
Transition to Motherhood: A Study on the Association between Somatic Symptoms during Pregnancy and Post-Partum Anxiety and Depression Symptoms


Abstract
1. Introduction
The Present Study
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Associations between Somatic Symptoms, Fear of Childbirth and Post-Partum Anxiety and Depression
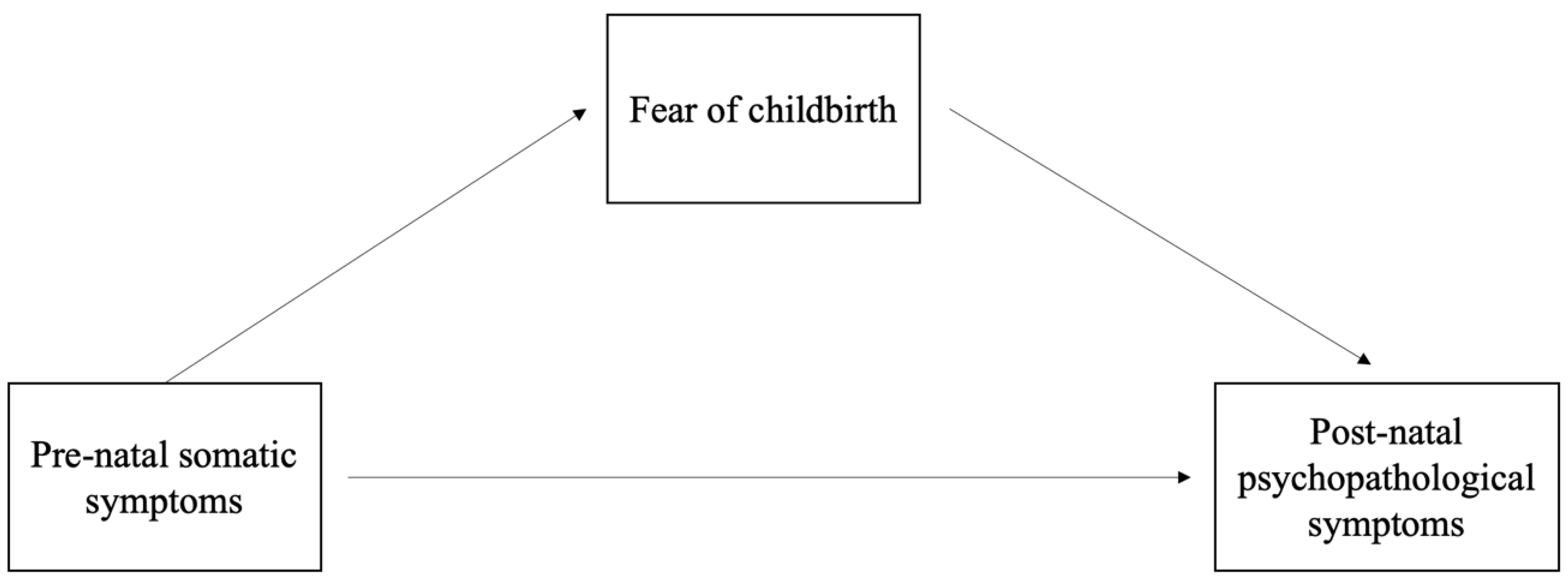
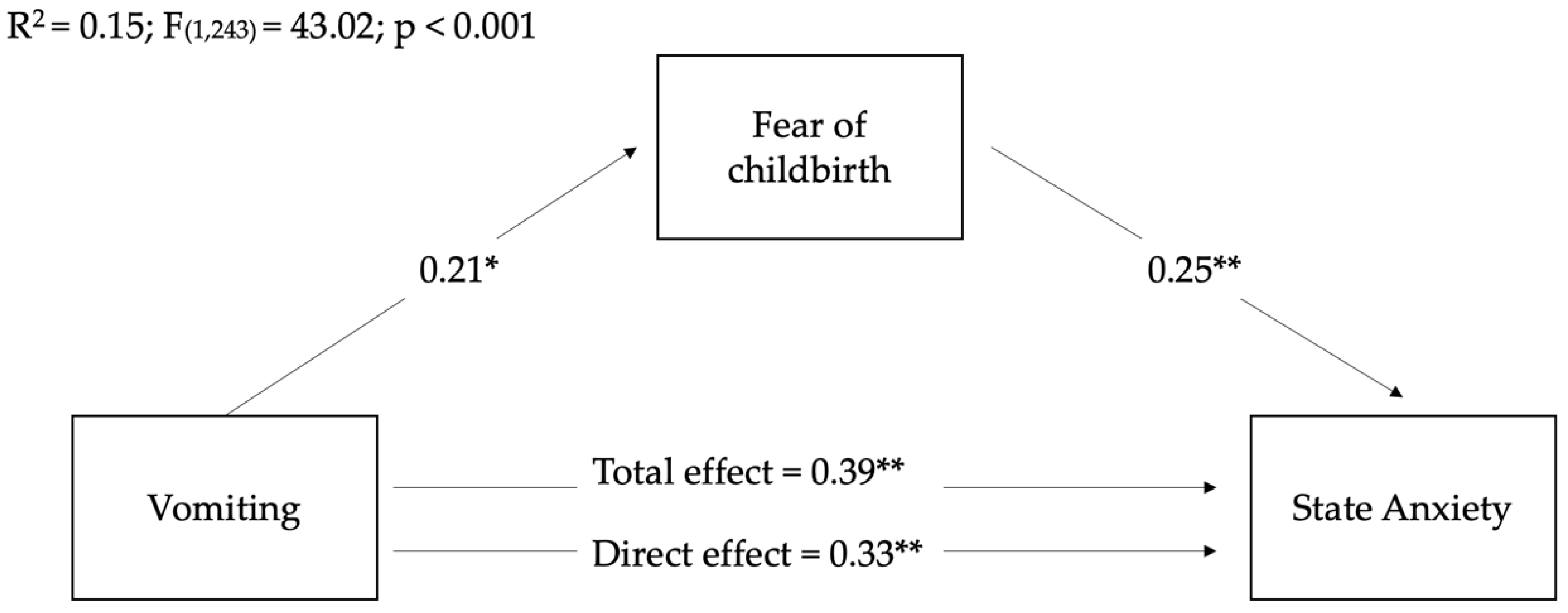
3.3. Fear of Childbirth Mediated the Relationship between Vomiting during Pregnancy and Post-Partum Anxiety and Depression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stern, D. The Motherhood Constellation: A Unified View of Parent–Infant Psychotherapy; Basic Books: New York, NY, USA, 1995. [Google Scholar]
- Bray, N.; Grasby, K.L.; Lind, P.A.; Painter, J.N.; Colodro-Conde, L.; Medland, S.E. The psychosocial impact of nausea and vomiting during pregnancy as a predictor of postpartum depression. J. Health Psychol. 2021, 26, 1061–1072. [Google Scholar] [CrossRef]
- Köken, G.; Yilmazer, M.; Cosar, E.N.; Sahin, F.G.K.; Cevrioglu, S.; Gecici, Ö. Nausea and vomiting in early pregnancy: Relationship with anxiety and depression. J. Psychosom. Obstet. Gynecol. 2008, 29, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Muchanga, S.M.J.; Eitoku, M.; Mbelambela, E.P.; Ninomiya, H.; Iiyama, T.; Komori, K.; Yasumitsu-Lovell, K.; Mitsuda, N.; Tozin, R.R.; Maeda, N.; et al. Association between nausea and vomiting of pregnancy and postpartum depression: The Japan Environment and Children’s Study. J. Psychosom. Obstet. Gynecol. 2020, 43, 2–10. [Google Scholar] [CrossRef]
- Jarvis, S.; Nelson-Piercy, C. Management of nausea and vomiting in pregnancy. BMJ 2011, 342, d3606. [Google Scholar] [CrossRef]
- Einarson, T.R.; Piwko, C.; Koren, G. Quantifying the global rates of nausea and vomiting of pregnancy: A meta-analysis. J. Popul. Ther. Clin. Pharmacol. 2013, 20, 171–183. [Google Scholar]
- Colodro-Conde, L.; Jern, P.; Johansson, A.; Sánchez-Romera, J.F.; Lind, P.A.; Painter, J.N.; Ordoñana, J.R.; Medland, S.E. Nausea and vomiting during pregnancy is highly heritable. Behav. Genet. 2016, 46, 481–491. [Google Scholar] [CrossRef]
- Beyazit, F.; Sahin, B. Effect of nausea and vomiting on anxiety and depression levels in early pregnancy. Eurasian J. Med. 2018, 50, 111. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, C.M. Nausea and vomiting in pregnancy. Br. J. Med. Psychol. 1984, 57, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Iliadis, S.I.; Axfors, C.; Johansson, S.; Skalkidou, A.; Mulic-Lutvica, A. Women with prolonged nausea in pregnancy have increased risk for depressive symptoms postpartum. Sci. Rep. 2018, 8, 1–9. [Google Scholar]
- Lee, N.M.; Saha, S. Nausea and vomiting of pregnancy. Gastroenterol. Clin. 2011, 40, 309–334. [Google Scholar] [CrossRef]
- Nylen, K.J.; Williamson, J.A.; O’Hara, M.W.; Watson, D.; Engeldinger, J. Validity of somatic symptoms as indicators of depression in pregnancy. Arch. Womens Ment. Health 2013, 16, 203–210. [Google Scholar] [CrossRef]
- Tsai, S.Y.; Lin, J.W.; Wu, W.W.; Lee, C.N.; Lee, P.L. Sleep disturbances and symptoms of depression and daytime sleepiness in pregnant women. Birth 2016, 43, 176–183. [Google Scholar] [CrossRef]
- Kramer, J.; Bowen, A.; Stewart, N.; Muhajarine, N. Nausea and vomiting of pregnancy: Prevalence, severity and relation to psychosocial health. MCN Am. J. Matern. Child Nurs. 2013, 38, 21–27. [Google Scholar] [CrossRef]
- Okun, M.L.; Hanusa, B.H.; Hall, M.; Wisner, K.L. Sleep complaints in late pregnancy and the recurrence of postpartum depression. Behav. Sleep Med. 2009, 7, 106–117. [Google Scholar] [CrossRef]
- Skouteris, H.; Germano, C.; Wertheim, E.H.; Paxton, S.J.; Milgrom, J. Sleep quality and depression during pregnancy: A prospective study. J. Sleep Res. 2008, 17, 217–220. [Google Scholar] [CrossRef]
- Aukia, L.; Paavonen, E.J.; Jänkälä, T.; Tolvanen, M.; Korja, R.; Karlsson, L.; Karlsson, H.; Polo-Kantola, P. Insomnia symptoms increase during pregnancy, but no increase in sleepiness-Associations with symptoms of depression and anxiety. Sleep Med. 2020, 72, 150–156. [Google Scholar] [CrossRef]
- Sarberg, M.; Bladh, M.; Svanborg, E.; Josefsson, A. Postpartum depressive symptoms and its association to daytime sleepiness and restless legs during pregnancy. BMC Pregnancy Childbirth 2016, 16, 1–8. [Google Scholar] [CrossRef]
- Saisto, T.; Halmesmäki, E. Fear of childbirth: A neglected dilemma. Acta Obstet. Et Gynecol. Scand. 2003, 82, 201–208. [Google Scholar] [CrossRef]
- Serçekuş, P.; Okumuş, H. Fears associated with childbirth among nulliparous women in Turkey. Midwifery 2009, 25, 155–162. [Google Scholar] [CrossRef]
- Molgora, S.; Fenaroli, V.; Prino, L.E.; Rollè, L.; Sechi, C.; Trovato, A.; Vismara, L.; Volpi, B.; Brustia, P.; Lucarelli, L.; et al. Fear of childbirth in primiparous Italian pregnant women: The role of anxiety, depression, and couple adjustment. Women Birth 2018, 31, 117–123. [Google Scholar] [CrossRef]
- Szeverenyi, P.; Poka, R.; Hetey, M.; Török, Z. Contents of childbirth-related fear among couples wishing the partner’s presence at delivery. J. Psychosom. Obstet. Gynecol. 1998, 19, 38–43. [Google Scholar] [CrossRef]
- Melender, H.L. Fears and coping strategies associated with pregnancy and childbirth in Finland. J. Midwifery Womens Health 2002, 47, 256–263. [Google Scholar] [CrossRef]
- Ayers, S. Fear of childbirth, postnatal post-traumatic stress disorder and midwifery care. Midwifery 2014, 30, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Richens, Y.; Smith, D.M.; Lavender, D.T. Fear of birth in clinical practice: A structured review of current measurement tools. Sex. Reprod. Healthc. 2018, 16, 98–112. [Google Scholar] [CrossRef]
- Bewley, S.; Cockburn, J. Responding to fear of childbirth. Lancet 2002, 359, 2128–2129. [Google Scholar] [CrossRef]
- Jomeen, J.; Martin, C.R.; Jones, C.; Marshall, C.; Ayers, S.; Burt, K.; Frodsham, L.; Horsch, A.; Midwinter, D.; O’Connell, M.; et al. Tokophobia and fear of birth: A workshop consensus statement on current issues and recommendations for future research. J. Reprod. Infant Psychol. 2020, 39, 2–15. [Google Scholar] [CrossRef]
- Haines, H.M.; Pallant, J.F.; Fenwick, J.; Gamble, J.; Creedy, D.K.; Toohill, J.; Hildingsson, I. Identifying women who are afraid of giving birth: A comparison of the fear of birth scale with the WDEQ-A in a large Australian cohort. Sex. Reprod. Healthc. 2015, 6, 204–210. [Google Scholar] [CrossRef]
- Badaoui, A.; Kassm, S.A.; Naja, W. Fear and anxiety disorders related to childbirth: Epidemiological and therapeutic issues. Curr. Psychiatry Rep. 2019, 21, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zar, M.; Wijma, K.; Wijma, B. Relations between anxiety disorders and fear of childbirth during late pregnancy. Clinic. Psychol. Psychother. 2002, 9, 122–130. [Google Scholar] [CrossRef]
- Johnson, R.; Slade, P. Does fear of childbirth during pregnancy predict emergency caesarean section? BJOG 2002, 109, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Wijma, K.; Wijma, B. Changes in anxiety during pregnancy and after delivery. In Reproductive life: Advances in Research in Psychosomatic Obstetrics and Gynaecology; The Parthenon Publishing Group: Carnforth, UK, 1992; pp. 81–88. [Google Scholar]
- Storksen, H.T.; Eberhard-Gran, M.; Garthus-Niegel, S.; Eskild, A. Fear of childbirth; the relation to anxiety and depression. Acta Obstet. Gynecol. Scand. 2012, 91, 237–242. [Google Scholar] [CrossRef]
- Vismara, L.; Rollè, L.; Agostini, F.; Sechi, C.; Fenaroli, V.; Molgora, S.; Neri, E.; Prino, L.E.; Odorisio, F.; Trovato, A.; et al. Perinatal parenting stress, anxiety, and depression outcomes in first-time mothers and fathers: A 3-to 6-months postpartum follow-up study. Front. Psychol. 2016, 7, 938. [Google Scholar] [CrossRef]
- Fisher, C.; Hauck, Y.; Fenwick, J. How social context impacts on women’s fears of childbirth: A Western Australian example. Soc. Sci. Med. 2006, 63, 64–75. [Google Scholar] [CrossRef]
- Räisänen, S.; Lehto, S.M.; Nielsen, H.S.; Gissler, M.; Kramer, M.R.; Heinonen, S. Fear of childbirth predicts postpartum depression: A population-based analysis of 511 422 singleton births in Finland. BMJ Open 2013, 3, e004047. [Google Scholar] [CrossRef] [PubMed]
- Klabbers, G.A.; Wijma, K.; van Bakel, H.J.; Paarlberg, K.M.; Vingerhoets, A.J. Resistance to fear of child birth and stability of mother-child bond. Early Child Dev. Care 2020, 190, 175–184. [Google Scholar] [CrossRef]
- Cimino, S.; Cerniglia, L.; Porreca, A.; Ballarotto, G.; Marzilli, E.; Simonelli, A. Impact of parental binge eating disorder: Exploring children’s emotional/behavioral problems and the quality of parent–child feeding interactions. Infant Ment. Health J. 2018, 39, 552–568. [Google Scholar] [CrossRef]
- Tambelli, R.; Cimino, S.; Cerniglia, L.; Ballarotto, G. Early maternal relational traumatic experiences and psychopathological symptoms: A longitudinal study on mother-infant and father-infant interactions. Sci. Rep. 2015, 5, 1–11. [Google Scholar] [CrossRef]
- Ballarotto, G.; Cerniglia, L.; Bozicevic, L.; Cimino, S.; Tambelli, R. Mother-child interactions during feeding: A study on maternal sensitivity in dyads with underweight and normal weight toddlers. Appetite 2021, 166, 105438. [Google Scholar] [CrossRef]
- Porreca, A.; Biringen, Z.; Parolin, M.; Saunders, H.; Ballarotto, G.; Simonelli, A. Emotional availability, neuropsychological functioning, and psychopathology: The context of parental substance use disorder. BioMed. Res. Int. 2018, 2018, 5359037. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Womens Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef]
- Tambelli, R.; Cerniglia, L.; Cimino, S.; Ballarotto, G. Parent-infant interactions in families with women diagnosed with postnatal depression: A longitudinal study on the effects of a psychodynamic treatment. Front. Psychol. 2015, 6, 1210. [Google Scholar] [CrossRef][Green Version]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. State-Trait Anxiety Inventory for Adults; Consulting Psychologists Press Inc.: Sunnyvale, CA, USA, 1983. [Google Scholar]
- Pedrabissi, L.; Santinello, M. Verifica Della Validità Dello STAI Forma Y di Spielberger; Giunti Organizzazioni Speciali: Florence, Italy, 1989. [Google Scholar]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postpartum depression–development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Benvenuti, P.; Ferrara, M.; Niccolai, C.; Valoriani, V.; Cox, J.L. The Edinburgh postnatal depression scale: Validation for an Italian sample. J. Affect Disord. 1999, 53, 137–141. [Google Scholar] [CrossRef]
- Bergink, V.; Kooistra, L.; Lambregtse-van den Berg, M.P.; Wijnen, H.; Bunevicius, R.; Van Baar, A.; Pop, V. Validation of the Edinburgh Depression Scale during pregnancy. J. Psychosom. Res. 2011, 70, 385–389. [Google Scholar] [CrossRef]
- Wijma, K.; Wijma, B.; Zar, M. Psychometric aspects of the WDEQ; a new questionnaire for the measurement of fear of childbirth. J. Psychosom. Obstet. Gynecol. 1998, 19, 84–97. [Google Scholar] [CrossRef]
- Fenaroli, V.; Saita, E. Fear of childbirth: A contribution to the validation of the Italian version of the Wijma Delivery Expectancy/Experience Questionnaire (WDEQ). TPM Test Psychom. Methodol. Appl. Psychol. 2013, 20, 131–154. [Google Scholar]
- Calderani, E.; Giardinelli, L.; Scannerini, S.; Arcabasso, S.; Compagno, E.; Petraglia, F.; Ricca, V. Tocophobia in the DSM-5 era: Outcomes of a new cut-off analysis of the Wijma delivery expectancy/experience questionnaire based on clinical presentation. J. Psychosom. Res. 2019, 116, 37–43. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford publications: New York, NY, USA, 2017. [Google Scholar]
- Coronado, P.J.; Fasero, M.; Álvarez-Sánchez, Á.; Rey, E. Prevalence and persistence of nausea and vomiting along the pregnancy. Rev. Esp. Enferm. Dig. 2014, 106, 318–324. [Google Scholar]
- O’Connell, M.A.; Leahy-Warren, P.; Khashan, A.S.; Kenny, L.C.; O’Neill, S.M. Worldwide prevalence of tocophobia in pregnant women: Systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 907–920. [Google Scholar] [CrossRef]
- Hu, M.; Zhou, Y.; Xue, M.; Ren, Y.; Li, S.; Wang, R.; Qi, L.; Zeng, L.; Liu, Z.; Qian, W.; et al. The prevalence and correlates of peripartum depression in different stages of pregnancy during COVID-19 pandemic in China. BMC Pregnancy Childbirth 2022, 22, 1–13. [Google Scholar] [CrossRef]
- Reck, C.; Struben, K.; Backenstrass, M.; Stefenelli, U.; Reinig, K.; Fuchs, T.; Sohn, C.; Mundt, C. Prevalence, onset and comorbidity of postpartum anxiety and depressive disorders. Acta Psychiatr. Scand. 2008, 118, 459–468. [Google Scholar] [CrossRef]
- Suárez-Rico, B.; Estrada-Gutierrez, G.; Sánchez-Martínez, M.; Perichart-Perera, O.; Rodríguez-Hernández, C.; González-Leyva, C.; Osorio-Valencia, E.; Cardona-Pérez, A.; Helguera-Repetto, A.; Sosa, S.E.Y.; et al. Prevalence of depression, anxiety, and perceived stress in postpartum Mexican women during the COVID-19 lockdown. Int. J. Environ. Res. Public Health 2021, 18, 4627. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; San Tam, W.W.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Babore, A.; Trumello, C.; Lombardi, L.; Candelori, C.; Chirumbolo, A.; Cattelino, E.; Baiocco, R.; Bramanti, S.M.; Viceconti, M.L.; Pignataro, S.; et al. Mothers’ and children’s mental health during the COVID-19 pandemic lockdown: The mediating role of parenting stress. Child Psychiatry Hum. Dev. 2021, 1–13. [Google Scholar] [CrossRef]
- Dekkers, G.W.; Broeren, M.A.; Truijens, S.E.; Kop, W.J.; Pop, V.J. Hormonal and psychological factors in nausea and vomiting during pregnancy. Psychol. Med. 2020, 50, 229–236. [Google Scholar] [CrossRef]
- Mariani, R.; Renzi, A.; Di Trani, M.; Trabucchi, G.; Danskin, K.; Tambelli, R. The impact of coping strategies and perceived family support on depressive and anxious symptomatology during the coronavirus pandemic (COVID-19) lockdown. Front. Psychiatry 2020, 11, 587724. [Google Scholar] [CrossRef]
- Babore, A.; Bramanti, S.M.; Lombardi, L.; Stuppia, L.; Trumello, C.; Antonucci, I.; Cavallo, A. The role of depression and emotion regulation on parenting stress in a sample of mothers with cancer. Support. Care Cancer 2019, 27, 1271–1277. [Google Scholar] [CrossRef]
- Babore, A.; Picconi, L.; Candelori, C.; Trumello, C. The emotional relationship with parents: A validation study of the LEAP among Italian adolescents. Eur. J. Dev. Psychol. 2014, 11, 728–739. [Google Scholar] [CrossRef]
- Cimino, S.; Cerniglia, L.; Ballarotto, G.; Marzilli, E.; Pascale, E.; D’Addario, C.; Adriani, W.; Tambelli, R. DNA methylation at the DAT promoter and risk for psychopathology: Intergenerational transmission between school-age youths and their parents in a community sample. Front. Psychiatry 2018, 8, 303. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Bevilacqua, A.; Ballarotto, G.; Marzilli, E.; Adriani, W.; Tambelli, R. Patterns of DNA methylation at specific loci of the dopamine transporter 1 gene and psychopathological risk in trios of mothers, fathers and children. Eur. J. Dev. Psychol. 2021, 18, 545–572. [Google Scholar] [CrossRef]
- Cimino, S.; Cerniglia, L.; Tambelli, R.; Ballarotto, G.; Erriu, M.; Paciello, M.; Oppenheim, D.; Koren-Karie, N. Dialogues about emotional events between mothers with anxiety, depression, anorexia nervosa, and no diagnosis and their children. Parenting 2020, 20, 69–82. [Google Scholar] [CrossRef]
- Werner, E.; Miller, M.; Osborne, L.M.; Kuzava, S.; Monk, C. Preventing postpartum depression: Review and recommendations. Arch. Womens Ment. Health 2015, 18, 41–60. [Google Scholar] [CrossRef]
- Šebela, A.; Hanka, J.; Mohr, P. Etiology, risk factors, and methods of postpartum depression prevention. Ceska Gynekol. 2018, 83, 468–473. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| I Trimester | II Trimester | III Trimester | |
|---|---|---|---|
| Sleep duration | |||
| 3–5 h per day | 21 (8.10%) | 33 (12.80%) | 78 (30.20%) |
| 6–8 h per day | 97 (37.60%) | 114 (44.20%) | 112 (43.40%) |
| 8–10 h per day | 102 (39.50%) | 103 (39.90%) | 52 (20.20%) |
| >10 h per day | 38 (14.70%) | 8 (3.10%) | 14 (5.40%) |
| Nausea | |||
| Never | 67 (26.0%) | 133 (51.60%) | 132 (51.20%) |
| <2 h per day | 65 (25.20%) | 75 (29.10%) | 69 (26.70%) |
| 3–5 h per day | 69 (26.70%) | 30 (11.60%) | 38 (14.70%) |
| >6 h per day | 57 (22.10%) | 20 (7.80%) | 17 (6.60%) |
| Vomiting | |||
| Never | 152 (58.90%) | 198 (76.70%) | 214 (82.90%) |
| once per day | 59 (22.90%) | 40 (15.50%) | 32 (12.40%) |
| 2–3 times per day | 21 (8.10%) | 8 (3.10%) | 3 (1.20%) |
| >3 times per day | 24 (9.30%) | 10 (3.90%) | 7 (2.70%) |
| Average Scores | SD | Minimum | Maximum | |
|---|---|---|---|---|
| WDEQ-B | 59.19 a | 27.19 | 13 | 145 |
| STAI-S | 40.05 b | 12.34 | 20 | 80 |
| EPDS | 8.11 c | 5.69 | 0 | 27 |
| STAI-S | EPDS | WDEQ-B | |
|---|---|---|---|
| Daily sleep duration | −0.08 | −0.12 | −0.09 |
| Nausea | 0.11 | 0.06 | 0.03 |
| Vomiting | 0.39 ** | 0.49 ** | 0.17 * |
| WDEQ-B | 0.34 ** | 0.39 ** | 1 |
| Indirect Effect | Effect (BootSE) | LLCI | ULCI |
|---|---|---|---|
| Vomiting WDEQ-B State Anxiety | 0.05 (0.02) | 0.02 | 0.10 |
| Vomiting WDEQ-B Depression | 0.06 (0.02) | 0.01 | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tambelli, R.; Ballarotto, G.; Trumello, C.; Babore, A. Transition to Motherhood: A Study on the Association between Somatic Symptoms during Pregnancy and Post-Partum Anxiety and Depression Symptoms. Int. J. Environ. Res. Public Health 2022, 19, 12861. https://doi.org/10.3390/ijerph191912861
Tambelli R, Ballarotto G, Trumello C, Babore A. Transition to Motherhood: A Study on the Association between Somatic Symptoms during Pregnancy and Post-Partum Anxiety and Depression Symptoms. International Journal of Environmental Research and Public Health. 2022; 19(19):12861. https://doi.org/10.3390/ijerph191912861
Chicago/Turabian StyleTambelli, Renata, Giulia Ballarotto, Carmen Trumello, and Alessandra Babore. 2022. "Transition to Motherhood: A Study on the Association between Somatic Symptoms during Pregnancy and Post-Partum Anxiety and Depression Symptoms" International Journal of Environmental Research and Public Health 19, no. 19: 12861. https://doi.org/10.3390/ijerph191912861
APA StyleTambelli, R., Ballarotto, G., Trumello, C., & Babore, A. (2022). Transition to Motherhood: A Study on the Association between Somatic Symptoms during Pregnancy and Post-Partum Anxiety and Depression Symptoms. International Journal of Environmental Research and Public Health, 19(19), 12861. https://doi.org/10.3390/ijerph191912861