
Comparison of First Childbirth Characteristics between Elite Judo Athletes and Non-Athletes: The Preliminary Retrospective Case–Control Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
- -
- Labor induction: artificial prompting of the uterus to contract before labor begins on its own. It may be implemented due to various medical indications related to maternal and fetal health status [28].
- -
- Labor augmentation: application of intravenous oxytocin to hasten labor and shorten the time to delivery (used in longer labors or less frequent uterine contractions) [29].
- -
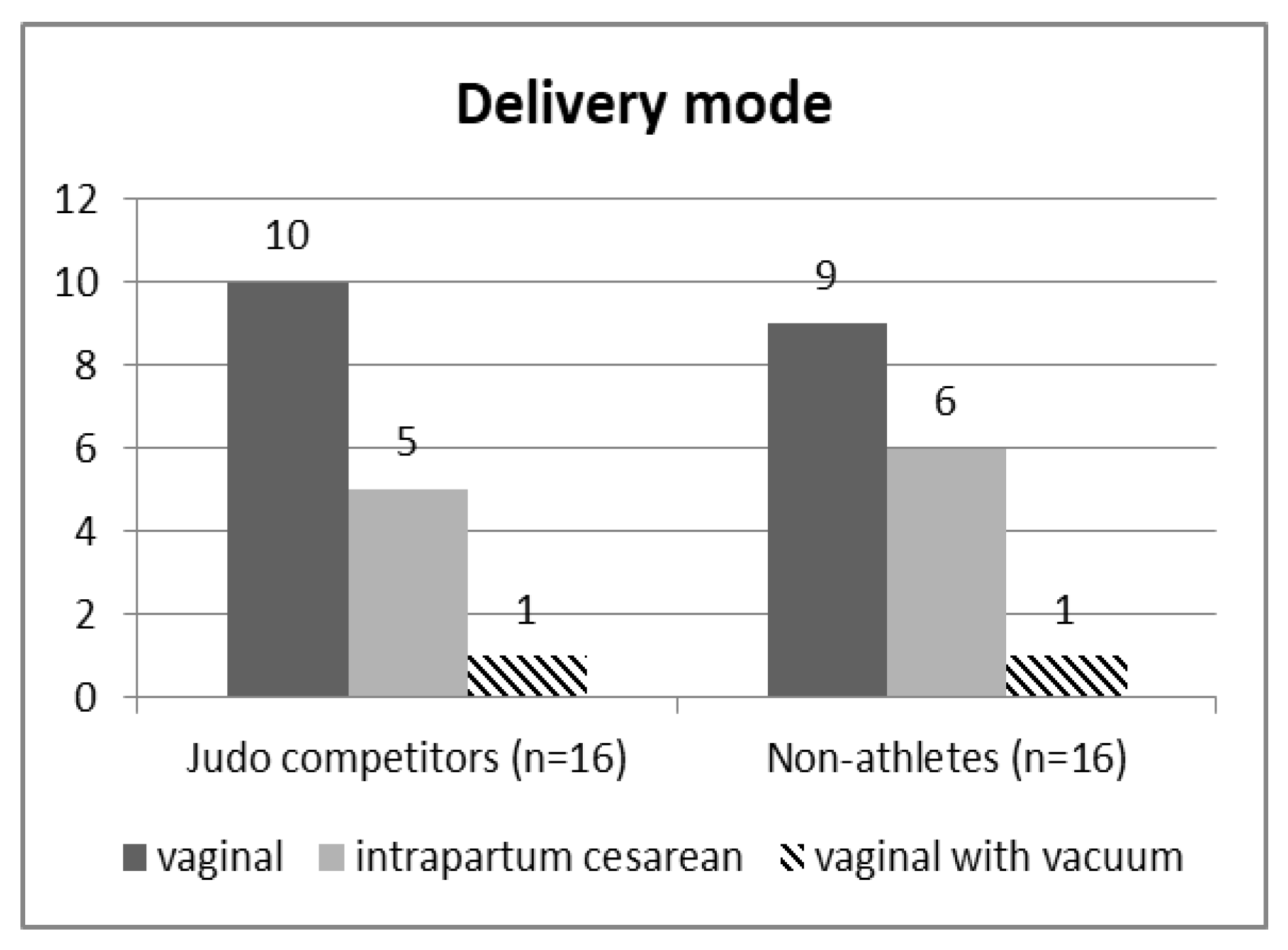
- Intrapartum (emergency) cesarean delivery is performed after labor onset [30].
- -
- The first stage of labor: starts with the onset of regular uterine contractions and ends with full cervical dilation to 10 cm. The absence of cervical change for greater than four hours in the presence of adequate contractions or six hours with inadequate contractions is considered the arrest of labor and may require clinical intervention [31].
- -
- The second stage of labor is the time between complete dilation of the cervix (about 10 cm) and neonate delivery. It typically lasts less than three hours in nulliparas and less than two hours in multiparas (in labors with neuraxial anesthesia it is longer) [31].
- -
- assisted (instrumental) vaginal deliveries mainly involve the use of forceps or a vacuum cup to expedite delivery, usually during delays in the second stage of labor when it is impossible or unsafe to perform a cesarean section [32].
- -
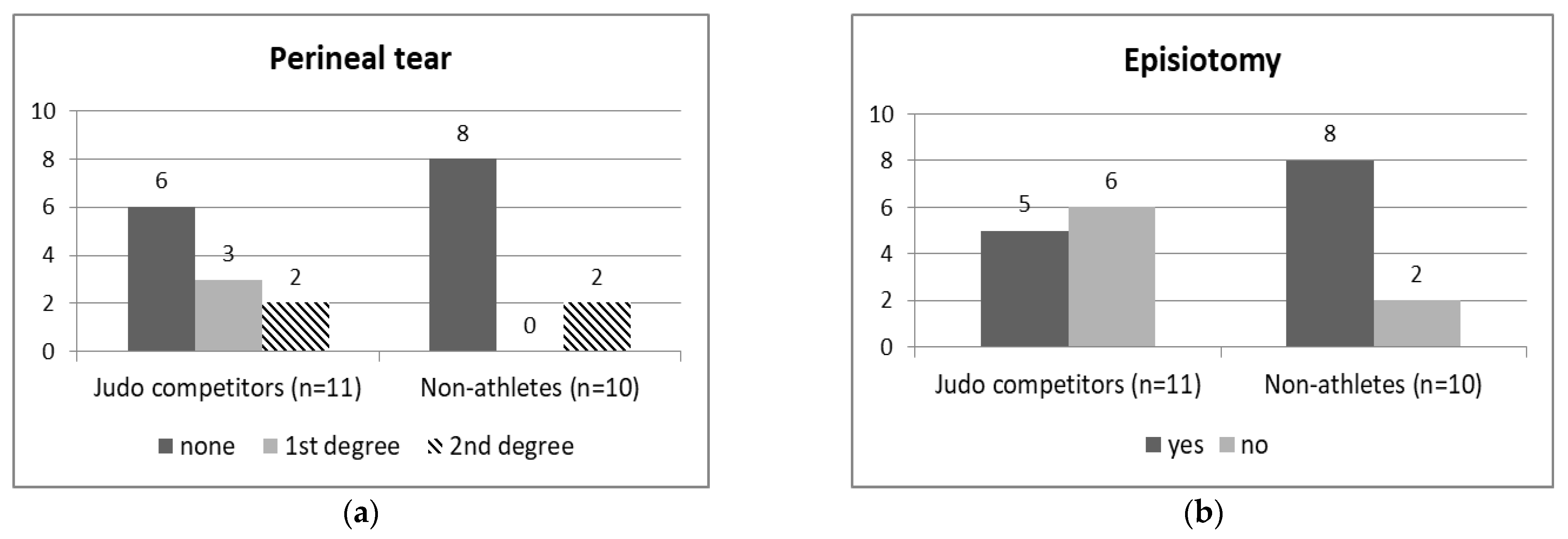
- Perineal tears differ in degree of laceration involving: (1) vaginal mucosa or perineal skin only, (2) the perineal muscles, (3) the anal sphincter muscles, and (4) the anal epithelium [33].
- -
- Episiotomy is a surgical incision of the perineum and the posterior vaginal wall aiming to widen the vaginal outlet, facilitate delivery, and reduce the rates of severe perineal tears; however, recent research has not supported the theory that it prevents pelvic floor trauma [33].
- -
- The Apgar scale is a tool used to assess a newborn’s clinical status. Apgar scores are reported at 1 and 5 min after birth for all infants. The acronym stands for the following characteristics in a newborn: Appearance—skin color, Pulse—heart rate, Grimace—reflexes, Activity—muscle tone, and Respiration—breathing. It does not predict individual neonatal mortality or neurologic outcome [34].
3. Results
4. Discussion
Study Limitations and Indications for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Franchini, E.; Del Vecchio, F.B.; Matsushigue, K.A.; Artioli, G.G. Physiological profiles of elite judo athletes. Sports Med. 2011, 41, 147–166. [Google Scholar] [CrossRef] [PubMed]
- Barbado, D.; Lopez-Valenciano, A.; Juan-Recio, C.; Montero-Carretero, C.; van Dieën, J.H.; Vera-Garcia, F.J. Trunk Stability, Trunk Strength and Sport Performance Level in Judo. PLoS ONE 2016, 27, e0156267, Erratum in PLoS ONE 2016, 11, e0162962. [Google Scholar] [CrossRef]
- Kruger, J.A.; Murphy, B.A.; Heap, S.W. Alterations in levator ani morphology in elite nulliparous athletes: A pilot study. Aust. N. Z. J. Obstet. Gynaecol. 2005, 45, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Kruger, J.A.; Dietz, H.P.; Murphy, B.A. Pelvic floor function in elite nulliparous athletes. Ultrasound Obstet. Gynecol. 2007, 30, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Borin, L.C.; Nunes, F.R.; Guirro, E.C. Assessment of pelvic floor muscle pressure in female athletes. PMR 2013, 5, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Sorrigueta-Hernández, A.; Padilla-Fernandez, B.Y.; Marquez-Sanchez, M.T.; Flores-Fraile, M.C.; Flores-Fraile, J.; Moreno-Pascual, C.; Lorenzo-Gomez, A.; Garcia-Cenador, M.B.; Lorenzo-Gomez, M.F. Benefits of physiotherapy on urinary incontinence in high-performance female athletes. Meta-analysis. J. Clin. Med. 2020, 9, 3240. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.B.; Barra, A.A.; Saltiel, F.; Silva-Filho, A.L.; Fonseca, A.M.; Figueiredo, E.M. Urinary incontinence and other pelvic floor dysfunctions in female athletes in Brazil: A cross-sectional study. Scand. J. Med. Sci. Sports 2016, 26, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Hoyte, L.; Damaser, M.S.; Warfield, S.K.; Chukkapalli, G.; Majumdar, A.; Choi, D.J.; Trivedi, A.; Krysl, P. Quantity and distribution of levator ani stretch during simulated vaginal childbirth. Am. J. Obstet. Gynecol. 2008, 199, 198.e1–198.e5. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.; Brunelli, E.; Pilu, G.; Dietz, H.P. The maternal pelvic floor and labor outcome. Am. J. Obstet. Gynecol. MFM 2021, 3, 100452. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kruger, J.A.; Chung, J.H.; Nash, M.P.; Nielsen, P.M. Modelling childbirth: Comparing athlete and non-athlete pelvic floor mechanics. Med. Image Comput. Comput. Assist. Interv. 2008, 11 Pt 2, 750–757. [Google Scholar] [CrossRef]
- Phipps, H.; Charlton, S.; Dietz, H.P. Can antenatal education influence how women push in labour? Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, G.; Beji, N.K. Effects of pushing techniques in birth on mother and fetus: A randomized study. Birth 2008, 35, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Wowdzia, J.B.; McHugh, T.L.; Thornton, J.; Sivak, A.; Mottola, M.F.; Davenport, M.H. Elite Athletes and Pregnancy Outcomes: A Systematic Review and Meta-analysis. Med. Sci. Sports Exerc. 2021, 53, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Bø, K.; Backe-Hansen, K.L. Do elite athletes experience low back, pelvic girdle and pelvic floor complaints during and after pregnancy? Scand. J. Med. Sci. Sports 2007, 17, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, J.; Sundgot-Borgen, C.; Myklebust, G.; Sølvberg, N.; Torstveit, M.K. Elite athletes get pregnant, have healthy babies and return to sport early postpartum. BMJ Open Sport Exerc. Med. 2019, 5, e000652. [Google Scholar] [CrossRef] [PubMed]
- Sigurdardottir, T.; Steingrimsdottir, T.; Geirsson, R.T.; Halldorsson, T.I.; Aspelund, T.; Bø, K. Do female elite athletes experience more complicated childbirth than non-athletes? A case-control study. Br. J. Sports Med. 2018, 53, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wei, Y.; Zhang, X.; Yue, Z.; Qianqian, X.; Yiying, S.; Shipping, S.; Li, Z.; Chunhong, L.; Yaru, F.; et al. Randomized clinical trial of exercise during pregnancy to prevent gestational diabetes mellitus and improve pregnancy outcome in overweight and obese pregnant women. Am. J. Obstet. Gynecol. 2017, 216, 340–351. [Google Scholar] [CrossRef]
- Magro-Malosso, E.R.; Saccone, G.; Di Mascio, D.; Berghella, V. Exercise during pregnancy and risk of preterm birth in overweight and obese women: A systematic review and meta-analysis of randomized controlled trials. Acta Obstet. Gynecol. Scand. 2017, 96, 263–273. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Lopez, C.; Montejo, R.; Coteron, J. Exercise during pregnancy reduces the rate of cesarean and instrumental deliveries: Results of a randomized controlled trial. J. Matern. Fetal Neonatal. Med. 2012, 25, 2372–2376. [Google Scholar] [CrossRef] [PubMed]
- Price, B.B.; Amini, S.B.; Kappeler, K. Exercise in pregnancy: Effect on fitness and obstetric outcomes-a randomized trial. Med. Sci. Sports Exerc. 2012, 44, 2263–2269. [Google Scholar] [CrossRef]
- Di Mascio, D.; Magro-Malosso, E.R.; Saccone, G.; Marhefka, G.D.; Berghella, V. Exercise during pregnancy in normal-weight women and risk of preterm birth: A systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2016, 215, 561–571. [Google Scholar] [CrossRef]
- Bø, K.; Hilde, G.; Staer-Jensen, J.; Siafarikas, F. Does general exercise training before and during pregnancy influence the pelvic floor “opening” and delivery outcome? A 3D/4D ultrasound study following nulliparous pregnant women from mid-pregnancy to childbirth. Br. J. Sports Med. 2015, 49, 196–199. [Google Scholar] [CrossRef]
- Salvesen, A.K.; Stafne, S.N.; Torbjørn, M.; Siv, M. Does regular exercise in pregnancy influence duration of labor? A secondary analysis of a randomized controlled trial. Acta Obstet. Gynecol. Scand. 2014, 93, 73–79. [Google Scholar] [CrossRef]
- Berghella, V.; Saccone, G. Exercise in pregnancy! Am. J. Obstet. Gynecol. 2017, 216, 335–337. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Larsen, K.; Kayser, B.; Kinnunen, T.I.; et al. Exercise and pregnancy in recreational and elite Athletes, 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 2-the effect of exercise on the fetus, labour and birth. Br. J. Sports Med. 2016, 50, 1297–1305. [Google Scholar] [CrossRef]
- Gimovsky, A.C. Defining arrest in the first and second stages of labor. Minerva Obstet. Gynecol. 2021, 73, 6–18. [Google Scholar] [CrossRef]
- Swann, C.; Moran, A.; Piggott, D. Defining elite athletes: Issues in the study of expert performance in sport psychology. Psychol. Sport Exerc. 2015, 16, 3–14. [Google Scholar] [CrossRef]
- Penfield, C.A.; Wing, D.A. Labor Induction Techniques: Which Is the Best? Obstet. Gynecol. Clin. N. Am. 2017, 44, 567–582. [Google Scholar] [CrossRef]
- Kernberg, A.; Caughey, A.B. Augmentation of Labor: A Review of Oxytocin Augmentation and Active Management of Labor. Obstet. Gynecol. Clin. N. Am. 2017, 44, 593–600. [Google Scholar] [CrossRef]
- Kominiarek, M.A.; VanVeldhuisen, P.; Gregory, K.; Fridman, M.; Kim, H.; Hibbard, J.U. Intrapartum cesarean delivery in nulliparas: Risk factors compared by two analytical approaches. J. Perinatol. 2015, 35, 167–172. [Google Scholar] [CrossRef][Green Version]
- Hutchison, J.; Mahdy, H.; Hutchison, J. Stages of Labor; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Feeley, C.; Crossland, N.; Betran, A.P.; Weeks, A.; Downe, S.; Kingdon, C. Training and expertise in undertaking assisted vaginal delivery (AVD): A mixed methods systematic review of practitioners views and experiences. Reprod. Health 2021, 18, 92. [Google Scholar] [CrossRef]
- Goh, R.; Goh, D.; Ellepola, H. Perineal tears—A review. Aust. J. Gen. Pract. 2018, 47, 35–38. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Committee on Fetus and Newborn; American College of Obstetricians and Gynecologists Committee on Obstetric Practice. The Apgar Score. Pediatrics 2015, 136, 819–822. [Google Scholar] [CrossRef]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 8: Qualitative data—Tests of association. Crit. Care 2004, 8, 46–53. [Google Scholar] [CrossRef]
- Watkins, V.Y.; O’Donnell, C.M.; Perez, M.; Zhao, P.; England, S.; Carter, E.B.; Kelly, J.C.; Frolova, A.; Raghuraman, N. The impact of physical activity during pregnancy on labor and delivery. Am. J. Obstet. Gynecol. 2021, 225, e1–e437. [Google Scholar] [CrossRef]
- Masoud, A.T.; AbdelGawad, M.M.; Elshamy, N.H.; Mohamed, O.M.; Hashem, Z.Y.; Abd Eltawab, A.K.; Samy, A.; Abbas, A.M. The effect of antenatal exercise on delivery outcomes: A systematic review and meta-analysis of randomized controlled trials. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101736. [Google Scholar] [CrossRef]
- Sobhgol, S.S.; Smith, C.A.; Dahlen, H.G. The effect of antenatal pelvic floor muscle exercises on labour and birth outcomes: A systematic review and meta-analysis. Int. Urogynecol. J. 2020, 31, 2189–2203. [Google Scholar] [CrossRef]
- Valdes, E.G. Examining Cesarean Delivery Rates by Race: A Population-Based Analysis Using the Robson Ten-Group Classification System. J. Racial. Ethn. Health Disparities 2021, 8, 844–851. [Google Scholar] [CrossRef]
- Blondel, B.; Alexander, S.; Bjarnadóttir, R.I.; Gissler, M.; Langhoff-Roos, J.; Novak-Antolič, Ž.; Prunet, C.; Zhang, W.H.; Hindori-Mohangoo, A.D.; Zeitlin, J. Euro-Peristat Scientific Committee. Variations in rates of severe perineal tears and episiotomies in 20 European countries: A study based on routine national data in Euro-Peristat Project. Acta Obstet. Gynecol. Scand. 2016, 95, 746–754. [Google Scholar] [CrossRef]
- Seijmonsbergen-Schermers, A.E.; van den Akker, T.; Rydahl, E.; Beeckman, K.; Bogaerts, A.; Binfa, L.; Frith, L.; Gross, M.M.; Misselwitz, B.; Hálfdánsdóttir, B.; et al. Variations in use of childbirth interventions in 13 high-income countries: A multinational cross-sectional study. PLoS Med. 2020, 17, e1003103. [Google Scholar] [CrossRef]
- Clesse, C.; Lighezzolo-Alnot, J.; De Lavergne, S.; Hamlin, S.; Scheffler, M. Statistical trends of episiotomy around the world: Comparative systematic review of changing practices. Health Care Women Int. 2018, 39, 644–662. [Google Scholar] [CrossRef]
- Macfarlane, A.J.; Blondel, B.; Mohangoo, A.D.; Cuttini, M.; Nijhuis, J.; Novak, Z.; Ólafsdóttir, H.S.; Zeitlin, J.; Euro-Peristat Scientific Committee. Wide differences in mode of delivery within Europe: Risk-stratified analyses of aggregated routine data from the Euro-Peristat study. BJOG 2016, 123, 559–568. [Google Scholar] [CrossRef]
- Sørbye, I.K.; Oppegaard, K.S.; Weeks, A.; Marsdal, K.; Jacobsen, A.F. Induction of labor and nulliparity: A nationwide clinical practice pilot evaluation. Acta Obstet. Gynecol. Scand. 2020, 99, 1700–1709. [Google Scholar] [CrossRef]
- Austad, F.E.; Eggebø, T.M.; Rossen, J. Changes in labor outcomes after implementing structured use of oxytocin augmentation with a 4-hour action line. J. Matern. Fetal Neonatal. Med. 2021, 34, 4041–4048. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ID | Category of “Eliteness” | The Period from Career Withdrawal to Conception (Months) |
|---|---|---|
| 1 | Successful | 0 |
| 2 | World-class | 2 |
| 3 | World-class | 0 |
| 3 | Competitive | 8 |
| 5 | Competitive | 0 |
| 6 | Competitive | 0 |
| 7 | Competitive | 5 |
| 8 | Competitive | 12 |
| 9 | World-class | 1 |
| 10 | Competitive | 0 |
| 11 | Successful | 6 |
| 12 | Successful | 12 |
| 13 | World-class | 2 |
| 14 | World-class | 11 |
| 15 | World-class | 0 |
| 16 | World-class | 2 |
| ID | Regular Physical Activity | 2nd Trimester Physical Activity Duration/Frequency | 3rd Trimester Physical Activity Duration/Frequency | Regular PFM * Exercises (3–5× Wk) | Trimester, Frequency, Series, Repetitions of PFM Exercises | Type of Regular Physical Activity |
|---|---|---|---|---|---|---|
| 1 | No | - | - | No | - | - |
| 2 | No | - | - | No | - | - |
| 3 | No | - | - | No | - | - |
| 4 | No | - | - | No | - | - |
| 5 | Yes | Daily, 60 min | Daily, 60 min | No | - | Walking |
| 6 | Yes | 2× wk, 30–40 min | 1–2× wk, 30 min | No | - | Swimming |
| 7 | No | - | - | No | - | - |
| 8 | Yes | 5× wk, 90 min | 5× wk, 90 min | No | - | Fitness, walking |
| 9 | Yes | Daily, 30 min | 2–3× wk, 30min | No | - | Joga, pilates, walking |
| 10 | No | - | - | Yes | 2nd and 3rd trimesters, 3–5× wk, 10× 2 series | - |
| 11 | No | - | - | No | - | - |
| 12 | No | - | - | No | - | - |
| 13 | No | - | - | Yes | 3rd trimester, 4× wk, 20–30× 2 series | - |
| 14 | No | - | - | No | - | - |
| 15 | No | - | - | Yes | 3rd trimester, 5× wk, 25× 4 series | - |
| 16 | No | - | - | No | - | - |
| Judo Athletes (n = 16) | Non-Athletes (n = 16) | U | p | |
|---|---|---|---|---|
| Age at childbirth (years) | 26.3 ± 4.1 (20–34) | 26.4 ± 2.5 (22–31) | 125.5 | 0.93 |
| Gestational age at childbirth (weeks) | 39.7 ± 2.0 (35–43) | 39.5 ± 2.0 (35–42) | 123 | 0.87 |
| Body height (cm) | 167.6 ± 7.8 (153–187) | 167.4 ± 5.0 (158–178) | 126.5 | 0.96 |
| Pre-pregnancy body mass (kg) | 63.4 ± 9.3 (47–78) | 63.8 ± 8.7 (54–81) | 127 | 0.99 |
| Pre-labor body mass (kg) | 83.5 ± 11.0 (60–103) | 79.0 ± 11.0 (63–110) | 86.5 | 0.12 |
| Pre-pregnancy BMI | 22.5 ± 2.4 (19.0–27.0) | 22.8 ± 3.1 (18.6–29.7) | 124 | 0.90 |
| Pre-labor BMI | 29.7 ± 3.3 (23.7–35.6) | 28.2 ± 4.1 (22.9–40.4) | 87 | 0.13 |
| Neonate birth weight (g) | 3301.6 ± 465.6 (2400–4180) | 3313.4 ± 454.5 (2525–4150) | 124.5 | 0.90 |
| The period from career withdrawal to conception (months) | 3.8 ± 4.6 (0–12) | - | - | - |
| Judo Athletes (n = 11) | Non-Athletes (n = 10) | U | p | |
|---|---|---|---|---|
| Whole labor (min) | 664.1 ± 667.9 (120–2160) | 507.3 ± 512.0 (90–1740) | 51 | 0.81 |
| 2nd stage of labor (min) | 45.5 ± 48.3 (5–180) | 46.8 ± 38.1 (10–128) | 52.5 | 0.86 |
| 1st min Apgar score | 7.6 ± 3.6 (0–10) | 9.5 ± 0.7 (8–10) | 36.5 | 0.2 |
| 5th min Apgar score | 8.8 ± 2.2 (4–10) | 9.6 ± 0.7 (8–10) | 52.5 | 0.86 |
| Judo Athletes | Non-Athletes | Statistical Analyses | ||
|---|---|---|---|---|
| n | n | U/χ2/FE * | p | |
| Age at childbirth | 10 | 16 | U = 72.5 | 0.7 |
| Gestational age at childbirth | 10 | 16 | U = 72.5 | 0.7 |
| Body height | 10 | 16 | U = 67 | 0.52 |
| Pre-pregnancy body mass | 10 | 16 | U = 71.5 | 0.66 |
| Pre-labor body mass | 10 | 16 | U = 52 | 0.15 |
| Pre-pregnancy BMI | 10 | 16 | U = 78 | 0.94 |
| Pre-labor BMI | 10 | 16 | U = 63 | 0.39 |
| Neonate birth weight | 10 | 16 | U = 64.5 | 0.42 |
| Labor induction (yes/no) | 10 | 16 | χ2 = 0.0 | 1.0 |
| Labor augmentation (yes/no) | 10 | 16 | FE | 0.46 |
| VD **/intrapartum CC *** | 10 | 16 | FE | 0.4 |
| Whole labor duration | 5 | 10 | U = 23.5 | 0.86 |
| 2nd stage labor duration | 5 | 10 | U = 23.5 | 0.86 |
| 1st min Apgar score (VD **) | 5 | 10 | U = 19 | 0.51 |
| 5th min Apgar score (VD **) | 5 | 10 | U = 24 | 0.95 |
| Episiotomy (yes/no; VD **) | 5 | 10 | FE | 0.4 |
| Perineal tear (yes/no; VD **) | 5 | 10 | FE | 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuczera, A.; Opala-Berdzik, A.; Malá, J.; Sodowski, M.; Chmielewska, D. Comparison of First Childbirth Characteristics between Elite Judo Athletes and Non-Athletes: The Preliminary Retrospective Case–Control Study. Int. J. Environ. Res. Public Health 2022, 19, 13218. https://doi.org/10.3390/ijerph192013218
Kuczera A, Opala-Berdzik A, Malá J, Sodowski M, Chmielewska D. Comparison of First Childbirth Characteristics between Elite Judo Athletes and Non-Athletes: The Preliminary Retrospective Case–Control Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13218. https://doi.org/10.3390/ijerph192013218
Chicago/Turabian StyleKuczera, Anna, Agnieszka Opala-Berdzik, Jitka Malá, Marcin Sodowski, and Daria Chmielewska. 2022. "Comparison of First Childbirth Characteristics between Elite Judo Athletes and Non-Athletes: The Preliminary Retrospective Case–Control Study" International Journal of Environmental Research and Public Health 19, no. 20: 13218. https://doi.org/10.3390/ijerph192013218
APA StyleKuczera, A., Opala-Berdzik, A., Malá, J., Sodowski, M., & Chmielewska, D. (2022). Comparison of First Childbirth Characteristics between Elite Judo Athletes and Non-Athletes: The Preliminary Retrospective Case–Control Study. International Journal of Environmental Research and Public Health, 19(20), 13218. https://doi.org/10.3390/ijerph192013218