

Pregnancy Complications in Pandemics: Is Pregnancy-Related Anxiety a Possible Physiological Risk Factor?
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants and Procedures
2.3. Measures
- Study demographics: questions related to age, nationality, education level, and job status.
- Physiological parameters: questions related to pregnancy history, trimester, number of previous pregnancies, number of previous miscarriages, comorbidities, and body mass index.
- Questions related to stress (ability to control personal life and problems) and quality of life (performing daily activities and taking care of others) during the COVID-19 pandemic.
- A validated scale, the generalized anxiety disorder assessment (GAD-7), was used to measure participant’s anxiety levels [10].
2.4. GAD-7 Scale
2.5. Statistical Analysis
3. Results
3.1. Study Demographics
3.2. Physiological Parameters
3.3. Anxiety Level and Its Correlation with Study Demographics
3.4. Anxiety Level and Its Correlation with Physiological Parameters
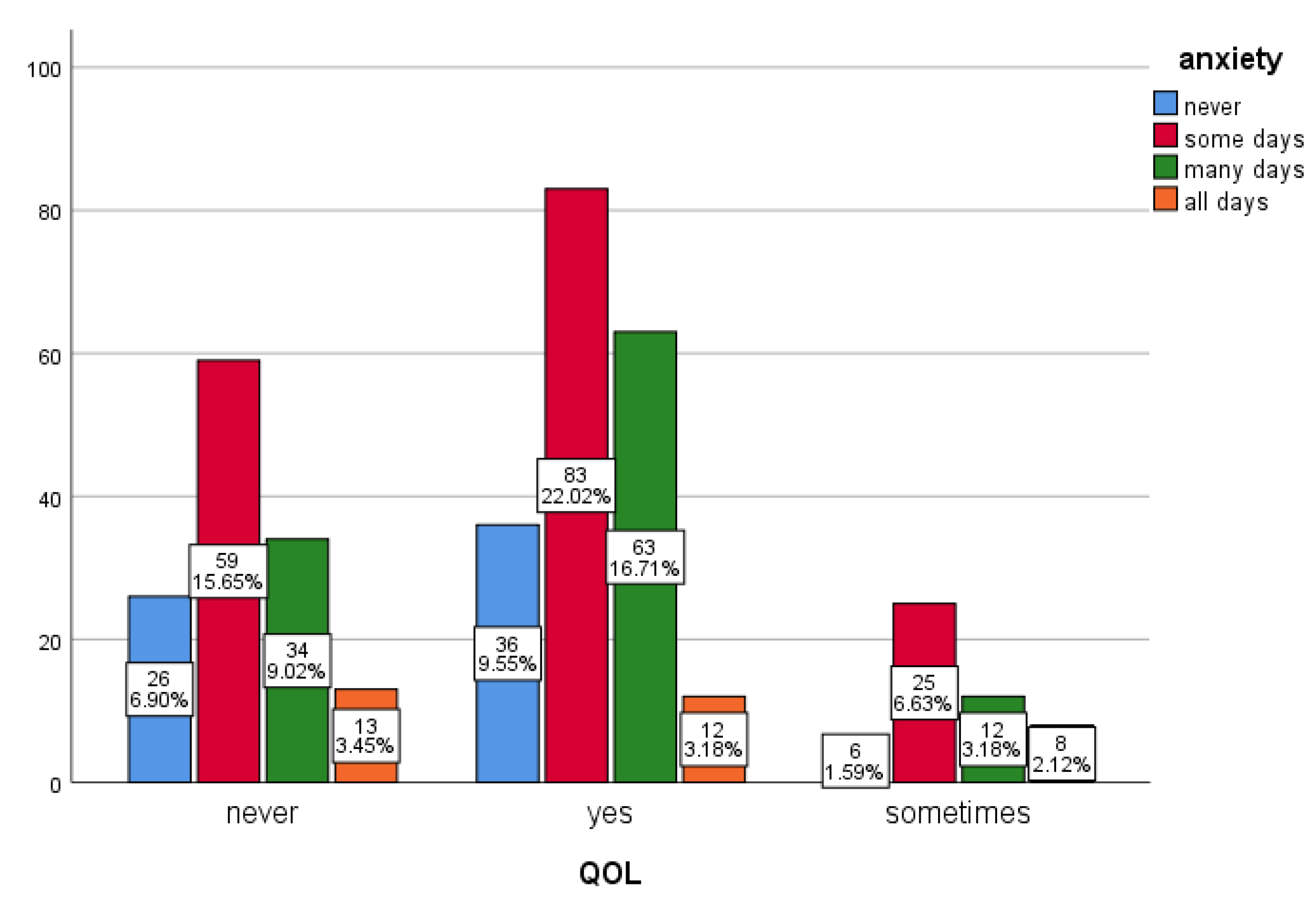
3.5. Anxiety Level and Its Correlation with Attitude toward the Pandemic
4. Discussion
5. Recommendations
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woodworth, K.R.; Olsen, E.O.M.; Neelam, V.; Lewis, E.L.; Galang, R.R.; Oduyebo, T.; Aveni, K.; Yazdy, M.M.; Harvey, E.; Longcore, N.D.; et al. Birth and Infant Outcomes Following Laboratory-Confirmed SARS-CoV-2 Infection in Pregnancy—SET-NET, 16 Jurisdictions, 29 March–14 October 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1635–1640. [Google Scholar] [CrossRef]
- Di Mascio, D.; Khalil, A.; Saccone, G.; Rizzo, G.; Buca, D.; Liberati, M.; Vecchiet, J.; Nappi, L.; Scambia, G.; Berghella, V.; et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100107. [Google Scholar] [CrossRef]
- Christian, L.M. Physiological reactivity to psychological stress in human pregnancy: Current knowledge and future directions. Prog. Neurobiol. 2012, 99, 106–116. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19), in StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- da Silva, M.L.; Rocha, R.S.B.; Buheji, M.; Jahrami, H.; Cunha, K.D.C. A systematic review of the prevalence of anxiety symptoms during coronavirus epidemics. J. Health Psychol. 2021, 26, 115–125. [Google Scholar] [CrossRef]
- Bigalke, J.A.; Greenlund, I.M.; Carter, J.R. Sex differences in self-report anxiety and sleep quality during COVID-19 stay-at-home orders. Biol. Sex Differ. 2020, 11, 56. [Google Scholar] [CrossRef]
- Almeida, M.; Shrestha, A.D.; Stojanac, D.; Miller, L.J. The impact of the COVID-19 pandemic on women’s mental health. Arch. Women’s Ment. Health 2020, 23, 741–748. [Google Scholar] [CrossRef]
- Loomans, E.M.; Van Dijk, A.E.; Vrijkotte, T.G.; Van Eijsden, M.; Stronks, K.; Gemke, R.J.B.J.; Van den Bergh, B.R.H. Psychosocial stress during pregnancy is related to adverse birth outcomes: Results from a large multi-ethnic community-based birth cohort. Eur. J. Public Health 2013, 23, 485–491. [Google Scholar] [CrossRef]
- Radoš, S.N.; Tadinac, M.; Herman, R. Anxiety During Pregnancy and Postpartum: Course, Predictors and Comorbidity with Postpartum Depression. Acta Clin. Croat. 2018, 57, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Swinson, R.P. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evidence-Based Med. 2006, 11, 184. [Google Scholar] [CrossRef]
- Perez, A.; Panagiotopoulou, E.; Curtis, P.; Roberts, R. Barriers and facilitators to mood and confidence in pregnancy and early parenthood during COVID-19 in the UK: Mixed-methods synthesis survey. BJPsych Open 2021, 7, e107. [Google Scholar] [CrossRef]
- Alqahtani, A.H.; Al-Khedair, K.; Al-Jeheiman, R.; Al-Turki, H.A.; Al Qahtani, N.H. Anxiety and depression during pregnancy in women attending clinics in a University Hospital in Eastern province of Saudi Arabia: Prevalence and associated factors. Int. J. Women’s Health 2018, 10, 101–108. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Mappa, I.; Distefano, F.A.; Rizzo, G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: A prospectic observational study. J. Périnat. Med. 2020, 48, 545–550. [Google Scholar] [CrossRef]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, January 22–June 7, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef]
- Pinheiro, R.L.; Areia, A.L.; Mota-Pinto, A.; Donato, H. Advanced Maternal Age: Adverse Outcomes of Pregnancy. A Meta-Analysis. Acta Med. Port. 2019, 32, 219–226. [Google Scholar] [CrossRef]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef]
- Panagiotakopoulos, L.; Myers, T.R.; Gee, J.; Lipkind, H.S.; Kharbanda, E.O.; Ryan, D.S.; Williams, J.T.; Naleway, A.L.; Klein, N.P.; Hambidge, S.J.; et al. SARS-CoV-2 Infection Among Hospitalized Pregnant Women: Reasons for Admission and Pregnancy Characteristics—Eight U.S. Health Care Centers, March 1-May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1355–1359. [Google Scholar] [CrossRef] [PubMed]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatr. 2020, 51, 102092. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Vlisides-Henry, R.D.; Deboeck, P.R.; Grill-Velasquez, W.; Mackey, S.; Ramadurai, D.K.; Urry, J.O.; Neff, D.; Terrell, S.; Gao, M.; Thomas, L.R.; et al. Behavioral and physiological stress responses: Within-person concordance during pregnancy. Biol. Psychol. 2021, 159, 108027. [Google Scholar] [CrossRef] [PubMed]
- Ostlund, B.D.; Vlisides-Henry, R.D.; Crowell, S.E.; Raby, K.L.; Terrell, S.; Brown, M.A.; Tinajero, R.; Shakiba, N.; Monk, C.; Shakib, J.H.; et al. Intergenerational transmission of emotion dysregulation: Part II. Developmental origins of newborn neurobehavior. Dev. Psychopathol. 2019, 31, 833–846. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Ding, Y.; Guo, W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychol. 2020, 11, 617001. [Google Scholar] [CrossRef] [PubMed]
- Adamson, B.; Letourneau, N.; Lebel, C. Prenatal maternal anxiety and children’s brain structure and function: A systematic review of neuroimaging studies. J. Affect. Disord 2018, 241, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Marcinko, V.M.; Marcinko, D.; Dordević, V.; Oresković, S. Anxiety and depression in pregnant women with previous history of spontaneous abortion. Coll. Antropol. 2011, 35, 225–228. [Google Scholar]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Havens, K.L.; Starnes, C.P.; Pickering, T.A.; Brito, N.H.; Hendrix, C.L.; Thomason, M.E.; Vatalaro, T.C.; Smith, B.A. Changes in social support of pregnant and postnatal mothers during the COVID-19 pandemic. Midwifery 2021, 103, 103162. [Google Scholar] [CrossRef] [PubMed]
- Colli, C.; Penengo, C.; Garzitto, M.; Driul, L.; Sala, A.; Degano, M.; Preis, H.; Lobel, M.; Balestrieri, M. Prenatal Stress and Psychiatric Symptoms During Early Phases of the COVID-19 Pandemic in Italy. Int. J. Women’s Health 2021, 13, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Ravaldi, C.; Ricca, V.; Wilson, A.; Homer, C.; Vannacci, A. Previous psychopathology predicted severe COVID-19 concern, anxiety, and PTSD symptoms in pregnant women during “lockdown” in Italy. Arch. Womens Ment. Health 2020, 23, 783–786. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Nationality: | |
| Non-Saudi | 17 (4.51) |
| Saudi | 360 (95.5) |
| Age: | |
| 18–26 | 115 (30.5) |
| 27–34 | 133 (35.3) |
| 35–43 | 120 (31.8) |
| >43 | 9 (2.4) |
| Education: | |
| Primary | 2 (0.53) |
| Secondary school | 6 (1.59) |
| High school | 51 (13.5) |
| University degree | 266 (70.6) |
| Post-graduate | 52 (13.8) |
| Employment: | |
| Health care practitioner | 21 (5.57) |
| Non health care practitioner | 130 (34.5) |
| Student | 40 (10.6) |
| Unemployed | 186 (49.3) |
| Monthly income: | |
| <5000 SAR | 138 (36.6) |
| 5000–10,000 SAR | 129 (34.2) |
| >10,000 SAR | 110 (29.2) |
| Accommodation type: | |
| Owned residence | 214 (56.8) |
| Rented housing | 163 (43.2) |
| Living with husband: | |
| No | 4 (1.06) |
| Yes | 373 (98.9) |
| Existence of comorbidities such as diabetes and hypertension: | |
| No | 318 (84.4) |
| Yes | 59 (15.6) |
| Previously infected with COVID-19: | |
| Yes | 100 (26.5%) |
| No | 277 (73.5) |
| Characteristics | n (%) |
|---|---|
| Pregnancy trimester: | |
| 1 to 3 | 108 (28.6) |
| 4 to 6 | 116 (30.8) |
| 7 to 9 | 153 (40.6) |
| Pregnancy order: | |
| First | 135 (35.8) |
| Second to fourth | 155 (41.1) |
| Fifth to seventh | 76 (20.2) |
| Eighth and more | 11 (2.92) |
| Previous miscarriages: | |
| None | 272 (72.1) |
| 1 to 3 | 99 (26.3) |
| >3 | 6 (1.59) |
| Planned pregnancy: | |
| No | 157 (41.6) |
| Yes | 220 (58.4) |
| Pregnancy news had a negative impact: | |
| No | 320 (84.9) |
| Yes | 57 (15.1) |
| GAD-7 Category: | n (%) |
|---|---|
| None (0–4) | 93 (24.7) |
| Mild (5–9) | 156 (41.4) |
| Moderate (10–14) | 77 (20.4) |
| Severe (>15) | 51 (13.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abahussain, E.; Al-Otaibi, M.; Al-Humaidi, K.; Al-Mutairi, S.; Al-Khatir, A.; Abualnaja, A.; Al-Mazidi, S. Pregnancy Complications in Pandemics: Is Pregnancy-Related Anxiety a Possible Physiological Risk Factor? Int. J. Environ. Res. Public Health 2022, 19, 12119. https://doi.org/10.3390/ijerph191912119
Abahussain E, Al-Otaibi M, Al-Humaidi K, Al-Mutairi S, Al-Khatir A, Abualnaja A, Al-Mazidi S. Pregnancy Complications in Pandemics: Is Pregnancy-Related Anxiety a Possible Physiological Risk Factor? International Journal of Environmental Research and Public Health. 2022; 19(19):12119. https://doi.org/10.3390/ijerph191912119
Chicago/Turabian StyleAbahussain, Eman, Manal Al-Otaibi, Khulud Al-Humaidi, Sultanah Al-Mutairi, Alexandra Al-Khatir, Amani Abualnaja, and Sarah Al-Mazidi. 2022. "Pregnancy Complications in Pandemics: Is Pregnancy-Related Anxiety a Possible Physiological Risk Factor?" International Journal of Environmental Research and Public Health 19, no. 19: 12119. https://doi.org/10.3390/ijerph191912119
APA StyleAbahussain, E., Al-Otaibi, M., Al-Humaidi, K., Al-Mutairi, S., Al-Khatir, A., Abualnaja, A., & Al-Mazidi, S. (2022). Pregnancy Complications in Pandemics: Is Pregnancy-Related Anxiety a Possible Physiological Risk Factor? International Journal of Environmental Research and Public Health, 19(19), 12119. https://doi.org/10.3390/ijerph191912119