
Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Literature Search
2.2. Study Selection
2.3. Types of Studies
2.4. Types of Participants
2.5. Types of Exposure and Control/Comparison
2.6. Measures of Effect
2.7. Types of Outcome Measures
2.8. Data Collection and Measurement of Treatment Effect
2.9. Risk of Bias in Individual Studies
2.10. Data Synthesis & Analyses
2.11. Assessment of Heterogeneity and Publication Bias
2.12. Assessment of Certainty of Evidence
3. Results
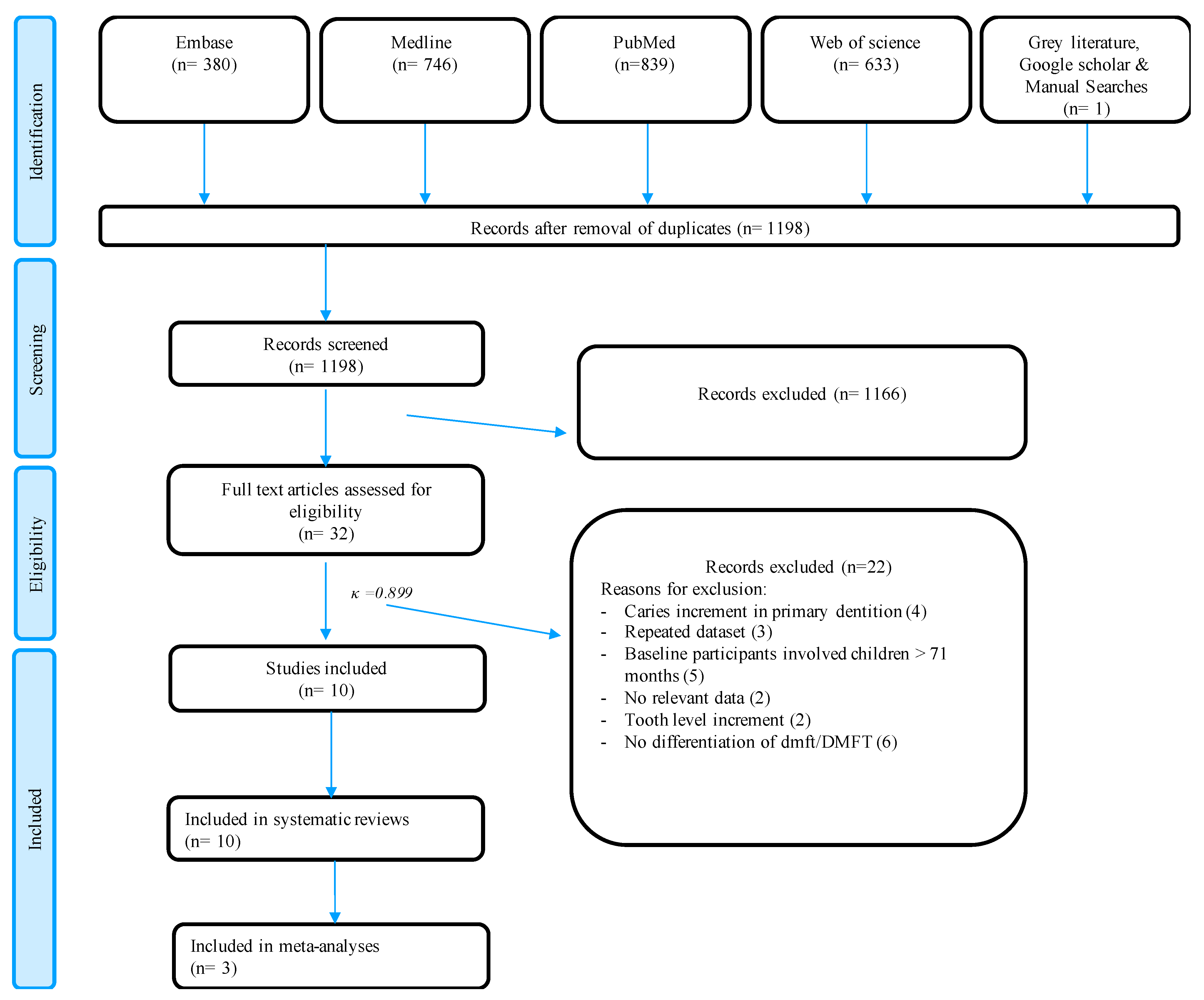
3.1. Selection Process
3.2. Data Extraction
3.3. Risk of Bias of Included Studies
3.4. Potential Factors Associated with Caries Increment in Permanent Teeth
3.4.1. Caries in Primary Dentition
3.4.2. Depth of Caries and Severity of ECC
3.4.3. Location of Caries
3.4.4. Gender
3.4.5. Sociodemographic Factors
3.4.6. Oral Hygiene and Dietary Habits
3.4.7. Bacterial Load
3.5. GRADE Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Academy of Pediatric Dentistry. Policy on Early Childhood Caries (ECC): Classifications, consequences, and preventive strategies. Pediatr. Dent. 2016, 38, 52–54. [Google Scholar]
- Uribe, S.E.; Innes, N.; Maldupa, I. The global prevalence of early childhood caries: A systematic review with meta-analysis using the WHO diagnostic criteria. Int. J. Paediatr. Dent. 2021, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Anil, S.; Anand, P.S. Early Childhood Caries: Prevalence, risk factors, and prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Heinrich-Weltzien, R.; Monse, B.; Benzian, H.; Heinrich, J.; Kromeyer-Hauschild, K. Association of dental caries and weight status in 6- to 7-year-old Filipino children. Clin. Oral Investig. 2012, 17, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.; McGrath, C.; King, N.; Lo, E. Oral Health-related quality of life in Hong Kong preschool children. Caries Res. 2011, 45, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Thomson, W.M.; Poulton, R.; Milne, B.J.; Caspi, A.; Broughton, J.R.; Ayers, K.M.S. Socioeconomic inequalities in oral health in childhood and adulthood in a birth cohort. Community Dent. Oral Epidemiol. 2004, 32, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Cortellazzi, K.L.; Tagliaferro, E.P.; Pereira, S.M.; Ambrosano, G.M.; Guerra, L.M.; De Vazquez, F.; De Meneghim, M.; Pereira, A.C. A Cohort study of caries incidence and baseline socioeconomic, clinical and demographic variables: A kaplan-meier survival analysis. Oral Health Prev. Dent. 2013, 11, 349–358. [Google Scholar] [CrossRef]
- Saethre-Sundli, H.B.; Wang, N.J.; Wigen, T.I. Do enamel and dentine caries at 5 years of age predict caries development in newly erupted teeth? A prospective longitudinal study. Acta Odontol. Scand. 2020, 78, 509–514. [Google Scholar] [CrossRef]
- Li, Y.; Wang, W. Predicting caries in permanent teeth from caries in primary teeth: An eight-year cohort study. J. Dent. Res. 2002, 81, 561–566. [Google Scholar] [CrossRef]
- Sounah, S.A.; Madfa, A.A. Correlation between dental caries experience and the level of Streptococcus mutans and lactobacilli in saliva and carious teeth in a Yemeni adult population. BMC Res. Notes 2020, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nanda, J.; Sachdev, V.; Sandhu, M.; Nanda, K.D.S. Correlation between dental caries experience and mutans streptococci counts using saliva and plaque as microbial risk indicators in 3–8 year old children. A cross Sectional study. J. Clin. Exp. Dent. 2015, 7, e114–e118. [Google Scholar] [CrossRef] [PubMed]
- Van Chuyen, N.; Van Du, V.; Van Ba, N.; Long, D.D.; Son, H.A. The prevalence of dental caries and associated factors among secondary school children in rural highland Vietnam. BMC Oral Health 2021, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Dörfer, C.; Schlattmann, P.; Page, L.F.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries. J. Dent. Res. 2014, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Nicoll, A.D.; Adair, P.M.; Pine, C.M. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent. Health 2004, 21, 71–85. [Google Scholar] [PubMed]
- Kirthiga, M.; Murugan, M.; Saikia, A.; Kirubakaran, R. Risk Factors for early childhood caries: A systematic review and meta-analysis of case control and cohort studies. Int. J. Clin. Pediatr. Dent. 2019, 41, 95–112. [Google Scholar]
- Leong, P.M.; Gussy, M.G.; De Silva-Sanigorski, A.; Waters, E.; Barrow, S.-Y.L.; Silva-Sanigorski, A. A systematic review of risk factors during first year of life for early childhood caries. Int. J. Paediatr. Dent. 2012, 23, 235–250. [Google Scholar] [CrossRef]
- Zhang, J.; Sardana, D.; Wong, M.; Leung, K.; Lo, E. Factors associated with dental root caries: A systematic review. JDR Clin. Transl. Res. 2019, 5, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Lu, H.; Lo, E. Caries increment over 2 years in preschool children: A life course approach. Int. J. Paediatr. Dent. 2011, 22, 77–84. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE reporting guidelines for meta-analyses of observational studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.-C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingström, P.; et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: Consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S39–S51. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Cuello, C.; Akl, E.A.; Mustafa, R.A.; Meerpohl, J.J.; Thayer, K.; Morgan, R.L.; Gartlehner, G.; Kunz, R.; Katikireddi, S.V.; et al. GRADE guidelines: 18. How ROBINS-I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. J. Clin. Epidemiol. 2018, 111, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Higgins, J.P.T.; Vist, G.E.; Glasziou, P.; Akl, E.A.; Skoetz, N.; Guyatt, G.H. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.3; Cochrane: London, UK, 2022. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.T.; Douglas, G.A. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.3; Cochrane: London, UK, 2022. [Google Scholar]
- Guyatt, G.; Rennie, D.; Meade, M.; Cook, D. Users’ Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice, 3rd ed.; AMA press: Chicago, IL, USA, 2015; Volume 706. [Google Scholar]
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A. Chapter 13: Assessing risk of bias due to missing results in a synthesis. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.3; Cochrane: London, UK, 2022. [Google Scholar]
- Al-Shalan, T.A.; Erickson, P.R.; Hardie, N.A. Primary incisor decay before age 4 as a risk factor for future dental caries. Pediatr. Dent. 1997, 19, 37–41. [Google Scholar] [PubMed]
- Du, Q.; Yu, M.; Li, Y.; Du, H.; Gao, W.; Mei, H.; Liu, S. Permanent caries experience is associated with primary caries experience: A 7-year longitudinal study in China. Community Dent. Oral Epidemiol. 2016, 45, 43–48. [Google Scholar] [CrossRef]
- Skeie, M.S.; Raadal, M.; Strand, G.V.; Espelid, I. The relationship between caries in the primary dentition at 5 years of age and permanent dentition at 10 years of age-a longitudinal study. Int. J. Paediatr. Dent. 2006, 16, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Straetemans, M.; Van Loveren, C.; De Soet, J.; De Graaff, J.; Cate, J.T. Colonization with Mutans Streptococci and Lactobacilli and the Caries Experience of Children after the Age of Five. J. Dent. Res. 1998, 77, 1851–1855. [Google Scholar] [CrossRef]
- Thibodeau, E.A.; O’Sullivan, D.M. Salivary mutans streptococci and caries development in the primary and mixed dentitions of children. Community Dent. Oral Epidemiol. 1999, 27, 406–412. [Google Scholar] [CrossRef]
- Alm, A.; Wendt, L.K.; Koch, G.; Birkhed, D.; Nilsson, M. Caries in adolescence-influence from early childhood. Community Dent. Oral Epidemiol. 2011, 40, 125–133. [Google Scholar] [CrossRef]
- Chankanka, O.; Cavanaugh, J.E.; Levy, S.M.; Marshall, T.A.; Warren, J.; Ms, B.B.; Kolker, J.L. Longitudinal associations between children’s dental caries and risk factors. J. Public Health Dent. 2011, 71, 289–300. [Google Scholar] [CrossRef]
- Li, Y.; Wulaerhan, J.; Liu, Y.; Abudureyimu, A.; Zhao, J. Prevalence of severe early childhood caries and associated socioeconomic and behavioral factors in Xinjiang, China: A cross-sectional study. BMC Oral Health 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Douglass, J.M.; Li, Y.; Tinanoff, N. Association of mutans streptococci between caregivers and their children. Pediatr. Dent. 2008, 30, 375–378. [Google Scholar] [PubMed]
- Manchanda, S.; Sardana, D.; Liu, P.; Lee, G.H.M.; Lo, E.C.M.; Yiu, C.K.Y. Horizontal Transmission of Streptococcus mutans in Children and its Association with Dental Caries: A Systematic Review and Meta-Analysis. Pediatr. Dent. 2021, 43, 1E–12E. [Google Scholar] [PubMed]
- Fakhruddin, K.S.; Ngo, H.C.; Samaranayake, L.P. Cariogenic microbiome and microbiota of the early primary dentition: A contemporary overview. Oral Dis. 2018, 25, 982–995. [Google Scholar] [CrossRef] [PubMed]
- Innes, N.; Chu, C.; Fontana, M.; Lo, E.; Thomson, W.; Uribe, S.; Heiland, M.; Jepsen, S.; Schwendicke, F. A Century of Change towards Prevention and Minimal Intervention in Cariology. J. Dent. Res. 2019, 98, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Lam, P.P.; Sardana, D.; Lo, E.C.; Yiu, C.K. Fissure sealant in a nutshell. Evidence-based meta-evaluation of sealants’ effectiveness in caries prevention and arrest. J. Evid. Based Dent. Pract. 2021, 21, 101587. [Google Scholar] [CrossRef] [PubMed]
- Innes, N.P.; Ricketts, D.; Chong, L.Y.; Keightley, A.J.; Lamont, T.; Santamaria, R.M. Preformed crowns for decayed primary molar teeth. Cochrane Database Syst. Rev. 2015, 2015, CD005512. [Google Scholar] [CrossRef]
- Klinke, T.; Urban, M.; Lück, C.; Hannig, C.; Kuhn, M.; Krämer, N. Changes in Candida spp., mutans streptococci and lactobacilli following treatment of early childhood caries: A 1-year follow-up. Caries Res. 2013, 48, 24–31. [Google Scholar] [CrossRef]
- Morinushi, T.; Murayama, M.; Kinjyo, S. Mutans streptococci, lactobacilli in saliva and acidity from organismsin dental plaque: Changes after restorative treatment. J. Clin. Pediatr. Dent. 2004, 28, 327–332. [Google Scholar] [CrossRef]
- Gray, M.M.; Marchment, M.D.; Anderson, R.J. The relationship between caries experience in the deciduous molars at 5 years and in first permanent molars of the same child at 7 years. Community Dent. Health 1991, 8, 3–7. [Google Scholar]
- Songur, F.; Derelioglu, S.S.; Yilmaz, S.; Koşan, Z. Assessing the impact of early childhood caries on the development of first permanent molar decays. Front. Public Health 2019, 7, 186. [Google Scholar] [CrossRef] [PubMed]
- Marinho, V.C.C.; Worthington, H.V.; Walsh, T.; Clarkson, J.E. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2013, 7, CD002279. [Google Scholar] [CrossRef] [PubMed]
- Ahovuo-Saloranta, A.; Forss, H.; Walsh, T.; Nordblad, A.; Mäkelä, M.; Worthington, H.V. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst. Rev. 2017, 7, CD001830. [Google Scholar] [CrossRef] [PubMed]
- Shaw, D.; Macpherson, L.; Conway, D. Tackling socially determined dental inequalities: Ethical aspects of childsmile, the national child oral health demonstration programme in Scotland. Bioethics 2009, 23, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Sakashita, R.; Ogura, M.; Nakanishi, E.; Sato, T. A Longitudinal study on the relationship of oral health at 4 years of age with that in adulthood. Dent. J. 2021, 9, 17. [Google Scholar] [CrossRef]
- Losilla, J.-M.; Oliveras, I.; Marin-Garcia, J.A.; Vives, J. Three risk of bias tools lead to opposite conclusions in observational research synthesis. J. Clin. Epidemiol. 2018, 101, 61–72. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Study (Year, Country a) | Commencement Year, Duration | N Subject Baseline/ Follow-Up; | Commencement Age/Age at Final Follow-Up | Factors Evaluated | Measurement of Effect | Significant Factors |
|---|---|---|---|---|---|---|---|
| 1 | Alm (2012, SWE) [33] | 1988, 14 years | 671/568 | 12 months/ 15 years |
|
|
|
| 2 | Al-Shalan (1997, USA) [28] | 1985, 3 years | 115/115 | 18–48 months/ 6–14 years |
|
|
|
| 3 | Chankanka (2011, THA) [34] | 1992, 5 years | 198/150 | 5 years/9 years |
|
|
|
| 4 | Cortellazzi (2013, BRA) [8] | 2005, 5 years | 427/246 | 3–5 years/ 10 years |
|
|
|
| 5 | Du (2017, CHA) [29] | 2006 7 years | 1885/1683 | 5 years/ 12 years |
|
|
|
| 6 | Li (2002, CHA) [35] | 1992, 8 years | 504/362 | 3–4 years/ 11–13 years |
|
|
|
| 7 | Saethre-Sundli (2020, NOR) [9] | 2007, 7 years | 3282/3282 | 5 years/ 12 years |
|
|
|
| 8 | Skeie (2006, NOR) [30] | 1993, 5 years | 217/186 | 5 years/ 10 years |
|
|
|
| 9 | Straetemans (1998, NLD) [31] | 1985, 6 years | 196/109 | 5 years/ 11 years |
|
|
|
| 10 | Thibodeau (1999, USA) [32] | NR, 6 years | 85/85 | 3 years/ 9 years |
|
|
|
| Comparison | Results | N Patient Age Range (Years) | N Studies | Risk of Bias b | Inconsistency c | Indirectness d | Imprecision e | Publication Bias f | Quality of Evidence (GRADE) | |
|---|---|---|---|---|---|---|---|---|---|---|
| I2 (%) | HETEROGENICITY χ2 Test (p Value) | |||||||||
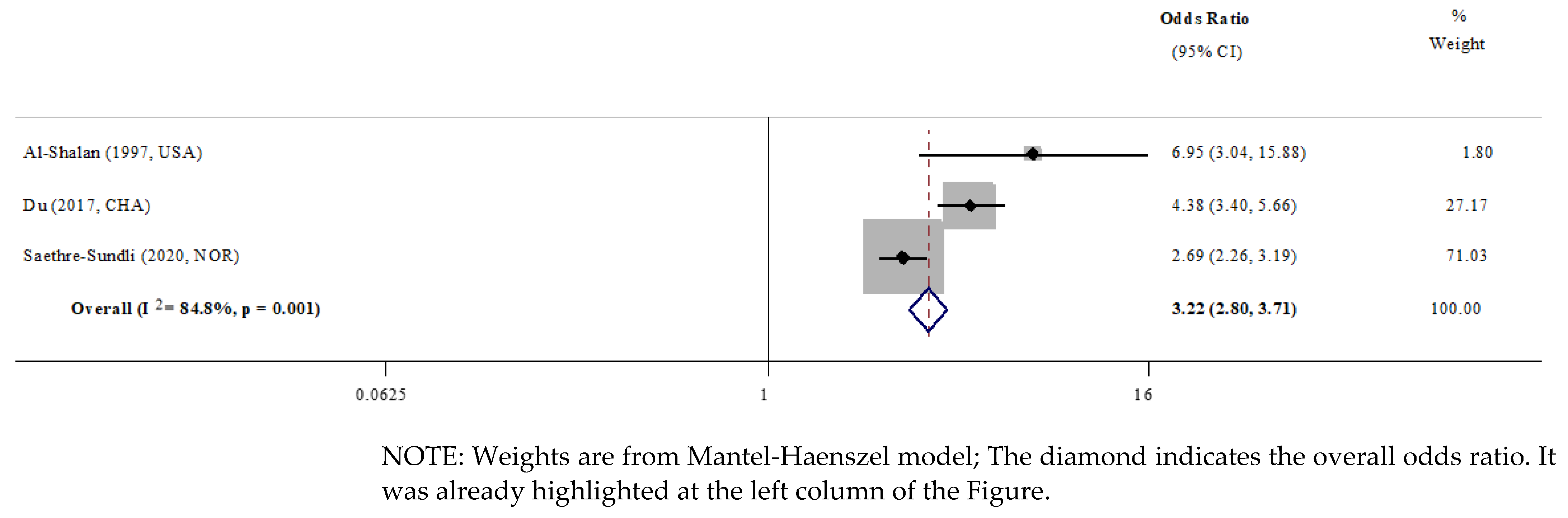
| Past caries experience | Children with ECC are 3.22 times as likely to develop caries in permanent teeth | 5080 (6–12) | 3 | Serious | 84.8% | 0.001 | Not serious | Not serious | N/A | ⊕OOO very low |
| ↓ | ↓ | -- | -- | -- | ||||||
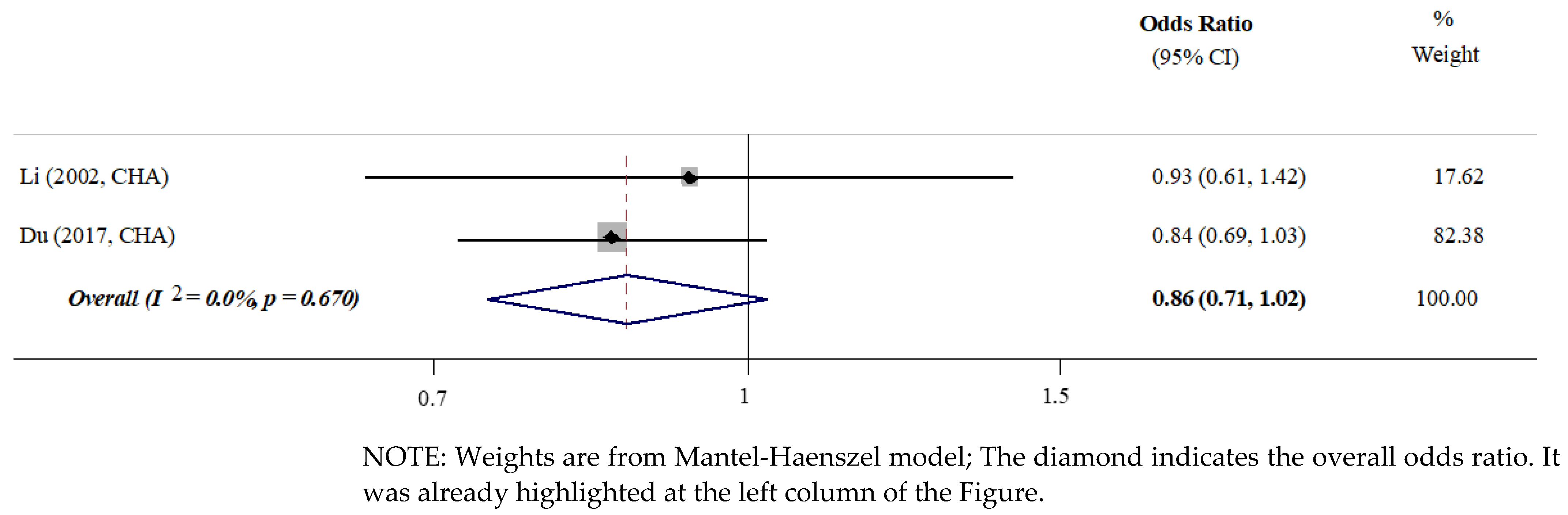
| Gender | No significant difference | 2045 (11–13) | 2 | Serious | 0.0% | 0.670 | Not serious | Not serious | N/A | ⊕⊕OO low |
| ↓ | -- | -- | -- | -- | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, P.P.Y.; Chua, H.; Ekambaram, M.; Lo, E.C.M.; Yiu, C.K.Y. Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 13459. https://doi.org/10.3390/ijerph192013459
Lam PPY, Chua H, Ekambaram M, Lo ECM, Yiu CKY. Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(20):13459. https://doi.org/10.3390/ijerph192013459
Chicago/Turabian StyleLam, Phoebe Pui Ying, Helene Chua, Manikandan Ekambaram, Edward Chin Man Lo, and Cynthia Kar Yung Yiu. 2022. "Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 20: 13459. https://doi.org/10.3390/ijerph192013459
APA StyleLam, P. P. Y., Chua, H., Ekambaram, M., Lo, E. C. M., & Yiu, C. K. Y. (2022). Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(20), 13459. https://doi.org/10.3390/ijerph192013459