
Comparison of Concordance of Peptic Ulcer Disease, Non-Adenomatous Intestinal Polyp, and Gallstone Disease in Korean Monozygotic and Dizygotic Twins: A Cross-Sectional Study

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Participants Selection
2.3. Survey
2.4. Exposure
2.5. Outcome
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, J.J.; Kuipers, E.J.; El-Serag, H.B. Systematic review: The global incidence and prevalence of peptic ulcer disease. Aliment. Pharmacol. Ther. 2009, 29, 938–946. [Google Scholar] [CrossRef]
- Markowitz, A.J.; Winawer, S.J. Management of colorectal polyps. CA Cancer J. Clin. 1997, 47, 93–112. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Yang, H.; Li, H.; He, C.; Yang, L.; Lv, G. Insights into modifiable risk factors of cholelithiasis: A Mendelian randomization study. Hepatology 2022, 75, 785–796. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Kang, H.S.; Lim, H.; Kim, J.H.; Kim, J.H.; Cho, S.J.; Nam, E.S.; Min, K.W.; Park, H.Y.; Kim, N.Y.; et al. Changes in the Incidence Rates of Gastrointestinal Diseases Due to the COVID-19 Pandemic in South Korea: A Long-Term Perspective. J. Pers. Med. 2022, 12, 1144. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address, e.e.e. EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J. Hepatol 2016, 65, 146–181. [Google Scholar] [CrossRef] [Green Version]
- Havens, J.M.; Castillo-Angeles, M.; Nitzschke, S.L.; Salim, A. Disparities in peptic ulcer disease: A nationwide study. Am. J. Surg. 2018, 216, 1127–1128. [Google Scholar] [CrossRef]
- Freeman, J.; Boomer, L.; Fursevich, D.; Feliz, A. Ethnicity and insurance status affect health disparities in patients with gallstone disease. J. Surg. Res. 2012, 175, 1–5. [Google Scholar] [CrossRef]
- Wallace, K.; Brandt, H.M.; Bearden, J.D.; Blankenship, B.F.; Caldwell, R.; Dunn, J.; Hegedus, P.; Hoffman, B.J.; Marsh, C.H.; Marsh, W.H.; et al. Race and Prevalence of Large Bowel Polyps Among the Low-Income and Uninsured in South Carolina. Dig. Dis. Sci. 2016, 61, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Katsika, D.; Grjibovski, A.; Einarsson, C.; Lammert, F.; Lichtenstein, P.; Marschall, H.U. Genetic and environmental influences on symptomatic gallstone disease: A Swedish study of 43,141 twin pairs. Hepatology 2005, 41, 1138–1143. [Google Scholar] [CrossRef]
- Raiha, I.; Kemppainen, H.; Kaprio, J.; Koskenvuo, M.; Sourander, L. Lifestyle, stress, and genes in peptic ulcer disease: A nationwide twin cohort study. Arch. Intern. Med. 1998, 158, 698–704. [Google Scholar] [CrossRef]
- Pilot, M.L.; Lenkoski, L.D.; Spiro, H.M.; Schafer, R. Duodenal ulcer in one of identical twins. Psychosom. Med. 1957, 19, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Riecker, H.H. Peptic ulcer in identical twins. Ann. Intern. Med. 1946, 24, 878–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotter, J.I.; Sones, J.Q.; Samloff, I.M.; Richardson, C.T.; Gursky, J.M.; Walsh, J.H.; Rimoin, D.L. Duodenal-ulcer disease associated with elevated serum pepsinogen I: An inherited autosomal dominant disorder. N. Engl. J. Med. 1979, 300, 63–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsika, D.; Tuvblad, C.; Einarsson, C.; Lichtenstein, P.; Marschall, H.U. Body mass index, alcohol, tobacco and symptomatic gallstone disease: A Swedish twin study. J. Intern. Med. 2007, 262, 581–587. [Google Scholar] [CrossRef]
- Park, Y.; Ki, M. Population Attributable Fraction of Helicobacter pylori Infection-Related Gastric Cancer in Korea: A Meta-Analysis. Cancer Res. Treat. 2021, 53, 744–753. [Google Scholar] [CrossRef]
- Cho, Y.A.; Ko, S.Y.; Suh, Y.J.; Kim, S.; Park, J.H.; Park, H.R.; Seo, J.; Choi, H.G.; Kang, H.S.; Lim, H.; et al. PIK3CA Mutation as Potential Poor Prognostic Marker in Asian Female Breast Cancer Patients Who Received Adjuvant Chemotherapy. Curr. Oncol. 2022, 29, 2895–2908. [Google Scholar] [CrossRef]
- Petersen, G.M.; Rotter, J.I. Genetic and evolutionary implications in peptic ulcer disease. Am. J. Phys. Anthropol. 1983, 62, 71–79. [Google Scholar] [CrossRef]
- Yim, J.Y.; Kim, N.; Choi, S.H.; Kim, Y.S.; Cho, K.R.; Kim, S.S.; Seo, G.S.; Kim, H.U.; Baik, G.H.; Sin, C.S.; et al. Seroprevalence of Helicobacter pylori in South Korea. Helicobacter 2007, 12, 333–340. [Google Scholar] [CrossRef]
- Choi, H.G.; Lee, H.K.; Kang, H.S.; Lim, H.; Kim, J.H.; Kim, J.H.; Kim, N.Y.; Cho, S.J.; Nam, E.S.; Min, K.W.; et al. Possible Association between the Use of Proton Pump Inhibitors and H2 Receptor Antagonists, and Esophageal Cancer: A Nested Case-Control Study Using a Korean National Health Screening Cohort. Pharmaceuticals 2022, 15, 517. [Google Scholar] [CrossRef]
- Lim, S.H.; Kwon, J.W.; Kim, N.; Kim, G.H.; Kang, J.M.; Park, M.J.; Yim, J.Y.; Kim, H.U.; Baik, G.H.; Seo, G.S.; et al. Prevalence and risk factors of Helicobacter pylori infection in Korea: Nationwide multicenter study over 13 years. BMC Gastroenterol 2013, 13, 104. [Google Scholar] [CrossRef]
- Jung, K.W.; Won, Y.J.; Hong, S.; Kong, H.J.; Im, J.S.; Seo, H.G. Prediction of Cancer Incidence and Mortality in Korea, 2021. Cancer Res. Treat. 2021, 53, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.J.; Kang, H.S.; Kim, J.H.; Kim, J.H.; Kim, S.H.; Kim, N.Y.; Nam, E.S.; Min, K.W.; Choi, H.G. Association between Statin Use and Gastric Cancer: A Nested Case-Control Study Using a National Health Screening Cohort in Korea. Pharmaceuticals 2021, 14, 1283. [Google Scholar] [CrossRef] [PubMed]
- Glambek, I.; Kvaale, G.; Arnesjo, B.; Soreide, O. Prevalence of gallstones in a Norwegian population. Scand. J. Gastroenterol. 1987, 22, 1089–1094. [Google Scholar] [CrossRef]
- Aerts, R.; Penninckx, F. The burden of gallstone disease in Europe. Aliment. Pharmacol. Ther. 2003, 18 (Suppl. 3), 49–53. [Google Scholar] [CrossRef]
- Jung, H.W.; Chun, K.S.; Kim, Y.S.; Kim, M.H.; Choi, H. Prevalence of gallstones in Korean. J. Korean Acad. Fam. Med. 1992, 13, 581–591. [Google Scholar]
- Lv, F.; Wang, G.; Ding, D.; Shen, C.; Liu, J.; Ji, F.; Kang, Y. Epidemiological survey to determine the prevalence of cholecystolithiasis in Uyghur, Kazakh, and Han Ethnic Groups in the Xinjiang Uyghur Autonomous Region of China: Cross-sectional studies. BMC Gastroenterol 2021, 21, 125. [Google Scholar] [CrossRef] [PubMed]
- Cortes, V.A.; Barrera, F.; Nervi, F. Pathophysiological connections between gallstone disease, insulin resistance, and obesity. Obes. Rev. 2020, 21, e12983. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Burgess, S. Appraising the causal role of smoking in multiple diseases: A systematic review and meta-analysis of Mendelian randomization studies. EBioMedicine 2022, 82, 104154. [Google Scholar] [CrossRef] [PubMed]
- Cannon-Albright, L.A.; Bishop, D.T.; Samowitz, W.; DiSario, J.A.; Lee, R.; Burt, R.W. Colonic polyps in an unselected population: Prevalence, characteristics, and associations. Am. J. Gastroenterol. 1994, 89, 827–831. [Google Scholar]
- Waye, J.D.; Lewis, B.S.; Frankel, A.; Geller, S.A. Small colon polyps. Am. J. Gastroenterol. 1988, 83, 120–122. [Google Scholar]
- Balazs, M. Giant inflammatory polyps associated with idiopathic inflammatory bowel disease. An ultrastructural study of five cases. Dis. Colon. Rectum. 1990, 33, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Oluyemi, A.O.; Odeghe, E.A.; Awolola, N.A. Solitary peutz-jeghers type hamartoma in a Nigerian: A case report of a rare finding and review of literature. Ann. Afr. Med. 2021, 20, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Katsika, D.; Magnusson, P.; Krawczyk, M.; Grunhage, F.; Lichtenstein, P.; Einarsson, C.; Lammert, F.; Marschall, H.U. Gallstone disease in Swedish twins: Risk is associated with ABCG8 D19H genotype. J. Intern. Med. 2010, 268, 279–285. [Google Scholar] [CrossRef]
- Sung, J.; Cho, S.I.; Lee, K.; Ha, M.; Choi, E.Y.; Choi, J.S.; Kim, H.; Kim, J.; Hong, K.S.; Kim, Y.; et al. Healthy Twin: A twin-family study of Korea—protocols and current status. Twin Res. Hum. Genet. 2006, 9, 844–848. [Google Scholar] [CrossRef]
- Sung, J.; Lee, K.; Song, Y.M.; Lee, M.K.; Lee, D.H. Heritability of eating behavior assessed using the DEBQ (Dutch Eating Behavior Questionnaire) and weight-related traits: The Healthy Twin Study. Obesity 2010, 18, 1000–1005. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G.; Ko, G.E.S.g. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Yoo, D.M.; Kwon, M.J.; Kim, J.H.; Kim, J.H.; Bang, W.J.; Choi, H.G. Comparison of the Differences in State-Trait Anxiety Inventory Scores and Insomnia Histories between Monozygotic and Dizygotic Twins: A Cross-Sectional Study Using KoGES HTS Data. J. Clin. Med. 2022, 11, 4011. [Google Scholar] [CrossRef]
- Song, Y.M.; Lee, D.; Lee, M.K.; Lee, K.; Lee, H.J.; Hong, E.J.; Han, B.; Sung, J. Validity of the zygosity questionnaire and characteristics of zygosity-misdiagnosed twin pairs in the Healthy Twin Study of Korea. Twin Res. Hum. Genet. 2010, 13, 223–230. [Google Scholar] [CrossRef]
- Sung, J.; Lee, K.; Song, Y.M. Heritabilities of Alcohol Use Disorders Identification Test (AUDIT) scores and alcohol biomarkers in Koreans: The KoGES (Korean Genome Epi Study) and Healthy Twin Study. Drug Alcohol Depend. 2011, 113, 104–109. [Google Scholar] [CrossRef]
- Czyz, W.; Morahan, J.M.; Ebers, G.C.; Ramagopalan, S.V. Genetic, environmental and stochastic factors in monozygotic twin discordance with a focus on epigenetic differences. BMC Med. 2012, 10, 93. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, N.; Ishikawa, H.; Eguchi, H.; Okazaki, Y.; Hirose, R.; Inoue, K.; Dohi, O.; Itoh, Y.; Mutoh, M.; Ishiguro, S.; et al. Promotion Effects of Smoking in Polyp Development in Monozygotic Twins with Atypical Colorectal Polyposis. Case Rep. Gastroenterol. 2022, 16, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Kaminsky, Z.A.; Tang, T.; Wang, S.C.; Ptak, C.; Oh, G.H.; Wong, A.H.; Feldcamp, L.A.; Virtanen, C.; Halfvarson, J.; Tysk, C.; et al. DNA methylation profiles in monozygotic and dizygotic twins. Nat. Genet. 2009, 41, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Vilchez-Vargas, R.; Skieceviciene, J.; Lehr, K.; Varkalaite, G.; Thon, C.; Urba, M.; Morkunas, E.; Kucinskas, L.; Bauraite, K.; Schanze, D.; et al. Gut microbial similarity in twins is driven by shared environment and aging. EBioMedicine 2022, 79, 104011. [Google Scholar] [CrossRef]
- Urba, M.; Skieceviciene, J.; Janciauskas, D.; Jonaitis, L.; Kupcinskas, L.; Fassan, M.; Rugge, M.; Kupcinskas, J. Gastritis Stages in Monozygotic and Dizygotic Dyspeptic Twins. Gastroenterol. Res. Pract. 2020, 2020, 9510717. [Google Scholar] [CrossRef] [PubMed]
- Rotter, J.I. The genetics of peptic ulcer: More than one gene, more than one disease. Prog. Med. Genet 1980, 4, 1–58. [Google Scholar] [PubMed]
- Antero Kesaniemi, Y.; Koskenvuo, M.; Vuoristo, M.; Miettinen, T.A. Biliary lipid composition in monozygotic and dizygotic pairs of twins. Gut 1989, 30, 1750–1756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvald, B.; Hauge, M. A catamnestic investigation of Danish twins; a preliminary report. Dan. Med. Bull. 1956, 3, 150–158. [Google Scholar]
- Kuo, K.K.; Shin, S.J.; Chen, Z.C.; Yang, Y.H.; Yang, J.F.; Hsiao, P.J. Significant association of ABCG5 604Q and ABCG8 D19H polymorphisms with gallstone disease. Br. J. Surg. 2008, 95, 1005–1011. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Participants | |||
|---|---|---|---|---|
| Monozygotic Twin | Dizygotic Twin | p-Value | ||
| Age (years old, n, %) | 0.004 * | |||
| 20–24 | 6 (0.6) | 0 (0) | ||
| 25–29 | 68 (6.5) | 4 (1.6) | ||
| 30–34 | 362 (34.5) | 87 (35.7) | ||
| 35–39 | 244 (23.2) | 65 (26.6) | ||
| 40–44 | 139 (13.2) | 36 (14.8) | ||
| 45–49 | 129 (12.3) | 20 (8.2) | ||
| 50–54 | 82 (7.8) | 22 (9) | ||
| 55–59 | 14 (1.3) | 10 (4.1) | ||
| 60–64 | 4 (0.4) | 0 (0) | ||
| 65+ | 2 (0.2) | 0 (0) | ||
| Sex (n, %) | 0.016 * | |||
| Males | 384 (36.6) | 134 (54.9) | ||
| Females | 666 (63.4) | 244 (100) | ||
| Income (n, %) | 0.978 | |||
| <2 million (KRW) | 349 (33.2) | 81 (33.2) | ||
| 2 to <3 million (KRW) | 282 (26.9) | 68 (27.9) | ||
| 3 to <4 million (KRW) | 214 (20.4) | 50 (20.5) | ||
| ≥4 million (KRW) | 205 (19.5) | 45 (18.4) | ||
| Education (n, %) | 0.743 | |||
| Under high school | 122 (11.6) | 25 (10.2) | ||
| Graduated from high school | 371 (35.3) | 92 (37.7) | ||
| Commercial college/dropped out of college | 123 (11.7) | 32 (13.1) | ||
| Graduated from high school | 434 (41.3) | 95 (38.9) | ||
| Marriage (n, %) | 0.302 | |||
| Unmarried | 240 (23.1) | 50 (20.5) | ||
| Married | 733 (70.5) | 173 (70.9) | ||
| Divorced or others | 67 (6.4) | 21 (8.6) | ||
| Physical Activity | ||||
| Hard (hour/week, mean, SD) | 3.1 (6.8) | 4.7 (9.7) | 0.013 * | |
| Moderate (hour/week, mean, SD) | 5.8 (10.5) | 6.2 (10.2) | 0.612 | |
| Walk (hour/week, mean, SD) | 6.1 (9.6) | 6.8 (10.9) | 0.291 | |
| Sit (hour/week, mean, SD) | 40.1 (22) | 37.9 (20.7) | 0.155 | |
| Obesity (n, %) | 0.203 | |||
| Underweight (BMI < 18.5) | 27 (2.6) | 5 (2) | ||
| Normal (BMI ≥ 18.5 to < 23) | 510 (48.6) | 113 (46.3) | ||
| Overweight (BMI 23 to < 25) | 220 (21) | 68 (27.9) | ||
| Obese I (BMI ≥ 25 to < 30) | 261 (24.9) | 52 (21.3) | ||
| Obese II (BMI ≥ 30) | 32 (3) | 6 (2.5) | ||
| Smoking status (n, %) | 0.138 | |||
| Nonsmoker | 691 (65.8) | 145 (59.4) | ||
| Past smoker | 108 (10.3) | 33 (13.5) | ||
| Current smoker | 251 (23.9) | 66 (27) | ||
| Frequency of drinking alcohol (n, %) | 0.314 | |||
| Nondrinker | 304 (29) | 64 (26.2) | ||
| ≤1 time per month | 238 (22.7) | 46 (18.9) | ||
| 2–4 times per month | 300 (28.6) | 80 (32.8) | ||
| ≥2 times per week | 208 (19.8) | 54 (22.1) | ||
| Sleeping hours (n, %) | 0.370 | |||
| ≤5 h | 53 (5) | 16 (6.6) | ||
| 6–7 h | 619 (59) | 146 (59.8) | ||
| 8–9 h | 350 (33.3) | 72 (29.5) | ||
| ≥10 h | 28 (2.7) | 10 (4.1) | ||
| Gastrointestinal diseases (categorical) | ||||
| Gastric/duodenal ulcer (n, %) | 111 (10.6) | 32 (13.1) | 0.254 | |
| Intestinal polyp (n, %) | 23 (2.2) | 3 (1.2) | 0.451 | |
| Cholelithiasis/cholangitis (n, %) | 35 (3.3) | 5 (2) | 0.319 | |
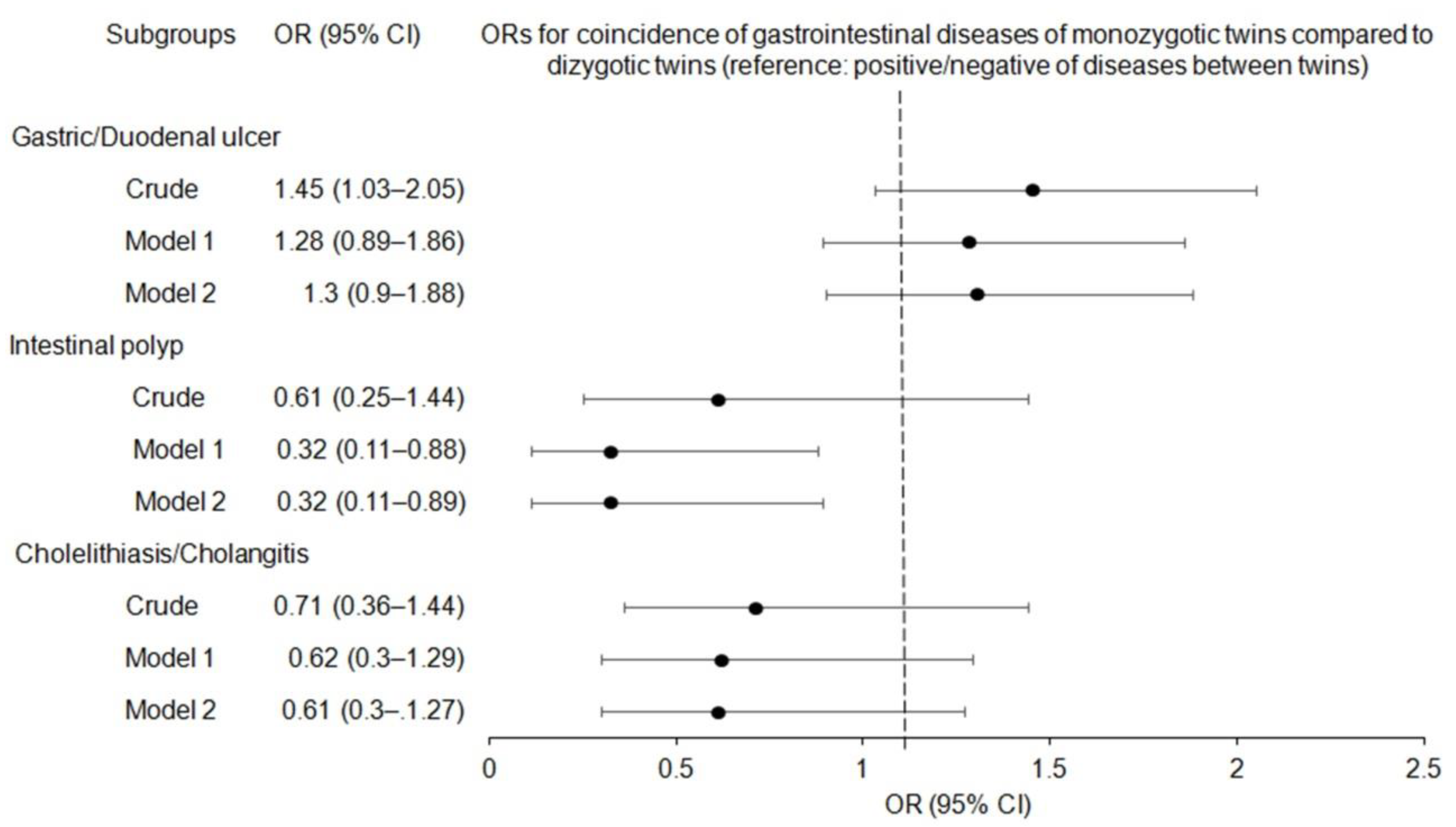
| Concordance of Diseases | Monozygotic Twin | Dizygotic Twin | Odds Ratios (95% Confidence Interval) | |||||
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | Crude | p | Model 1 † | p | Model 2 ‡ | p | |
| Gastric/duodenal ulcer | ||||||||
| concordant | 878/1050 (83.6) | 190/244 (77.9) | 1.45 (1.03–2.05) | 0.034 * | 1.28 (0.89–1.86) | 0.187 | 1.30 (0.90–1.88) | 0.169 |
| discordant | 172/1050 (16.4) | 54/244 (22.1) | 1 | 1 | 1 | |||
| Intestinal polyp | ||||||||
| concordant | 1008/1050 (96.0) | 238/244 (97.5) | 0.61 (0.25–1.44) | 0.256 | 0.32 (0.11–0.88) | 0.028 * | 0.32 (0.11–0.89) | 0.028 * |
| discordant | 42/1050 (4.0) | 6/244 (2.5) | 1 | 1 | 1 | |||
| Cholelithiasis/cholangitis | ||||||||
| concordant | 990/1050 (94.3) | 234/244 (95.9) | 0.71 (0.36–1.44) | 0.317 | 0.62 (0.30–1.29) | 0.204 | 0.61 (0.30–1.27) | 0.190 |
| discordant | 60/1050 (5.7) | 10/244 (4.1) | 1 | 1 | 1 | |||
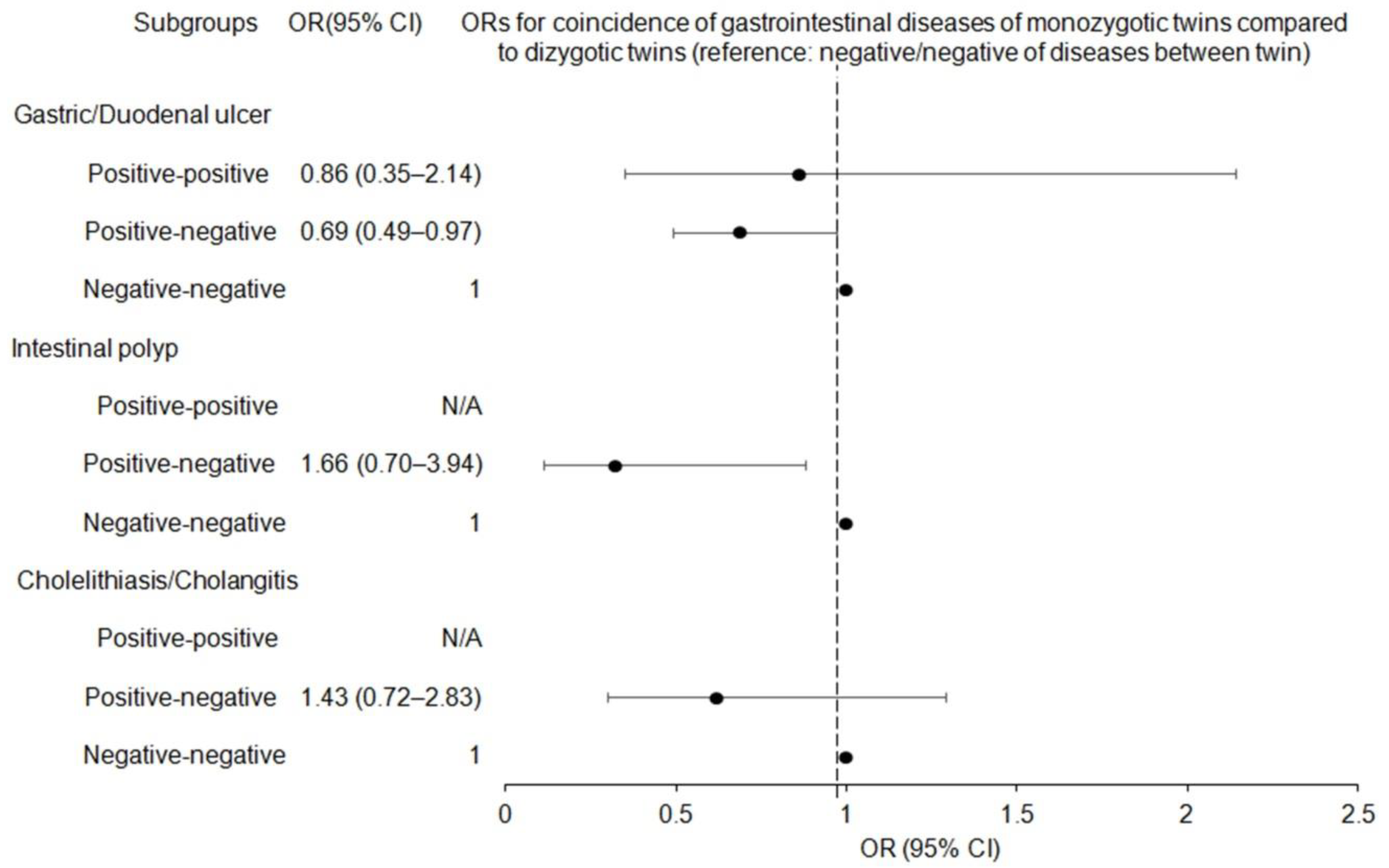
| Concordance of Diseases | Monozygotic Twin | Dizygotic Twin | Odds Ratios (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | Crude | p | Model 1 * | p | Model 2 † | p | |
| Gastric/duodenal ulcer | ||||||||
| Positive-positive | 24/1050 (2.3) | 6/244 (2.5) | 0.86 (0.35–2.14) | 0.748 | 1.01 (0.39–2.63) | 0.990 | 1.00 (0.38–2.61) | 0.994 |
| Positive-negative | 172/1050 (16.4) | 54/244 (22.1) | 0.69 (0.49–0.97) | 0.032 * | 0.73 (0.51–1.05) | 0.088 | 0.72 (0.51–1.04) | 0.077 |
| Negative-negative | 854/1050 (81.3) | 184/244 (75.4) | 1 | 1 | 1 | |||
| Intestinal polyp | ||||||||
| Positive-positive | 2/1050 (0.2) | 0/244 (0.0) | N/A | N/A | N/A | N/A | N/A | N/A |
| Positive-negative | 42/1050 (4.0) | 6/244 (2.5) | 1.66 (0.70–3.94) | 0.254 | 2.04 (0.82–5.07) | 0.125 | 2.05 (0.82–5.11) | 0.124 |
| Negative-negative | 1006/1050 (95.8) | 238/244 (97.5) | 1 | 1 | 1 | |||
| Cholelithiasis/cholangitis | ||||||||
| Positive-positive | 6/1050 (0.6) | 0/244 (0.0) | N/A | N/A | N/A | N/A | N/A | N/A |
| Positive-negative | 60/1050 (5.7) | 10/244 (4.1) | 1.43 (0.72–2.83) | 0.309 | 1.57 (0.78–3.16) | 0.209 | 1.58 (0.78–3.19) | 0.201 |
| Negative-negative | 984/1050 (93.7) | 234/244 (95.9) | 1 | 1 | 1 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.G.; Kim, S.Y.; Lim, H.; Kim, J.-H.; Kim, J.H.; Cho, S.-J.; Nam, E.S.; Min, K.-W.; Park, H.Y.; Kim, N.Y.; et al. Comparison of Concordance of Peptic Ulcer Disease, Non-Adenomatous Intestinal Polyp, and Gallstone Disease in Korean Monozygotic and Dizygotic Twins: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12708. https://doi.org/10.3390/ijerph191912708
Choi HG, Kim SY, Lim H, Kim J-H, Kim JH, Cho S-J, Nam ES, Min K-W, Park HY, Kim NY, et al. Comparison of Concordance of Peptic Ulcer Disease, Non-Adenomatous Intestinal Polyp, and Gallstone Disease in Korean Monozygotic and Dizygotic Twins: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12708. https://doi.org/10.3390/ijerph191912708
Chicago/Turabian StyleChoi, Hyo Geun, So Young Kim, Hyun Lim, Joo-Hee Kim, Ji Hee Kim, Seong-Jin Cho, Eun Sook Nam, Kyueng-Whan Min, Ha Young Park, Nan Young Kim, and et al. 2022. "Comparison of Concordance of Peptic Ulcer Disease, Non-Adenomatous Intestinal Polyp, and Gallstone Disease in Korean Monozygotic and Dizygotic Twins: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 12708. https://doi.org/10.3390/ijerph191912708
APA StyleChoi, H. G., Kim, S. Y., Lim, H., Kim, J.-H., Kim, J. H., Cho, S.-J., Nam, E. S., Min, K.-W., Park, H. Y., Kim, N. Y., Hong, S., Choi, Y., Kang, H. S., & Kwon, M. J. (2022). Comparison of Concordance of Peptic Ulcer Disease, Non-Adenomatous Intestinal Polyp, and Gallstone Disease in Korean Monozygotic and Dizygotic Twins: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(19), 12708. https://doi.org/10.3390/ijerph191912708