


Best Practices from Eight European Dementia-Friendly Study Cases of Innovation


Abstract
1. Introduction
2. Materials and Methods
2.1. Selection of Study Cases
2.2. Visits and Data Collection
- Review of existing guidelines, national, and local plans that promote ‘dementia-friendly communities and cities’ or ‘dementia-friendly’ initiatives’.
- Guided visits to the building or project. In the case of buildings, analysis and observation of the urban environment and outdoor spaces were undertaken. The observation technique consisted of ‘procedures and instruments that are used by the researcher in order to experience social realities, as well as seeing the people in their usual context where they usually develop their routines, including the social, cultural, and physical environment’ [24]. All the visits included a non-participatory observation that consisted of a guided visit with complementary information about their functioning and programs. Pictures were taken under the consent of the responsible person, otherwise public media were used.
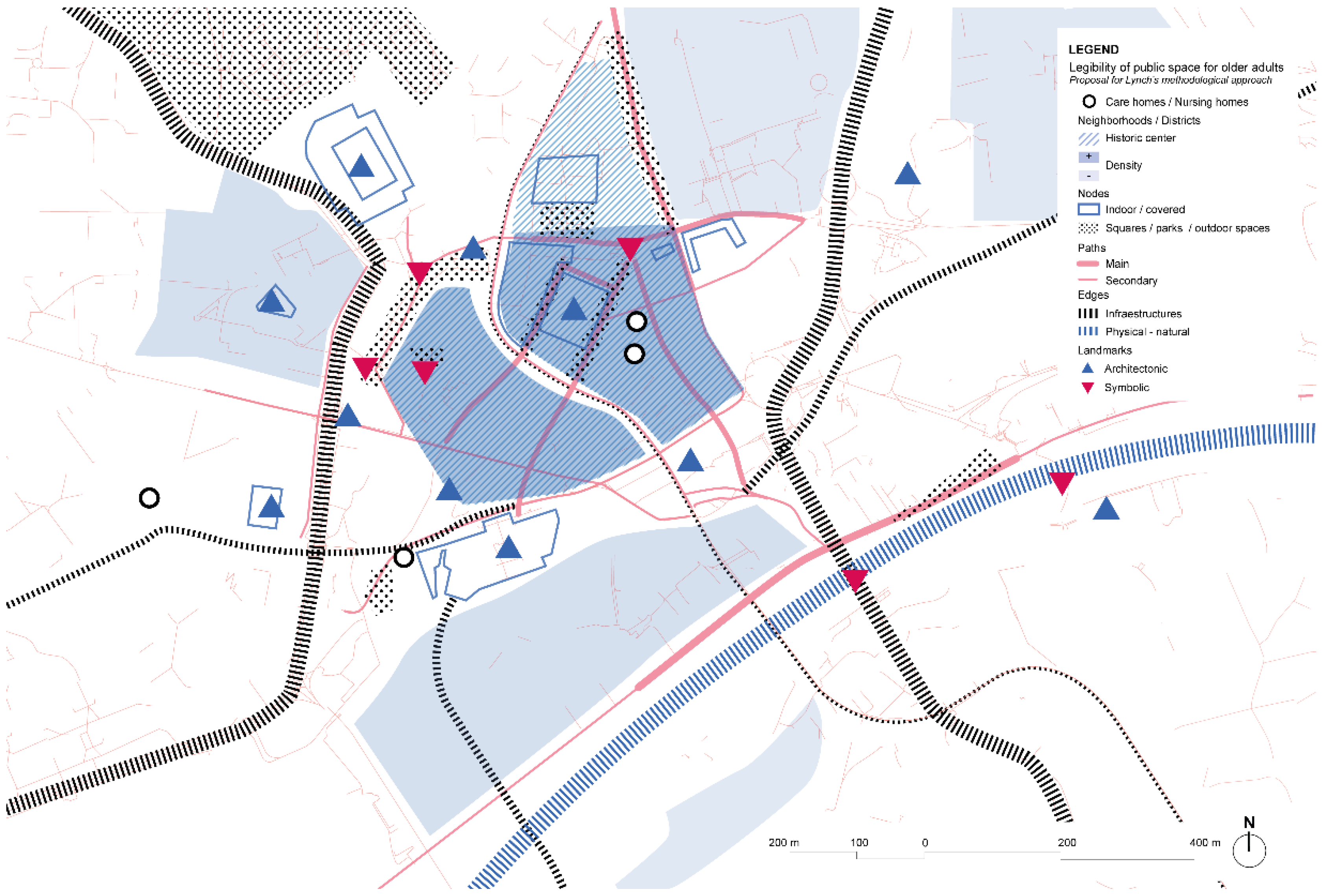
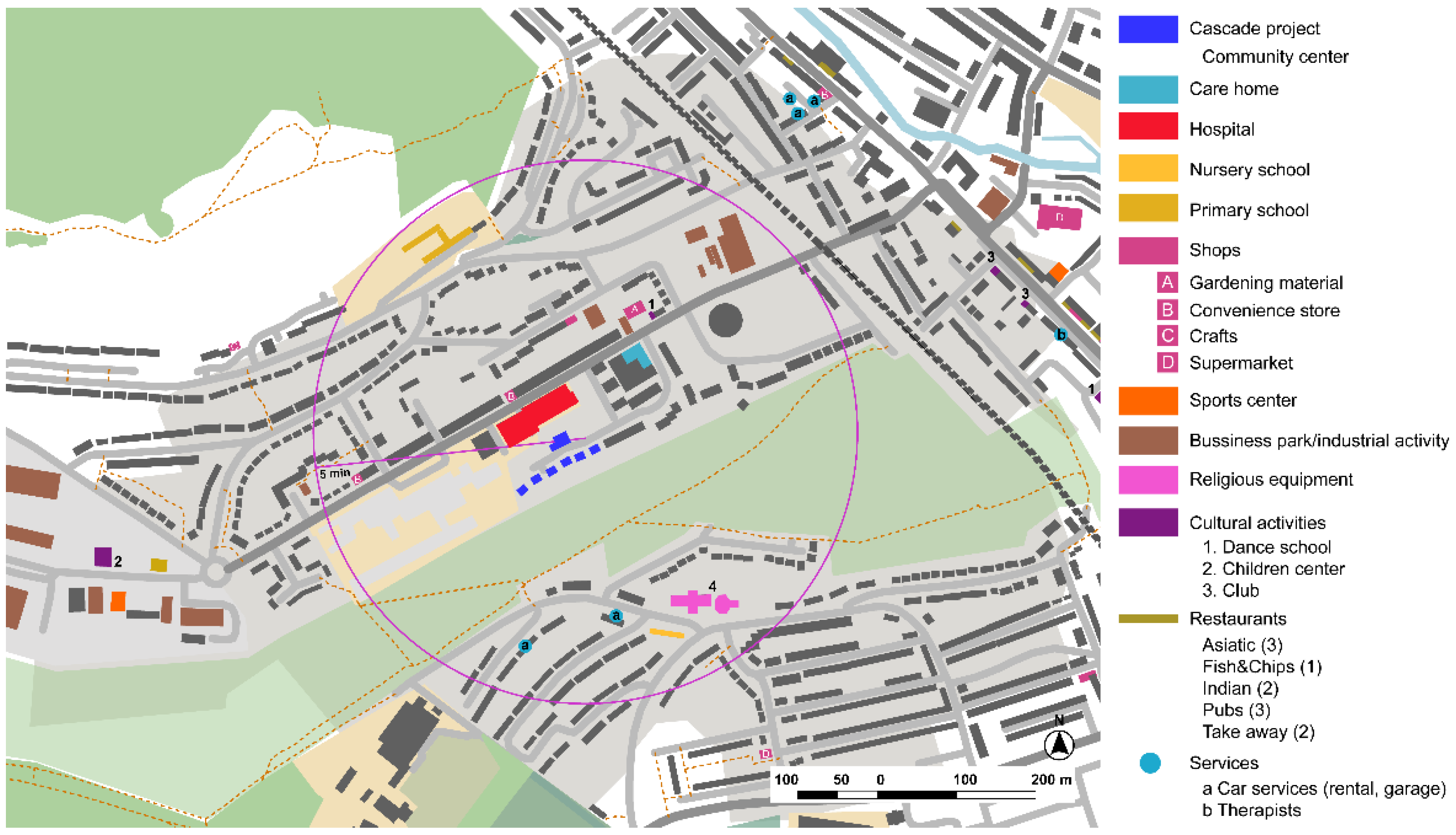
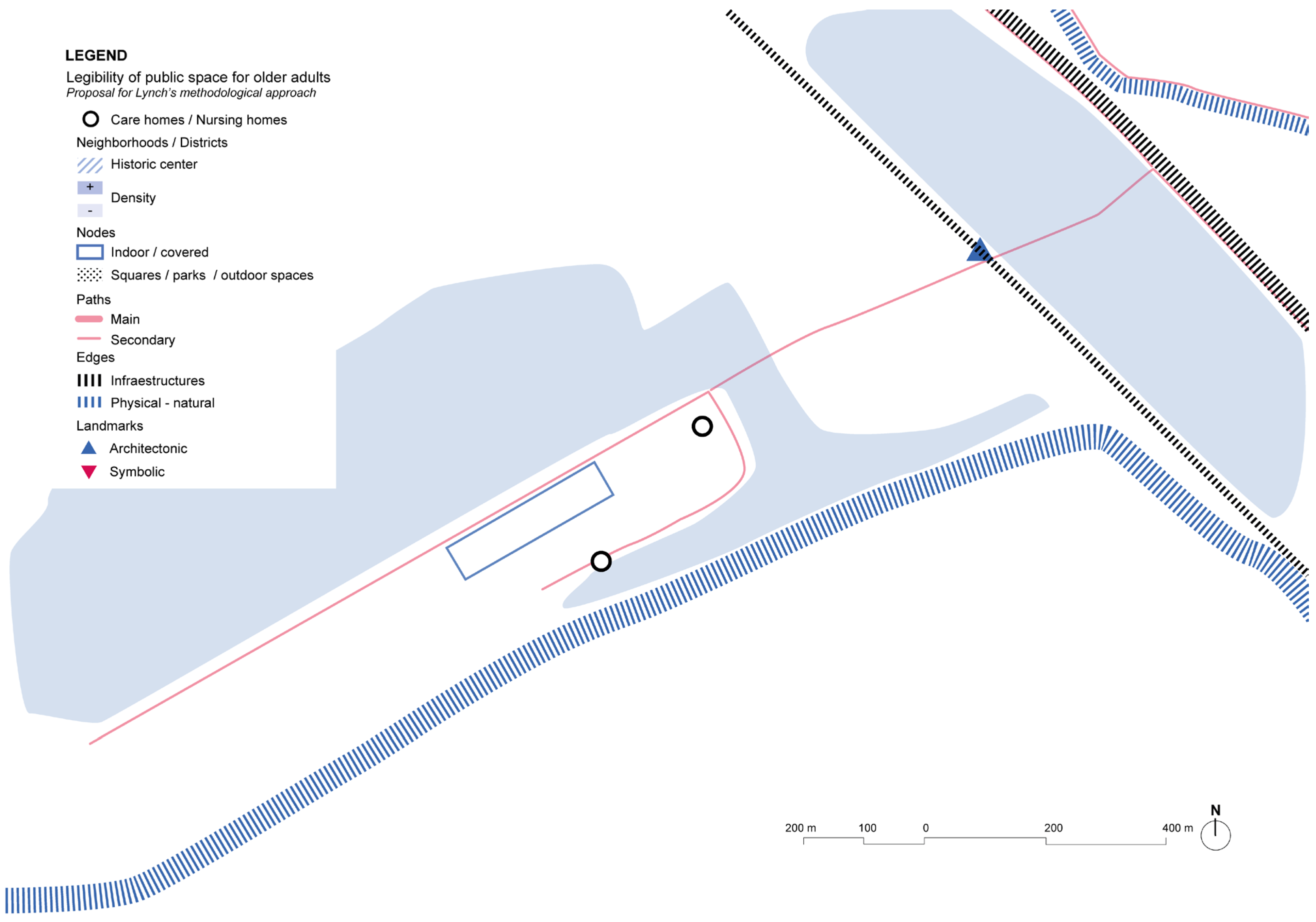
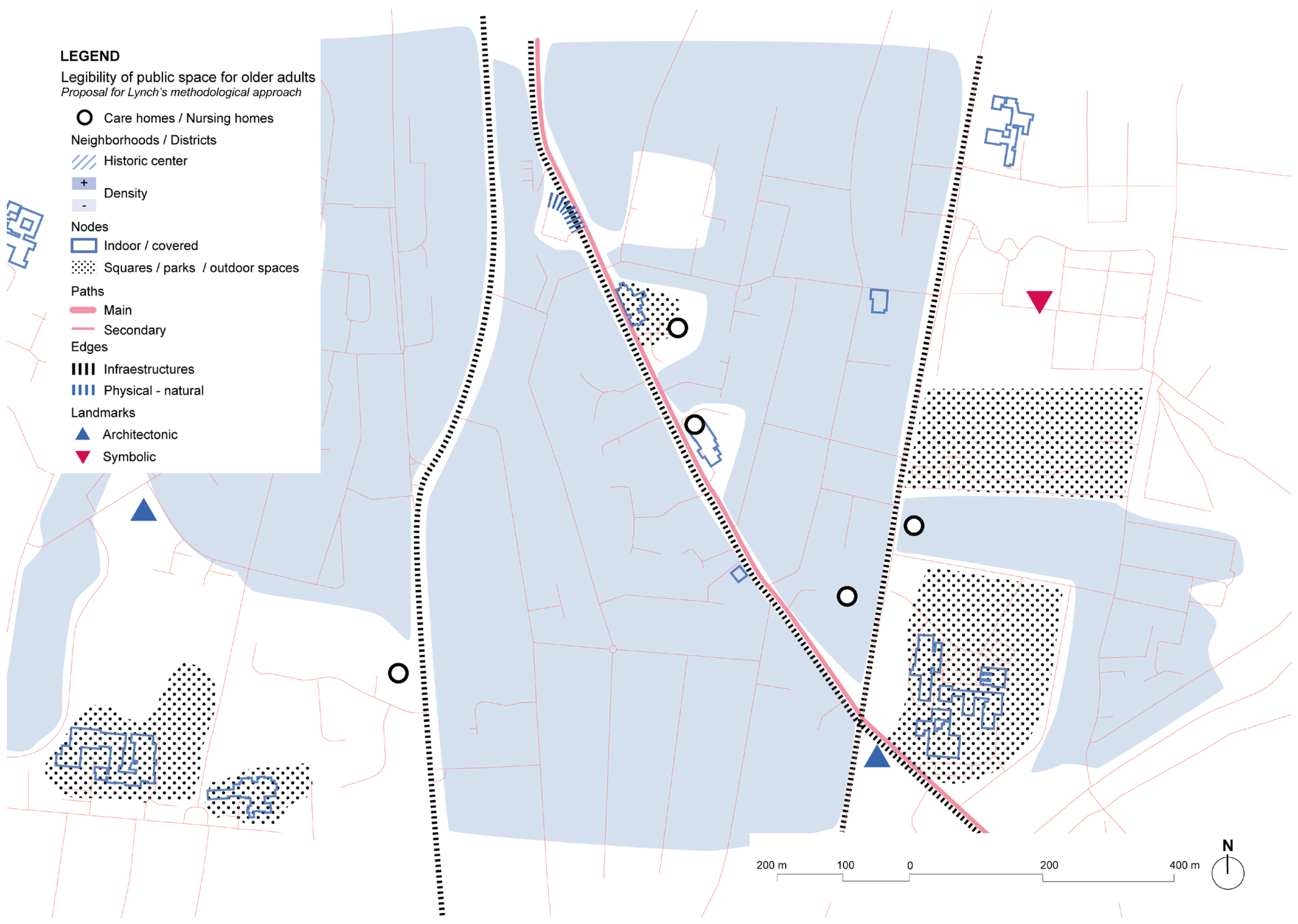
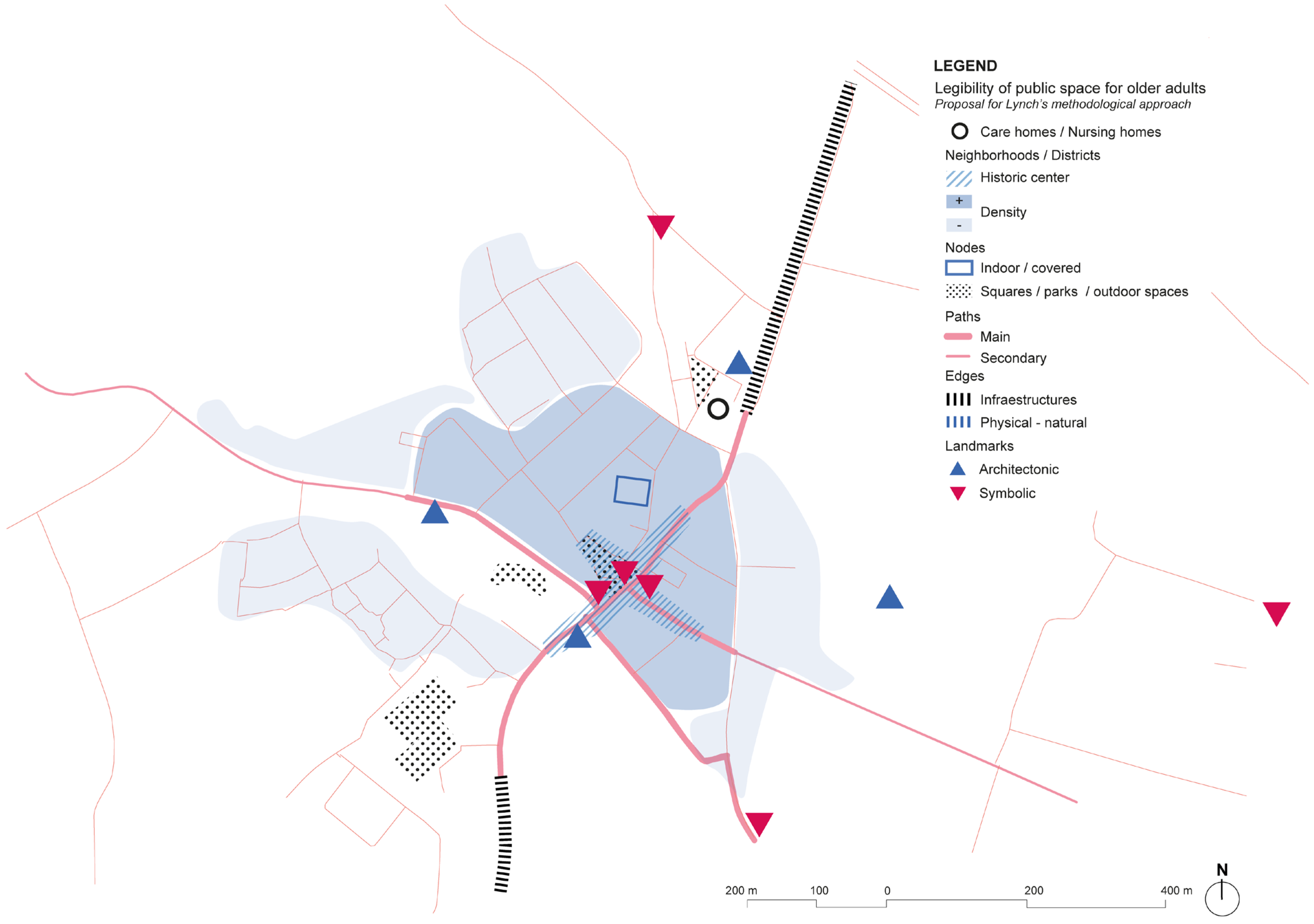
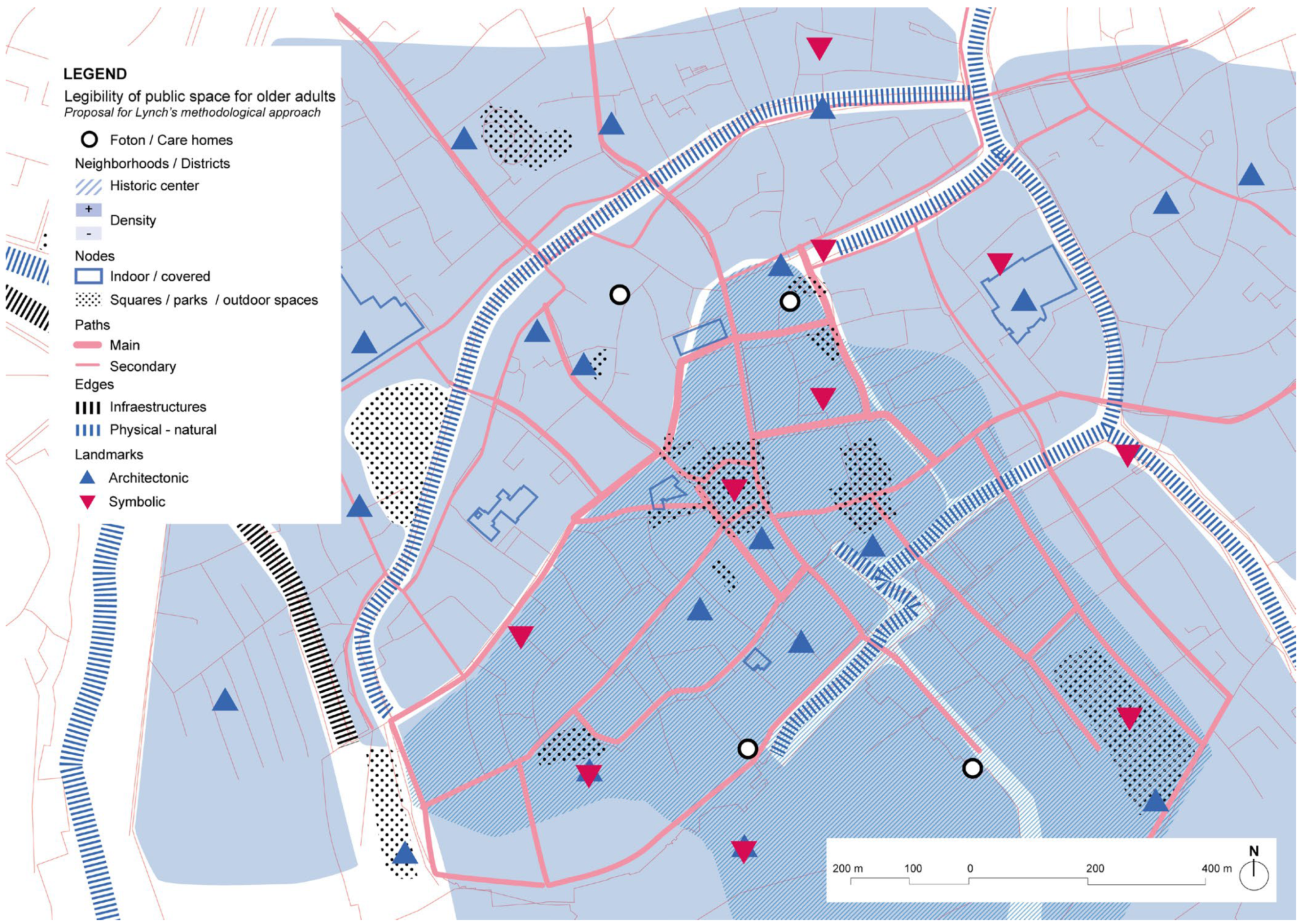
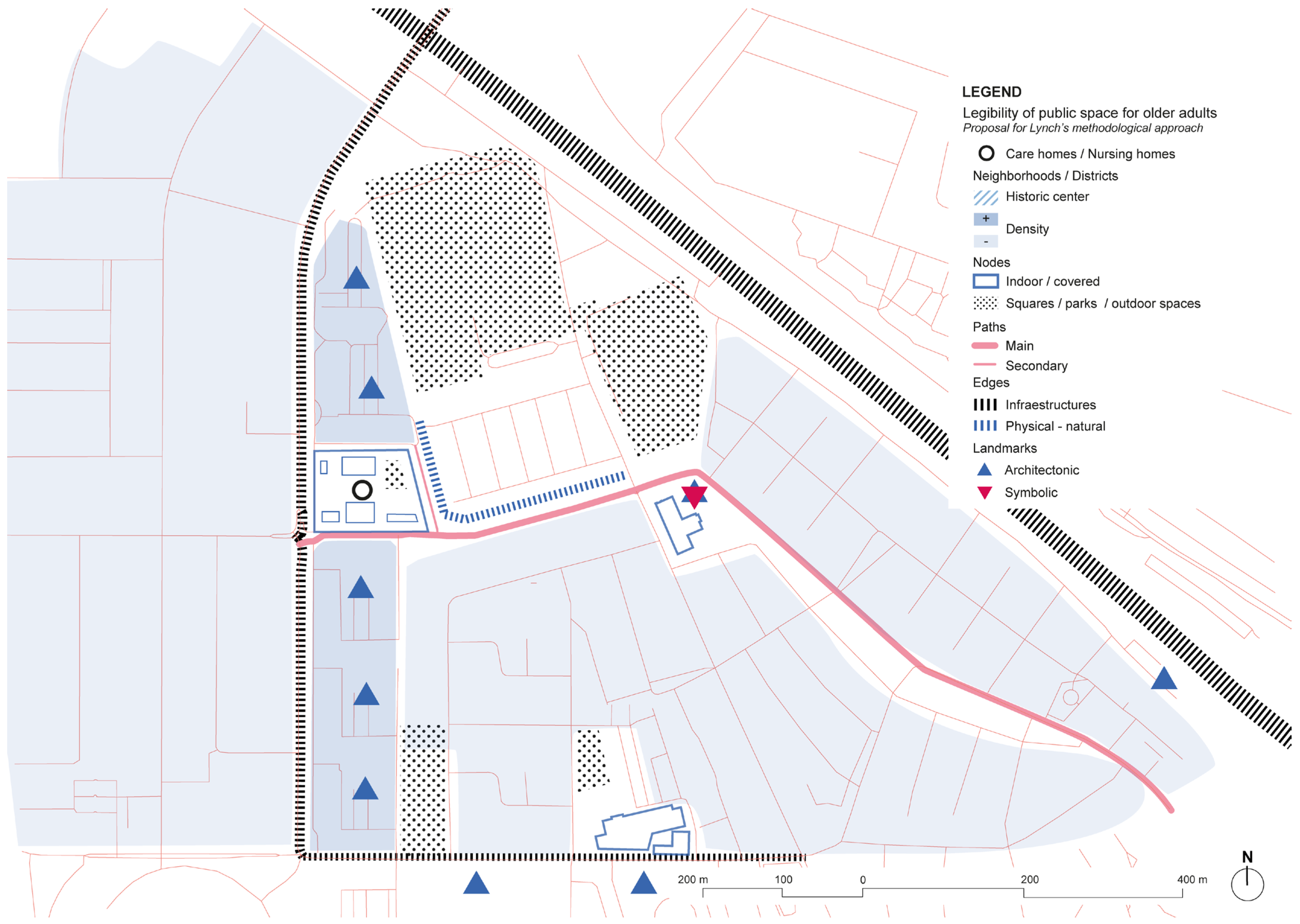
- Cartographic drawings of each study case that were based on the key elements of Lynch were developed in order to understand the different urban contexts regarding both positive and negative aspects of building a dementia-friendly environment and facility.
- Semi-structured interviews with the responsible person (before and after the visit). According to Zarco et al. (2019) [24], interviews have the main objective of ‘establishing a dialogue that enables obtaining deeper information about the contexts’. Although the content of the interviews was designed following common criteria and structure, the different typologies and contexts of each project made it necessary to adapt it to each specific case, in order to consider the particular aspects of their best practice.
- The information was systematically analyzed in different categories to describe and identify the main elements that have been considered to create dementia-friendly environments.
- Finally, secondary resources were consulted in order to complete some missing information.
2.3. Interviews
3. Results
3.1. United Kingdom
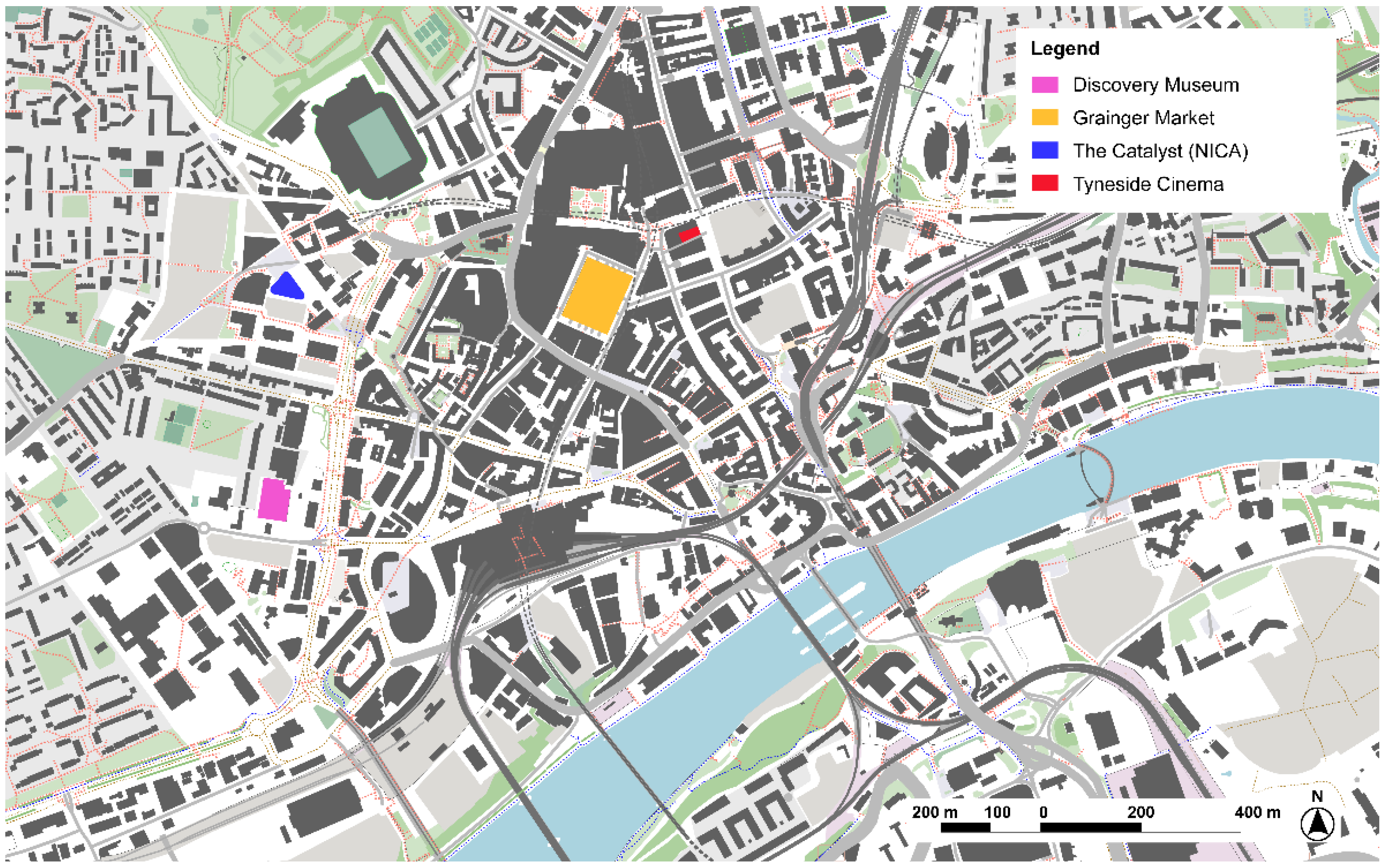
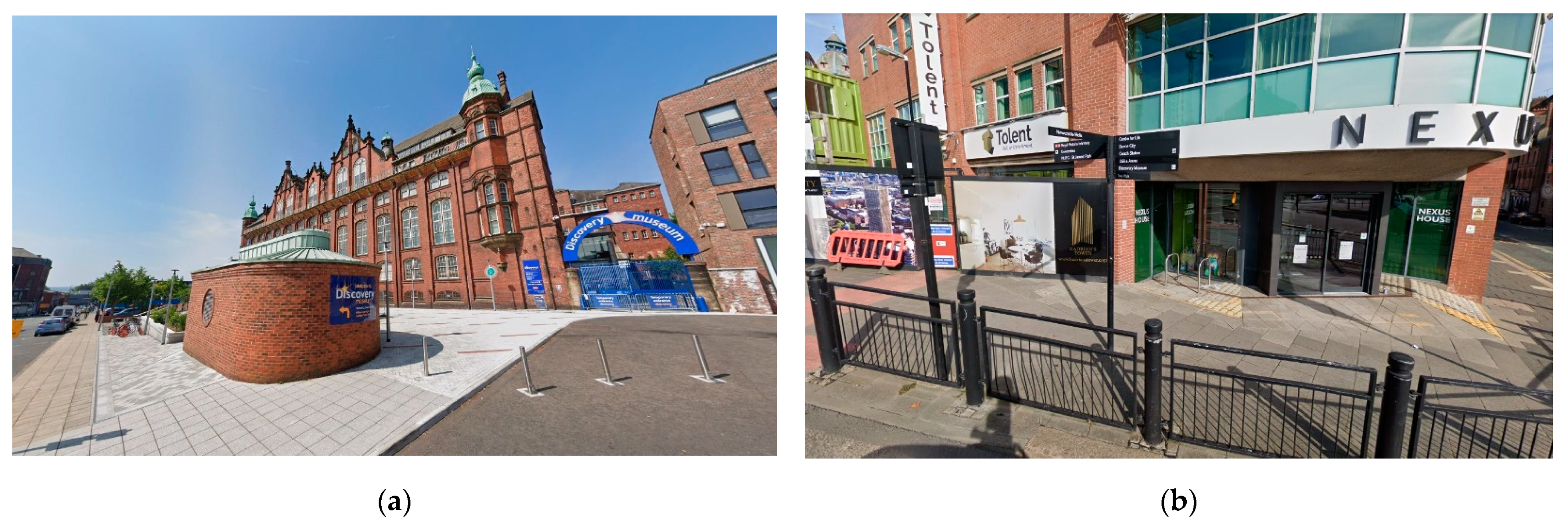
3.1.1. Discovery Museum, Newcastle-upon-Tyne
‘We have trained the staff up to be dementia-friends, so they’ve just got that little bit extra knowledge. So, if people with dementia are coming into the museum, the staff understand a little bit more and hopefully have a little bit more confidence to deal with anyone that needed help’.
‘I would say I’ve got a lot of relationships with people like dementia care in Newcastle and Age UK. And they’re the ones who bring groups to me, but I also go and see them, so because I’ve got these good relationships with the members of staff, I’ll see them once a month. So, I think next week dementia care is coming in again. And I’ll take them around to the gallery or I’ll sit with some of the objects and things and Age UK, we’ve got… it’s a group called The Time Travellers. They called themselves The Time Travellers because they didn’t want to be known as the Age UK dementia group (…) we look at different periods of time and so that’s again once a month and they will meet in the museum with myself and I’ll do some sort of topic (…) that used to be once a week and so, I used to see this group once a week, which was great. The group got to know each other, they’d be seeing each other outside of the group, there were all people with early-stage dementia and their caregivers and so, they were making friends and I was seeing them like once a week’.
3.1.2. Harmonia Village, Dementia Village, CASCADE Project, Dover
‘We have been looking for other facilities, we know the necessities for the residents very well. We know the case of De Hogeweyk in Holland for long time, but it’s very expensive. (…) We could not replicate all the services in the community inside the walls (…) And we felt that was quite isolating. We want people to use the community facilities and become more normal for people with dementia to be in the community’.
‘It’s only when they deviate from the norm when you go and have a look at what’s happened. So, once we’ve got that profile for each person the system will monitor them on an ongoing basis and then on a weekly or monthly basis… and the clinical staff will look at the information and they’ll see what sort of correlations there are and trends’.
‘One of the things we’re measuring here is the economic impact of this facility on the local community. So, the construction contract was only open to local companies. We’re basically employing local people and all the technology, everything we’re using is locally sourced (…) instead of having a hairdresser’s in here, or a cinema…we’re going to go out and use those services in the local community. And thereby have a beneficial economic impact also’.
3.1.3. Harmony House, Respite Home, CASCADE Project, Rochester
‘One of the aspects that we wanted to look at (…) was focusing on healthcare professionals (…) care professionals, such as the voluntary sector colleagues, the charity sector, the local authority (…), and then, our European colleagues had brought in the aspect of tourism, which was something we’d not thought of at all. However here in Rochester we’re in a really good spot for tourism. We have Dickens (…), there’s a castle, there are museums, we have the dockyard down the road, we have access to other places such as Leeds castle (…) just because somebody’s got dementia doesn’t mean to say they can’t ever go on holiday again’.
‘As well, we did have some pushback from the local residents, we had a couple of local residents’ meetings, we invited them to look at plans (…) but people didn’t understand what we were trying to do and came with preconceptions of what they thought dementia was’.
‘She’s not a nurse, has no nursing experience at all (…) what we wanted was somebody that shared our enthusiasm for the project (…) with the whole of the team we recruited for values more than skills. (…) We have two senior personal assistants, and we have seven personal assistants and a number of those have not come from care, which is great I think… (…) because we’re not about caring we want to be about enabling’.
‘Sometimes we really focus on risk too much. So, in terms of public spaces (…) we’ve got some really nice public spaces in Medway, some really nice garden areas, but a lot of them have little gates on them and for somebody living with dementia that is a nightmare. It’s bad enough if you haven’t got dementia and you don’t know how to get in (…) the accessibility in terms of being able to actually enter that space in the first place is really difficult and quite challenging’.
3.2. Belgium
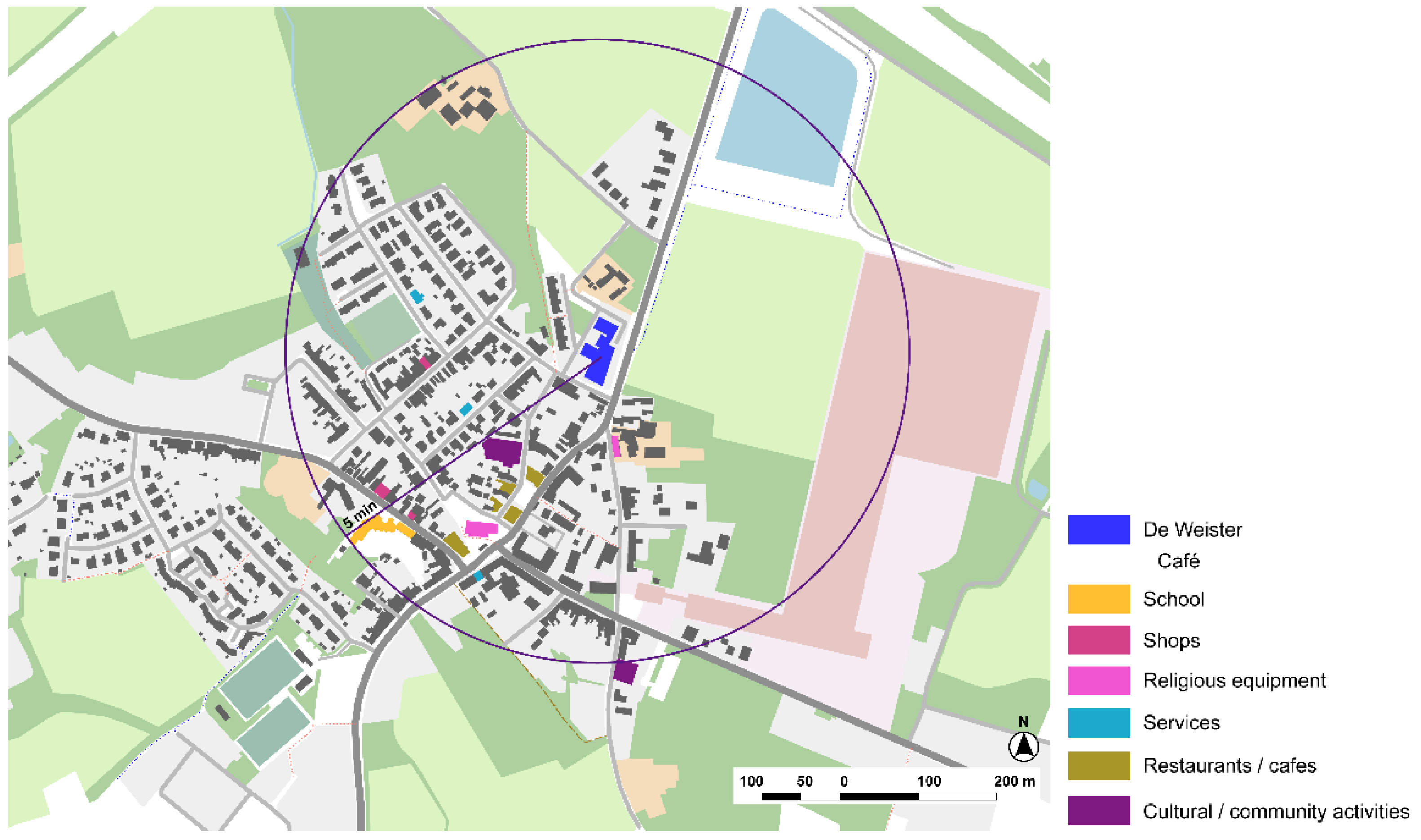
3.2.1. Woonzorgcentrum (WZC) De Weister, Nursing Home, Aalbeke, Kortrijk
‘It’s all about stigma, acceptance… and if you can create this, then you have a dementia-friendly community (…) So, the first thing is that we have to create citizenship, so it is about making people part of a community (…); the second thing is getting rid of the stigma. And then a healthy mind in a healthy body (…) so, health promotion’.
‘We create a social context so people can meet and that’s in our living rooms (…) we really live in the living room with the kitchen, we cook together with the residents, so we create a relational context or a social context where people can meet. It’s not because you’re in a nursing home you’re staying in your room. We live together, okay? But there’s free choice’.
‘… the intergenerational move garden (…) the aim was to make people move, improve intergenerational contacts through movement, but also through music. Because music is also very important for people with dementia. (…) we worked also together with the local community, and we chose those things to move (…)’.
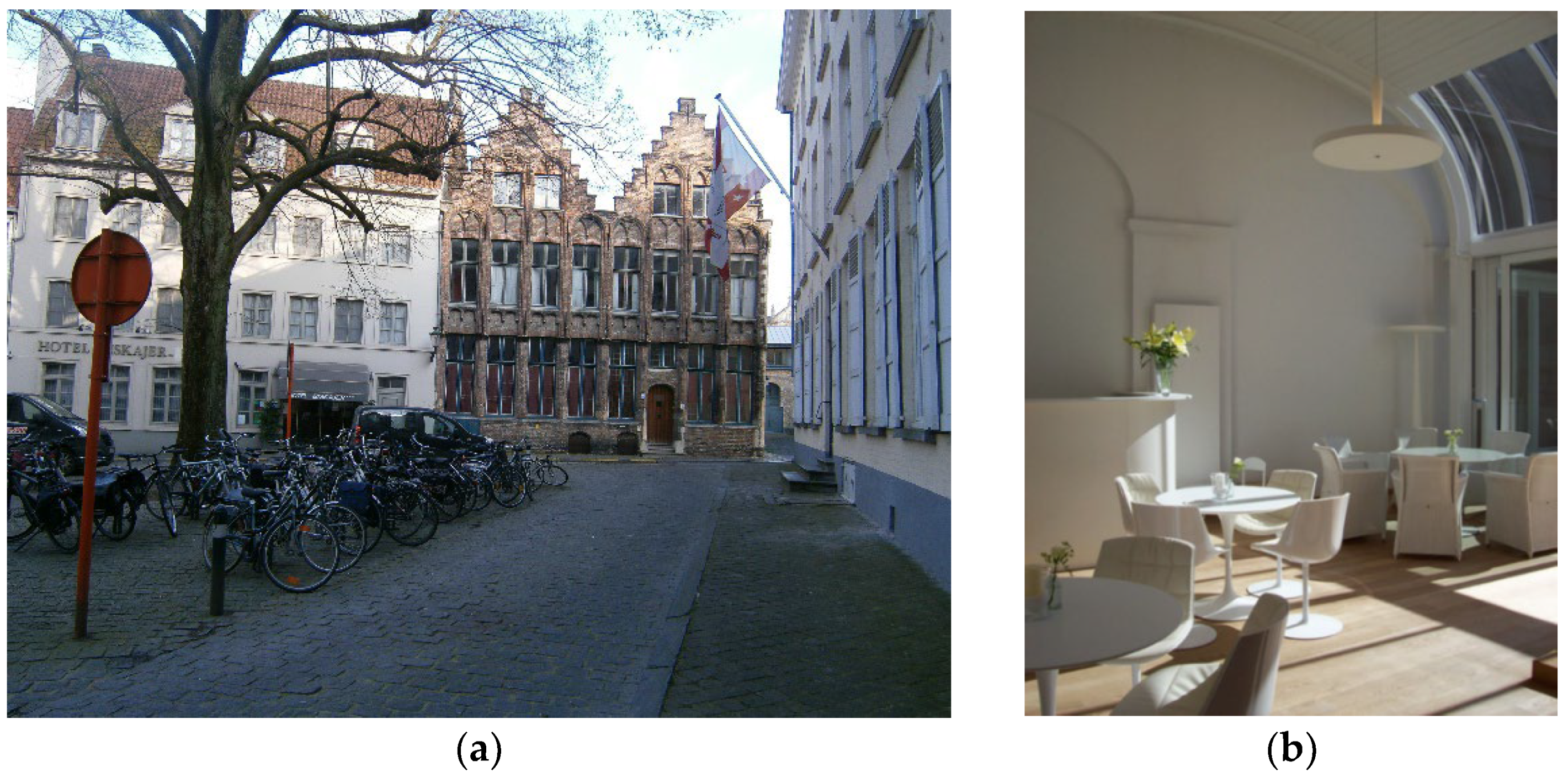
3.2.2. Foton, Expertise Center of Dementia of Flanders, Bruges
‘We have made a movie, where some of the persons that come here acted to make a movie to show to the other people who are working in the shops how you can communicate with people with dementia. (…) So, they had the opportunity to have a few evenings that they can talk about it. So, for the whole city, it was a little bit much. So, the group of volunteers went to a few streets and they visited the shop owners or the people who work in the shop to talk about the initiative, to give a sticker. So some people were ready to put it on the window, other people say ‘oh, we will do it’. And they don’t do it (…). That’s why at one shop you can see them, at the other not… (…) But there has also have been a campaign for the pharmacist. (…) So, one day they distribute the information (…) there are a lot of people of the of the area who come to the pharmacy…’.
‘You cannot call it café, but it’s a quiet place, where you can drink something, where you can have a chat also, what are lonely people, most of them are people who don’t have too much family, or they have a disease… or some little problem. They come here and they can have a cup of coffee or tea’.
3.2.3. Huis Perrekes, Osterloo, Geel
‘… All the people that live here or stay here for short stay… we know the whole continuum of the possibilities they all have after a dementia diagnosis (…). In this group, it’s very heterogeneous so there is a very big mix of types of dementia stages, so it’s not only for older people with dementia, but also for young people with dementia. It’s a mix, we don’t have a separate group because we think every person with dementia needs a care (…) which is individually adapted and (…) no matter the age. So, in every house live about 15 or 16 people with dementia and every group is heterogeneous. It’s not that people have to move from the house when they develop further in their process. (…) It’s a choice to do. It’s like this because then people can manage and mean more for each other…’.
‘We try to reach out by doing things that we do in the Huis Perrekes like the choir, all things that we do with textiles, but also (…) we organize readings or organize exhibitions, a lot of things where we invite families and people from the neighborhoods and that’s also why the garden is open, the gate is always unlocked, not during the night. So people who work or walk or bike in the neighborhood, they can come in, and they walk here and take a rest. The toilets of the building, they are also always open, so people always can… or, for example in summer, we had a freezer in the garden house (…) we put a board outside you can buy glace here and then people could walk by come in take a glace…’.
3.3. The Netherlands
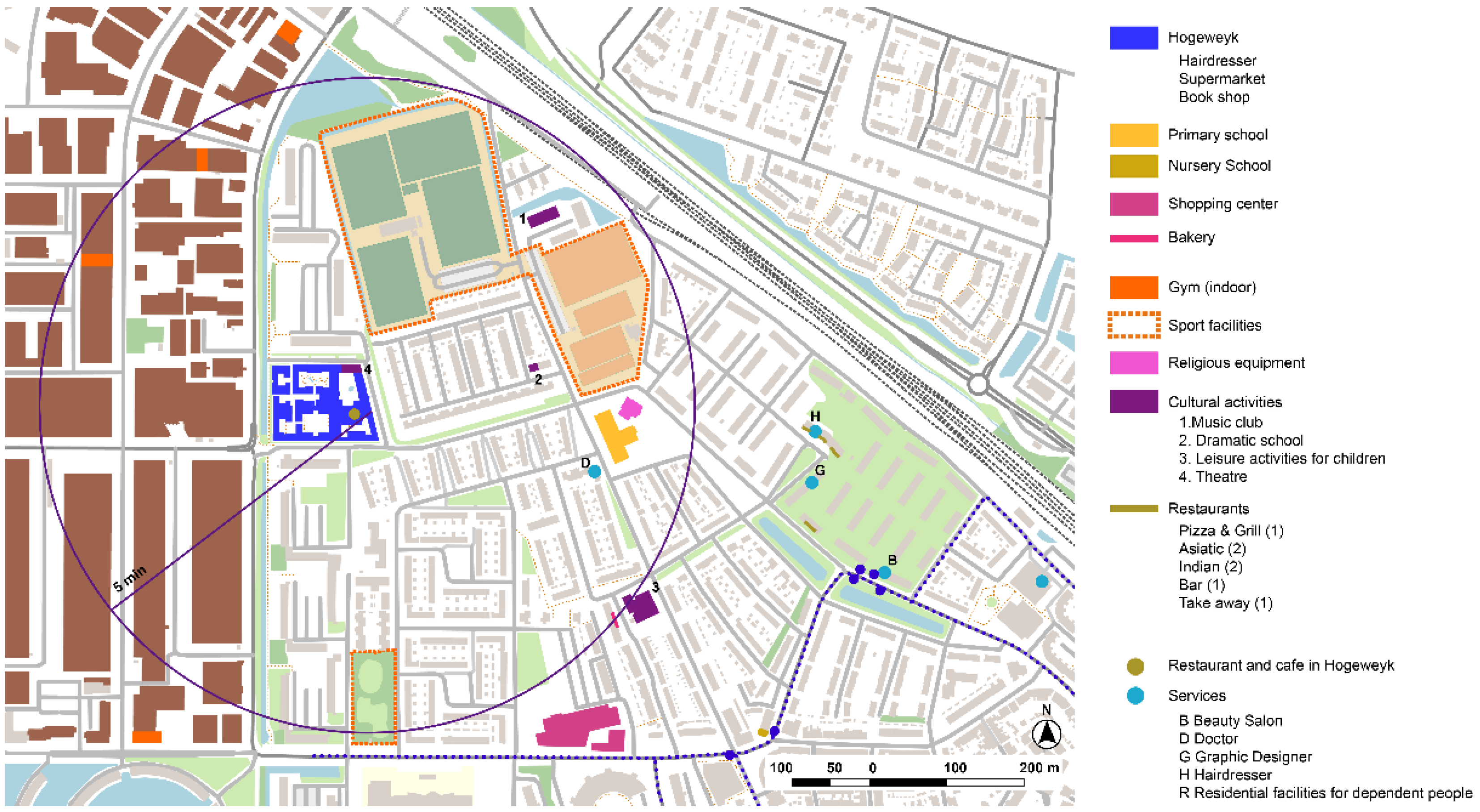
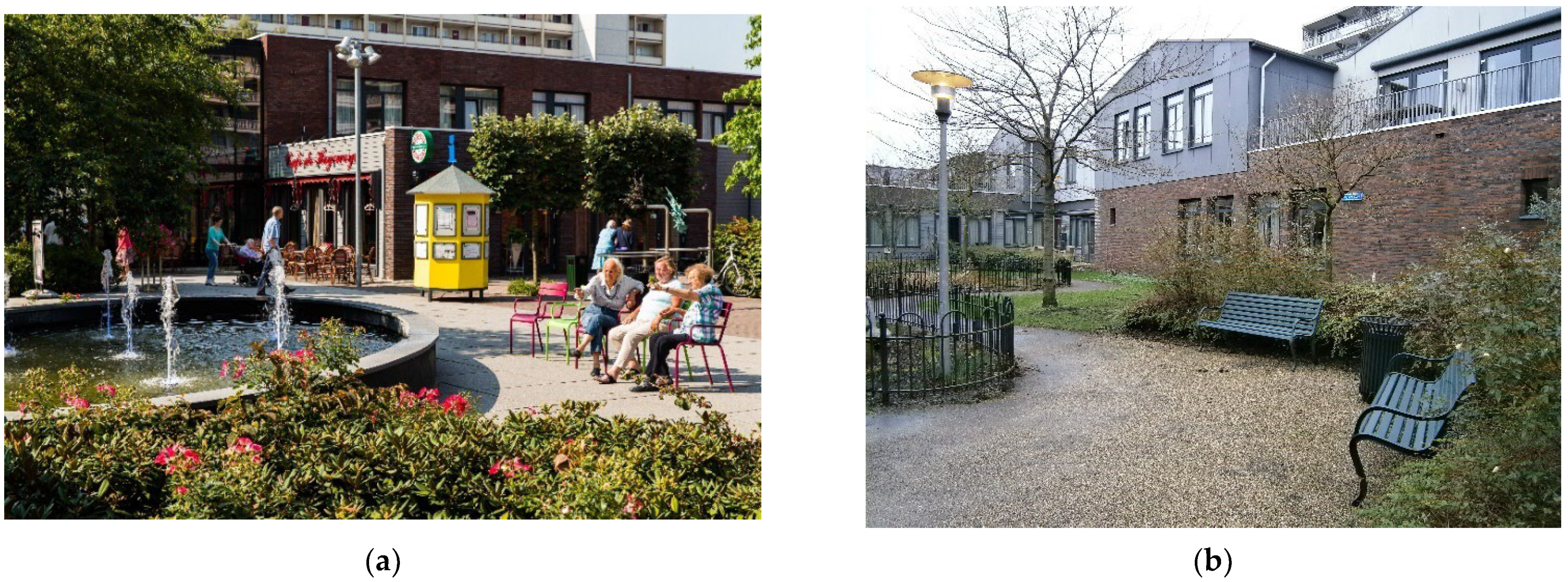
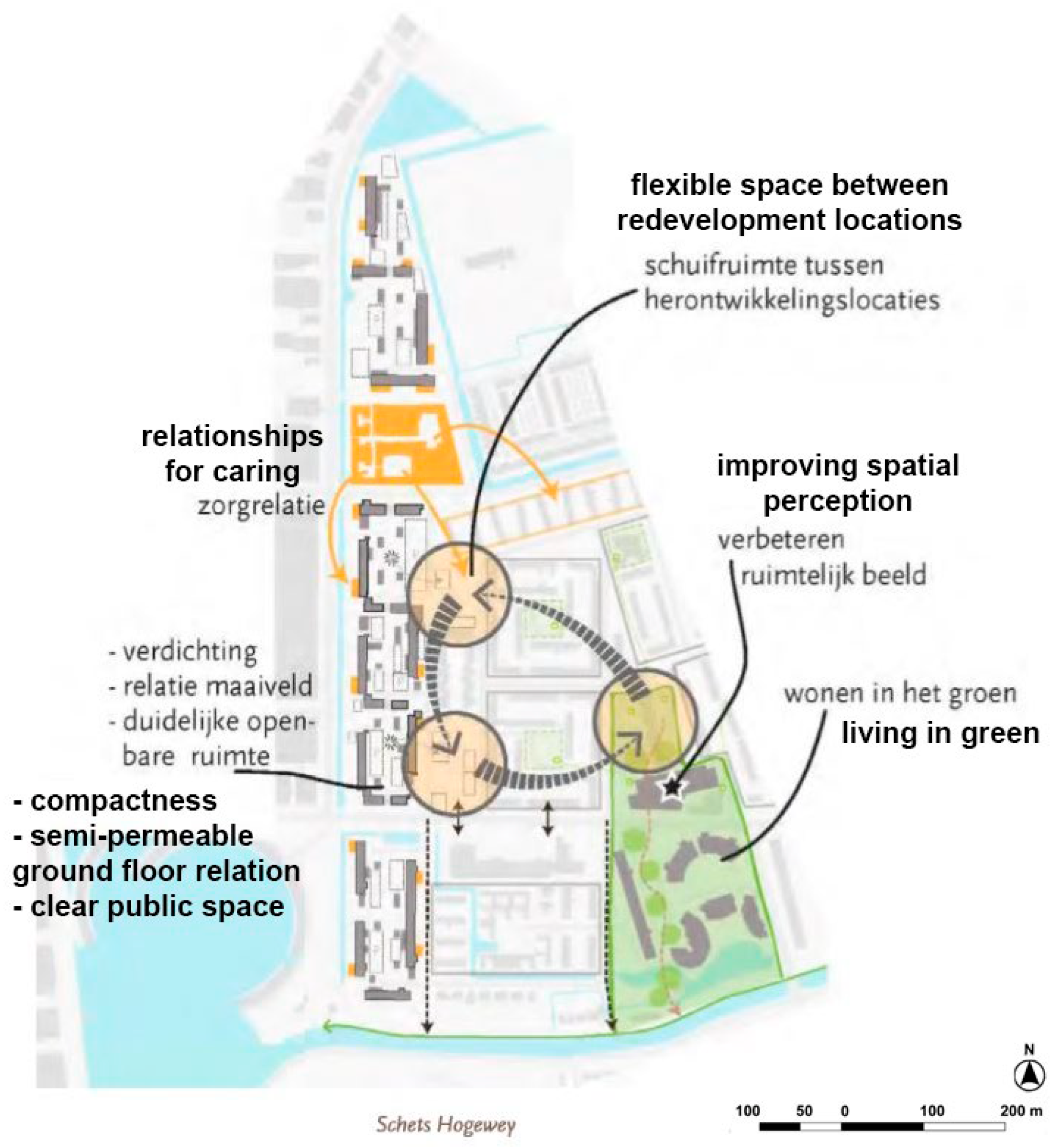
3.3.1. De Hogeweyk, Dementia Village, Weesp
‘…Everybody was living together towards a small group with like-minded people, so we developed the lifestyles, so we matched people in a group of 11 people where we brought back the normal daily living activities (…) We made a supermarket in that old building so you could go to the supermarket, we created club rooms and an event office outside the wards, so you have to go to your club event (…) You make your individual choice, you go to a club, to a place where you meet other people, where you do nice things you like. It’s your personal choice to go over there (…). We moved from 3 groups of 11 with wards, towards a house for 6, 7, or 8 people. You have immediately the quietness of a normal house where you have your own front door, where you go inside and nobody else comes there, unless you have to do something there (…) Wards give a lot of rumor noises, you don’t recognize people (…) You reduce the stress of 11 to 8 (…) And you reduce a lot of the stress and agitation because it’s a home, it’s a real house instead of a living room with wards. And a front door you can step outside, and you really walk outside, and it reduces also stress’.
‘So we must go back to what human beings really want and need and then apply the right support for the disease and those outcomes (…) if you compare the place at home—because the policy in The Netherlands is stay at home as long as possible—with good support, health support, home care support, etc… but in the end, for a person living with dementia that apartment or that house is often a cage, it’s closed, and the relative wants to keep mum or dad inside because outside it’s unsafe. And mum will walk away and so, mum is locked up (…) so, mum becomes aggressive or is lying (…) And here you get more freedom and you can you get 24 × 7 professional support so you see a different mum often here (…) Challenging behavior—behavior we don’t understand—is still part of what we have to deal with, we still have a locked door over there which I don’t like, so I hope with the new law implemented in The Netherlands we can unlock the door, but officially according to the Dutch law, residents who are living here, patients are our responsibility, so they are not allowed to leave De Hogeweyk without somebody else. Of course, they leave a lot, they go on bus trips, on a walk and a bike tour, etc., but always with somebody else’.
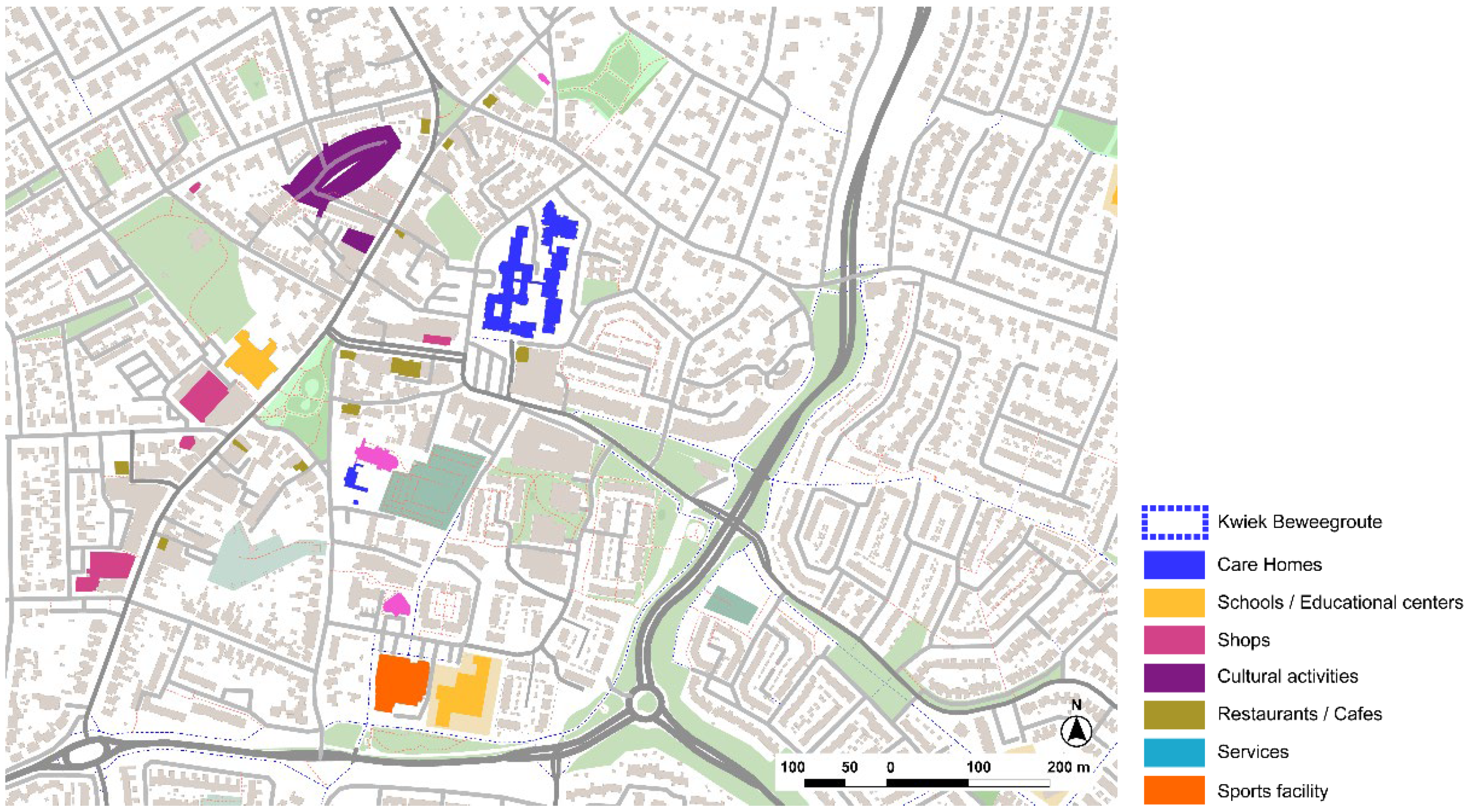
3.3.2. Kwiek Beweegroute, Nuenen, Eindhoven
‘The first question came from the community of Eindhoven to say “OK, we have so many designers in the city, we have some social issues. Let’s define a project. We have in this case, senior neighborhoods where the percentage of seniors is very high”. We had several teams of designers that got into one neighborhood and the subject of the call was public space and seniors. And you had to design a public space not even maybe the most necessary but come with a project that helps society or covers certain issues’.
‘The feeling of being engaged in something constructive and built together that they are part of, and they can use the public space through an interesting itinerary that can be something for them that makes them more inclusive’.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alzheimer Disease International. Dementia Friendly Communities-Key Principles; Alzheimer Disease International: London, UK, 2016; Volume 16. [Google Scholar]
- Alzheimer’s Society Dementia-Friendly Communities. Available online: https://www.alzheimers.org.uk/get-involved/dementia-friendly-communities/what-dementia-friendly-community (accessed on 8 September 2022).
- WHO. Towards a Dementia-Inclusive Society: WHO Toolkit for Dementia-Friendly Initiatives (DFIs); World Health Organization: Geneva, Switzerland, 2021; Volume 65. [Google Scholar]
- WHO Dementia-Friendly Initiatives. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/5206 (accessed on 8 October 2022).
- Shannon, K.; Bail, K.; Neville, S. Dementia-Friendly Community Initiatives: An Integrative Review. J. Clin. Nurs. 2019, 28, 2035–2045. [Google Scholar] [CrossRef] [PubMed]
- Hebert, C.A.; Scales, K. Dementia Friendly Initiatives: A State of the Science Review. Dementia 2019, 18, 1858–1895. [Google Scholar] [CrossRef] [PubMed]
- Fleming, R.; Zeisel, J.; Bennett, K. World Alzheimer Report 2020. Design, Dignity, Dementia: Dementia-Related Design and the Built Environment; Alzheimer’s Disease International: London, UK, 2020; Volume 2. [Google Scholar]
- Bernales, A.J. Evaluación de Las Condiciones de Habitabilidad Del Adulto Mayor, En Las Viviendas Autoconstruidas En El Hábitat Informal de Los Cerros de Valparaíso; Universidad de Chile: Santiago, Chile, 2021. [Google Scholar]
- Altman, I.; Rogoff, B. World View in Psychology: Trait Interactionist, Organismic and Transactional Approaches. In Handbook of Environmental Psychology; Wiley: New York, NY, USA, 1986. [Google Scholar]
- Werner, C.M.; Altman, I.; Oxley, D. Temporal Aspects of Homes. In Home Environments. Human Behaviour and Environment; Altman, I., Werner, C.M., Eds.; Springer: Boston, MA, USA, 1985; pp. 1–32. ISBN 978-1-4899-2266-3. [Google Scholar]
- Lynch, K. The Image of the City, 2nd ed.; Harvard-MIT Joint Center for Urban Studies Series; MIT Press: Cambridge, MA, USA, 1964; ISBN 9780262620017. [Google Scholar]
- Blackman, T.; Mitchell, L.; Burton, E.; Jenks, M.; Parsons, M.; Raman, S.; Williams, K. The Accessibility of Public Spaces for People with Dementia: A New Priority for the “Open City”. Disabil. Soc. 2003, 18, 357–371. [Google Scholar] [CrossRef]
- Mitchell, L.; Burton, E. Neighbourhoods for Life: Designing Dementia-Friendly Outdoor Environments. Qual. Ageing Older Adults 2006, 7, 26–33. [Google Scholar] [CrossRef]
- Price, C.; Tsouros, A.D. Our Cities, Our Future: Policies and Action Plans for Health and Sustainable Development; WHO Healthy Cities Project Office: Copenhague, Denmark, 1996. [Google Scholar]
- Grahame, A. What Would an Age-Friendly City Look Like? Guard 2018. [Google Scholar]
- van Hoof, J.; Kazak, J.K.; Perek-Białas, J.M.; Peek, S.T.M. The Challenges of Urban Ageing: Making Cities Age-Friendly in Europe. Int. J. Environ. Res. Public Health 2018, 15, 2473. [Google Scholar] [CrossRef] [PubMed]
- Fariña, J.; Higueras, E.; Román, E.; Pozo, E. Guía Para Planificar Ciudades Saludables; Ministerio de Sanidad, FEMP: Madrid, Spain, 2022.
- Yin, R.K. Case Study Research and Applications. Design and Methods, 6th ed.; SAGE Publications: Los Angeles, CA, USA, 2017. [Google Scholar]
- Runeson, P.; Höst, M. Guidelines for Conducting and Reporting Case Study Research in Software Engineering. Empir. Softw. Eng. 2009, 14, 131–164. [Google Scholar] [CrossRef]
- Centre for Health Design. Building the Evidence Base: Understanding Research in Healthcare Design. EDAC Study Guide Series, 2nd ed.; Center of Health Design: Concord, CA, USA, 2018; ISBN 9780981900520. [Google Scholar]
- Alzheimer’s Disease International. Dementia Friendly Communities Global Developments; Alzheimer’s Disease International: London, UK, 2017. [Google Scholar]
- Alzheimer’s Society List of Dementia Friendly Communities. Available online: https://www.dementiafriends.org.uk/ (accessed on 8 September 2022).
- EFID. Mapping Dementia-Friendly Communities across Europe. A Study Commissioned by the European Foundations’ Initiative on Dementia (EFID). 2016. Available online: https://www.age-platform.eu/publications/mapping-dementia-friendly-communities-across-europe (accessed on 8 October 2022).
- Colón, Z.; Juan Ramasco Gutiérrez, M.; Marcos Pedraz, A.; Palmar Santos, A.M. Investigación Cualitativa En Salud (Cuadernos Metodológicos); Centro de Investigaciones Sociológicas: Madrid, Spain, 2019; ISBN 978-8474768053. [Google Scholar]
- Lennon, S. Country’s First Dementia Village, Harmonia in Randolph Road, Dover, to Open in December. KentOnline. 2019. Available online: https://www.kentonline.co.uk/dover/news/first-dementia-village-on-the-way-213942/ (accessed on 10 October 2022).
- CASCADE Community Areas of Sustainable Care and Dementia Excellence in Europe. Available online: https://www.interreg2seas.eu/en/cascade (accessed on 25 February 2020).
- World Population Prospects 2022; United Nations: New York, NY, USA, 2022; ISBN 978-92-1-148373-4.
- World Urbanization Prospects: The 2018 Revision; United Nations: New York, NY, USA, 2019.
- Brodsky, J.; Habib, J.; Hirschfeld, M.; Siegel, B. Care of the Frail Elderly in Developed and Developing Countries: The Experience and the Challenges. Aging Clin. Exp. Res. 2002, 14, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Edvardsson, D.; Backman, A.; Bergland, Å.; Björk, S.; Bölenius, K.; Kirkevold, M.; Lindkvist, M.; Lood, Q.; Lämås, K.; Lövheim, H.; et al. The Umeå Ageing and Health Research Programme (U-Age): Exploring Person-Centred Care and Health-Promoting Living Conditions for an Ageing Population. Nord. J. Nurs. Res. 2016, 36, 168–174. [Google Scholar] [CrossRef]
- WHO Global Action Plan on the Public Health Response to Dementia 2017–2025; WHO: Geneva, Switzerland, 2017.
- Heward, M.; Innes, A.; Cutler, C.; Hambidge, S. Dementia-Friendly Communities: Challenges and Strategies for Achieving Stakeholder Involvement. Health Soc. Care Community 2017, 25, 858–867. [Google Scholar] [CrossRef] [PubMed]
- BSI. Code of Practice for the Recognition of Dementia-Friendly Communities in England; BSI: London, UK, 2015; PAS 1365:2015. [Google Scholar]
- Mitchell, L.; Burton, E.; Raman, S. Dementia-Friendly Cities: Designing Intelligible Neighbourhoods for Life. J. Urban Des. 2004, 9, 89–101. [Google Scholar] [CrossRef]
- Lewis, S. Dementia and Town Planning: Creating Better Environments for People Living with Dementia; Royal Town Planning Institute: London, UK, 2017; pp. 1–16. [Google Scholar]
- Alzheimer’s Australia Dementia Care and the Built Environment. Alzheimer’s Aust. 2004, 3, 1–16.
- Mmako, N.J.; Courtney-Pratt, H.; Marsh, P. Green Spaces, Dementia and a Meaningful Life in the Community: A Mixed Studies Review. Health Place 2020, 63, 102344. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, G.; Büter, K.; Motzek, T. Impact of the Design of the Built Environment on People with Dementia: An Evidence-Based Review. Health Environ. Res. Des. J. 2014, 9, 127–157. [Google Scholar] [CrossRef] [PubMed]



























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Center | Oceania | Asia | Latin America | North America | Africa | Europe | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | N | C | A | O 1 | ||||||
| Elderly day care center | 2 | 12 | 2 | 1 | 0 | 1 | 0 | 0 | 3 | 0 |
| Care home | 19 | 9 | 1 | 10 | 1 | 2 | 3 | 1 | 7 | 5 |
| Public equipment | 1 | 1 | - | 1 | - | - | 1 | 1 | - | |
| Hospital | - | - | - | - | - | - | - | 1 | - | |
| TOTAL | 22 | 22 | 3 | 12 | 1 | 3 | 4 | 1 | 12 | 5 |
| City | Type of Project | Name and Details | Criteria |
|---|---|---|---|
| 1. United Kingdom | |||
| 1.1. Newcastle-upon-Tyne | Dementia-friendly city | Discovery museum | International reference on Active Ageing: National Centre of Active Ageing (NICA) and community local initiatives |
| 1.2. Dover | Dementia village | Harmonia Village, new residential care concept for people with dementia | European project CASCADE selected in competitive call, founded by European Union, Interreg 2Seas Mers Zeeën Program (2017–2023) |
| 1.3. Rochester | Respite Center | Community center with different services for people with dementia and relatives | |
| 2. Belgium | |||
| 2.1. Kortrijk | Reminiscence walks | Care home WZC de Weister | European Award EFID 2014 |
| 2.2. Bruges | Dementia-friendly Bruges | FOTON. Regional Expertise Centre. Familierzorg West-Vlaanderen VZW (Family Care in West-Flanders) | European Award EFID 2012 and 2020 ‘Together for a dementia-friendly Bruges’. Golden Ear for Foton Volunteers |
| 2.3. Osterloo, Geel | Small-scale care home | Huis Perrekes | Best practice nomination in ADI, 2017. Presentation at ‘International Mind Conference 2019’. Publication in Flanders Architectural Review No. 14. ‘When Attitudes Take Form’. |
| 3. The Netherlands | |||
| 3.1. Weesp | The Hogeweyk, dementia village | Care home for people living with dementia. | Several publications at national and international level. Awards and prizes: Hospitality Care Award 2010 Nominated for the Hedy d’Ancona Award 2010, excellence in Healthcare architecture Golden label for Quality by Perspect 2006 Project of the World, Expo 2000 Hannover International Hospital Federation Award 1995 Dien Cornelissenprijs 1993 |
| 3.2. Nuenen | Active walks: Kwiek beweegroute | Healthy and activity walks in local neighbors around care homes. | First prize UKON Uniek Prijs 2014 Third prize Your Street Design Indaba 2012 |
| Interviews’ Script |
|---|
| 1. How many people live in the community? How many people regularly visit the community? What is the level of dementia and dependency? |
| 2. What is the average number of years a person spends living in the community? |
| 3. Do you know how many people (without dementia) visit and join the community? What profile? What kind of activities do they join? |
| 4. Is there any relationship with other institutions that support and collaborate with the care home? (schools, universities, healthcare services…) |
| 5. How many volunteers participate normally? What kinds of activities are organized? |
| 6. Is the care home well connected to the city center by public transport? |
| 7. What kind of buildings or services are next to the care home? Is there any relationship (use/function/activities…)? |
| 8. Is the care home designed considering any of the dementia-friendly guidelines? Which ones? Which outdoor spaces do residents usually use? |
| 9. Is there any special consideration about housing/public spaces/transportation/design guidelines in a local Urban Master Plan? |
| 10. Is design conceived from the dementia-friendly guidelines? How? |
| 11. How can design be adapted to create more inclusive environments both indoor and outdoor from your experience? |
| 12. Is there any project or planning about the proximity of green areas? Therapeutic gardens/horticultural activities? |
| 13. How do you work with sensorial activities and design? |
| 14. Is the public space accessible enough to promote autonomy? Do people with dementia use it? Existence of benches, outdoor features, iconic landmarks, and buildings, etc. |
| 15. Are features such as thermal/lighting/wind comfort considered in the design? |
| 16. In your opinion, what is the most important thing of your community for people with dementia? What are the main initiatives that are being developed in your city/community for the dementia-friendly community? |
| 17. What features in public space do you think are the most valuable for people with dementia? Is there any specific built environment in the city (square, market, garden, healthcare residence…) that is adapted and how for people with dementia? |
| Project | Charge/Role | Duration [Min] |
|---|---|---|
| 1. United Kingdom | ||
| 1.1. Discovery Museum, Dementia-friendly Newcastle-upon-Tyne | Leader and champion of the Platinum Program | 40′ |
| 1.2. Harmonia Village, Dementia village, Dover | Director of the new care home Harmonia Village | 38′ |
| 1.3. Harmony House, Respite Center, Rochester | Director of the new respite center | 83′ |
| 2.Belgium | ||
| 2.1. WZC De Weister, small-scale care home, Aalbeke, Kortrijk | Director of 2 care homes in Kortrijk, one of which is WZC De Weister | 112′ |
| 2.2. Fotonhouse, Dementia Expertise Centre, Bruges | Director of the Familiezorg West-Vlaanderen VZW and coordinator of the project Foton | 23′ |
| 2.3. Huis Perrekes, Geel, Osterloo | Worker at Huis Perrekes | 84′ |
| 3. The Netherlands | ||
| 3.1. De Hogeweyk, Weesp | CEO and senior consultant, co-founder of De Hogeweyk | 166′ |
| 3.2. Kwiek Beweegroute, Nuenen | Founder of the Kwiek beweegroute | 24′ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pozo Menéndez, E.; Higueras García, E. Best Practices from Eight European Dementia-Friendly Study Cases of Innovation. Int. J. Environ. Res. Public Health 2022, 19, 14233. https://doi.org/10.3390/ijerph192114233
Pozo Menéndez E, Higueras García E. Best Practices from Eight European Dementia-Friendly Study Cases of Innovation. International Journal of Environmental Research and Public Health. 2022; 19(21):14233. https://doi.org/10.3390/ijerph192114233
Chicago/Turabian StylePozo Menéndez, Elisa, and Ester Higueras García. 2022. "Best Practices from Eight European Dementia-Friendly Study Cases of Innovation" International Journal of Environmental Research and Public Health 19, no. 21: 14233. https://doi.org/10.3390/ijerph192114233
APA StylePozo Menéndez, E., & Higueras García, E. (2022). Best Practices from Eight European Dementia-Friendly Study Cases of Innovation. International Journal of Environmental Research and Public Health, 19(21), 14233. https://doi.org/10.3390/ijerph192114233