
The Influence of Alcohol Consumption, Depressive Symptoms and Sleep Duration on Cognition: Results from the China Health and Retirement Longitudinal Study

Abstract
1. Introduction
2. Materials and Methods
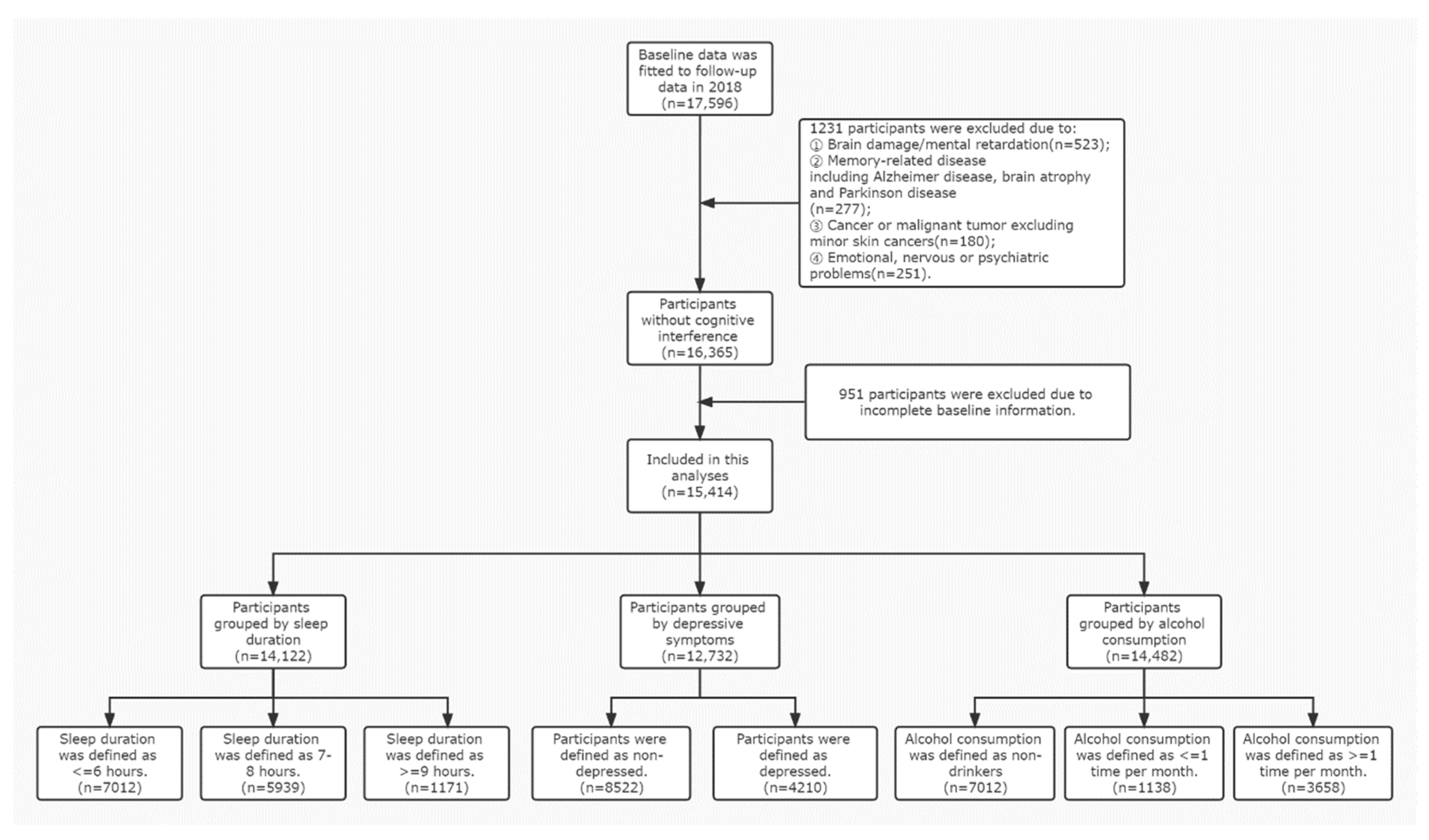
2.1. Data
2.2. Outcome
2.3. Exposure
2.4. Mediator
2.5. Moderator
2.6. Covariates
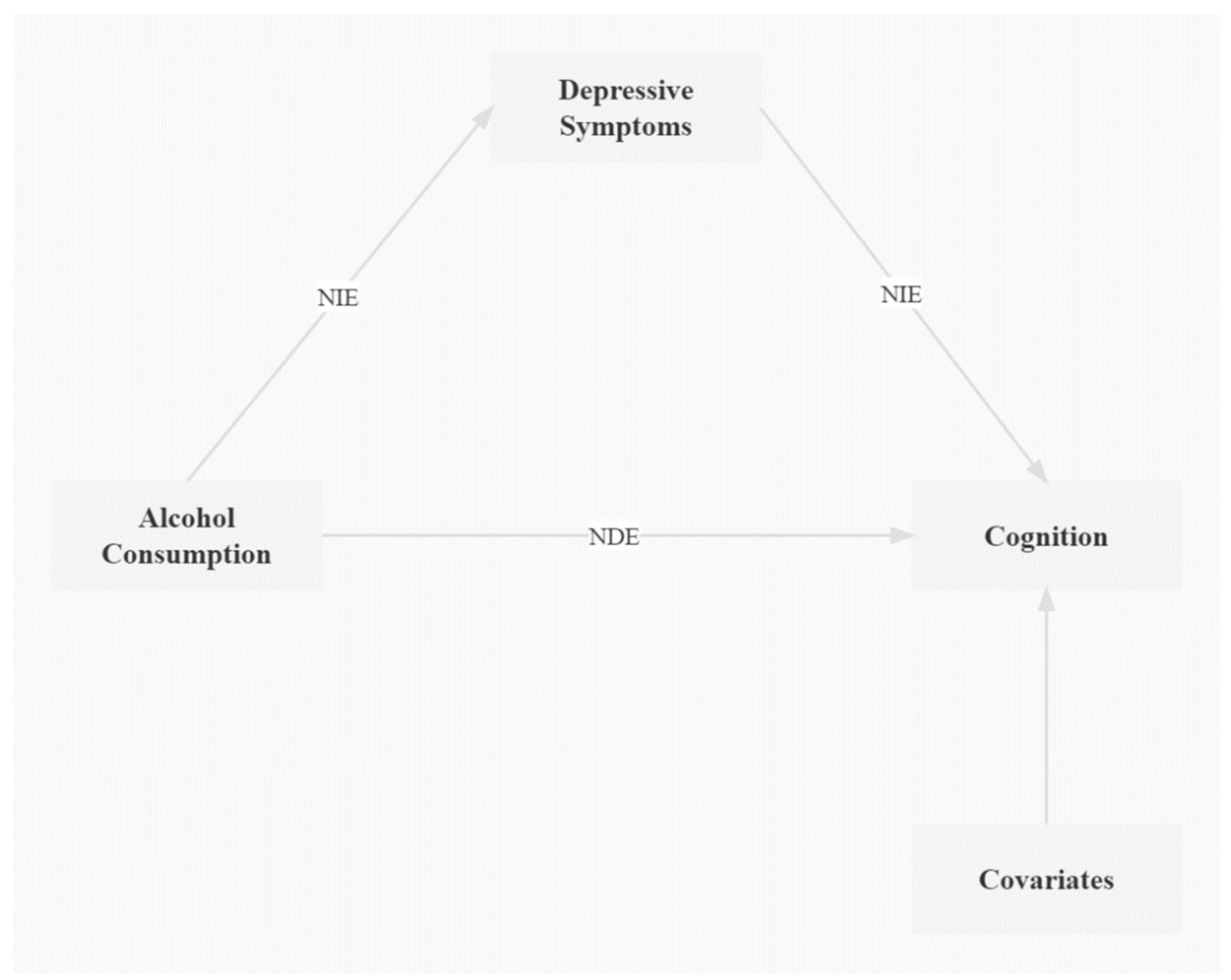
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Participants
3.2. Baseline Alcohol Consumption, Depressive Symptoms, Sleep Duration, and Cognition z Scores in Cross-Sectional Analyses
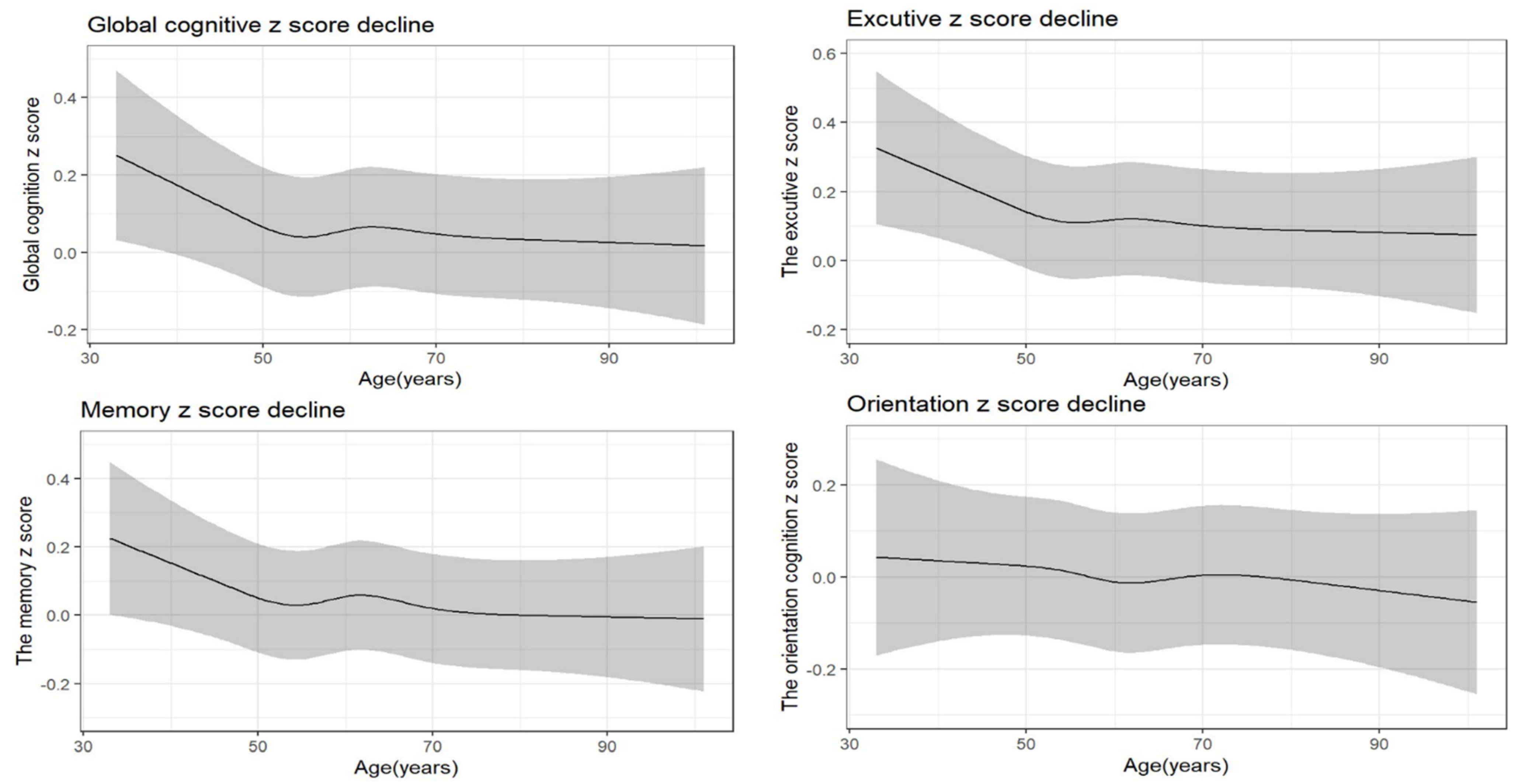
3.3. Mean Difference in Overall Rate of Change in Cognitive Decline during Follow-Up
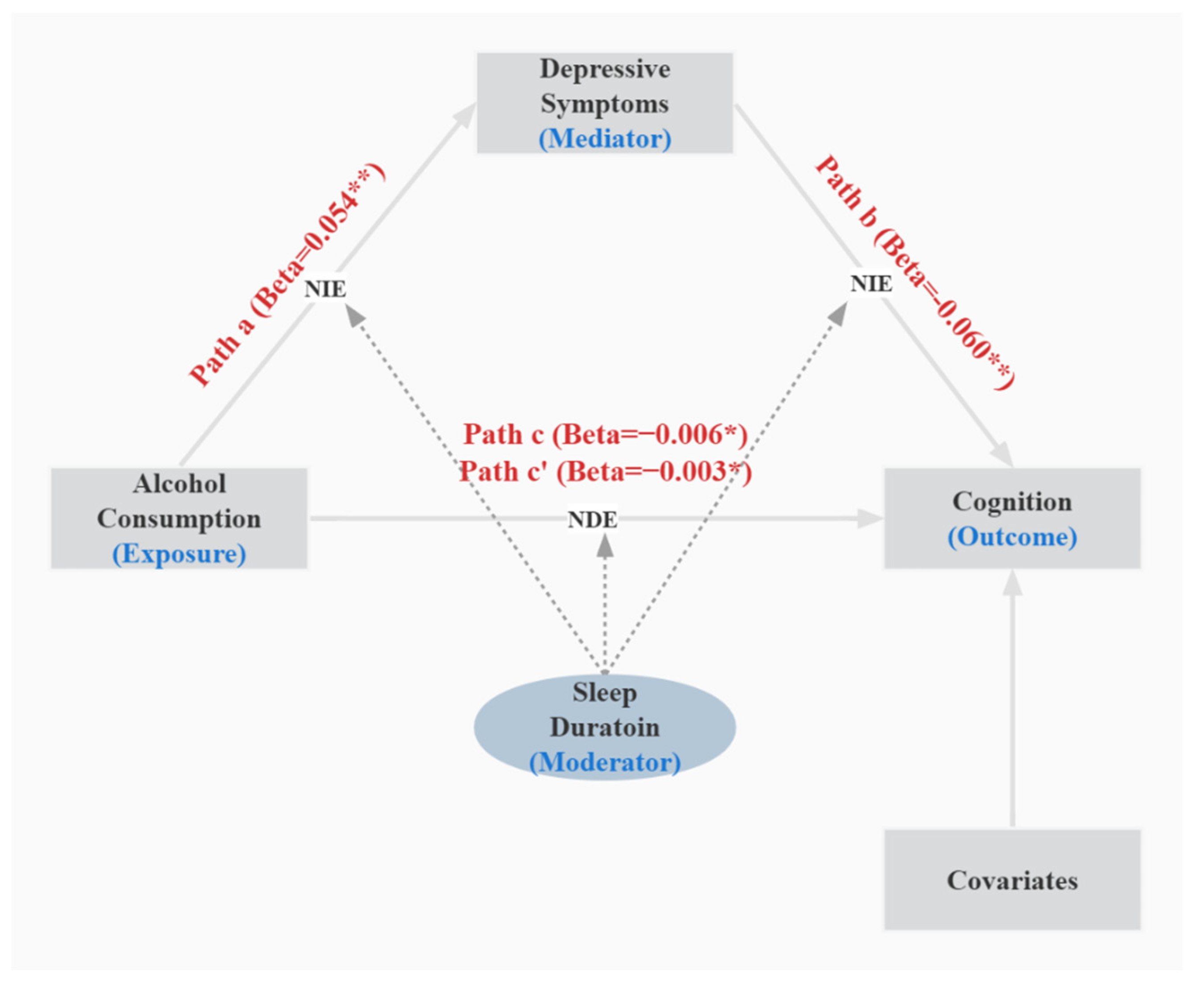
3.4. Adjusted Direct and Indirect Associations Model and Conditional Indirect Effect Model during Follow-Up
3.5. Sensitivity Analyses
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanford, A.M. Mild Cognitive Impairment. Clin. Geriatr. Med. 2017, 33, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Hugo, J.; Ganguli, M. Dementia and cognitive impairment: Epidemiology, diagnosis, and treatment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef]
- Rouanet, A.; Avila-Rieger, J.; Dugravot, A.; Lespinasse, J.; Stuckwisch, R.; Merrick, R.; Anderson, E.; Long, L.; Helmer, C.; Jacqmin-Gadda, H.; et al. How Selection Over Time Contributes to the Inconsistency of the Association Between Sex/Gender and Cognitive Decline Across Cognitive Aging Cohorts. Am. J. Epidemiol. 2022, 191, 441–452. [Google Scholar] [CrossRef]
- Wu, P.; Li, W.; Cai, X.; Yan, H.; Chen, M.; Alzheimer’s Disease Neuroimaging Initiative. Associations of cigarette smoking with memory decline and neurodegeneration among cognitively normal older individuals. Neurosci. Lett. 2020, 714, 134563. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Conner, K.R.; Caine, E.D.; Xiao, S.; Xu, L.; Gong, Y.; Zhang, R.; Phillips, M.R. Epidemiology of alcohol use in rural men in two provinces of China. J. Stud. Alcohol. Drugs 2011, 72, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Deng, J.; He, Y.; Deng, X.; Huang, J.; Huang, G.; Gao, X.; Zhang, W.H.; Lu, C. Alcohol use and alcohol-related problems among adolescents in China: A large-scale cross-sectional study. Medicine 2016, 95, e4533. [Google Scholar] [CrossRef]
- Mostofsky, E.; Chahal, H.S.; Mukamal, K.J.; Rimm, E.B.; Mittleman, M.A. Alcohol and Immediate Risk of Cardiovascular Events: A Systematic Review and Dose-Response Meta-Analysis. Circulation 2016, 133, 979–987. [Google Scholar] [CrossRef]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Rumgay, H.; Shield, K.; Charvat, H.; Ferrari, P.; Sornpaisarn, B.; Obot, I.; Islami, F.; Lemmens, V.E.P.P.; Rehm, J.; Soerjomataram, I. Global burden of cancer in 2020 attributable to alcohol consumption: A population-based study. Lancet Oncol. 2021, 22, 1071–1080. [Google Scholar] [CrossRef]
- Xu, W.; Wang, H.; Wan, Y.; Tan, C.; Li, J.; Tan, L.; Yu, J.T. Alcohol consumption and dementia risk: A dose-response meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 31–42. [Google Scholar] [CrossRef]
- Zanjani, F.; Downer, B.G.; Kruger, T.M.; Willis, S.L.; Schaie, K.W. Alcohol effects on cognitive change in middle-aged and older adults. Aging Ment. Health 2013, 17, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Topiwala, A.; Allan, C.L.; Valkanova, V.; Zsoldos, E.; Filippini, N.; Sexton, C.; Mahmood, A.; Fooks, P.; Singh-Manoux, A.; Mackay, C.E.; et al. Moderate alcohol consumption as risk factor for adverse brain outcomes and cognitive decline: Longitudinal cohort study. BMJ 2017, 357, j2353. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Dong, W.; Pan, X.F.; Feng, L.; Yuan, J.M.; Pan, A.; Koh, W.P. Relation of cigarette smoking and alcohol drinking in midlife with risk of cognitive impairment in late life: The Singapore Chinese Health Study. Age Ageing 2019, 48, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying neurocognitive disorders: The DSM-5 approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Akers, L.; Chou, L.S.; Pidgeon, D.; Voit, J.; Winters-Stone, K. Effectiveness of a Therapeutic Tai Ji Quan Intervention vs a Multimodal Exercise Intervention to Prevent Falls Among Older Adults at High Risk of Falling: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1301–1310. [Google Scholar] [CrossRef]
- Shi, L.; Chen, S.J.; Ma, M.Y.; Bao, Y.P.; Han, Y.; Wang, Y.M.; Shi, J.; Vitiello, M.V.; Lu, L. Sleep disturbances increase the risk of dementia: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 40, 4–16. [Google Scholar] [CrossRef]
- Ma, Y.; Liang, L.; Zheng, F.; Shi, L.; Zhong, B.; Xie, W. Association Between Sleep Duration and Cognitive Decline. JAMA Netw. Open 2020, 3, e2013573. [Google Scholar] [CrossRef]
- Yaffe, K.; Falvey, C.M.; Hoang, T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014, 13, 1017–1028. [Google Scholar] [CrossRef]
- Devore, E.E.; Grodstein, F.; Duffy, J.F.; Stampfer, M.J.; Czeisler, C.A.; Schernhammer, E.S. Sleep duration in midlife and later life in relation to cognition. J. Am. Geriatr. Soc. 2014, 62, 1073–1081. [Google Scholar] [CrossRef]
- Yaffe, K.; Nasrallah, I.; Hoang, T.D.; Lauderdale, D.S.; Knutson, K.L.; Carnethon, M.R.; Launer, L.J.; Lewis, C.E.; Sidney, S. Sleep Duration and White Matter Quality in Middle-Aged Adults. Sleep 2016, 39, 1743–1747. [Google Scholar] [CrossRef]
- Holmquist, S.; Nordstrom, A.; Nordstrom, P. The association of depression with subsequent dementia diagnosis: A Swedish nationwide cohort study from 1964 to 2016. PLoS Med. 2020, 17, e1003016. [Google Scholar] [CrossRef] [PubMed]
- Verdelho, A.; Madureira, S.; Moleiro, C.; Ferro, J.M.; O’Brien, J.T.; Poggesi, A.; Pantoni, L.; Fazekas, F.; Scheltens, P.; Waldemar, G.; et al. Depressive symptoms predict cognitive decline and dementia in older people independently of cerebral white matter changes: The LADIS study. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1250–1254. [Google Scholar] [CrossRef]
- Ganguli, M.; Snitz, B.; Vander Bilt, J.; Chang, C.C. How much do depressive symptoms affect cognition at the population level? The Monongahela-Youghiogheny Healthy Aging Team (MYHAT) study. Int. J. Geriatr. Psychiatry 2009, 24, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Lou, V.W.; Chi, I.; Kwan, C.W.; Leung, A.Y. Trajectories of social engagement and depressive symptoms among long-term care facility residents in Hong Kong. Age Ageing 2013, 42, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Moss, T.G.; Carney, C.E.; Haynes, P.; Harris, A.L. Is daily routine important for sleep? An investigation of social rhythms in a clinical insomnia population. Chronobiol. Int. 2015, 32, 92–102. [Google Scholar] [CrossRef]
- Naismith, S.L.; Rogers, N.L.; Lewis, S.J.; Terpening, Z.; Ip, T.; Diamond, K.; Norrie, L.; Hickie, I.B. Sleep disturbance relates to neuropsychological functioning in late-life depression. J. Affect. Disord. 2011, 132, 139–145. [Google Scholar] [CrossRef]
- Song, D.; Zhou, J.; Ma, J.; Chang, J.; Qiu, Y.; Zhuang, Z.; Xiao, H.; Zeng, L. Sleep disturbance mediates the relationship between depressive symptoms and cognitive function in older adults with mild cognitive impairment. Geriatr. Nurs. 2021, 42, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.; Fu, Y. The role of sleep disturbances in cognitive function and depressive symptoms among community-dwelling elderly with sleep complaints. Int. J. Geriatr. Psychiatry 2021, 36, 96–105. [Google Scholar] [CrossRef]
- Grant, B.F.; Goldstein, R.B.; Saha, T.D.; Chou, S.P.; Jung, J.; Zhang, H.; Pickering, R.P.; Ruan, W.J.; Smith, S.M.; Huang, B.; et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry 2015, 72, 757–766. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef]
- Xie, W.; Zheng, F.; Yan, L.; Zhong, B. Cognitive Decline Before and After Incident Coronary Events. J. Am. Coll. Cardiol. 2019, 73, 3041–3050. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Yan, L.; Yang, Z.; Zhong, B.; Xie, W. HbA1c, diabetes and cognitive decline: The English Longitudinal Study of Ageing. Diabetologia 2018, 61, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zhang, Z.; Li, L.; Liu, J. Early life exposure to China’s 1959–61 famine and midlife cognition. Int. J. Epidemiol. 2018, 47, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Chen, L.; Zhang, F.; Zhu, R.; Lin, X.; Meng, X.; Li, H.; Lei, X.; Zhao, Y. Trends in Alcohol Intake and the Association between Socio-Demographic Factors and Volume of Alcohol Intake amongst Adult Male Drinkers in China. Int. J. Environ. Res. Public Health 2019, 16, 573. [Google Scholar] [CrossRef]
- Hoang, T.D.; Byers, A.L.; Barnes, D.E.; Yaffe, K. Alcohol consumption patterns and cognitive impairment in older women. Am. J. Geriatr. Psychiatry 2014, 22, 1663–1667. [Google Scholar] [CrossRef]
- Li, C.; Miles, T.; Shen, L.; Shen, Y.; Liu, T.; Zhang, M.; Li, S.; Huang, C. Early-life exposure to severe famine and subsequent risk of depressive symptoms in late adulthood: The China Health and Retirement Longitudinal Study. Br. J. Psychiatry 2018, 213, 579–586. [Google Scholar] [CrossRef]
- Chen, H.; Mui, A.C. Factorial validity of the Center for Epidemiologic Studies Depression Scale short form in older population in China. Int. Psychogeriatr. 2014, 26, 49–57. [Google Scholar] [CrossRef]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef]
- Ge, S.; Wei, Z.; Liu, T.; Wang, J.; Li, H.; Feng, J.; Li, C. Alcohol Use and Cognitive Functioning Among Middle-Aged and Older Adults in China: Findings of the China Health and Retirement Longitudinal Study Baseline Survey. Alcohol. Clin. Exp. Res. 2018, 42, 2054–2060. [Google Scholar] [CrossRef]
- Li, J.; Cacchione, P.Z.; Hodgson, N.; Riegel, B.; Keenan, B.T.; Scharf, M.T.; Richards, K.C.; Gooneratne, N.S. Afternoon Napping and Cognition in Chinese Older Adults: Findings from the China Health and Retirement Longitudinal Study Baseline Assessment. J. Am. Geriatr. Soc. 2017, 65, 373–380. [Google Scholar] [CrossRef]
- Zhang, R.; Shen, L.; Miles, T.; Shen, Y.; Cordero, J.; Qi, Y.; Liang, L.; Li, C. Association of Low to Moderate Alcohol Drinking With Cognitive Functions From Middle to Older Age Among US Adults. JAMA Netw. Open 2020, 3, e207922. [Google Scholar] [CrossRef] [PubMed]
- Topiwala, A.; Ebmeier, K.P.; Maullin-Sapey, T.; Nichols, T.E. No safe level of alcohol consumption for brain health: Observational cohort study of 25,378 UK Biobank participants. medRxiv 2021. [Google Scholar] [CrossRef]
- Van Oostrom, S.H.; Nooyens, A.C.J.; van Boxtel, M.P.J.; Verschuren, W.M.M. Long sleep duration is associated with lower cognitive function among middle-age adults—The Doetinchem Cohort Study. Sleep Med. 2018, 41, 78–85. [Google Scholar] [CrossRef]
- Yang, R.; Xu, D.; Wang, H.; Xu, J. Longitudinal trajectories of physical functioning among Chinese older adults: The role of depressive symptoms, cognitive functioning and subjective memory. Age Ageing 2021, 50, 1682–1691. [Google Scholar] [CrossRef] [PubMed]
- Guan, Q.; Hu, X.; Ma, N.; He, H.; Duan, F.; Li, X.; Luo, Y.; Zhang, H. Sleep Quality, Depression, and Cognitive Function in Non-Demented Older Adults. J. Alzheimers Dis. 2020, 76, 1637–1650. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Biddinger, K.J.; Emdin, C.A.; Haas, M.E.; Wang, M.; Hindy, G.; Ellinor, P.T.; Kathiresan, S.; Khera, A.V.; Aragam, K.G. Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw. Open 2022, 5, e223849. [Google Scholar] [CrossRef] [PubMed]
- Ohara, T.; Honda, T.; Hata, J.; Yoshida, D.; Mukai, N.; Hirakawa, Y.; Shibata, M.; Kishimoto, H.; Kitazono, T.; Kanba, S.; et al. Association Between Daily Sleep Duration and Risk of Dementia and Mortality in a Japanese Community. J. Am. Geriatr. Soc. 2018, 66, 1911–1918. [Google Scholar] [CrossRef]
- Suh, S.W.; Han, J.W.; Lee, J.R.; Byun, S.; Kwon, S.J.; Oh, S.H.; Lee, K.H.; Han, G.; Hong, J.W.; Kwak, K.P.; et al. Sleep and cognitive decline: A prospective nondemented elderly cohort study. Ann. Neurol. 2018, 83, 472–482. [Google Scholar] [CrossRef]
- Hoiseth, G.; Hilberg, T.; Trydal, T.; Husa, A.; Vindenes, V.; Bogstrand, S.T. The alcohol marker phosphatidyl ethanol is closely related to AST, GGT, ferritin and HDL-C. Basic Clin. Pharmacol. Toxicol. 2022, 130, 182–190. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Alcohol Consumption (Times per Month) (n = 14,482) | Depressive Symptoms (n = 12,732) | Sleep Duration (Hours per Night) (n = 14,122) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nondrinkers | ≤1 | >1 | p Value | Nondepressed | Depressed | p Value | ≤6 h | 7–8 h | ≥9 h | p Value | ||
| N (%) | 15,414 | 9686 (66.9) | 1138 (7.8) | 3658 (25.3) | 8522 (66.9) | 4210 (33.1) | 7012 (49.6) | 5939 (42.1) | 1171 (8.3) | |||
| Age (years), mean (SD) | 59.02 (10.14) | 58.93 (10.10) | 59.14 (9.92) | 59.13 (10.24) | 0.532 | 58.95 (10.12) | 59.02 (10.09) | 0.691 | 59.05 (10.14) | 59.09 (10.20) | 58.88 (9.75) | 0.813 |
| Gender (women), n (%) | 8036 (52.1) | 5027 (51.9) | 590 (51.8) | 1927 (52.7) | 0.698 | 4396 (51.6) | 2218 (52.7) | 0.237 | 3669 (52.4) | 3042 (51.2) | 628 (53.7) | 0.218 |
| Education level, n (%) | 0.122 | 0.910 | 0.033 | |||||||||
| No formal education or illiterate | 4195 (27.3) | 2570 (26.6) | 311 (27.4) | 1065 (29.2) | 2287 (26.9) | 1165 (27.8) | 1909 (27.3) | 1562 (26.4) | 360 (30.9) | |||
| Did not finish primary school | 2676 (17.4) | 1675 (17.4) | 207 (18.2) | 636 (17.5) | 1466 (17.3) | 716 (17.1) | 1243 (17.8) | 995 (16.8) | 204 (17.5) | |||
| Finished middle school | 8062 (52.5) | 5129 (53.1) | 587 (51.7) | 1856 (50.9) | 4497 (53.0) | 2197 (52.3) | 3642 (52.1) | 3192 (53.9) | 576 (49.4) | |||
| Higher and further education | 368 (2.4) | 241 (2.5) | 27 (2.4) | 72 (2.0) | 209 (2.5) | 102 (2.4) | 173 (2.5) | 146 (2.5) | 20 (1.7) | |||
| Others | 63 (0.4) | 39 (0.4) | 4 (0.4) | 15 (0.4) | 33 (0.4) | 17 (0.4) | 24 (0.3) | 25 (0.4) | 5 (0.4) | |||
| Living with a partner, n (%) | 12,342 (80.1) | 7784 (80.5) | 906 (79.6) | 2914 (79.8) | 0.016 | 6859 (80.6) | 3362 (80.0) | 0.516 | 5635 (80.5) | 4746 (80.1) | 928 (79.5) | 0.598 |
| Cigarette consumption, n (%) | 6052 (39.3) | 3778 (39.1) | 456 (40.2) | 1470 (40.3) | 0.397 | 3435 (40.4) | 1601 (38.1) | 0.016 | 2690(38.4) | 2351 (39.6) | 428 (36.5) | 0.098 |
| Blood pressure, mean (SD), mm Hg | ||||||||||||
| Systolic | 130.70 (21.67) | 130.9 (21.83) | 131.80 (22.72) | 130.21 (21.24) | 0.106 | 130.50 (21.83) | 131.15 (21.47) | 0.143 | 130.46 (21.56) | 130.99 (21.84) | 130.96 (21.75) | 0.413 |
| Diastolic | 75.95 (12.22) | 76.07 (12.24) | 76.34 (13.25) | 75.67 (11.98) | 0.194 | 75.82 (12.23) | 76.18 (12.24) | 0.154 | 75.91 (12.21) | 75.99 (12.31) | 75.91 (12.06) | 0.935 |
| Body mass index (kg/m2) | 23.45 (3.95) | 23.41 (3.95) | 23.46 (3.68) | 23.57 (4.08) | 0.185 | 23.45 (4.05) | 23.43 (3.85) | 0.730 | 23.49 (4.02) | 23.40 (3.87) | 23.44 (4.03) | 0.516 |
| Cognitive function scores (z-scores, mean (SD)) | ||||||||||||
| Memory score | −0.00 (1.00) | −0.03 (1.01) | 0.16 (0.98) | 0.03 (0.97) | <0.001 | 0.12 (1.01) | −0.18 (0.94) | <0.001 | −0.02 (1.00) | 0.03 (1.00) | −0.02 (1.00) | 0.038 |
| Orientation score | 0.00 (1.00) | −0.04 (1.02) | 0.10 (0.95) | 0.08 (0.95) | <0.001 | 0.12 (0.95) | −0.19 (1.06) | <0.001 | −0.01 (1.01) | 0.04 (0.98) | −0.05 (1.02) | 0.007 |
| Executive score | −0.00 (1.03) | −0.08 (1.02) | 0.12 (1.02) | 0.17 (1.01) | <0.001 | 0.27 (0.94) | −0.09 (0.97) | <0.001 | −0.02 (1.03) | 0.02 (1.02) | −0.07 (1.04) | 0.009 |
| Global z scores | 0.00 (1.00) | −0.07 (1.02) | 0.19 (0.95) | 0.12 (0.94) | <0.001 | 0.15 (0.97) | −0.26 (0.97) | <0.001 | −0.002 (1.00) | 0.03 (0.99) | −0.03 (1.00) | 0.017 |
| Hypertension n (%) | 3712 (24.1) | 2338 (24.3) | 285 (25.2) | 870 (24.0) | 0.725 | 2101 (24.8) | 984 (23.6) | 0.126 | 1798 (25.8) | 1341 (22.7) | 286 (24.5) | <0.001 |
| Diabetes, n (%) | 847 (5.5) | 545 (5.7) | 73 (6.5) | 181 (5.0) | 0.112 | 470 (5.6) | 226 (5.4) | 0.711 | 422 (6.1) | 319 (5.4) | 50 (4.3) | 0.030 |
| Dyslipidemia, n (%) | 1382 (9.0) | 879 (9.3) | 110 (9.8) | 323 (9.0) | 0.712 | 784 (9.4) | 356 (8.6) | 0.156 | 673 (9.8) | 533 (9.1) | 90 (7.8) | 0.075 |
| Coronary heart disease, n (%) | 1800 (11.7) | 1128 (11.7) | 436 (12.0) | 130 (11.6) | 0.885 | 990 (11.7) | 500 (12.0) | 0.650 | 972 (14.0) | 608 (10.3) | 112 (9.6) | <0.001 |
| Stroke, n (%) | 291 (1.9) | 187 (1.9) | 15 (1.3) | 74 (2.0) | 0.305 | 164 (1.9) | 79 (1.9) | 0.885 | 146 (2.1) | 92 (1.6) | 24 (2.1) | 0.071 |
| Chronic lung disease, n (%) | 1489 (9.7) | 912 (9.5) | 122 (10.8) | 359 (9.9) | 0.342 | 800 (9.4) | 439 (10.5) | 0.063 | 822 (11.8) | 464 (7.8) | 103 (8.8) | <0.001 |
| Asthma, n (%) | 515 (3.3) | 320 (3.3) | 38 (3.4) | 126 (3.5) | 0.917 | 294 (3.5) | 140 (3.3) | 0.731 | 286 (4.1) | 150 (2.5) | 40 (3.4) | <0.001 |
| β, 95% CI | ||||||||
|---|---|---|---|---|---|---|---|---|
| Memory Score | Orientation Score | Executive Score | Global Cognition z Score | |||||
| Model 1 a (n = 10,335) | Model 2 b (n = 8215) | Model 1 a (n = 10,782) | Model 2 b (n = 8615) | Model 1 a (n = 11,580) | Model 2 b (n = 9257) | Model 1 a (n = 9710) | Model 2 b (n = 7715) | |
| Alcohol Consumption (times per month) | ||||||||
| Nondrinkers | REF | REF | REF | REF | REF | REF | REF | REF |
| ≤1 | 0.173 | 0.186 | 0.036 | 0.087 | 0.268 | −0.070 | 0.204 | 0.193 |
| −0.006 to 0.352 | −0.192 to 0.564 | −0.108 to 0.180 | −0.261 to 0.435 | 0.135 to 0.400 | −0.393 to 0.253 | 0.055 to 0.352 | −0.176 to 0.561 | |
| p value | 0.058 | 0.334 | 0.623 | 0.624 | <0.001 | 0.671 | 0.007 | 0.306 |
| >1 | 0.038 | 0.221 | 0.123 | 0.079 | 0.261 | 0.303 | 0.123 | 0.334 |
| −0.081 to 0.158 | 0.006 to 0.437 | 0.029 to 0.217 | −0.127 to 0.286 | 0.175 to 0.347 | 0.110 to 0.496 | 0.026 to 0.220 | 0.120 to 0.548 | |
| p value | 0.532 | 0.044 | 0.010 | 0.452 | <0.001 | 0.002 | 0.013 | 0.002 |
| Depressive Symptoms | ||||||||
| Nondepressed | REF | REF | REF | REF | REF | REF | REF | REF |
| Depressed | −0.368 | −0.411 | −0.223 | −0.367 | −0.337 | −0.464 | −0.396 | −0.496 |
| −0.496 to −0.239 | −0.604 to −0.219 | −0.319 to −0.128 | −0.553 to −0.182 | −0.426 to −0.248 | −0.632 to−0.296 | −0.494 to −0.298 | −0.694 to −0.297 | |
| p value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Sleep Duration (hours per night) | ||||||||
| ≤6 h | −0.148 | 0.006 | −0.053 | −0.084 | −0.082 | −0.055 | −0.105 | −0.025 |
| −0.240 to −0.056 | −0.166 to 0.177 | −0.133 to 0.028 | −0.252 to 0.085 | −0.157 to −0.006 | −0.210 to 0.101 | −0.187 to −0.023 | −0.198 to 0.147 | |
| p value | 0.002 | 0.947 | 0.199 | 0.331 | 0.033 | 0.491 | 0.012 | 0.772 |
| 7–8 h | REF | REF | REF | REF | REF | REF | REF | REF |
| ≥9 h | 0.047 | 0.128 | −0.074 | −0.070 | 0.003 | 0.218 | 0.079 | 0.158 |
| −0.124 to 0.217 | −0.218 to 0.474 | −0.222 to 0.074 | −0.389 to 0.249 | −0.135 to 0.142 | −0.082 to 0.518 | −0.075 to 0.232 | −0.185 to 0.501 | |
| p value | 0.592 | 0.468 | 0.326 | 0.667 | 0.962 | 0.154 | 0.315 | 0.367 |
| Age (years) | 0.000 | −0.001 | 0.000 | −0.001 | 0.001 | 0.001 | 0.000 | −0.001 |
| −0.002 to 0.002 | −0.004 to 0.001 | −0.002 to 0.002 | −0.03 to 0.001 | −0.001 to 0.003 | −0.001 to 0.003 | −0.002 to 0.002 | −0.003 to 0.002 | |
| p value | 0.939 | 0.291 | 0.839 | 0.448 | 0.219 | 0.457 | 0.747 | 0.654 |
| Gender | 0.014 | 0.011 | 0.023 | 0.018 | 0.010 | −0.010 | 0.012 | 0.006 |
| −0.026 to 0.054 | −0.035 to 0.057 | −0.016 to 0.063 | −0.026 to 0.063 | −0.027 to 0.046 | −0.051 to 0.031 | −0.029 to 0.053 | −0.040 to 0.051 | |
| p value | 0.497 | 0.634 | 0.245 | 0.417 | 0.600 | 0.626 | 0.558 | 0.811 |
| Education Level | 0.011 | 0.007 | 0.016 | 0.012 | 0.016 | 0.011 | 0.018 | 0.016 |
| 0.000 to 0.021 | −0.005 to 0.019 | 0.006 to 0.026 | 0.001 to 0.024 | 0.007 to 0.025 | 0.001 to 0.022 | 0.007 to 0.028 | 0.004 to 0.028 | |
| p value | 0.042 | 0.258 | 0.002 | 0.037 | 0.001 | 0.035 | 0.001 | 0.009 |
| Marriage | −0.002 | 0.001 | −0.008 | −0.002 | 0.002 | 0.007 | 0.002 | 0.007 |
| −0.017 to 0.014 | −0.016 to 0.018 | −0.023 to 0.007 | −0.019 to 0.014 | −0.011 to 0.016 | −0.008 to 0.022 | −0.013 to 0.017 | −0.011 to 0.024 | |
| p value | 0.838 | 0.906 | 0.302 | 0.790 | 0.736 | 0.356 | 0.794 | 0.452 |
| Blood Pressure | ||||||||
| Systolic | NA | 0.001 | NA | 0.001 | NA | 0.000 | NA | 0.001 |
| −0.001 to 0.002 | 0.000 to 0.002 | −0.001 to 0.002 | −0.001 to 0.002 | |||||
| p value | 0.463 | 0.110 | 0.512 | 0.315 | ||||
| Diastolic | NA | −0.001 | NA | −0.003 | NA | −0.003 | NA | −0.002 |
| −0.004 to 0.002 | −0.005 to −0.001 | −0.005 to 0.000 | −0.004 to 0.001 | |||||
| p value | 0.416 | 0.018 | 0.022 | 0.226 | ||||
| Body Mass Index (kg/m2) | NA | 0.000 | NA | −0.001 | NA | −0.002 | NA | −0.002 |
| −0.006 to 0.005 | −0.006 to 0.004 | −0.007 to 0.002 | −0.008 to 0.003 | |||||
| p value | 0.903 | 0.733 | 0.325 | 0.397 | ||||
| Cigarette Consumption | NA | 0.025 | NA | 0.043 | NA | 0.025 | NA | 0.048 |
| −0.019 to 0.069 | 0.000 to 0.086 | −0.015 to 0.064 | 0.004 to 0.092 | |||||
| p value | 0.267 | 0.048 | 0.216 | 0.034 | ||||
| Hypertension | NA | 0.048 | NA | −0.006 | NA | −0.016 | NA | 0.014 |
| −0.005 to 0.101 | −0.057 to 0.046 | −0.063 to 0.032 | −0.040 to 0.067 | |||||
| p value | 0.076 | 0.829 | 0.515 | 0.617 | ||||
| Diabetes | NA | −0.061 | NA | −0.026 | NA | −0.013 | NA | −0.074 |
| −0.160 to 0.039 | −0.122 to 0.071 | −0.101 to 0.076 | −0.175 to 0.026 | |||||
| p value | 0.233 | 0.602 | 0.780 | 0.145 | ||||
| Dyslipidemia | NA | 0.044 | NA | 0.031 | NA | −0.008 | NA | 0.050 |
| −0.036 to 0.125 | −0.047 to 0.110 | −0.080 to 0.064 | −0.030 to 0.131 | |||||
| p value | 0.278 | 0.434 | 0.834 | 0.222 | ||||
| Coronary Heart Disease | NA | −0.059 | NA | 0.034 | NA | 0.004 | NA | −0.054 |
| −0.127 to 0.010 | −0.033 to 0.102 | −0.058 to 0.065 | −0.124 to 0.015 | |||||
| p value | 0.093 | 0.315 | 0.904 | 0.124 | ||||
| Stroke | NA | −0.087 | NA | 0.049 | NA | 0.028 | NA | −0.003 |
| −0.245 to 0.072 | −0.106 to 0.204 | −0.114 to 0.170 | −0.163 to 0.157 | |||||
| p value | 0.284 | 0.535 | 0.704 | 0.971 | ||||
| Chronic Lung Disease | NA | 0.003 | NA | −0.006 | NA | 0.031 | NA | 0.002 |
| −0.072 to 0.078 | −0.079 to 0.068 | −0.036 to 0.098 | −0.074 to 0.078 | |||||
| p value | 0.943 | 0.879 | 0.370 | 0.951 | ||||
| Asthma | NA | 0.156 | NA | 0.051 | NA | 0.029 | NA | 0.095 |
| 0.032 to 0.279 | −0.068 to 0.170 | −0.080 to 0.139 | −0.029 to 0.219 | |||||
| p value | 0.013 | 0.403 | 0.601 | 0.133 | ||||
| β (95% CI) a | p Value | |
|---|---|---|
| Sleep Duration (hours per night) | ||
| ≤6 h | −0.056 (NA) | <0.001 |
| 7–8 h | REF | REF |
| ≥9 h | 0.225 (NA) | <0.001 |
| Depressive Symptoms | ||
| Nondepressed | REF | REF |
| Depressed | −0.271 (−0.411 to −0.130) | <0.001 |
| Alcohol Consumption (times per month) | ||
| No | REF | REF |
| ≤1 | 0.072 (−0.184 to 0.327) | 0.582 |
| >1 | 0.156 (0.007 to 0.305) | <0.05 |
| Depressive Symptoms * Alcohol Consumption | 0.539 | |
| Sleep Duration * Alcohol Consumption | 0.305 | |
| Depressive Symptoms * Sleep Duration | 0.324 | |
| Depressive Symptoms * Alcohol Consumption * Sleep Duration | <0.05 | |
| Age (years) | −0.001 (−0.003 to 0.000) | 0.114 |
| Gender | 0.034 (0.002 to 0.067) | <0.05 |
| Education Level | 0.013 (0.005 to 0.022) | <0.05 |
| Marriage | 0.007 (−0.005 to 0.020) | 0.252 |
| Blood Pressure | ||
| Systolic | 0.001 (0.000 to 0.002) | 0.164 |
| Diastolic | 0.000 (−0.002 to 0.001) | 0.637 |
| Body Mass Index (kg/m2) | −0.001 (−0.004 to 0.003) | 0.793 |
| Cigarette Consumption | 0.036 (0.004 to 0.068) | <0.05 |
| Hypertension | 0.019 (−0.019 to 0.057) | 0.327 |
| Diabetes | −0.060 (−0.132 to 0.011) | 0.097 |
| Dyslipidemia | −0.017 (−0.075 to 0.042) | 0.577 |
| Coronary Heart Disease | −0.008 (−0.057 to 0.042) | 0.767 |
| Stroke | NA (−0.116 to 0.116) | 1.000 |
| Chronic Lung Disease | 0.026 (−0.028 to 0.079) | 0.349 |
| Asthma | 0.026(−0.061 to 0.113) | 0.557 |
| Model 1 a (n= 11,416) | Model 2 b (n = 11,344) | Model 3 c (n = 9000) | ||||
|---|---|---|---|---|---|---|
| β(95% CI) | p Value | β(95% CI) | p Value | β(95% CI) | p Value | |
| Alcohol Consumption | ||||||
| Total Association | −0.008 (−0.030 to 0.013) | 0.447 | −0.009 (−0.031 to 0.012) | 0.404 | −0.006 (−0.031 to 0.018) | 0.600 |
| Direct Association | −0.005 (−0.027 to 0.016) | 0.635 | −0.006 (−0.027 to 0.016) | 0.585 | −0.003 (−0.027 to 0.021) | 0.793 |
| Indirect Association via Depressive Symptoms | −0.003 (−0.005 to −0.001) | 0.001 | −0.003 (−0.005 to −0.001) | 0.001 | −0.003 (−0.005 to −0.001) | 0.003 |
| Proportion Mediated, % | 100 | 100 | 100 | |||
| Model 1 a (n = 10,460) | Model 2 b (n = 10,396) | Model 3 c (n = 8300) | |||||
|---|---|---|---|---|---|---|---|
| Effect | 95% CI | Effect | 95% CI | Effect | 95% CI | ||
| Depressive Symptoms | Low level (−1 SD) | −0.004 | −0.008 to −0.001 | −0.004 | −0.008 to −0.001 | −0.004 | −0.008 to −0.001 |
| Mean level | −0.004 | −0.005 to −0.001 | −0.003 | −0.006 to −0.001 | −0.003 | −0.005 to −0.001 | |
| High level (+1 SD) | −0.003 | −0.005 to 0.001 | −0.002 | −0.006 to 0.000 | −0.002 | −0.005 to 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guan, T.; Zhang, C.; Zou, X.; Chen, C.; Zhou, L.; Wu, X.; Hao, J. The Influence of Alcohol Consumption, Depressive Symptoms and Sleep Duration on Cognition: Results from the China Health and Retirement Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 12574. https://doi.org/10.3390/ijerph191912574
Guan T, Zhang C, Zou X, Chen C, Zhou L, Wu X, Hao J. The Influence of Alcohol Consumption, Depressive Symptoms and Sleep Duration on Cognition: Results from the China Health and Retirement Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12574. https://doi.org/10.3390/ijerph191912574
Chicago/Turabian StyleGuan, Tianyue, Chao Zhang, Xuanmin Zou, Chen Chen, Li Zhou, Xiaochang Wu, and Jiahu Hao. 2022. "The Influence of Alcohol Consumption, Depressive Symptoms and Sleep Duration on Cognition: Results from the China Health and Retirement Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 19: 12574. https://doi.org/10.3390/ijerph191912574
APA StyleGuan, T., Zhang, C., Zou, X., Chen, C., Zhou, L., Wu, X., & Hao, J. (2022). The Influence of Alcohol Consumption, Depressive Symptoms and Sleep Duration on Cognition: Results from the China Health and Retirement Longitudinal Study. International Journal of Environmental Research and Public Health, 19(19), 12574. https://doi.org/10.3390/ijerph191912574