

Aerobic Training for Healthy Men and Women: Determining Intensities by Different Equations

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
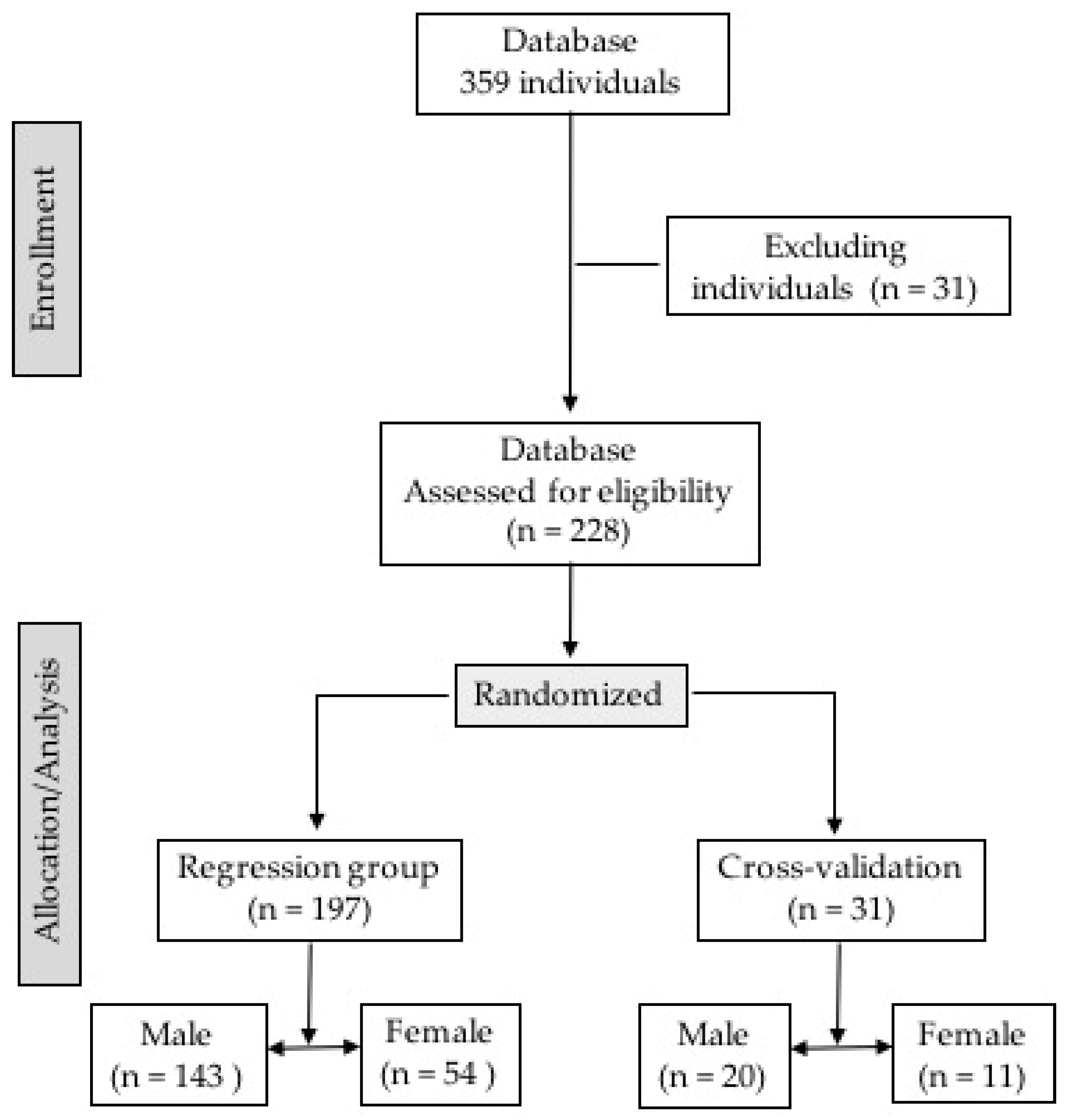
2.1. Study Design
2.2. Incremental Degree CPET Protocol
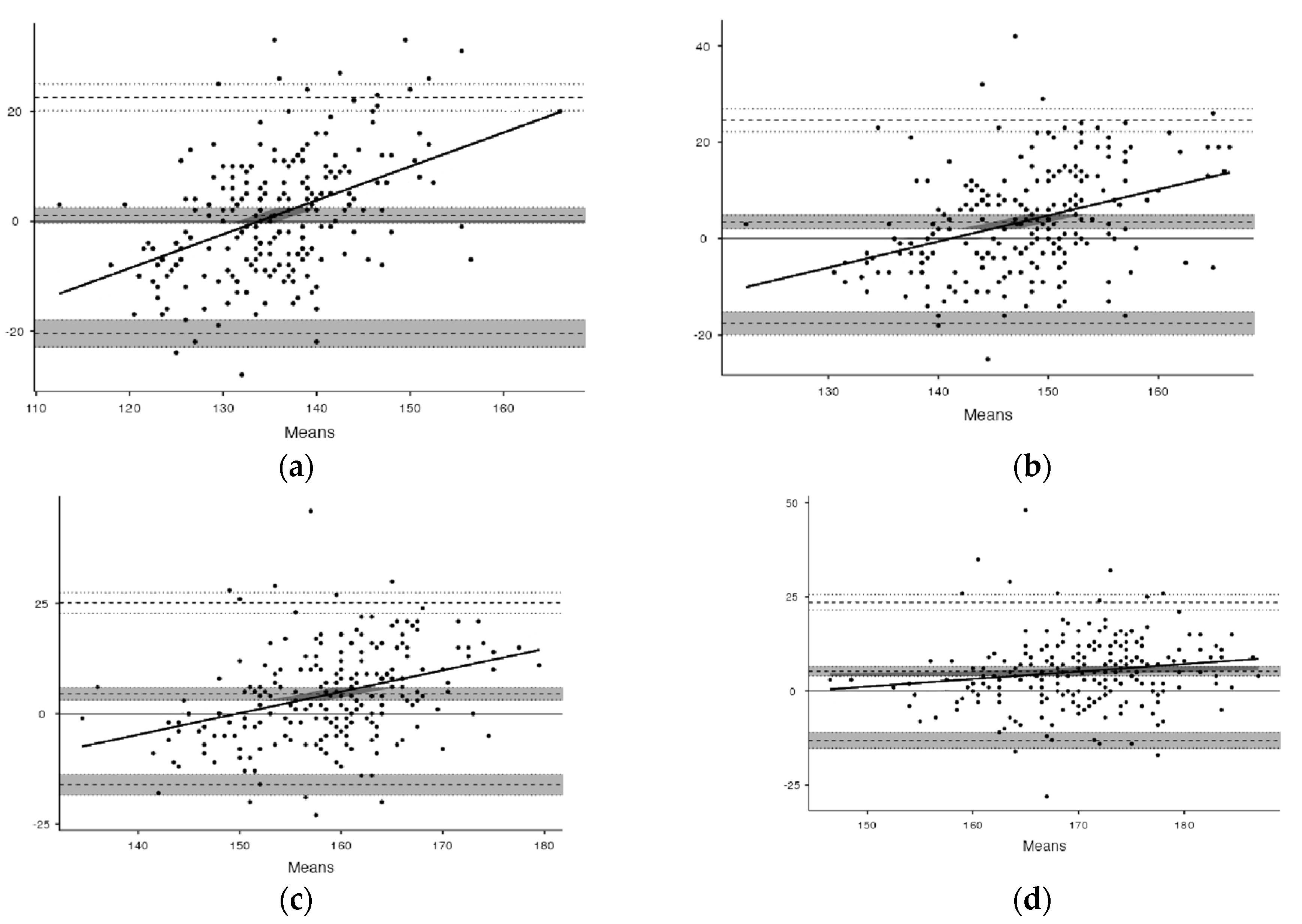
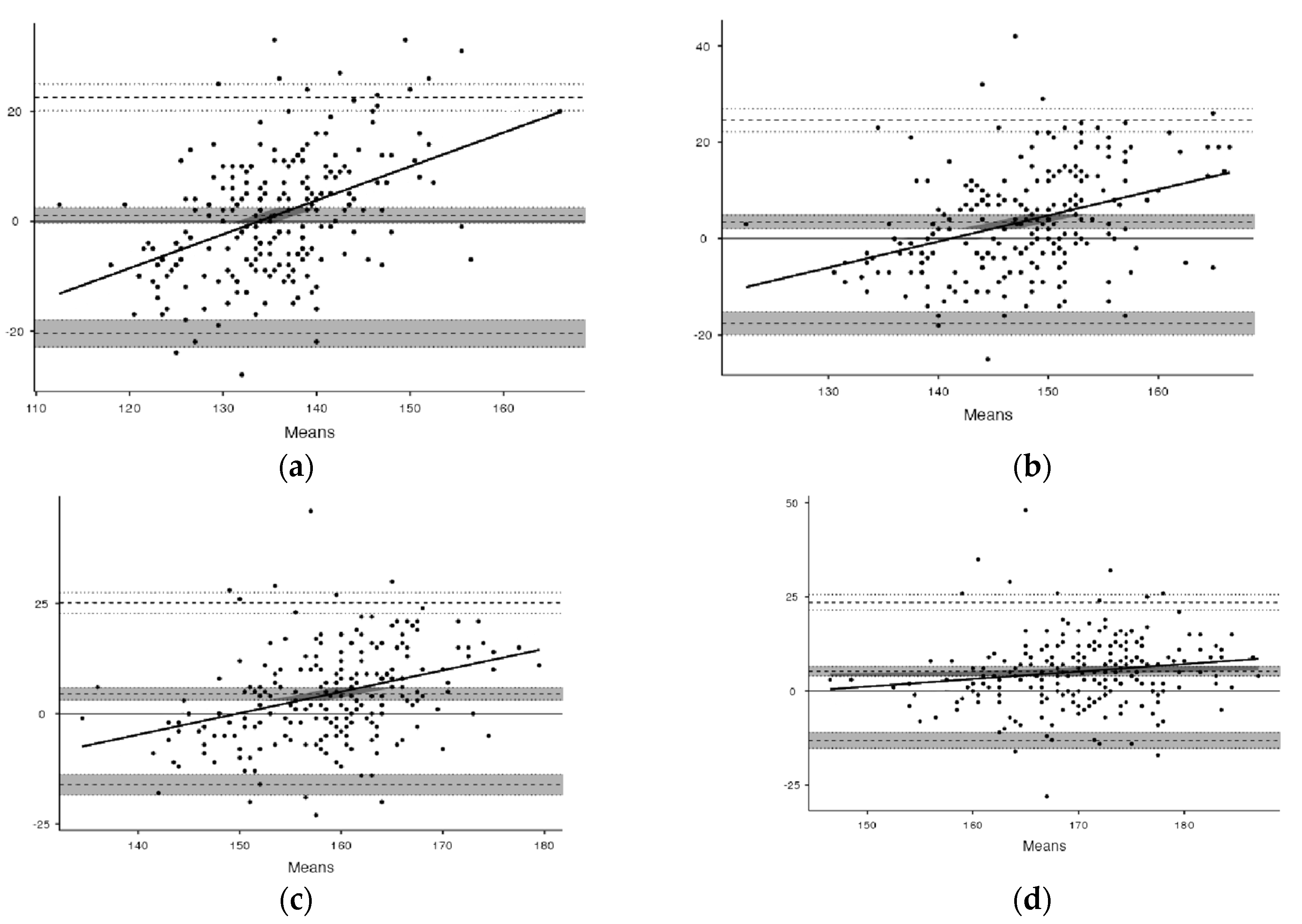
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. Int. Jt. Conf. Artif. Intell. 1995, 14, 1137–1145. [Google Scholar]
- Osuka, Y.; Kojima, N.; Wakaba, K.; Miyauchi, D.; Tanaka, K.; Kim, H. Effects of resistance training and/or beta-hydroxy-beta-methylbutyrate supplementation on muscle mass, muscle strength and physical performance in older women with reduced muscle mass: Protocol for a randomised, double-blind, placebo-controlled trial. BMJ Open 2019, 9, e025723. [Google Scholar] [CrossRef] [PubMed]
- Kisaka, T.; Stringer, W.W.; Koike, A.; Agostoni, P.; Wasserman, K. Mechanisms that modulate peripheral oxygen delivery during exercise in heart failure. Ann. Am. Thorac. Soc. 2017, 14, S40–S47. [Google Scholar] [CrossRef] [PubMed]
- Zuntz, N.; Geppert, J. Ueber die Natur der normalen Athemreize und den Ort ihrer Wirkung. Pflüger Arch. 1886, 38, 337–338. [Google Scholar] [CrossRef]
- Nobrega, A.C.L.; O’Leary, D.; Silva, B.; Marongiu, E.; Piepoli, M.F.; Crisafulli, A. Neural regulation of cardiovascular response to exercise: Role of central command and peripheral afferents. BioMed Res. Int. 2014, 2014, 478965. [Google Scholar] [CrossRef] [PubMed]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDONALD, A.; Russi, G.D.; Moudgil, V.K. Longitudinal modeling of the relationship between age and maximal heart rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Londeree, B.R.; Ames, S.A. Trend analysis of the vo2 max-hr regression. Med. Sci. Sports Exerc. 1976, 8, 122–125. [Google Scholar] [CrossRef]
- Karvonen, M.; Kentala, E.; Mustala, O. The effects of training on heart rate: A longitudinal study. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. Available online: http://www.ncbi.nlm.nih.gov/pubmed/13470504 (accessed on 3 October 2021).
- Swain, D.P.; Leutholtz, B.C. Heart rate reserve is equivalent to %VO2Reserve, not to %VO2max. Med. Sci. Sports Exerc. 1997, 29, 410–414. [Google Scholar] [CrossRef]
- Lounana, J.; Campion, F.; Noakes, T.D.; Medelli, J. Relationship between %HRmax, %HR Reserve, %V˙O2max, and %V˙O2 Reserve in Elite Cyclists. Med. Sci. Sports Exerc. 2007, 39, 350–357. [Google Scholar] [CrossRef]
- Hofmann, P.; Von Duvillard, S.P.; Seibert, F.J.; Pokan, R.; Wonisch, M.; Lemura, L.M.; Schwaberger, G. %HRmax target heart rate is dependent on heart rate performance curve deflection. Med. Sci. Sports Exerc. 2001, 33, 1726–1731. [Google Scholar] [CrossRef] [PubMed]
- Rolnick, N.; Schoenfeld, B.J. Can Blood Flow Restriction Used During Aerobic Training Enhance Body Composition in Physique Athletes? Strength Cond. J. 2020, 42, 37–47. [Google Scholar] [CrossRef]
- Peters, R.d.S.; Cruz, M.D.S.L.; Hernández-Mosqueira, C.; Martinez-Salazar, C.; Barbosa, F.P. The influence of body position on determining aerobic exercise intensity for healthy individuals. Int. J. Environ. Res. Public Health 2021, 18, 11773. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; LaMonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Herdy, A.H.; Uhlendorf, D. Reference values for cardiopulmonary exercise testing for sedentary and active men and women. Arq. Bras Cardiol. 2011, 96, 54–59. [Google Scholar] [CrossRef]
- Loe, H.; Rognmo, Ø.; Saltin, B.; Wisløff, U. Aerobic Capacity Reference Data in 3816 Healthy Men and Women 20–90 Years. PLoS ONE 2013, 8, e64319. [Google Scholar] [CrossRef]
- Mourão Jr, C.A. Biostatistical questions: The sample size. Rev. Interdiscip. Estud. Exp. Anim. Hum. Interdiscip. J. Exp. Stud. 2009, 1, 26–28. [Google Scholar] [CrossRef]
- Jackson, A.S.; Pollock, M.L. Generalized equations for predicting body density of men. Br. J. Nutr. 1978, 40, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Jackson, A.S.; Pollock, M.L.; Ward, A. Generalized equations for predicting body density of women. Med. Sci. Sports Exerc. 1980, 12, 175–181. Available online: http://www.ncbi.nlm.nih.gov/pubmed/7402053 (accessed on 5 October 2021). [CrossRef] [Green Version]
- Siri, W.E. Body composition from fluid spaces and density: Analysis of methods. 1961. Nutrition 1993, 9, 480–491. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8286893 (accessed on 5 October 2021).
- Weisman, I.M.; Weisman, I.M.; Marciniuk, D.; Martinez, F.J.; Sciurba, F.; Sue, D.; Myers, J. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Barbosa, F.P.; Cruz, M.S.L. Protocolo de Rampa vs. Escalonado: Análise do Consumo de Oxigênio e Frequência Cardíaca em Jovens. Rev. Bras. Ciência Mov. 2016, 24, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Jezek, F.; Randall, E.B.; Carlson, B.E.; Beard, D.A. Systems analysis of the mechanisms governing the cardiovascular response to changes in posture and in peripheral demand during exercise. J. Mol. Cell. Cardiol. 2022, 163, 33–55. [Google Scholar] [CrossRef] [PubMed]
- Brum, P.C.; Forjaz, C.L.d.M.; Tinucci, T.; Negrão, C.E. Adaptações agudas e crônicas do exercício físico no sistema cardiovascular. Rev. Paul. Educ. Fís. 2004, 18, 21–31. Available online: http://www.exerciciofisicoesaude.com.br/PDF/artigos/alessandra/2.pdf (accessed on 3 October 2021).
- Rivera-Brown, A.M.; Frontera, W.R. Principles of Exercise Physiology: Responses to Acute Exercise and Long-term Adaptations to Training. PMR 2012, 4, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Engels, H.-J.; Zhu, W.; Moffatt, R.J. An Empirical Evaluation of the Prediction of Maximal Heart Rate. Res. Q. Exerc. Sport 1998, 69, 94–98. [Google Scholar] [CrossRef]
- Policarpo, F.; Valdivia-Moral, P.; Luna-Cruz, M.D.S.; Véliz-Burgos, A.; Mansilla-Sepulveda, J.; Estay-Sepulveda, J.G. Comparison between different prescription methods for aerobic training in young adults. Sustainability 2019, 11, 6420. [Google Scholar] [CrossRef] [Green Version]
- Iannetta, D.; Keir, D.A.; Fontana, F.Y.; Inglis, E.C.; Mattu, A.T.; Paterson, D.H.; Pogliaghi, S.; Murias, J.M. Evaluating the Accuracy of Using Fixed Ranges of METs to Categorize Exertional Intensity in a Heterogeneous Group of Healthy Individuals: Implications for Cardiorespiratory Fitness and Health Outcomes. Sport Med. 2021, 51, 2411–2421. [Google Scholar] [CrossRef]
- Robergs, R.; Landwehr, R. The Surprising History of the “HRmax=220-age” Equation. JEPonline 2002, 5, 1–10. [Google Scholar]
- Eriksson, J.S.; Olsson, K.S.E.; Rosdahl, H.; Schantz, P. Heart Rate Methods Can Be Valid for Estimating Intensity Spectrums of Oxygen Uptake in Field Exercise. Front. Physiol. 2021, 12, 7566. [Google Scholar] [CrossRef]
- McConnell, A. Respiratory muscle training: Theory and practice. Elsevier Health Sci. 2013, 37–55. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Men (n = 143) | Women (n = 54) | General (n = 197) | |
|---|---|---|---|
| Age | 25.4 ± 6.4 | 22.2 ± 4.7 | 24.6 ± 6.2 |
| Height (cm) | 175.0 ± 6.4 | 162.4 ± 6.5 | 171.0 ± 8.6 |
| Body mass (kg) | 73.2 ± 10.0 | 57.1 ± 8.4 | 68.7 ± 11.8 |
| BMI (kg/m2) | 23.9 ± 2.9 | 21.6 ± 2.7 | 23.3 ± 3.0 |
| % body fat | 13.2 ± 6.4 | 20.1 ± 6.3 | 15.2 ± 7.1 |
| Equations | R | R2 | SEE | p Value |
|---|---|---|---|---|
| HRt 50% = 93.6 + (HRrest × 0.6) − (age × 0.2) | 0.69 | 0.48 | 5.4 | p = 0.01 |
| HRt 60% = 111.9 + (HRrest × 0.5) − (age × 0.2) | 0.58 | 0.34 | 6.0 | p = 0.01 |
| HRt 70% = 130.7 + (HRrest × 0.4) − (age × 0.2) | 0.51 | 0.26 | 6.6 | p = 0.01 |
| HRt 80% = 149.6 + (HRrest r × 0.3) − (age × 0.3) | 0.42 | 0.18 | 7.2 | p = 0.01 |
| HR/VO2 | Equations | |
|---|---|---|
| HRt50% | 135.7 ± 12.4 | 135.3 ± 4.7 |
| HRt60% | 148.8 ± 12.6 | 146.4 ± 4.1 ** |
| HRt70% | 161.0 ± 12.0 | 157.5 ± 3.7 ** |
| HRt80% | 172.6 ± 11.0 | 169.0 ± 3.7 ** |
| Men (n = 20) | Women Woman (n = 11) | |
|---|---|---|
| Age | 28.0 ± 6.7 | 29.0 ± 8.6 |
| Height (cm) | 175.1 ± 5.3 | 162.0 ± 8.3 |
| Body mass (kg) | 77.1 ± 13.0 | 60.0 ± 9.8 |
| BMI (kg/m2) | 25.0 ± 3.3 | 23.2 ± 3.3 |
| % body fat | 14.1 ± 6.7 | 25.1 ± 5.5 |
| HR/VO2 (bpm) | HR equation (bpm) | SEE (bpm) | |
|---|---|---|---|
| HRt50% | 129.6 ± 13.1 | 134.6 ± 7.6 * | 2.1 |
| HRt60% | 140.5 ± 12.8 | 145.4 ± 6.5 * | 2.1 |
| HRt70% | 154.1 ± 11.2 | 156.1 ± 5.6 | 2.0 |
| HRt80% | 165.1 ± 11.5 | 166.7 ± 5.1 | 2.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Policarpo Barbosa, F.; Oliveira, A.M.; Hernández-Mosqueira, C.; Pavez-Adasme, G.; Luna-Villouta, P.; Azocar-Gallardo, J. Aerobic Training for Healthy Men and Women: Determining Intensities by Different Equations. Int. J. Environ. Res. Public Health 2022, 19, 12862. https://doi.org/10.3390/ijerph191912862
Policarpo Barbosa F, Oliveira AM, Hernández-Mosqueira C, Pavez-Adasme G, Luna-Villouta P, Azocar-Gallardo J. Aerobic Training for Healthy Men and Women: Determining Intensities by Different Equations. International Journal of Environmental Research and Public Health. 2022; 19(19):12862. https://doi.org/10.3390/ijerph191912862
Chicago/Turabian StylePolicarpo Barbosa, Fernando, Andre M. Oliveira, Claudio Hernández-Mosqueira, Gustavo Pavez-Adasme, Pablo Luna-Villouta, and Jairo Azocar-Gallardo. 2022. "Aerobic Training for Healthy Men and Women: Determining Intensities by Different Equations" International Journal of Environmental Research and Public Health 19, no. 19: 12862. https://doi.org/10.3390/ijerph191912862
APA StylePolicarpo Barbosa, F., Oliveira, A. M., Hernández-Mosqueira, C., Pavez-Adasme, G., Luna-Villouta, P., & Azocar-Gallardo, J. (2022). Aerobic Training for Healthy Men and Women: Determining Intensities by Different Equations. International Journal of Environmental Research and Public Health, 19(19), 12862. https://doi.org/10.3390/ijerph191912862