



Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
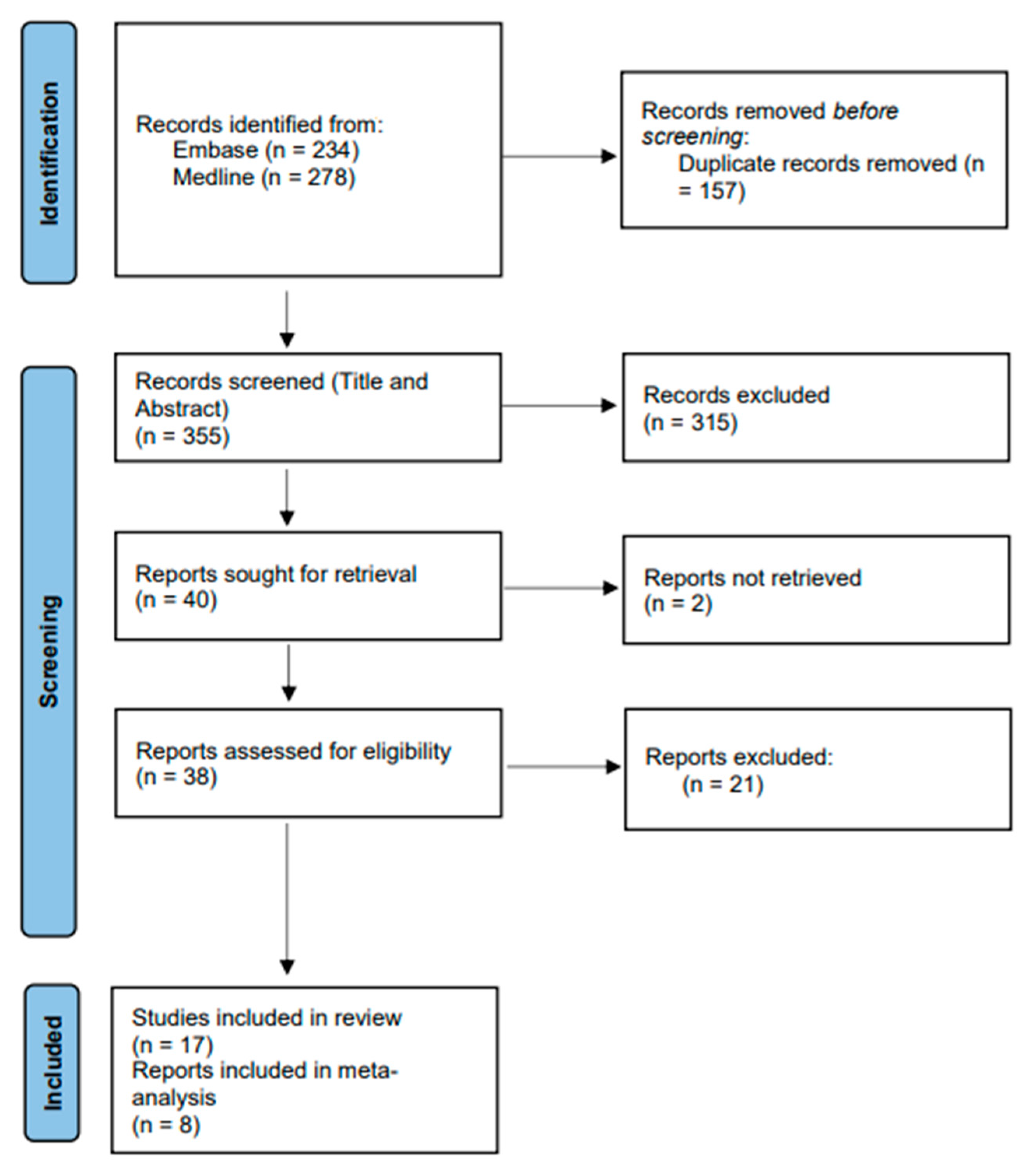
2.2. Data Screening and Synthesis
2.3. Quality Assessment
3. Results
3.1. Summary of Included Studies
3.2. iNO Administration
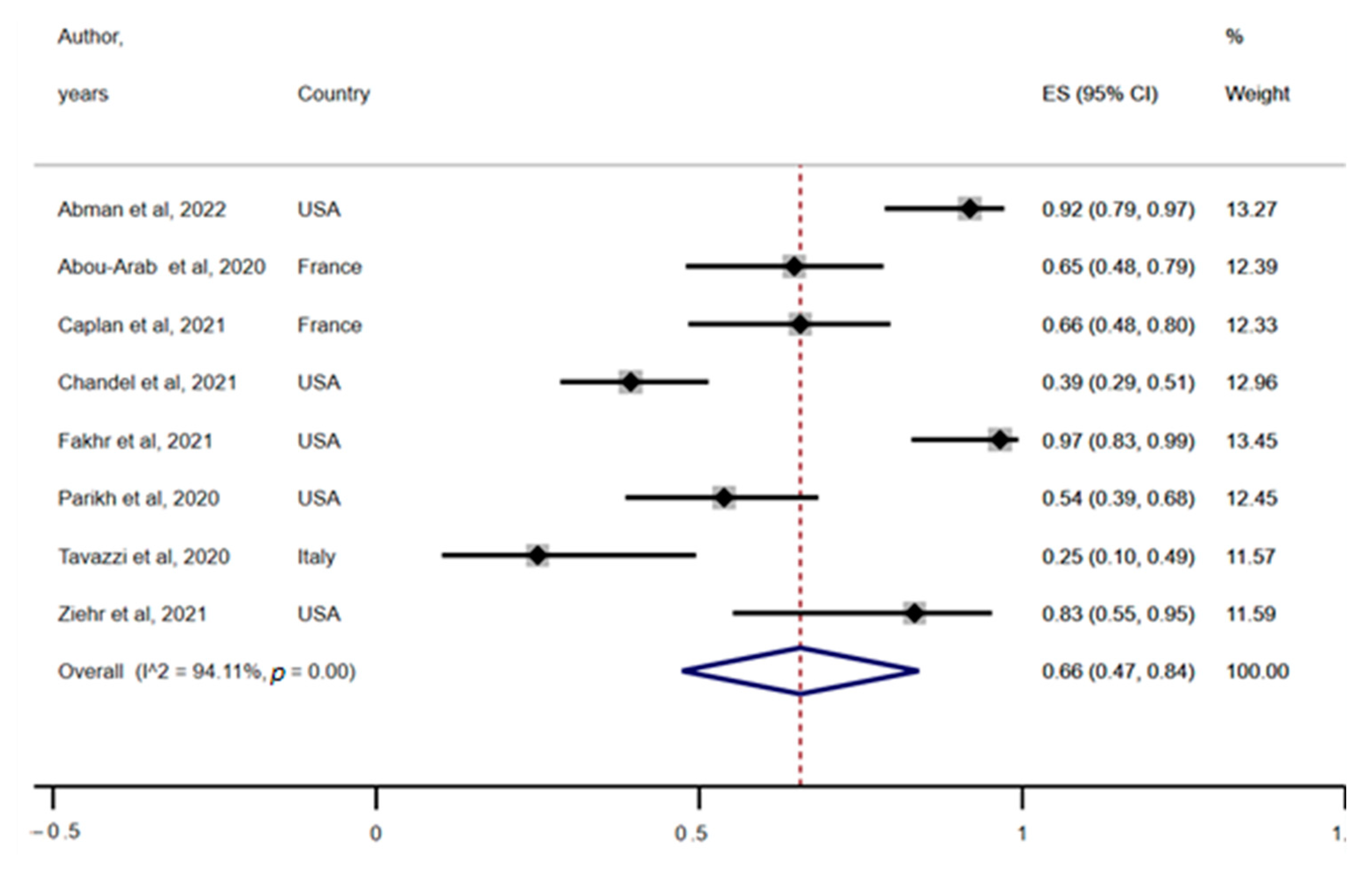
3.3. Response to iNO
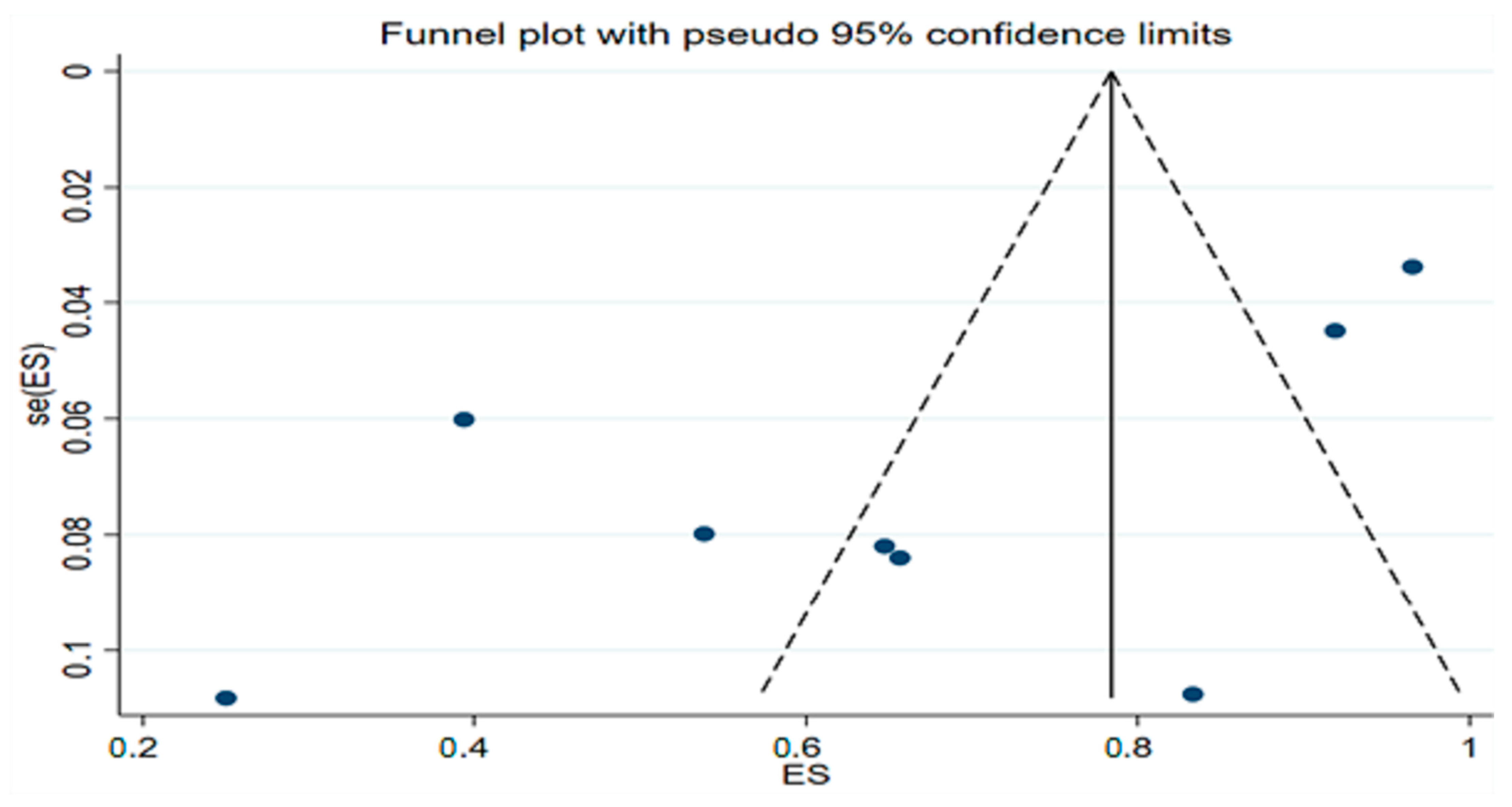
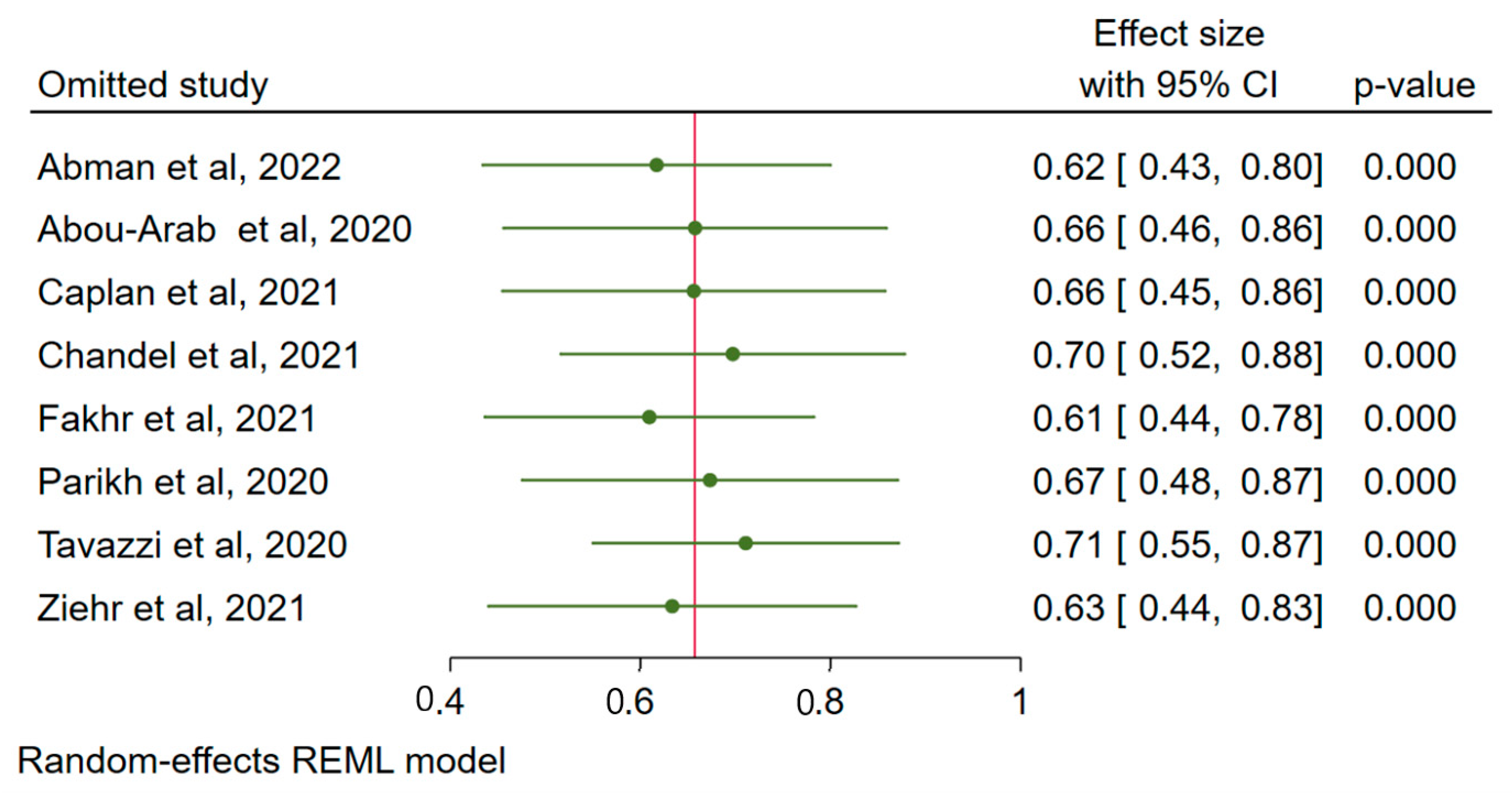
3.4. Publication Bias
3.5. Effect of Cofounders
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abman, S.H.; Fox, N.R.; Malik, M.I.; Kelkar, S.S.; Corman, S.L.; Rege, S.; Bhaloo, J.; Shah, R.; Shei, R.J.; Saporito, D.; et al. Real-world use of inhaled nitric oxide therapy in patients with COVID-19 and mild-to-moderate acute respiratory distress syndrome. Drugs Context 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Abou-Arab, O.; Huette, P.; Debouvries, F.; Dupont, H.; Jounieaux, V.; Mahjoub, Y. Inhaled nitric oxide for critically ill Covid-19 patients: A prospective study. Crit. Care 2020, 24, 645. [Google Scholar] [CrossRef]
- Bagate, F.; Tuffet, S.; Masi, P.; Perier, F.; Razazi, K.; de Prost, N.; Carteaux, G.; Payen, D.; Mekontso Dessap, A. Rescue therapy with inhaled nitric oxide and almitrine in COVID-19 patients with severe acute respiratory distress syndrome. Ann. Intensive Care 2020, 10, 151. [Google Scholar] [CrossRef] [PubMed]
- Bonizzoli, M.; Lazzeri, C.; Cianchi, G.; Guetti, C.; Fulceri, G.E.; Socci, F.; Peris, A. Effects of rescue inhaled nitric oxide on right ventricle and pulmonary circulation in severe COVID-related acute respiratory distress syndrome. J. Crit. Care 2022, 153987. [Google Scholar] [CrossRef] [PubMed]
- Caplan, M.; Goutay, J.; Bignon, A.; Jaillette, E.; Favory, R.; Mathieu, D.; Parmentier-Decrucq, E.; Poissy, J.; Duburcq, T.; on behalf of the Lille Intensive Care COVID-19 Group. Almitrine Infusion in Severe Acute Respiratory Syndrome Coronavirus 2-Induced Acute Respiratory Distress Syndrome: A Single-Center Observational Study. Crit. Care Med. 2021, 49, e191–e198. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; Patolia, S.; Ahmad, K.; Aryal, S.; Brown, A.W.; Sahjwani, D.; Khangoora, V.; Shlobin, O.A.; Cameron, P.C.; Singhal, A.; et al. Inhaled Nitric Oxide via High-Flow Nasal Cannula in Patients with Acute Respiratory Failure Related to COVID-19. Clin. Med. Insights Circ. Respir. Pulm. Med. 2021, 15. [Google Scholar] [CrossRef] [PubMed]
- DeGrado, J.R.; Szumita, P.M.; Schuler, B.R.; Dube, K.M.; Lenox, J.; Kim, E.Y.; Weinhouse, G.L.; Massaro, A.F. Evaluation of the Efficacy and Safety of Inhaled Epoprostenol and Inhaled Nitric Oxide for Refractory Hypoxemia in Patients With Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0259. [Google Scholar] [CrossRef]
- Safaee Fakhr, B.; Di Fenza, R.; Gianni, S.; Wiegand, S.B.; Miyazaki, Y.; Araujo Morais, C.C.; Gibson, L.E.; Chang, M.G.; Mueller, A.L.; Rodriguez-Lopez, J.M.; et al. Inhaled high dose nitric oxide is a safe and effective respiratory treatment in spontaneous breathing hospitalized patients with COVID-19 pneumonia. Nitric Oxide—Biol. Chem. 2021, 116, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Santini, A.; Protti, A.; Andreis, D.T.; Iapichino, G.; Castellani, G.; Rendiniello, V.; Costantini, E.; Cecconi, M. Inhaled nitric oxide in mechanically ventilated patients with COVID-19. J. Crit. Care 2020, 60, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Herranz, L.; da Silveira, J.G.; Trocado, L.F.L.; Alvaraes, A.L.; Fittipaldi, J. Inhaled Nitric Oxide in Patients with Severe COVID-19 Infection at Intensive Care Unit–A Cross Sectional Study. J. Crit. Care Med. 2021, 7, 318–319. [Google Scholar] [CrossRef] [PubMed]
- Laghlam, D.; Rahoual, G.; Malvy, J.; Estagnasie, P.; Brusset, A.; Squara, P. Use of Almitrine and Inhaled Nitric Oxide in ARDS Due to COVID-19. Front. Med. 2021, 8, 918. [Google Scholar] [CrossRef] [PubMed]
- Lubinsky, A.S.; Brosnahan, S.B.; Lehr, A.; Elnadoury, O.; Hagedorn, J.; Garimella, B.; Bender, M.T.; Amoroso, N.; Artigas, A.; Bos, L.D.J.; et al. Inhaled pulmonary vasodilators are not associated with improved gas exchange in mechanically ventilated patients with COVID-19: A retrospective cohort study. J. Crit. Care 2022, 69, 153990. [Google Scholar] [CrossRef] [PubMed]
- Matthews, L.; Baker, L.; Ferrari, M.; Sanchez, W.; Pappachan, J.; Grocott, M.P.; Dushianthan, A. Compassionate use of Pulmonary Vasodilators in Acute Severe Hypoxic Respiratory Failure due to COVID-19. J. Intensive Care Med. 2022, 37, 8850666221086521. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.; Wilson, C.; Weinberg, J.; Gavin, D.; Murphy, J.; Reardon, C.C. Inhaled nitric oxide treatment in spontaneously breathing COVID-19 patients. Ther. Adv. Respir. Dis. 2020, 14, 1753466620933510. [Google Scholar] [CrossRef]
- Robba, C.; Ball, L.; Battaglini, D.; Cardim, D.; Moncalvo, E.; Brunetti, I.; Bassetti, M.; Giacobbe, D.R.; Vena, A.; Patroniti, N.; et al. Early effects of ventilatory rescue therapies on systemic and cerebral oxygenation in mechanically ventilated COVID-19 patients with acute respiratory distress syndrome: A prospective observational study. Crit. Care 2021, 25, 111. [Google Scholar] [CrossRef] [PubMed]
- Tavazzi, G.; Pozzi, M.; Mongodi, S.; Dammassa, V.; Romito, G.; Mojoli, F. Correction to: Inhaled nitric oxide in patients admitted to intensive care unit with COVID-19 pneumonia. Crit Care 2020, 24, 665. [Google Scholar] [CrossRef]
- Ziehr, D.R.; Alladina, J.; Wolf, M.E.; Brait, K.L.; Malhotra, A.; La Vita, C.; Berra, L.; Hibbert, K.A.; Hardin, C.C. Respiratory Physiology of Prone Positioning With and Without Inhaled Nitric Oxide Across the Coronavirus Disease 2019 Acute Respiratory Distress Syndrome Severity Spectrum. Crit. Care Explor. 2021, 3, e0471. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet. Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef]
- Alqahtani, J.S. Prevalence, incidence, morbidity and mortality rates of COPD in Saudi Arabia: Trends in burden of COPD from 1990 to 2019. PLoS ONE 2022, 17, e0268772. [Google Scholar] [CrossRef]
- Phillips, D.B.; Brotto, A.R.; Ross, B.A.; Bryan, T.L.; Wong, E.Y.L.; Meah, V.L.; Fuhr, D.P.; van Diepen, S.; Stickland, M.K. Inhaled nitric oxide improves ventilatory efficiency and exercise capacity in patients with mild COPD: A randomized-control cross-over trial. J. Physiol. 2021, 599, 1665–1683. [Google Scholar] [CrossRef] [PubMed]
- Germann, P.; Braschi, A.; Della Rocca, G.; Dinh-Xuan, A.T.; Falke, K.; Frostell, C.; Gustafsson, L.E.; Hervé, P.; Jolliet, P.; Kaisers, U.; et al. Inhaled nitric oxide therapy in adults: European expert recommendations. Intensive Care Med. 2005, 31, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Lee, H.Y.; Lee, J.; Lee, S.-M. Effect of prone positioning on oxygenation and static respiratory system compliance in COVID-19 ARDS vs. non-COVID ARDS. Respir. Res. 2021, 22, 220. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Aldabayan, Y.S.; AlAhmari, M.D.; AlRabeeah, S.M.; Aldhahir, A.M.; Alghamdi, S.M.; Oyelade, T.; Althobiani, M.; Alrajeh, A.M. Clinical Practice and Barriers of Ventilatory Support Management in COVID-19 Patients in Saudi Arabia: A Survey of Respiratory Therapists. Saudi J. Med. Med. Sci. 2021, 9, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Marini, J.J.; Gattinoni, L. Management of COVID-19 Respiratory Distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Fink, J.B.; Augustynovich, A.E.; Mirza, S.; Kallet, R.H.; Dhand, R. Effects of Inhaled Epoprostenol and Prone Positioning in Intubated Coronavirus Disease 2019 Patients With Refractory Hypoxemia. Crit. Care Explor. 2020, 2, e0307. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Years | Aim | Country | Study Type | Experimental Design | Settings | Sample Size (Men) | Age Mean ± SD or Median, Range | iNO Used in (No of Patients) | iNO Amount (Range) | iNO Duration | Delivery Mode | Concomitant Respiratory Stimulants | Responder | Non-Responder | Response Definition | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abman et al., 2022 [1] | To assess real-world iNO use and outcomes in patients with COVID-19 with mild-to-moderate ARDS | USA | Research article | Retrospective observational | General ward | 37 (23) | 62.0 ± 10.2 | All | 9–40 ppm | 24 h (continuous) | Inhaled | NR | 34 | 3 | P/F increased from 136.7 (34.4) at baseline to 140.3 (53.2) at 48 h after iNO initiation | iNO was associated with improvement in the P/F ratio with no reported toxicity in hospitalized patients with COVID-19 and mild-to-moderate ARDS |
| Abou-Arab et al., 2020 [2] | To assess the effect of iNO administration on oxygenation in COVID-19-ARDS patients | France | Letter | Prospective observational | ICU | 34 (NR) | NR | All | 10 ppm | 15–30 min (continuous) | Invasive mechanical ventilation | NR | 22 | 12 | PaO2/FiO2 over 20% during over 30 min following its administration of iNO | A 65% response rate to iNO was found in COVID-19 patients with severe pneumonia |
| Bagate et al., 2020 [3] | To assess whether inhaled iNO–almitrine combination can improve oxygenation in COVID-19-ARDS patients | France | Research article | Pilot | ICU | 10 (7) | 60 (52–72) | All | 10 ppm | 30 min (continuous) | Invasive mechanical ventilation | Almitrine and ACE inhibitors or ARB (angiotensin receptors blockers) | NR | NR | PaO2/FiO2 ratio increased from 102 (89–134) mmHg at baseline to 124 (108–146) mmHg after iNO (p = 0.13) and 180 (132–206) mmHg after iNO and almitrine | iNO–almitrine combination was associated with rapid and significant improvement of oxygenation in patients with severe COVID-19 ARDS |
| Bonizzoli et al., 2022 [4] | To assess the effect of iNO administration on cardiac function and oxygenation in COVID-19-ARDS patients | Italy | Case series | Case series | ICU | 12 (8) | 61.7 ± 17 | All | 40 ppm | 24 h (continuous) | Invasive mechanical ventilation | NR | 0 | 12 | An improvement in oxygenation, as indicated by an increase in P/F ratio | iNO administration did not ameliorate oxygenation nor pulmonary hypertension in patients with severe COVID-19 ARDS |
| Caplan et al., 2021 [5] | To assess the effect of almitrine on arterial oxygenation in COVID-19-ARDS patients | France | Research article | Retrospective observational | ICU | 32 (25) | 63 (52–69) | All | 10 ppm | NR | Inhaled | Almitrine | 21 | 11 | An improvement in oxygenation, as indicated by an increase in P/F ratio | Almitrine infusion improved oxygenation in severe COVID-19 ARDS patients syndrome without adverse effects |
| Chandel et al., 2021 [6] | To assess the effect of continuous iNO via high-flow nasal cannula (HFNC) in COVID-19-ARDS patients | USA | Research article | Retrospective observational | ICU | 66 (45) | 57 ± 13 | All | 20–40 ppm | 88 h | High-flow nasal cannula | NR | 26 | 29 | Reduced need for mechanical ventilation or extension in hospital stay | iNO delivered via HFNC did not reduce oxygen requirements in most patients with COVID-19-ARDS or improve clinical outcomes |
| DeGrado et al., 2020 [7] | To evaluate safety and efficacy of inhaled epoprostenol and nitric oxide in patients with COVID-19-related refractory hypoxemia | USA | Research article | Retrospective observational | ICU | 38 (24) | 61 ± 12 | 11 (29) | 29.1 ± 18.7 ppm | 50.2 ± 31.3 h | Invasive mechanical ventilation | Inhaled epoprostenol | NR | NR | Significant change in oxygenation metrics such as P/F, PaO2, or SpO2 | Inhaled epoprostenol and iNO in patients with refractory hypoxemia secondary to coronavirus disease 2019 not associated with significant change in oxygenation metrics |
| Fakhr et al., 2021 [8] | To assess the feasibility and effect of high-dose iNO in spontaneously breathing, non-intubated COVID-19 patients | USA | Research article | Randomized interventional | General ward | 29 (16) | 50 (41–60) | All | 160 ppm | 30 min (twice daily) | Face mask | NR | 28 | 1 | An improvement in respiratory rate of tachypneic patient’s oxygenation, as indicated by an increase in P/F ratio. Reduced need for intubation and mechanical ventilation | Administration of iNO improved the respiratory rate of tachypneic patients and systemic oxygenation of hypoxemic patients |
| Ferrari et al., 2020 [9] | To assess the response to iNO in mechanically ventilated COVID-19 patients | Italy | Research article | Interventional | ICU | 10 (NR) | 55 ± 9 | All | 20 ppm | 30 min | Invasive mechanical ventilation | NR | NR | NR | Significant change in oxygenation metrics such as P/F, PaO2, or SpO2 | iNO administration did not improve oxygenation in patients with severe hypoxemia due to COVID-19 |
| Herranz et al., 2021 [10] | To assess the role of iNO in mechanically ventilated COVID-19-ARDS patients | Brazil | Letter | Retrospective cross-sectional | ICU | 34 (24) | Median (60yrs) | 12 (35) | 20–20 ppm | For up to 5 days | Invasive mechanical ventilation | NR | NR | NR | Significant change in oxygenation metrics such as P/F, PaO2, or SpO2 | iNO improved oxygenation (measured by PaO2/FiO2 ratio) in critically ill COVID-19 patients who are mechanically ventilated |
| Laghlam et al., 2021 [11] | To assess the effect of iNO and almitrine on oxygenation in COVID-19-ARDS patients | France | Brief research report | Prospective observational | ICU | 12 (9) | 71.8 ± 8.7 | All | 10 ppm | 30 min | Invasive mechanical ventilation | Almitrine | NR | NR | Significant change in oxygenation metrics such as P/F, PaO2, or SpO2 | Concomitant administration of iNO and infused almitrine shortly increased oxygenation in patients with COVID-19-related ARDS |
| Lubinsky et al., 2022 [12] | To assess the effect of iNO and inhaled epoprostenol (iEPO) on gas exchange in mechanically ventilated COVID-19-ARDS patients. | USA | Research article | Retrospective observational | ICU | 84 (63) | NR | 69 (49) | 10–40 ppm | 106 h (median) | Invasive mechanical ventilation | Inhaled epoprostenol | NS | NS | Significant change in oxygenation metrics such as P/F, oxygenation index (OI) (FiO2xmean airway pressure/PaO2), or CO2 elimination (ventilatory ratio (VR)) | Inhaled pulmonary vasodilators not associated with significant improvement in oxygenation in mechanically ventilated COVID-19 patients |
| Matthews et al., 2022 [13] | To assess the response to iNO or prostaglandin in COVID-19-ARDS patients | UK | Research article | Prospective observational | ICU | 59 (37) | 60 (54–66) | 48 (NR) | 20–40 ppm | NR | Invasive mechanical ventilation | Iloprost | NR | NR | Significant change or improvement in oxygenation metrics such as P/F ratio | iNO and Iloprost (prostaglandin) may offer therapeutic value for ARDS-COVID-19 patients and should be investigated further |
| Parikh et al., 2020 [14] | To assess whether iNO therapy has any benefit for treatment of spontaneously breathing COVID-19 patients | USA | Letter | Prospective observational | General ward | 39 (22) | 61(NR) | All | 30 ppm | 2.1 days | Nasal cannula, nasal pendant with oxymizer, and nonrebreather mask | NR | 21 | 18 | Improvement in oxygenation measured by SpO2/FiO2 (SF) ratio, a surrogate for P/F ratio | iNO therapy may have a role in preventing progression of hypoxic respiratory failure in COVID-19 patients |
| Robba et al., 2021 [15] | To assess the effects of recruitment maneuvers (RM), prone positioning (PP), inhaled nitric oxide (iNO), and carbon dioxide removal by ECCO2R on systemic and cerebral oxygenation in mechanically ventilated COVID-19-ARDS patients | Italy | Research article | Prospective observational | ICU | 22 (18) | 62 [57–68.5] | 9(NR) | 20 ppm | Invasive mechanical ventilation | NR | NR | NR | Improvement in cerebral or systemic oxygenation PEEP, Pplat, Crs, VT, FiO2, saturation of oxygen (SpO2), pHa, PaO2, partial pressure of carbon dioxide (PaCO2), systemic (MAP, HR), and neuromonitoring parameters (TCD and NIRSderived indices) | Rescue therapy results in different effect on systemic and cerebral oxygenation in ARDS-COVID-19 patients and should be considered in choosing the right therapy | |
| Tavazzi et al., 2020 [16] | To assess the effect of iNO administration in COVID-19 mechanically ventilated patients with refractory hypoxemia and/or right ventricular dysfunction | Italy | Letter | NR | ICU | 72 (67) | 66.0 [59.6–69.7] | 16(NR) | 20–30 ppm | 15–30 min | Invasive mechanical ventilation | NR | 4 | 12 | Increase oxygenation measured by P/F ratio post administration of iNO | iNO did not improve oxygenation in COVID-19 patients with refractory hypoxemia |
| Ziehr et al., 2021 [17] | To understand the effect of prone position with and without iNO administration on respiratory functions in patients with COVID-19-ARDS | USA | Research article | Retrospective cohort | ICU | 122 (72) | 60 (51–71) | 12 | NR | 16hr (2–36 hr) | Invasive mechanical ventilation | NR | 10 | 2 | Significant increase (>=20%) in P/F ratio | Prone positioning confers an additive benefit in oxygenation among patients treated with inhaled nitric oxide |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, J.S.; Aldhahir, A.M.; Al Ghamdi, S.S.; AlBahrani, S.; AlDraiwiesh, I.A.; Alqarni, A.A.; Latief, K.; Raya, R.P.; Oyelade, T. Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12803. https://doi.org/10.3390/ijerph191912803
Alqahtani JS, Aldhahir AM, Al Ghamdi SS, AlBahrani S, AlDraiwiesh IA, Alqarni AA, Latief K, Raya RP, Oyelade T. Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(19):12803. https://doi.org/10.3390/ijerph191912803
Chicago/Turabian StyleAlqahtani, Jaber S., Abdulelah M. Aldhahir, Shouq S. Al Ghamdi, Salma AlBahrani, Ibrahim A. AlDraiwiesh, Abdullah A. Alqarni, Kamaluddin Latief, Reynie Purnama Raya, and Tope Oyelade. 2022. "Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 19: 12803. https://doi.org/10.3390/ijerph191912803
APA StyleAlqahtani, J. S., Aldhahir, A. M., Al Ghamdi, S. S., AlBahrani, S., AlDraiwiesh, I. A., Alqarni, A. A., Latief, K., Raya, R. P., & Oyelade, T. (2022). Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(19), 12803. https://doi.org/10.3390/ijerph191912803