

Environmental Regulation and Chronic Conditions: Evidence from China’s Air Pollution Prevention and Control Action Plan

Abstract
:1. Introduction
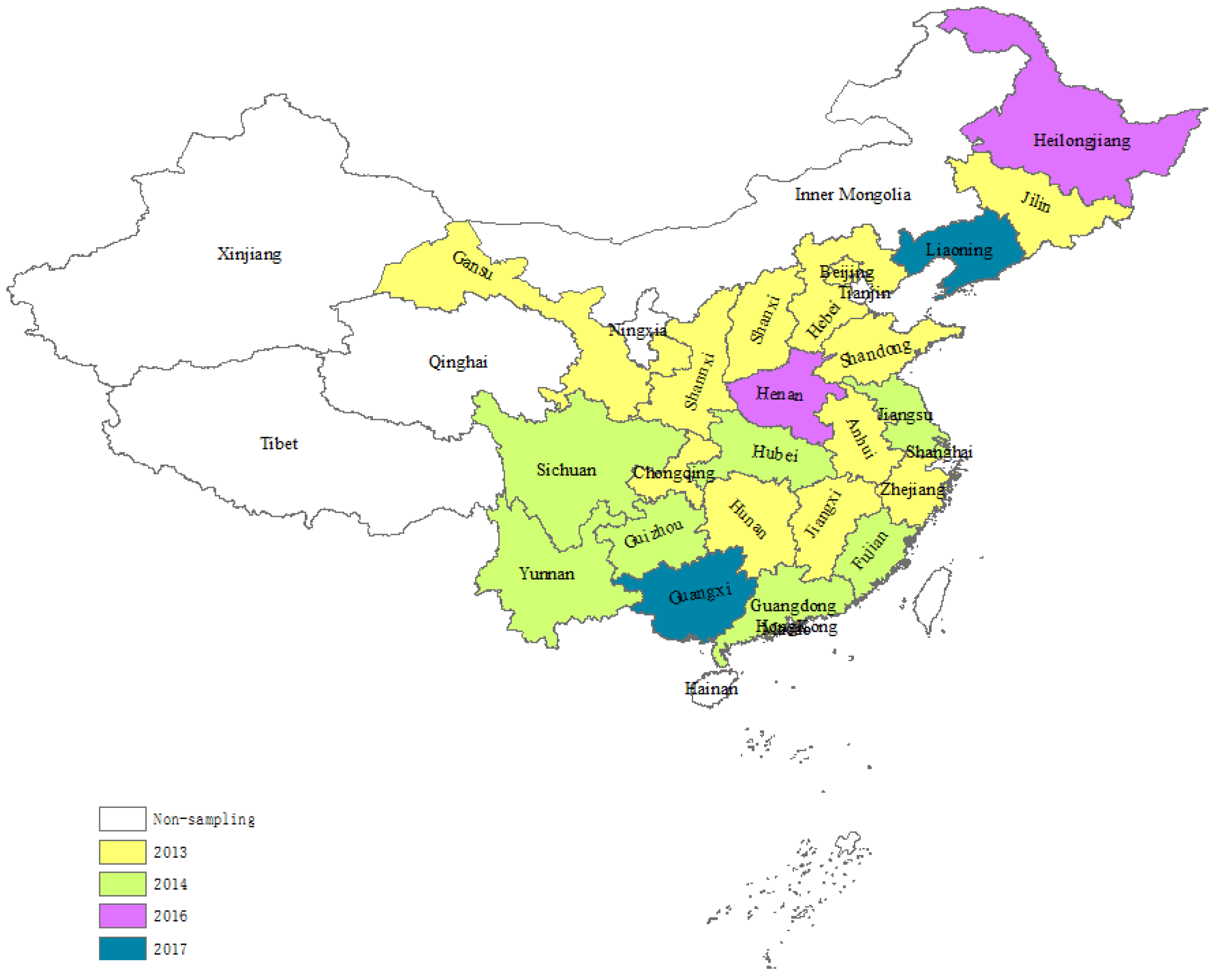
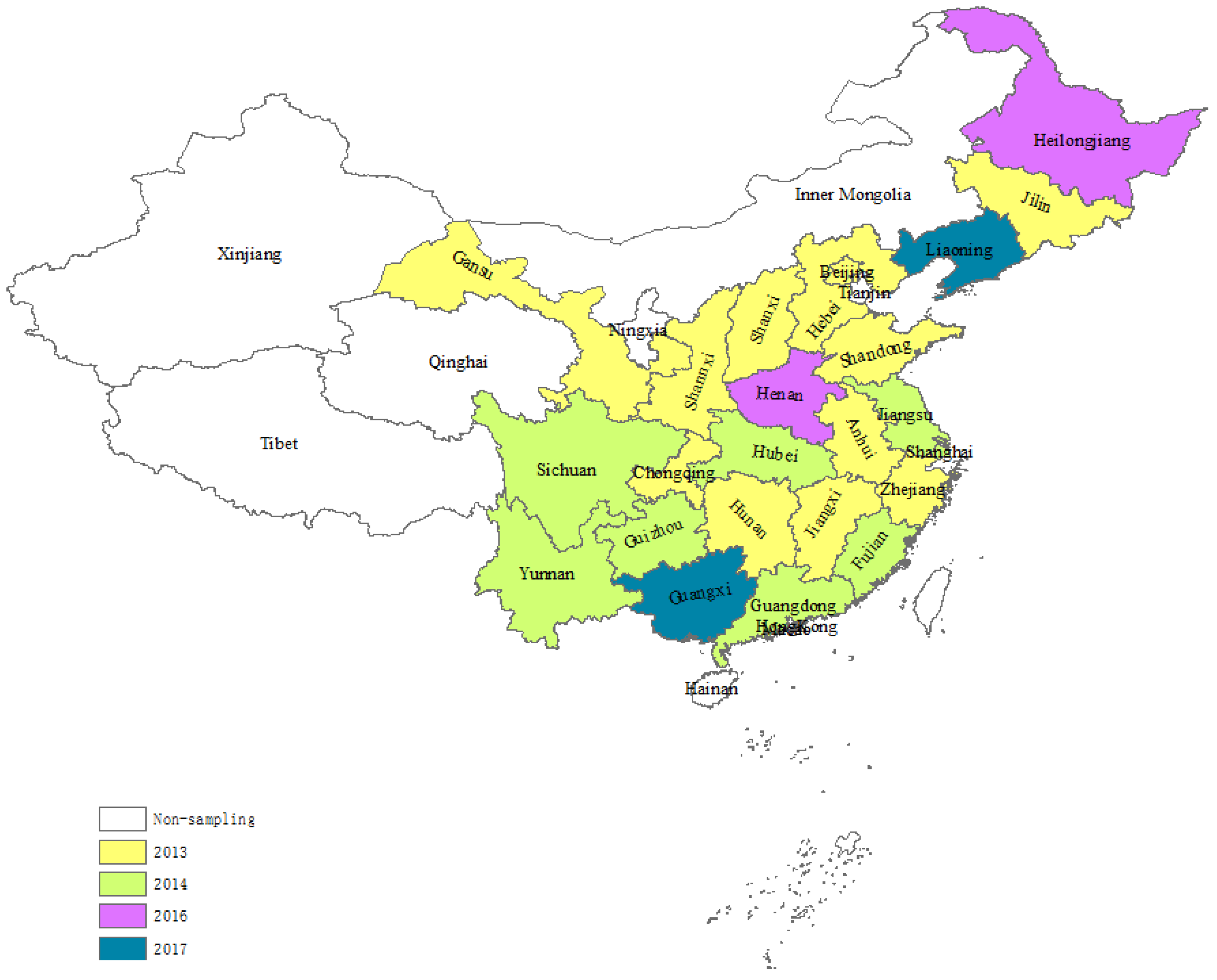
2. Air Pollution Prevention and Control Action Plan (2013–2017)
3. Data: China Family Panel Studies
3.1. Dependent Variables
3.2. Weather Conditions
4. The Econometric Model
5. Results
5.1. All Adults
5.2. Results by Subsample
5.2.1. Sex and Age
5.2.2. Socioeconomic Status
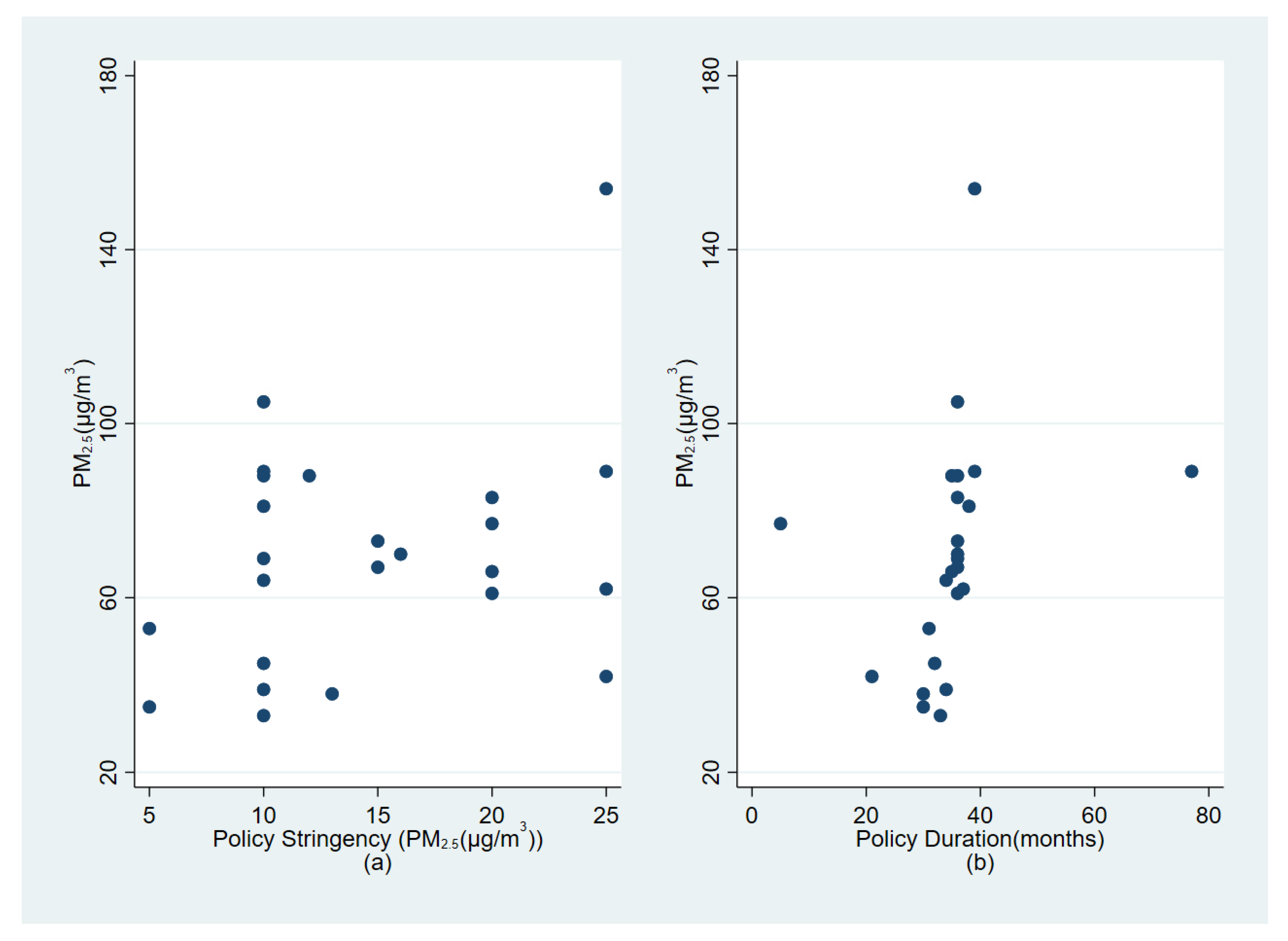
5.3. Results by Policy Characteristics
5.4. Placebo Test
5.4.1. In-Time Placebo Test
5.4.2. Placebo Outcome Test
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. 7 Million Premature Deaths Annually Linked to Air Pollution. Available online: https://www.who.int/news/item/25-03-2014-7-million-premature-deaths-annually-linked-to-air-pollution (accessed on 22 August 2022).
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Pan, X.; Guo, X.; Li, G. Health impact of China’s Air Pollution Prevention and Control Action Plan: An analysis of national air quality monitoring and mortality data. Lancet Planet. Health 2018, 2, e313–e323. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Xu, P.; Chen, Y.; Ye, X. Haze, air pollution, and health in China. Lancet 2013, 382, 2067. [Google Scholar] [CrossRef]
- Ministry of Ecology and Environment of the People’s Republic of China. 2014 Report on the State of the Environment in China. Available online: https://www.mee.gov.cn/hjzl/sthjzk/zghjzkgb/201605/P020160526564730573906.pdf (accessed on 22 August 2022).
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; WHO: Geneva, Switzerland, 2021; pp. 74–88. ISBN 978-92-4-003422-8. [Google Scholar]
- Rohde, R.A.; Muller, R.A. Air pollution in China: Mapping of concentrations and sources. PLoS ONE 2015, 10, e0135749. [Google Scholar]
- Zhang, J.; Mauzerall, D.L.; Zhu, T.; Liang, S.; Ezzati, M.; Remais, J.V. Environmental health in China: Progress towards clean air and safe water. Lancet 2010, 375, 1110–1119. [Google Scholar] [CrossRef] [Green Version]
- Liang, L.; Cai, Y.; Barratt, B.; Lyu, B.; Chan, Q.; Hansell, A.L.; Xie, W.; Zhang, D.; Kelly, F.J.; Tong, Z. Associations between daily air quality and hospitalisations for acute exacerbation of chronic obstructive pulmonary disease in Beijing, 2013–2017: An ecological analysis. Lancet Planet. Health 2019, 3, e270–e279. [Google Scholar] [CrossRef] [Green Version]
- Brunekreef, B.; Holgate, S.T. Air pollution and health. Lancet 2002, 360, 1233–1242. [Google Scholar] [CrossRef]
- Krall, J.R.; Anderson, G.B.; Dominici, F.; Bell, M.L.; Peng, R.D. Short-term exposure to particulate matter constituents and mortality in a national study of US urban communities. Environ. Health Perspect. 2013, 121, 1148–1153. [Google Scholar] [CrossRef] [Green Version]
- Landrigan, P.J.; Fuller, R.; Horton, R. Environmental pollution, health, and development: A Lancet–global alliance on health and pollution—Icahn School of Medicine at Mount Sinai Commission. Lancet 2015, 386, 1429–1431. [Google Scholar] [CrossRef]
- Rich, D.Q.; Kipen, H.M.; Huang, W.; Wang, G.; Wang, Y.; Zhu, P.; Ohman-Strickland, P.; Hu, M.; Philipp, C.; Diehl, S.R. Association between changes in air pollution levels during the Beijing Olympics and biomarkers of inflammation and thrombosis in healthy young adults. JAMA 2012, 307, 2068–2078. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Deng, F.; Niu, J.; Huang, Q.; Liu, Y.; Guo, X. Association of heart rate variability in taxi drivers with marked changes in particulate air pollution in Beijing in 2008. Environ. Health Perspect. 2010, 118, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rückerl, R.; Schneider, A.; Breitner, S.; Cyrys, J.; Peters, A. Health effects of particulate air pollution: A review of epidemiological evidence. Inhal. Toxicol. 2011, 23, 555–592. [Google Scholar] [CrossRef] [PubMed]
- Wamble, D.E.; Ciarametaro, M.; Dubois, R. The effect of medical technology innovations on patient outcomes, 1990–2015: Results of a physician survey. J. Manag. Care Spec. Pharm. 2019, 25, 66–71. [Google Scholar] [CrossRef]
- Fang, D.; Chen, B.; Hubacek, K.; Ni, R.; Chen, L.; Feng, K.; Lin, J. Clean air for some: Unintended spillover effects of regional air pollution policies. Sci. Adv. 2019, 5, eaav4707. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.; Huang, W.; Zhu, T.; Hu, M.; Brunekreef, B.; Zhang, Y.; Liu, X.; Cheng, H.; Gehring, U.; Li, C. Acute respiratory inflammation in children and black carbon in ambient air before and during the 2008 Beijing Olympics. Environ. Health Perspect. 2011, 119, 1507–1512. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Liu, T.; Fang, F.; Xiao, J.; Zeng, W.; Li, X.; Guo, L.; Tian, L.; Schootman, M.; Stamatakis, K.A. Mortality benefits of vigorous air quality improvement interventions during the periods of APEC Blue and Parade Blue in Beijing, China. Environ. Pollut. 2017, 220, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; Zhu, Y.; Jang, C.; Lin, C.-J.; Wang, S.; Fu, J.; Gao, J.; Deng, S.; Xie, J.; Qiu, X. Evaluation of health benefit using BenMAP-CE with an integrated scheme of model and monitor data during Guangzhou Asian Games. J. Environ. Sci. 2016, 42, 9–18. [Google Scholar] [CrossRef]
- Chen, R.; Chu, C.; Tan, J.; Cao, J.; Song, W.; Xu, X.; Jiang, C.; Ma, W.; Yang, C.; Chen, B. Ambient air pollution and hospital admission in Shanghai, China. J. Hazard. Mater. 2010, 181, 234–240. [Google Scholar] [CrossRef]
- Wang, S.; Zhao, B.; Cai, S.; Klimont, Z.; Nielsen, C.; Morikawa, T.; Woo, J.; Kim, Y.; Fu, X.; Xu, J. Emission trends and mitigation options for air pollutants in East Asia. Atmos. Chem. Phys. 2014, 14, 6571–6603. [Google Scholar] [CrossRef] [Green Version]
- Greenstone, M.; Hanna, R. Environmental Regulations, Air and Water Pollution, and Infant Mortality in India. Am. Econ. Rev. 2014, 104, 3038–3072. [Google Scholar] [CrossRef]
- Yin, P.; Brauer, M.; Cohen, A.J.; Wang, H.; Li, J.; Burnett, R.T.; Stanaway, J.D.; Causey, K.; Larson, S.; Godwin, W. The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990–2017: An analysis for the Global Burden of Disease Study 2017. Lancet Planet. Health 2020, 4, e386–e398. [Google Scholar] [CrossRef]
- Pope, C.A., III; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Zheng, X.-Y.; Chung, K.F.; Zhong, N.-S. Impact of air pollution on the burden of chronic respiratory diseases in China: Time for urgent action. Lancet 2016, 388, 1939–1951. [Google Scholar] [CrossRef]
- Seaton, A.; Godden, D.; MacNee, W.; Donaldson, K. Particulate air pollution and acute health effects. Lancet 1995, 345, 176–178. [Google Scholar] [CrossRef]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef] [Green Version]
- Patel, J.C.; Khurana, P.; Sharma, Y.K.; Kumar, B.; Ragumani, S. Chronic lifestyle diseases display seasonal sensitive comorbid trend in human population evidence from Google Trends. PLoS ONE 2018, 13, e0207359. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics of China. China Statistical Yearbook 2013; Environmental Section, China Statistics Press: Beijing, China, 2013; ISBN 7503769637. [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook 2014; Environmental Section, China Statistics Press: Beijing, China, 2014; ISBN 9787503772801. [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook 2015; Environmental Section, China Statistics Press: Beijing, China, 2015; ISBN 9787503776380. [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook 2016; Environmental Section, China Statistics Press: Beijing, China, 2016; ISBN 9787503779176. [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook 2017; Environmental Section, China Statistics Press: Beijing, China, 2017; ISBN 9787503782534. [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook 2018; Environmental Section, China Statistics Press: Beijing, China, 2018; ISBN 9787503785870. [Google Scholar]
- Iqbal, N.; Fareed, Z.; Shahzad, F.; He, X.; Shahzad, U.; Lina, M. The nexus between COVID-19, temperature and exchange rate in Wuhan city: New findings from partial and multiple wavelet coherence. Sci. Total Environ. 2020, 729, 138916. [Google Scholar] [CrossRef]
- Bergtold, J.S.; Yeager, E.A.; Featherstone, A.M. Inferences from logistic regression models in the presence of small samples, rare events, nonlinearity, and multicollinearity with observational data. J. Appl. Stat. 2018, 45, 528–546. [Google Scholar] [CrossRef]
- Beck, T.; Levine, R.; Levkov, A. Big bad banks? The winners and losers from bank deregulation in the United States. J. Financ. 2010, 65, 1637–1667. [Google Scholar] [CrossRef] [Green Version]
- Hardman, R.; Begg, S.; Spelten, E. What impact do chronic disease self-management support interventions have on health inequity gaps related to socioeconomic status: A systematic review. BMC Health Serv. Res. 2020, 20, 150. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Peng, R.D.; Meng, X.; Zhou, Z.; Chen, B.; Kan, H. Seasonal variation in the acute effect of particulate air pollution on mortality in the China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2013, 450, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacks, J.D.; Stanek, L.W.; Luben, T.J.; Johns, D.O.; Buckley, B.J.; Brown, J.S.; Ross, M. Particulate matter–induced health effects: Who is susceptible? Environ. Health Perspect. 2011, 119, 446–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Zhang, J.; Xu, Y.; Sun, H.; Ding, Z. Associations between individual perceptions of PM2.5 pollution and pulmonary function in Chinese middle-aged and elderly residents. BMC Public Health 2020, 20, 899. [Google Scholar] [CrossRef]
- Bryazka, D.; Reitsma, M.B.; Griswold, M.G.; Abate, K.H.; Abbafati, C.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abdoli, A.; Abdollahi, M.; Abdullah, A.Y.M. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: A systematic analysis for the Global Burden of Disease Study 2020. Lancet 2022, 400, 185–235. [Google Scholar] [CrossRef]
- Granados-Canal, D.; Chardon, B.; Lefranc, A.; Gremy, I. Air pollution and respiratory hospital admissions in greater Paris: Exploring sex differences. Arch. Environ. Occup. Health 2005, 60, 307–313. [Google Scholar] [CrossRef]
- Shin, H.H.; Parajuli, R.P.; Gogna, P.; Maquiling, A.; Dehghani, P. Pollutant-sex specific differences in respiratory hospitalization and mortality risk attributable to short-term exposure to ambient air pollution. Sci. Total Environ. 2021, 755, 143135. [Google Scholar] [CrossRef]
- Su, C.; Breitner, S.; Schneider, A.; Liu, L.; Franck, U.; Peters, A.; Pan, X. Short-term effects of fine particulate air pollution on cardiovascular hospital emergency room visits: A time-series study in Beijing, China. Int. Arch. Occup. Environ. Health 2016, 89, 641–657. [Google Scholar] [CrossRef]
- Xia, X.; Zhang, A.; Liang, S.; Qi, Q.; Jiang, L.; Ye, Y. The association between air pollution and population health risk for respiratory infection: A case study of Shenzhen, China. Int. J. Environ. Res. Public Health 2017, 14, 950. [Google Scholar] [CrossRef] [Green Version]
- Anderson, H.; Atkinson, R.; Bremner, S.; Marston, L. Particulate air pollution and hospital admissions for cardiorespiratory diseases: Are the elderly at greater risk? Eur. Respir. J. 2003, 21, 39s–46s. [Google Scholar] [CrossRef] [Green Version]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Laaksonen, M.; Rahkonen, O.; Martikainen, P.; Lahelma, E. Socioeconomic position and self-rated health: The contribution of childhood socioeconomic circumstances, adult socioeconomic status, and material resources. Am. J. Public Health 2005, 95, 1403–1409. [Google Scholar] [CrossRef]
- Cesaroni, G.; Badaloni, C.; Romano, V.; Donato, E.; Perucci, C.A.; Forastiere, F. Socioeconomic position and health status of people who live near busy roads: The Rome Longitudinal Study (RoLS). Environ. Health 2010, 9, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spalt, E.W.; Curl, C.L.; Allen, R.W.; Cohen, M.; Williams, K.; Hirsch, J.A.; Adar, S.D.; Kaufman, J.D. Factors influencing time-location patterns and their impact on estimates of exposure: The Multi-Ethnic Study of Atherosclerosis and Air Pollution (MESA Air). J. Expo. Sci. Environ. Epidemiol. 2016, 26, 341–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggers, A.C.; Tuñón, G.; Dafoe, A. Placebo Tests for Causal Inference. 2021. Available online: https://pelg.ucsd.edu/Eggers_2021.pdf (accessed on 22 August 2022).
- Mideksa, T.K. The economic impact of natural resources. J. Environ. Econ. Manag. 2013, 65, 277–289. [Google Scholar] [CrossRef]
- Hartman, E.; Hidalgo, F.D. An equivalence approach to balance and placebo tests. Am. J. Political Sci. 2018, 62, 1000–1013. [Google Scholar] [CrossRef]
- Dube, A.; Dube, O.; García-Ponce, O. Cross-border spillover: US gun laws and violence in Mexico. Am. Political Sci. Rev. 2013, 107, 397–417. [Google Scholar] [CrossRef] [Green Version]
- Yue, H.; He, C.; Huang, Q.; Yin, D.; Bryan, B.A. Stronger policy required to substantially reduce deaths from PM2.5 pollution in China. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.-Y.; Dunea, D.; Iordache, S.; Pohoata, A. A review of airborne particulate matter effects on young children’s respiratory symptoms and diseases. Atmosphere 2018, 9, 150. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Tal, A. From Pollution Charge to Environmental Protection Tax: A Comparative Analysis of the Potential and Limitations of China’s New Environmental Policy Initiative. J. Comp. Policy Anal. Res. Pract. 2018, 20, 223–236. [Google Scholar] [CrossRef]
- Zhou, N.; Price, L.; Yande, D.; Creyts, J.; Khanna, N.; Fridley, D.; Lu, H.; Feng, W.; Liu, X.; Hasanbeigi, A. A roadmap for China to peak carbon dioxide emissions and achieve a 20% share of non-fossil fuels in primary energy by 2030. Appl. Energy 2019, 239, 793–819. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, W.; Liu, C.; Chen, R.; Kan, H. The association between long-term fine particulate air pollution and life expectancy in China, 2013 to 2017. Sci. Total Environ. 2020, 712, 136507. [Google Scholar] [CrossRef] [PubMed]
- Crane, K.; Mao, Z. Costs of Selected Policies to Address Air Pollution in China; RAND Corporation: Santa Monica, CA, USA, 2015. [Google Scholar]


{kind=link}
{kind=link}
| Administrative Division | APPCAP Enacted Time | Duration |
|---|---|---|
| Shandong | July 2013 | ~2020 |
| Beijing | September 2013 | ~2017 |
| Hebei | September 2013 | ~2017 |
| Shanxi | October 2013 | ~2017 |
| Shanghai | November 2013 | ~2017 |
| Anhui | December 2013 | ~2017 |
| Chongqing | December 2013 | ~2017 |
| Shannxi | December 2013 | ~2017 |
| Jilin | December 2013 | ~2017 |
| Zhejiang | December 2013 | ~2017 |
| Jiangxi | December 2013 | ~2017 |
| Hunan | December 2013 | ~2017 |
| Gansu | December 2013 | ~2017 |
| Hubei | January 2014 | ~2017 |
| Jiangsu | January 2014 | ~2017 |
| Guangdong | February 2014 | ~2017 |
| Sichuan | February 2014 | ~2017 |
| Yunnan | March 2014 | ~2017 |
| Guizhou | May 2014 | ~2017 |
| Fujian | June 2014 | ~2017 |
| Heilongjiang | March 2016 | ~2018 |
| Henan | July 2016 | ~2017 |
| Liaoning | April 2017 | ~2020 |
| Guangxi | June 2017 | ~2020 |
| Variables | Mean | Standard Deviation |
|---|---|---|
| Dependent Variables | ||
| Respiratory diseases (%) | 1.44 | 0.12 |
| Circulatory system diseases (%) | 6.57 | 0.17 |
| Independent Variables | ||
| Weather Conditions | ||
| Mean Temperature (°C) | 21.62 | 9.48 |
| Humidity (%) | 71.99 | 8.69 |
| Precipitation (mm) | 127.57 | 109.72 |
| Sunshine (hour) | 181.89 | 53.06 |
| Demographic characteristics of CFPS surveys | ||
| Age (year) | 48.66 | 14.81 |
| Mean annual household income a (log form) | 7.14 | 4.60 |
| Male (%) | 48.09 | 0.50 |
| Urban (%) | 46.63 | 0.50 |
| Labor force participation (%) | 72.80 | 0.44 |
| Primary school or less (%) | 26.67 | 0.46 |
| Middle/high school (%) | 29.93 | 0.46 |
| University or above (%) | 43.40 | 0.49 |
| Married (%) | 85.69 | 0.35 |
| Smoke (%) | 29.84 | 0.46 |
| Drink (%) | 16.29 | 0.37 |
| Coal (%) | 6.67 | 0.25 |
| Observations | 56,958 | |
| Air-Pollution-Related Diseases | ||
|---|---|---|
| Variables | Respiratory | Circulatory |
| Treatment × Post | −0.489 ** | −0.239 ** |
| (0.192) | (0.099) | |
| Age | 0.027 *** | 0.085 *** |
| (0.004) | (0.003) | |
| Male | 0.611 *** | −0.179 *** |
| (0.111) | (0.065) | |
| Urban | −0.002 | −0.003 |
| (0.100) | (0.057) | |
| Alcohol | −0.319 | −0.316 *** |
| (0.132) | (0.077) | |
| Tobacco | −0.681 | −0.329 *** |
| (0.120) | (0.069) | |
| Coal heating | −0.017 | −0.020 |
| (0.187) | (0.092) | |
| Married | −0.151 | 0.868 *** |
| (0.225) | (0.245) | |
| Cohabitating | 0.967 | 0.994 ** |
| (0.621) | (0.483) | |
| Divorced | 0.227 | 1.122 *** |
| (0.403) | (0.322) | |
| Widowed | −0.079 | 0.583 ** |
| (0.297) | (0.263) | |
| Employed | −0.091 | −0.318 *** |
| (0.109) | (0.058) | |
| ln (Annual household income) | 0.006 | 0.007 |
| (0.010) | (0.005) | |
| Middle/high school | −0.133 | 0.014 |
| (0.126) | (0.068) | |
| University or above | −0.053 | 0.009 |
| (0.207) | (0.122) | |
| Constant | −6.623 *** | −8.995 *** |
| (1.129) | (0.683) | |
| Observations | 56,958 | 56,958 |
| Marginal effects at means for Treatment × Post | −0.499 ** | −0.757 ** |
| (0.196) | (0.312) | |
| Dependent variable mean (×100) | 1.44 | 6.57 |
| Respiratory System Disease | ||||||
| Sex | Age | |||||
| Total | Male | Female | 16–39 | 40–64 | 65– | |
| Treatment Post | −0.489 ** (0.192) | −0.725 ** (0.296) | −0.338 (0.259) | −0.436 (0.399) | −0.421 (0.269) | −0.766 * (0.408) |
| Observations | 56,958 | 27,855 | 29,015 | 15,906 | 32,179 | 8649 |
| Marginal effects at means for Treatment × Post | −0.499 ** (0.196) | −0.737 ** (0.30) | −0.319 (0.244) | −0.259 (0.235) | −0.410 (0.260) | −1.367 * (0.718) |
| Dependent variable mean (×100) | 1.443 | 1.578 | 1.315 | 0.965 | 1.400 | 2.464 |
| Circulatory System Disease | ||||||
| Sex | Age | |||||
| Total | Male | Female | 16–39 | 40–64 | 65– | |
| Treatment × Post | −0.239 ** (0.099) | 0.043 (0.150) | −0.434 *** (0.132) | 0.303 (0.480) | −0.275 ** (0.119) | −0.286 * (0.165) |
| Observations | 56,958 | 27,855 | 29,103 | 15,906 | 32,179 | 8649 |
| Marginal effects at means for Treatment × Post | −0.757 ** (0.312) | 0.120 (0.419) | −1.508 *** (0.459) | −0.121 (0.188) | −1.109 ** (0.519) | −2.948 ** (1.700) |
| Dependent variable mean (×100) | 6.570 | 7.432 | 5.669 | 0.689 | 6.760 | 16.490 |
| Respiratory System Disease | ||||
| Educational Attainment Levels | ||||
| Total | Primary | Middle | College and above | |
| Treatment × Post | −0.489 ** (0.192) | −0.702 *(0.379) | −0.487 (0.398) | 0.232 (0.473) |
| Observations | 56,958 | 14,841 | 16,867 | 24,361 |
| Marginal effects at means for Treatment × Post | −0.499 ** (0.196) | −0.702 * (0.377) | −0.343 (0.278) | 0.269 (0.547) |
| Dependent variable mean (×100) | 1.443 | 1.579 | 1.119 | 1.584 |
| Circulatory System Disease | ||||
| Educational Attainment Levels | ||||
| Total | Primary | Middle | College and above | |
| Treatment × Post | −0.239 ** (0.099) | −0.246 * (0.173) | −0.045 (0.204) | 0.229 (0.317) |
| Observations | 56,958 | 15,188 | 16,986 | 24,578 |
| Marginal effects at means for Treatment × Post | −0.757 ** (0.312) | −1.003 * (0.705) | −0.099 (0.444) | 0.753 (1.046) |
| Dependent variable mean (×100) | 6.570 | 7.787 | 4.559 | 7.210 |
| Air-Pollution-Related Diseases | ||||
|---|---|---|---|---|
| Respiratory | Circulatory | Respiratory | Circulatory | |
| Stringency | −0.026 *** (0.009) | −0.022 *** (0.005) | ||
| Duration | −0.011 ** (0.004) | −0.005 ** (0.002) | ||
| Observations | 56,958 | 56,958 | 56,958 | 56,958 |
| Marginal effects at means | −0.027 *** (0.010) | −0.070 *** (0.016) | −0.011 ** (0.005) | −0.017 ** (0.008) |
| Dependent variable mean (×100) | 1.443 | 6.570 | 1.443 | 6.570 |
| Air-Pollution-Related Diseases | ||
|---|---|---|
| Respiratory | Circulatory | |
| Treatment Post (6-month in advance) | 0.152 (0.426) | −0.003 (0.202) |
| Observations | 30,111 | 30,111 |
| Marginal effects at means for Treatment × Post | 0.00130 (0.00365) | −0.00007 (0.00532) |
| Treatment Post (1-year in advance) | 0.138 (0.333) | −0.160 (0.140) |
| Observations | 26,899 | 26,899 |
| Marginal effects at means for Treatment × Post | 0.00121 (0.00291) | −0.00442 (0.00387) |
| Non-air-pollution-related diseases | ||
| Treatment Post | 0.061 (0.073) | |
| Observations | 56,958 | |
| Marginal effects at means for Treatment × Post | 0.00409 (0.00487) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Kim, B. Environmental Regulation and Chronic Conditions: Evidence from China’s Air Pollution Prevention and Control Action Plan. Int. J. Environ. Res. Public Health 2022, 19, 12584. https://doi.org/10.3390/ijerph191912584
Zhao Y, Kim B. Environmental Regulation and Chronic Conditions: Evidence from China’s Air Pollution Prevention and Control Action Plan. International Journal of Environmental Research and Public Health. 2022; 19(19):12584. https://doi.org/10.3390/ijerph191912584
Chicago/Turabian StyleZhao, Yang, and Beomsoo Kim. 2022. "Environmental Regulation and Chronic Conditions: Evidence from China’s Air Pollution Prevention and Control Action Plan" International Journal of Environmental Research and Public Health 19, no. 19: 12584. https://doi.org/10.3390/ijerph191912584
APA StyleZhao, Y., & Kim, B. (2022). Environmental Regulation and Chronic Conditions: Evidence from China’s Air Pollution Prevention and Control Action Plan. International Journal of Environmental Research and Public Health, 19(19), 12584. https://doi.org/10.3390/ijerph191912584