tests, avoidance of reification, and an approach to the “box canyon problem”. Am. J. Psychiatry 2014, 171, 1248–1250. [Google Scholar] [CrossRef]
- Dalgleish, T.; Black, M.; Johnston, D.; Bevan, A. Transdiagnostic approaches to mental health problems: Current status and future directions. J. Consult. Clin. Psychol. 2020, 88, 179. [Google Scholar] [CrossRef]
- Lingiardi, V.; McWilliams, N. (Eds.) Psychodynamic Diagnostic Manual: PDM-2; The Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Vanheule, S. Working with Clinical Case Formulations: Methodological Considerations. In Psychiatric Diagnosis Revisited; Palgrave Macmillan: London, UK, 2017; pp. 167–211. [Google Scholar] [CrossRef]
- Winters, N.C.; Hanson, G.; Stoyanova, V. The case formulation in child and adolescent psychiatry. Child Adolesc. Psychiatr. Clin. 2007, 16, 111–132. [Google Scholar] [CrossRef]
- McClain, T.; O’Sullivan, P.S.; Clardy, J.A. Biopsychosocial formulation: Recognizing educational shortcomings. Acad. Psychiatry 2004, 28, 88–94. [Google Scholar] [CrossRef]
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 50, 370–396. [Google Scholar] [CrossRef]
- Dunn, W. Supporting children to participate successfully in everyday life by using sensory processing knowledge. Infants Young Child. 2007, 20, 84–101. [Google Scholar] [CrossRef]
- De Bruin, C. The Essential 5; Graviant Publishers: Doetinchem, The Netherlands, 2012. [Google Scholar]
- Romberg, A.R.; Saffran, J.R. Expectancy learning from probabilistic input by infants. Front. Psychol. 2013, 3, 610. [Google Scholar] [CrossRef]
- Young, J.E.; Klosko, J.S.; Weishaar, M. Schema Therapy: A Practitioner’s Guide; Guilford Publications: New York, NY, USA, 2003. [Google Scholar]
- Dawson, P.; Guare, R. Executive Skills in Children and Adolescents: A Practical Guide to Assessment and Intervention; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Ivtzan, I.; Gardner, H.E.; Bernard, I.; Sekhon, M.; Hart, R. Wellbeing through self-fulfilment: Examining developmental aspects of self-actualization. Humanist. Psychol. 2013, 41, 119. [Google Scholar] [CrossRef]
- Sibley, M.H. Supporting autonomy development in teens with ADHD: How professionals can help. ADHD Rep. 2017, 25, 1. [Google Scholar] [CrossRef]
- Claudia, S.; Lucia, L. Social Skills, Autonomy and Communication in Children with Autism. Technium Soc. Sci. J. 2022, 30, 442. [Google Scholar]
- Critz, C.; Blake, K.; Nogueira, E. Sensory processing challenges in children. J. Nurse. Pract. 2015, 11, 710–716. [Google Scholar] [CrossRef]
- Ziv, Y.; Leibovich, I.; Shechtman, Z. Bullying and victimization in early adolescence: Relations to social information processing patterns. Aggress. Behav. 2013, 39, 482–492. [Google Scholar] [CrossRef]
- Hutton, P. Investigation into the Prevalence of Sensory Processing Difficulties in Children Identified as Having Behavioural, Emotional or Social Difficulties at School; Cardiff University: Cardiff, UK, 2012. [Google Scholar]
- Gourley, L.; Wind, C.; Henninger, E.M.; Chinitz, S. Sensory processing difficulties, behavioral problems, and parental stress in a clinical population of young children. J. Child. Fam. Stud. 2013, 22, 912–921. [Google Scholar] [CrossRef]
- Fox, C.; Snow, P.C.; Holland, K. The relationship between sensory processing difficulties and behaviour in children aged 5–9 who are at risk of developing conduct disorder. Emot. Behav. Diffic. 2014, 19, 71–88. [Google Scholar] [CrossRef]
- Lowe, M.X.; Stevenson, R.A.; Wilson, K.E.; Ouslis, N.E.; Barense, M.D.; Cant, J.S.; Ferber, S. Sensory processing patterns predict the integration of information held in visual working memory. J. Exp. Psychol. Hum. Percept. Perform. 2016, 42, 294. [Google Scholar] [CrossRef] [PubMed]
- Galiana-Simal, A.; Vela-Romero, M.; Romero-Vela, V.M.; Oliver-Tercero, N.; García-Olmo, V.; Benito-Castellanos, P.J.; Muñoz-Martinez, V.; Beato-Fernandez, L. Sensory processing disorder: Key points of a frequent alteration in neurodevelopmental disorders. Cogent Med. 2020, 7, 1736829. [Google Scholar] [CrossRef]
- Craig, F.; Margari, F.; Legrottaglie, A.R.; Palumbi, R.; De Giambattista, C.; Margari, L.A. Review of executive function deficits in autism spectrum disorder and attention-deficit/hyperactivity disorder. Neuropsychiatr. Dis. Treat. 2016, 12, 1191. [Google Scholar] [CrossRef]
- Aupperle, R.L.; Melrose, A.J.; Stein, M.B.; Paulus, M.P. Executive function and PTSD: Disengaging from trauma. Neuropharmacology 2012, 62, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Geier, D.A.; Sykes, L.K.; Geier, M.R.; Deth, R.C. Are ASD and ADHD a continuum? A comparison of pathophysiological similarities between the disorders. J. Atten. Disord. 2015, 19, 805–827. [Google Scholar] [CrossRef] [PubMed]
- Chu, B.C.; Temkin, A.B.; Toffey, K. Transdiagnostic mechanisms and treatment for children and adolescents: An emerging field. In Oxford Handbook Topics in Psychology; online ed.; Oxford Academic: Oxford, UK, 2014. [Google Scholar] [CrossRef]
- Ehrenreich-May, J.; Chu, B.C. Overview of transdiagnostic mechanisms and treatments for youth psychopathology. In Transdiagnostic Treatments for Children and Adolescents: Principles and Practices; Ehrenreich-May, J., Chu, B.C., Eds.; The Guilford Press: New York, NY, USA, 2013; pp. 3–14. [Google Scholar]
- Snyder, H.R.; Miyake, A.; Hankin, B.L. Advancing understanding of executive function impairments and psychopathology: Bridging the gap between clinical and cognitive approaches. Front. psychol. 2015, 6, 328. [Google Scholar] [CrossRef]
- Snyder, H.R.; Friedman, N.P.; Hankin, B.L. Transdiagnostic mechanisms of psychopathology in youth: Executive functions, dependent stress, and rumination. Cognit. Ther. Res. 2019, 43, 834–851. [Google Scholar] [CrossRef]
- Cummings, E.M.; Davies, P.T.; Campbell, S.B. Children and the marital subsystem. In Developmental Psychopathology and Family Process: Theory, Research, and Clinical Implications; The Guilford Press: New York, NY, USA, 2020; pp. 251–298. [Google Scholar]
- Holly, L.E.; Fenley, A.R.; Kritikos, T.K.; Merson, R.A.; Abidin, R.R.; Langer, D.A. Evidence-base update for parenting stress measures in clinical samples. J. Clin. Child Adolesc. Psychol. 2019, 48, 685–705. [Google Scholar] [CrossRef]
- Neece, C.L.; Green, S.A.; Baker, B.L. Parenting stress and child behavior problems: A transactional relationship across time. Am. J. Intellect. Dev. Disabil. 2012, 117, 48–66. [Google Scholar] [CrossRef]
- Truijens, D. BOAM Self-Diagnostics. New Explanatory Diagnostics for Adults and Children with Mental Health Problems, in prep.
- Omer, H. Non-Violent Resistance: A New Approach to Violent and Self-Destructive Children; Cambridge University Press: Cambridge, UK, 2021. [Google Scholar]
- Verhulst, F.C.; Van der Ende, J. Handleiding ASEBA-Vragenlijsten Voor Leeftijden 6 t/m 18 Jaar: CBCL/6-18, YSR en TRF; ASEBA Nederland: Rotterdam, The Netherlands, 2013. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Smidts, D.P.; Huizinga, M. BRIEF Executieve Functies Gedragsvragenlijst: Handleiding; Hogrefe: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Gioia, G.A.; Isquith, P.K. , Guy, S.C., Kenworthy, L. Behavior Rating Inventory of Executive Function: Professional Manual; Psychological Assessment Resources: Lutz, FL, USA, 2000. [Google Scholar]
- Veerman, J.W.; Janssen, J.; Kroes, G.; De Meyer, R.; Nguyen, L.; Vermulst, A. Vragenlijst Gezinsfunctioneren Volgens Ouders (VGFO); Praktikon: Nijmegen, The Netherlands, 2016. [Google Scholar]
- De Brock, A.J.L.L.; Vermulst, A.A.; Gerris, J.R.M.; Abidin, R.R. NOSI, Nijmeegse Ouderlijke Stress Index. Experimentele Versie. Handleiding; Swets & Zeitlinger: Lisse, The Netherlands, 1992. [Google Scholar]
- Abidin, R.R. Parenting Stress Index Manual; Pediatric Psychology Press: Charlottesville, VA, USA, 1983. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hosenbocus, S.; Chahal, R. A review of executive function deficits and pharmacological management in children and adolescents. J. Can. Acad. Child Adolesc. Psychiatry 2012, 21, 223. [Google Scholar]
- Mak, C.; Whittingham, K.; Cunnington, R.; Boyd, R.N. Efficacy of mindfulness-based interventions for attention and executive function in children and adolescents—A systematic review. Mindfulness 2018, 9, 59–78. [Google Scholar] [CrossRef]
- Pasqualotto, A.; Mazzoni, N.; Bentenuto, A.; Mulè, A.; Benso, F.; Venuti, P. Effects of cognitive training programs on executive function in children and adolescents with Autism Spectrum Disorder: A systematic review. Brain Sci. 2021, 11, 1280. [Google Scholar] [CrossRef] [PubMed]
- Takacs, Z.K.; Kassai, R. The efficacy of different interventions to foster children’s executive function skills: A series of meta-analyses. Psychol. Bull. 2019, 145, 653. [Google Scholar] [CrossRef] [PubMed]
- Racer, K.H.; Dishion, T.J. Disordered attention: Implications for understanding and treating internalizing and externalizing disorders in childhood. Cogn. Behav. Pract. 2012, 19, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Breaux, R.P.; Harvey, E.A. A longitudinal study of the relation between family functioning and preschool ADHD symptoms. J. Clin. Child Adolesc. Psychol. 2019, 48, 749–764. [Google Scholar] [CrossRef]
- Thompson, R.A. What more has been learned? The science of early childhood development 15 years after neurons to neighborhoods. Zero Three J. 2016, 36, 18–24. [Google Scholar]
- Pinquart, M.; Ebeling, M. Parental educational expectations and academic achievement in children and adolescents—a meta-analysis. Educ. Psychol. Rev. 2020, 32, 463–480. [Google Scholar] [CrossRef]
- Zimmerman, F.J.; Christakis, D.A. Associations between content types of early media exposure and subsequent attentional problems. Pediatrics 2007, 120, 986–992. [Google Scholar] [CrossRef]
- Lillard, A.S.; Peterson, J. The immediate impact of different types of television on young children’s executive function. Pediatrics 2011, 128, 644–649. [Google Scholar] [CrossRef]
- UNICEF. Advantage or Paradox? The Challenge for Children and Young People of Growing Up Urban; United Nations Children’s Fund: New York, NY, USA, 2019. [Google Scholar]
- Matson, J.L.; Kozlowski, A.M. The increasing prevalence of autism spectrum disorders. Res. Autism. Spectr. Disord. 2011, 5, 418–425. [Google Scholar] [CrossRef]
- Rehm, J.; Shield, K.D. Global burden of disease and the impact of mental and addictive disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.G. Autism and urbanization. Am. J. Public Health 2010, 100, 1156–1157. [Google Scholar] [CrossRef] [PubMed]
- van der Wal, J.M.; van Borkulo, C.D.; Deserno, M.K.; Breedvelt, J.J.; Lees, M.; Lokman, J.C.; Wiers, R.W. Advancing urban mental health research: From complexity science to actionable targets for intervention. Lancet Psychiatry 2011, 8, 991–1000. [Google Scholar] [CrossRef]
- Zhang, J.; Yan, L.; Yuan, Y. Rural-urban migration and mental health of Chinese migrant children: Systematic review and meta-analysis. J. Affect. Disord. 2019, 257, 684–690. [Google Scholar] [CrossRef]
- Schauder, K.B.; Bennetto, L. Toward an interdisciplinary understanding of sensory dysfunction in autism spectrum disorder: An integration of the neural and symptom literatures. Front. Neurosci. 2016, 10, 268. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | 7-Point Likert Scale |
|---|---|
| 1 = dissatisfied, 7 = very satisfied | |
| About the improvement, I feel… | 5.7 (1.3) |
| 1 = not suitable at all, 7 = very suitable | |
| The method (BOAM) used was… | 6.4 (.9) |
| 1 = strongly advise against, 7 = strongly recommend | |
| To what extent would you recommend BOAM to other families? | 6.3 (1.1) |
| 1 = very negative, 7 = very positive | |
| How do you feel about what you have learned? | 6.0 (1.1) |
| Question | 10-Point Likert Scale |
| 1 = not at all, 10 = very suitable | |
| In how far was BOAM suitable for the reason of referral? | 8.5 (1.5) |
| 1 = not at all, 10 very much | |
| How content were you about the therapist? | 9.2 (1.1) |
| To what extent can you use what you have learned in daily life? | 8.0 (1.2) |
| To what extend did your self-knowledge increase? | 8.2 (1.1) |
| To what extend did your confidence in the future increase? | 7.7 (1.2) |
| Outcome Variable | Pre-Test | Post-Test | 3-Month Follow-Up | |||
|---|---|---|---|---|---|---|
| n | M (SD) | n | M (SD) | n | M (SD) | |
| Primary outcomes | ||||||
| Internalizing psychopathology | 34 | 18.1 (9.1) | 20 | 13.6 (10.1) | 20 | 15.0 (10.8) |
| Externalizing psychopathology | 34 | 17.9 (10.0) | 20 | 11.6 (6.8) | 20 | 13.0 (8.7) |
| Secondary outcomes and mechanisms | ||||||
| Attention problems | 34 | 9.6 (3.6) | 20 | 8.0 (3.3) | 20 | 7.5 (3.6) |
| Executive function problems | 33 | 161.7 (18.6) | 18 | 149.9 (19.6) | 18 | 152.6 (22.9) |
| Family systemic problems | 32 | 22.6 (5.1) | 16 | 20.4 (3.8) | 15 | 18.9 (4.7) |
| Partner relationship problems | 25 | 3.7 (3.2) | 15 | 2.9 (3.3) | 13 | 3.3 (3.1) |
| Parenting stress | 33 | 88.6 (25.4) | 19 | 77.1 (20.6) | 17 | 80.2 (28.2) |
| Outcome Variable | Pre-Test–Post-Test | Pre-Test–Follow-Up | ||||
|---|---|---|---|---|---|---|
| n | 95% CI | d | n | 95% CI | d | |
| Primary outcomes | ||||||
| Internalizing psychopathology | 20 | 0.98–7.97 | 0.60 | 20 | 0.66–5.74 | 0.59 |
| Externalizing psychopathology | 20 | 1.81–8.19 | 0.73 | 20 | 1.66–7.84 | 0.72 |
| Secondary outcomes and mechanisms | ||||||
| Attention problems | 20 | 0.10–3.50 | 0.49 | 20 | 0.22–3.98 | 0.52 |
| Executive function problems | 18 | 3.85–20.81 | 0.72 | 18 | 1.17–18.33 | 0.57 |
| Family systemic problems | 16 | 0.54–5.58 | 0.65 | 15 | 0.18–6.75 | 0.58 |
| Partner relationship problems | 15 | 0.14–2.05 | 0.64 | 12 | −0.05–1.30 | 0.59 |
| Parenting stress | 19 | 6.48–21.72 | 0.89 | 17 | 0.13–22.98 | 0.52 |
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | |
|---|---|---|---|---|---|---|---|
| Primary outcomes | |||||||
| 1. Internalizing psychopathology | - | 0.30 | 0.15 | 0.26 | 0.23 | 0.32 | 0.39 |
| 2. Externalizing psychopathology | - | - | 0.27 | 0.55 | 0.34 | 0.28 | 0.75 |
| Secondary outcomes and mechanisms | |||||||
| 3. Attention problems | - | - | - | 0.39 | 0.16 | 0.08 | 0.28 |
| 4. Executive function problems | - | - | - | - | −0.05 | 0.19 | 0.60 |
| 5. Family systemic problems | - | - | - | - | - | 0.37 | 0.39 |
| 6. Partner relationship problems | - | - | - | - | - | - | 0.39 |
| 7. Parenting stress | - | - | - | - | - | - | - |
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | |
|---|---|---|---|---|---|---|---|
| Primary outcomes | |||||||
| 1. Internalizing psychopathology | - | 0.62 | 0.68 | 0.38 | 0.37 | 0.03 | 0.52 |
| 2. Externalizing psychopathology | - | - | 0.49 | 0.69 | 0.28 | 0.09 | 0.53 |
| Secondary outcomes and mechanisms | |||||||
| 3. Attention problems | - | - | - | 0.40 | 0.52 | 0.32 | 0.66 |
| 4. Executive function problems | - | - | - | - | 0.35 | 0.04 | 0.69 |
| 5. Family systemic problems | - | - | - | - | - | 0.63 | 0.54 |
| 6. Partner relationship | - | - | - | - | - | - | 0.23 |
| 7. Parenting stress | - | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potharst, E.S.; Truijens, D.; Seegers, I.C.M.; Spaargaren, J.F.; van Steensel, F.J.A.; Bögels, S.M. BOAM: A Visual, Explanatory Diagnostic and Psychoeducation System Used in Collaboration with Families—Feasibility and Acceptability for Children Who Are Non-Responsive to Treatment as Usual. Int. J. Environ. Res. Public Health 2022, 19, 14693. https://doi.org/10.3390/ijerph192214693
Potharst ES, Truijens D, Seegers ICM, Spaargaren JF, van Steensel FJA, Bögels SM. BOAM: A Visual, Explanatory Diagnostic and Psychoeducation System Used in Collaboration with Families—Feasibility and Acceptability for Children Who Are Non-Responsive to Treatment as Usual. International Journal of Environmental Research and Public Health. 2022; 19(22):14693. https://doi.org/10.3390/ijerph192214693
Chicago/Turabian StylePotharst, Eva S., Damiët Truijens, Isabelle C. M. Seegers, Julia F. Spaargaren, Francisca J. A. van Steensel, and Susan M. Bögels. 2022. "BOAM: A Visual, Explanatory Diagnostic and Psychoeducation System Used in Collaboration with Families—Feasibility and Acceptability for Children Who Are Non-Responsive to Treatment as Usual" International Journal of Environmental Research and Public Health 19, no. 22: 14693. https://doi.org/10.3390/ijerph192214693
APA StylePotharst, E. S., Truijens, D., Seegers, I. C. M., Spaargaren, J. F., van Steensel, F. J. A., & Bögels, S. M. (2022). BOAM: A Visual, Explanatory Diagnostic and Psychoeducation System Used in Collaboration with Families—Feasibility and Acceptability for Children Who Are Non-Responsive to Treatment as Usual. International Journal of Environmental Research and Public Health, 19(22), 14693. https://doi.org/10.3390/ijerph192214693