
Surveying and Modelling 21st Century Online Learning Patterns of Medical Students


Abstract
1. Introduction
1.1. Composition of the 21st Century Online Learning Survey (21 CLS) for Medical Students
1.2. Intercorrelations of the 21 CLS Components
2. Materials and Methods
2.1. Instrument
2.2. Data Analysis
3. Results
3.1. Participants
3.2. Confirmatory Factor Analyses for the 21 CLS
3.3. Agreement with 21 CLS for Medical Students, Subscale Intercorrelations and Internal Consistency
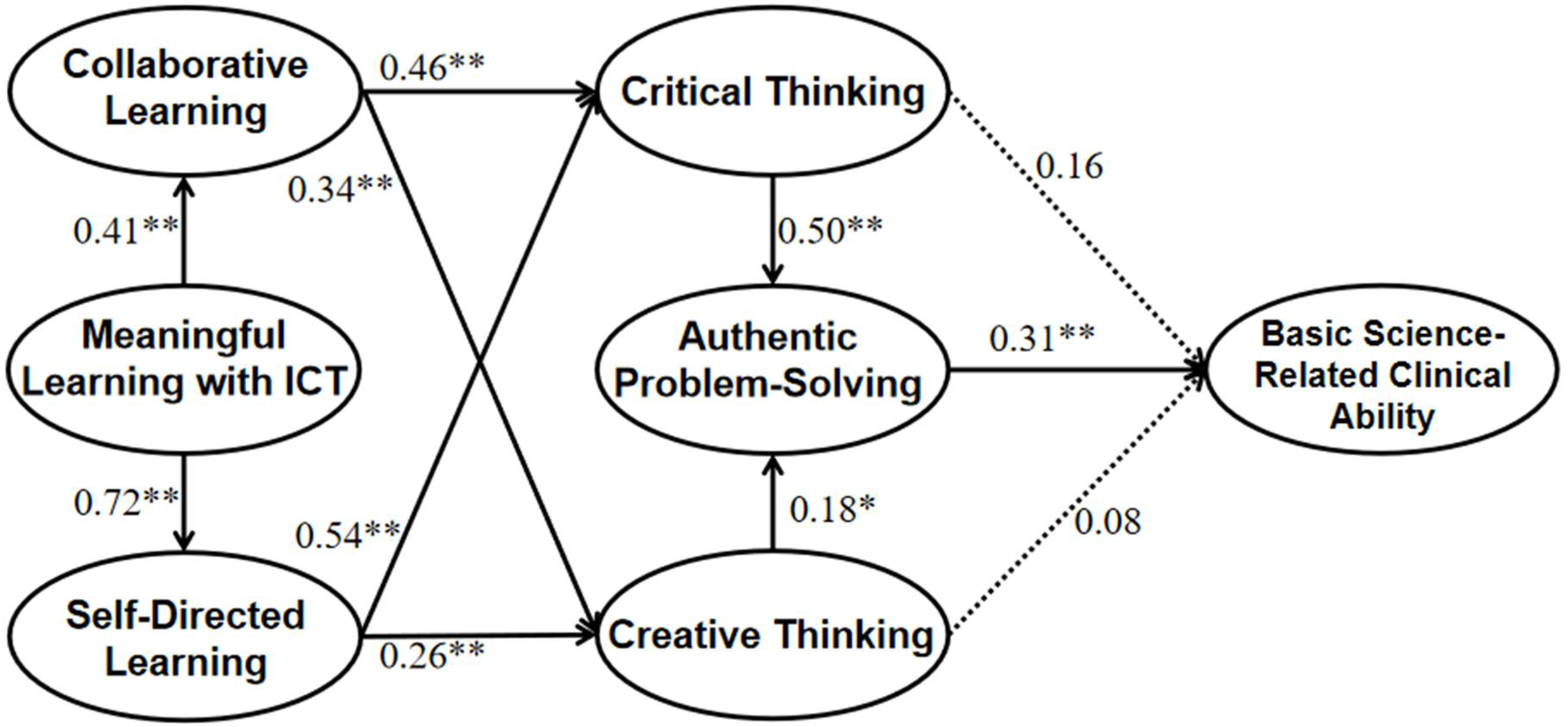
3.4. Structural Equation Model for Exploring the Patterns of Medical Students’ 21st Century Online Learning Practices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghebreyesus, T.A.; Fore, H.; Birtanov, Y.; Jakab, Z. Primary health care for the 21st century, universal health coverage, and the Sustainable Development Goals. Lancet 2018, 392, 1371–1372. [Google Scholar] [CrossRef]
- Masic, I.; Pandza, H.; Toromanovic, S.; Masic, F.; Sivic, S.; Zunic, L.; Masic, Z. Information Technologies (ITs) in Medical Education. Acta Inf. Med. 2011, 19, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Kamei, R.K.; Cook, S.; Puthucheary, J.; Starmer, C.F. 21st Century Learning in Medicine: Traditional Teaching versus Team-based Learning. Med. Sci. Educ. 2012, 22, 57–64. [Google Scholar] [CrossRef]
- Dabbagh, N.; Marra, R.M.; Howland, J.L. Meaningful Online Learning: Integrating Strategies, Activities, and Learning Technologies for Effective Designs; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Stoehr, F.; Müller, L.; Brady, A.; Trilla, A.; Mähringer-Kunz, A.; Hahn, F.; Düber, C.; Becker, N.; Wörns, M.A.; Chapiro, J.; et al. How COVID-19 kick-started online learning in medical education-The DigiMed study. PLoS ONE 2021, 16, e0257394. [Google Scholar] [CrossRef]
- Chai, C.S.; Kong, S.C. Professional learning for 21st century education. J. Comput. Educ. 2017, 4, 1–4. [Google Scholar] [CrossRef]
- Heisler, M. The future of medical education: Areas that should receive increased focus in the 21st Century. Rev. Med. 2016, 95, 30–31. [Google Scholar] [CrossRef]
- Gwee, M.C.; Samarasekera, D.; Chay-Hoon, T. Role of basic sciences in 21st century medical education: An Asian perspective. Med. Sci. Educ. 2010, 20, 299–306. [Google Scholar]
- Ganguly, P.; Yaqinuddin, A.; Al-Kattan, W.; Kemahli, S.; AlKattan, K. Medical education dilemma: How can we best accommodate basic sciences in a curriculum for 21st century medical students? Can. J. Physiol. Pharmacol. 2019, 97, 293–296. [Google Scholar] [CrossRef]
- Sang, G.; Liang, J.C.; Chai, C.S.; Dong, Y.; Tsai, C.C. Teachers’ actual and preferred perceptions of twenty-first century learning competencies: A Chinese perspective. Asia Pac. Educ. Rev. 2018, 19, 307–317. [Google Scholar] [CrossRef]
- Malau-Aduli, B.S.; Alele, F.O.; Heggarty, P.; Teague, P.A.; Sen Gupta, T.; Hays, R. Perceived clinical relevance and retention of basic sciences across the medical education continuum. Adv. Physiol. Educ. 2019, 43, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Woods, N.N.; Neville, A.J.; Levinson, A.J.; Howey, E.H.; Oczkowski, W.J.; Norman, G.R. The value of basic science in clinical diagnosis. Acad. Med. 2006, 81, S124–S127. [Google Scholar] [CrossRef]
- Gruppuso, P.A.; Dollase, R.; Dumenco, L.; Taylor, J.; Green, E. The Warren Alpert Medical School of Brown University. Acad. Med. 2010, 85, S520–S524. [Google Scholar] [CrossRef]
- Smith, S.R.; Dollase, R. AMEE Guide No. 14: Outcome-based education: Part 2—Planning, implementing and evaluating a competency-based curriculum. Med. Teach. 1999, 21, 15–22. [Google Scholar] [CrossRef]
- Chai, C.S.; Liang, J.; Tsai, C.; Dong, Y. Surveying and modelling China high school students’ experience of and preferences for twenty-first-century learning and their academic and knowledge creation efficacy. Educ. Stud. 2020, 46, 658–675. [Google Scholar]
- Myers, T.; Blackman, A.; Andersen, T.; Hay, R.; Lee, I.; Gray, H. Cultivating ICT students’ interpersonal soft skills in online learning environments using traditional active learning techniques. J. Learn. Des. 2014, 7, 38–53. [Google Scholar] [CrossRef]
- Tkachuk, V.; Yechkalo, Y.; Semerikov, S.; Kislova, M.; Hladyr, Y. Using Mobile Ict for Online Learning during COVID-19 Lockdown. In International Conference on Information and Communication Technologies in Education, Research, and Industrial Applications; Springer: Cham, Switzerland, 2020; pp. 46–67. [Google Scholar]
- Herrera-Pavo, M.Á. Collaborative learning for virtual higher education. Learn. Cult. Soc. Interact. 2021, 28, 100437. [Google Scholar] [CrossRef]
- Ansari, J.A.; Khan, N.A. Exploring the role of social media in collaborative learning the new domain of learning. Smart Learn. Environ. 2020, 7, 9. [Google Scholar] [CrossRef]
- Sumuer, E. Factors related to college students’ self-directed learning with technology. Australas. J. Educ. Technol. 2018, 34, 29–43. [Google Scholar] [CrossRef]
- Asfar, N.; Zainuddin, Z. Secondary students’ perceptions of information, communication and technology (ICT) use in promoting self directed learning in Malaysia. Online J. Distance Educ. E-Learn. 2015, 3, 67–82. [Google Scholar]
- Bevis, E.O. Teaching and Learning: A Practical Commentary. In Toward a Caring Curriculum: A New Pedagogy for Nursing; Bevis, E.O., Watson, J., Eds.; National League for Nursing: New York, NY, USA, 1989. [Google Scholar]
- Kusumawati, R.; Hadi, A.F. Implementation of integrated inquiry collaborative learning based on the lesson study for learning community to improve students’ creative thinking skill. J. Phys. Conf. Ser. 2019, 1211, 012097. [Google Scholar] [CrossRef]
- Geng, S.; Law, K.M.; Niu, B. Investigating self-directed learning and technology readiness in blending learning environment. Int. J. Educ. Technol. High. Educ. 2019, 16, 17. [Google Scholar] [CrossRef]
- Ericsson, K.A.; Hastie, R. Contemporary Approaches to the Study of Thinking and Problem Solving. In Thinking and Problem-Solving; Sternberg, R.J., Ed.; Academic Press: New York, NY, USA, 1994; pp. 37–79. [Google Scholar]
- Wilkerson, L.A.; Stevens, C.M.; Krasne, S. No Content Without Context: Integrating Basic, Clinical, and Social Sciences in a Pre-clerkship Curriculum. Med. Teach. 2009, 31, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Saiyad, S.; Virk, A.; Mahajan, R.; Singh, T. Online teaching in medical training: Establishing good online teaching practices from cumulative experience. Int. J. Appl. Basic Med. Res. 2020, 10, 149. [Google Scholar] [PubMed]
- Naidoo, N.; Akhras, A.; Banerjee, Y. Confronting the challenges of anatomy education in a competency-based medical curriculum during normal and unprecedented times (COVID-19 pandemic): Pedagogical framework development and implementation. JMIR Med. Educ. 2020, 6, e21701. [Google Scholar] [CrossRef] [PubMed]
- Biggs, J. Student Approaches to Learning and Studying; Australian Council for Educational Research: Melbourne, Australia, 1987. [Google Scholar]
- Romanelli, F.; Bird, E.; Ryan, M. Learning styles: A review of theory, application, and best practices. Am. J. Pharm. Educ. 2009, 73, 9. [Google Scholar] [CrossRef]
- Daniel, M.; Rencic, J.; Durning, S.J.; Holmboe, E.; Santen, S.A.; Lang, V.; Ratcliffe, T.; Gordon, D.; Heist, B.; Lubarsky, S.; et al. Clinical reasoning assessment methods: A scoping review and practical guidance. Acad. Med. 2019, 94, 902–912. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Field, A.P. Discovering Statistics Using SPSS; SAGE Publications: London, UK, 2009. [Google Scholar]
- Raubenheimer, J. An item selection procedure to maximize scale reliability and validity. SA J. Ind. Psychol. 2004, 30, 59–64. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Schmitt, T.A.; Sass, D.A.; Chappelle, W.; Thompson, W. Selecting the “best” factor structure and moving measurement validation forward: An illustration. J. Personal. Assess. 2018, 100, 345–362. [Google Scholar] [CrossRef]
- Wang, J.C.; Wang, X.Q. Structural Equation Modeling, 3rd ed.; Wiley Series in Probability and Statistics; Wiley: Somerset, Australia, 2012. [Google Scholar]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis, 7th ed.; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Cullen, M.W.; Geske, J.B.; Anavekar, N.S.; McAdams, J.A.; Beliveau, M.E.; Ommen, S.R.; Nishimura, R.A. Reinvigorating continuing medical education: Meeting the challenges of the digital age. Mayo Clin. Proc. 2019, 94, 2501–2509. [Google Scholar] [CrossRef]
- Wartman, S.A. The empirical challenge of 21st-century medical education. Acad. Med. 2019, 94, 1412–1415. [Google Scholar] [CrossRef]
- Pujiati, P.A. The difference in clinical reasoning competence between pre-clinical students and clinical students on pediatric tropical disease cases. Sains Med. J. Kedokt. Dan Kesehat. 2015, 6, 25–29. [Google Scholar] [CrossRef][Green Version]
- Al Kadri, H.M.; Al-Moamary, M.S.; Elzubair, M.; Magzoub, M.E.; AlMutairi, A.; Roberts, C.; van der Vleuten, C. Exploring factors affecting undergraduate medical students’ study strategies in the clinical years: A qualitative study. Adv. Health Sci. Educ. Theory Pract. 2011, 16, 553–567. [Google Scholar] [CrossRef]
- Birgili, B. Creative and Critical Thinking Skills in Problem-based Learning Environments. J. Gift. Educ. Creat. 2015, 2, 71–80. [Google Scholar]
- Hamza, M.K.; Griffith, K.G. Fostering problem-solving & creative thinking in the classroom: Cultivating a creative mind. Natl. Forum Appl. Educ. Res. J.-Electron. 2006, 9, 1–32. [Google Scholar]
- Song, Y.; Lee, Y.; Lee, J. Mediating effects of self-directed learning on the relationship between critical thinking and problem-solving in student nurses attending online classes: A cross-sectional descriptive study. Nurse Educ. Today 2022, 109, 105227. [Google Scholar] [CrossRef] [PubMed]
- Chai, C.S.; Hwee Ling Koh, J.; Teo, Y.H. Enhancing and Modeling Teachers’ Design Beliefs and Efficacy of Technological Pedagogical Content Knowledge for 21st Century Quality Learning. J. Educ. Comput. Res. 2019, 57, 360–384. [Google Scholar] [CrossRef]
- Chacko, T. Blended learning in the 21st century: The need to tailor it to the changing learner self-direction levels during different phases of health professions education and beyond. Arch. Med. Health Sci. 2021, 9, 16–18. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Items | Mean | SD | Skew * | Kurt * | Item Loading |
|---|---|---|---|---|---|
| Collaborative Learning and Professionalism (CoL) | Cronbach’s α = 0.92, CR = 0.92, AVE = 0.73 | ||||
| 1. In this class, my classmates and I discuss different views we have and about things we are learning. | 4.75 | 1.34 | −0.53 | −0.14 | 0.87 |
| 2. In this class, I get helpful comments about my work from other classmates. | 4.61 | 1.36 | −0.47 | −0.15 | 0.83 |
| 3. In this class, my classmates and I actively work together to learn new things. | 4.74 | 1.35 | −0.51 | −0.15 | 0.89 |
| 4. In this class, my classmates and I actively share and explain our understanding. | 4.77 | 1.30 | −0.50 | −0.16 | 0.83 |
| Critical Thinking (CriT) | Cronbach’s α = 0.91, CR = 0.91, AVE = 0.73 | ||||
| 1. In this class, I distinguish what is supported by evidence and what is not. | 5.12 | 1.09 | −0.53 | 0.67 | 0.76 |
| 2. In this class, I think about other possible ways of understanding what I am learning. | 5.22 | 1.12 | −0.68 | 0.90 | 0.88 |
| 3. In this class, I evaluate different opinions to see which one makes more sense. | 5.21 | 1.13 | −0.67 | 1.08 | 0.91 |
| 4. In this class, I decide what kind of information can be trusted. | 5.15 | 1.09 | −0.62 | 0.77 | 0.85 |
| Self-Directed Learning (SDL) | Cronbach’s α = 0.93, CR = 0.91, AVE = 0.71 | ||||
| 1. In this class, I set goals for my studying. | 5.47 | 1.24 | −0.87 | 0.86 | 0.86 |
| 2. In this class, I check my progress when I study. | 5.47 | 1.13 | −0.82 | 1.29 | 0.85 |
| 3. In this class, I think about different ways or methods I can use to improve my study. | 5.54 | 1.16 | −0.85 | 1.18 | 0.82 |
| 4. In this class, I reflect on the ways I study. | 5.53 | 1.12 | −0.76 | 1.10 | 0.84 |
| Creative Thinking (CreT) | Cronbach’s α = 0.95, CR = 0.84, AVE = 0.95 | ||||
| 1. In this class, I suggest new ways of doing things. | 4.38 | 1.39 | −0.24 | −0.28 | 0.92 |
| 2. In this class, I design objects that may be helpful. | 4.18 | 1.49 | −0.25 | −0.39 | 0.87 |
| 3. In this class, I produce ideas that are likely to be useful. | 4.49 | 1.36 | −0.40 | 0.05 | 0.94 |
| 4. In this class, I develop innovative ideas. | 4.26 | 1.41 | −0.24 | −0.24 | 0.92 |
| Meaningful Learning with ICT (MLT) | Cronbach’s α = 0.90, CR = 0.95, AVE = 0.83 | ||||
| 1. In this class, my classmates and I actively communicate online (e.g., LMS, Discussion Forum, Facebook, Wiki, WhatsApp, WeChat etc.) to learn new things together. | 5.29 | 1.22 | −0.74 | 0.60 | 0.65 |
| 2. In this class, I find out useful information on the Internet to facilitate my learning. | 5.69 | 1.17 | −0.83 | 0.45 | 0.89 |
| 3. In this class, I use the computer to organize, retrieve and save the information for my learning. (e.g., Blackboard.) | 5.72 | 1.15 | −0.75 | 0.40 | 0.88 |
| 4. In this class, I can use information technology to access accurate and reliable medical information. | 5.68 | 1.12 | −0.92 | 0.95 | 0.91 |
| Authentic Problem Solving (APS) | Cronbach’s α = 0.94, CR = 0.93, AVE = 0.77 | ||||
| 1. In this class, I learn about real-life problems. | 5.34 | 1.14 | −0.74 | 1.06 | 0.89 |
| 2. In this class, I investigate the reasons that give rise to real-world problems. | 5.28 | 1.17 | −0.66 | 0.66 | 0.90 |
| 3. In this class, I apply the knowledge I have to solve real-life problems. | 5.22 | 1.15 | −0.49 | 0.52 | 0.89 |
| 4. In this class, I can simultaneously apply and integrate the medical knowledge I learn to diagnose a problem. | 5.24 | 1.15 | −0.53 | 0.52 | 0.82 |
| Ability of using Basic Science in the Practice of Medicine (ABS) | Cronbach’s α = 0.93, CR = 0.89, AVE = 0.63 | ||||
| 1. I am able to describe the normal structure, function, and development of the human body. | 5.22 | 1.01 | −0.39 | 0.42 | 0.80 |
| 2. I can describe the risk factors, pathophysiologic mechanisms, structural and functional changes, and consequences of the underlying health problem. | 5.02 | 1.14 | −0.70 | 0.95 | 0.84 |
| 3. I can develop a therapeutic plan, incorporating risks and benefits, based on the mechanistic understanding of disease pathogenesis. | 4.57 | 1.38 | −0.59 | 0.02 | 0.87 |
| 4. I can measure and analyze the effectiveness of an applied intervention. | 4.58 | 1.36 | −0.56 | 0.14 | 0.88 |
| 5. I can articulate the pathophysiologic and pharmacologic rationales for the chosen therapy and expected outcomes at an appropriate level. | 4.62 | 1.33 | −0.61 | 0.31 | 0.52 |
| Factor | CoL | CriT | SDL | CreT | MLT | APS |
|---|---|---|---|---|---|---|
| CriT | 0.54 ** | |||||
| SDL | 0.43 ** | 0.60 ** | ||||
| CreT | 0.49 ** | 0.54 ** | 0.38 ** | |||
| MLT | 0.65 ** | 0.55 ** | 0.68 ** | 0.24 ** | ||
| APS | 0.43 ** | 0.57 ** | 0.59 ** | 0.38 ** | 0.62 ** | |
| ABS | 0.29 ** | 0.44 ** | 0.39 ** | 0.40 ** | 0.28 ** | 0.44 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, S.; Chai, C.S.; Lee, V.W.Y. Surveying and Modelling 21st Century Online Learning Patterns of Medical Students. Int. J. Environ. Res. Public Health 2022, 19, 12648. https://doi.org/10.3390/ijerph191912648
Liang S, Chai CS, Lee VWY. Surveying and Modelling 21st Century Online Learning Patterns of Medical Students. International Journal of Environmental Research and Public Health. 2022; 19(19):12648. https://doi.org/10.3390/ijerph191912648
Chicago/Turabian StyleLiang, Siya, Ching Sing Chai, and Vivian W. Y. Lee. 2022. "Surveying and Modelling 21st Century Online Learning Patterns of Medical Students" International Journal of Environmental Research and Public Health 19, no. 19: 12648. https://doi.org/10.3390/ijerph191912648
APA StyleLiang, S., Chai, C. S., & Lee, V. W. Y. (2022). Surveying and Modelling 21st Century Online Learning Patterns of Medical Students. International Journal of Environmental Research and Public Health, 19(19), 12648. https://doi.org/10.3390/ijerph191912648