


Increased Risk of Chronic Obstructive Pulmonary Disease in Patients with Hyperlipidemia: A Nationwide Population-Based Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Hill, M.F.; Bordoni, B. Hyperlipidemia; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- The Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2021 GOLD Reports—Global Initiative for Chronic Obstructive Lung Disease. 2021. Available online: https://goldcopd.org/2021-gold-reports/ (accessed on 11 November 2021).
- André, S.; Conde, B.; Fragoso, E.; Boléo-Tomé, J.P.; Areias, V.; Cardoso, J. COPD and cardiovascular disease. Pulmonology 2019, 25, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease among adults—United States, 2011. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 938–943. [Google Scholar]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global burden of disease study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Pi, X.; Xie, L.; Patterson, C. Emerging roles of vascular endothelium in metabolic homeostasis. Circ. Res. 2018, 123, 477–494. [Google Scholar] [CrossRef]
- Zafirova-Ivanovska, B.; Stojkovikj, J.; Dokikj, D.; Anastasova, S.; Debresliovska, A.; Zejnel, S.; Stojkovikj, D. The level of cholesterol in COPD patients with severe and very severe stage of the disease. Open Access Maced. J. Med. Sci. 2016, 4, 277–282. [Google Scholar] [CrossRef]
- Mitra, R.; Datta, S.; Pal, M.; Ghosh, K.; Paul, D.; Pal, K. Lipid profile status in chronic obstructive pulmonary disease and association with interleukin 8. Br. J. Med. Med. Res. 2015, 9, 1–7. [Google Scholar] [CrossRef]
- Polverino, F.; Celli, B.R.; Owen, C.A. COPD as an endothelial disorder: Endothelial injury linking lesions in the lungs and other organs? (2017 Grover Conference Series). Pulm. Circ. 2018, 8, 2045894018758528. [Google Scholar] [CrossRef]
- Cheng, T.M. Taiwan’s new national health insurance program: Genesis and experience so far. Health Aff. 2003, 22, 61–76. [Google Scholar] [CrossRef]
- Chen, Y.A.; Lin, Y.J.; Lin, C.L.; Lin, H.J.; Wu, H.S.; Hsu, H.Y.; Sun, Y.C.; Wu, H.Y.; Lai, C.H.; Kao, C.H. Simvastatin therapy for drug repositioning to reduce the risk of prostate cancer mortality in patients with hyperlipidemia. Front. Pharmacol. 2018, 9, 225. [Google Scholar] [CrossRef]
- Hsu, T.W.; Lee, P.S.; Nfor, O.N.; Lee, C.L.; Chen, P.H.; Tantoh, D.M.; Lin, L.Y.; Chou, M.C.; Lee, Y.C.; Liaw, Y.P. The interaction between sex and hyperlipidemia on gout risk is modulated by HLA-B polymorphic variants in adult Taiwanese. Genes 2019, 10, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsing, A.W.; Ioannidis, J.P. Nationwide population science: Lessons from the Taiwan national health insurance research database. JAMA Intern. Med. 2015, 175, 1527–1529. [Google Scholar] [CrossRef] [PubMed]
- Gunay, S.; Sariaydin, M.; Acay, A. New predictor of atherosclerosis in subjects with COPD: Atherogenic indices. Respir. Care. 2016, 61, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Can, U.; Yerlikaya, F.H.; Yosunkaya, S. Role of oxidative stress and serum lipid levels in stable chronic obstructive pulmonary disease. J. Chin. Med. Assoc. 2015, 78, 702–708. [Google Scholar] [CrossRef]
- Sabbatinelli, J.; Vignini, A.; Salvolini, E.; Nanetti, L.; Mazzanti, L.; Anna Rabini, R. Platelet-derived NO in subjects affected by type 2 diabetes with and without complications: Is there any relationship with their offspring? Exp. Clin. Endocrinol. Diabetes 2017, 125, 290–296. [Google Scholar] [CrossRef]
- Förstermann, U.; Münzel, T. Endothelial nitric oxide synthase in vascular disease: From marvel to menace. Circulation 2006, 113, 1708–1714. [Google Scholar] [CrossRef] [PubMed]
- Warnholtz, A.; Mollnau, H.; Oelze, M.; Wendt, M.; Münzel, T. Antioxidants and endothelial dysfunction in hyperlipidemia. Curr. Hypertens. Rep. 2001, 3, 53–60. [Google Scholar] [CrossRef]
- Sabbatinelli, J.; Orlando, P.; Galeazzi, R.; Silvestri, S.; Cirilli, I.; Marcheggiani, F.; Dludla, P.V.; Giuliani, A.; Bonfigli, A.R.; Mazzanti, L.; et al. Ubiquinol ameliorates endothelial dysfunction in subjects with mild-to-moderate dyslipidemia: A randomized clinical trial. Nutrients 2020, 12, 1098. [Google Scholar] [CrossRef]
- Kim, J.A.; Montagnani, M.; Chandrasekran, S.; Quon, M.J. Role of lipotoxicity in endothelial dysfunction. Heart Fail. Clin. 2012, 8, 589–607. [Google Scholar] [CrossRef]
- Sitia, S.; Tomasoni, L.; Atzeni, F.; Ambrosio, G.; Cordiano, C.; Catapano, A.; Tramontana, S.; Perticone, F.; Naccarato, P.; Camici, P.; et al. From endothelial dysfunction to atherosclerosis. Autoimmun. Rev. 2010, 9, 830–834. [Google Scholar] [CrossRef]
- Kim, J.A.; Montagnani, M.; Koh, K.K.; Quon, M.J. Reciprocal relationships between insulin resistance and endothelial dysfunction: Molecular and pathophysiological mechanisms. Circulation 2006, 113, 1888–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, A.H.; Scherer, P.E. Adipose tissue, inflammation, and cardiovascular disease. Circ. Res. 2005, 96, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, H.O.; Chaker, H.; Leaming, R.; Johnson, A.; Brechtel, G.; Baron, A.D. Obesity/insulin resistance is associated with endothelial dysfunction. Implications for the syndrome of insulin resistance. J. Clin. Invest. 1996, 97, 2601–2610. [Google Scholar] [CrossRef]
- Dinh-Xuan, A.T.; Higenbottam, T.W.; Clelland, C.A.; Pepke-Zaba, J.; Cremona, G.; Butt, A.Y.; Large, S.R.; Wells, F.C.; Wallwork, J. Impairment of endothelium-dependent pulmonary-artery relaxation in chronic obstructive lung disease. N. Engl. J. Med. 1991, 324, 1539–1547. [Google Scholar] [CrossRef]
- Peinado, V.I.; Barbera, J.A.; Ramirez, J.; Gómez, F.P.; Roca, J.; Jover, L.; Gimferrer, J.M.; Rodriguez-Roisin, R. Endothelial dysfunction in pulmonary arteries of patients with mild COPD. Am. J. Physiol. 1998, 274, L908–L913. [Google Scholar] [CrossRef]
- Barr, R.G.; Mesia-Vela, S.; Austin, J.H.; Basner, R.C.; Keller, B.M.; Reeves, A.P.; Shimbo, D.; Stevenson, L. Impaired flow-mediated dilation is associated with low pulmonary function and emphysema in ex-smokers: The Emphysema and Cancer Action Project (EMCAP) Study. Am. J. Respir. Crit. Care Med. 2007, 176, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Moro, L.; Pedone, C.; Scarlata, S.; Malafarina, V.; Fimognari, F.; Antonelli-Incalzi, R. Endothelial dysfunction in chronic obstructive pulmonary disease. Angiology 2008, 59, 357–364. [Google Scholar] [CrossRef]
- Eickhoff, P.; Valipour, A.; Kiss, D.; Schreder, M.; Cekici, L.; Geyer, K.; Kohansal, R.; Burghuber, O.C. Determinants of systemic vascular function in patients with stable chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2008, 178, 1211–1218. [Google Scholar] [CrossRef]
- Vukic Dugac, A.; Ruzic, A.; Samarzija, M.; Badovinac, S.; Kehler, T.; Jakopovic, M. Persistent endothelial dysfunction turns the frequent exacerbator COPD from respiratory disorder into a progressive pulmonary and systemic vascular disease. Med. Hypotheses. 2015, 84, 155–158. [Google Scholar] [CrossRef]
- Casanova, C.; de Torres, J.P.; Navarro, J.; Aguirre-Jaíme, A.; Toledo, P.; Cordoba, E.; Baz, R.; Celli, B.R. Microalbuminuria and hypoxemia in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care. Med. 2010, 182, 1004–1010. [Google Scholar] [CrossRef]
- Polverino, F.; Laucho-Contreras, M.E.; Petersen, H.; Bijol, V.; Sholl, L.M.; Choi, M.E.; Divo, M.; Pinto-Plata, V.; Chetta, A.; Tesfaigzi, Y.; et al. A pilot study linking endothelial injury in lungs and kidneys in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2017, 195, 1464–1476. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A., Jr.; García-Cardeña, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [PubMed]
- Drexler, H.; Hornig, B. Endothelial dysfunction in human disease. J. Mol. Cell Cardiol. 1999, 31, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Quyyumi, A.A.; Patel, R.S. Endothelial dysfunction and hypertension: Cause or effect? Hypertension 2010, 55, 1092–1094. [Google Scholar] [CrossRef]
- Sander, M.; Chavoshan, B.; Victor, R.G. A large blood pressure-raising effect of nitric oxide synthase inhibition in humans. Hypertension 1999, 33, 937–942. [Google Scholar] [CrossRef]
- Juonala, M.; Viikari, J.S.; Rönnemaa, T.; Helenius, H.; Taittonen, L.; Raitakari, O.T. Elevated blood pressure in adolescent boys predicts endothelial dysfunction: The cardiovascular risk in young Finns study. Hypertension 2006, 48, 424–430. [Google Scholar] [CrossRef]
- Gkaliagkousi, E.; Douma, S.; Zamboulis, C.; Ferro, A. Nitric oxide dysfunction in vascular endothelium and platelets: Role in essential hypertension. J. Hypertens. 2009, 27, 2310–2320. [Google Scholar] [CrossRef]
- Dohi, Y.; Thiel, M.A.; Bühler, F.R.; Lüscher, T.F. Activation of endothelial L-arginine pathway in resistance arteries. Effect of age and hypertension. Hypertension 1990, 16, 170–179. [Google Scholar] [CrossRef]
- Hermann, M.; Flammer, A.; Lüscher, T.F. Nitric oxide in hypertension. J. Clin. Hypertens. 2006, 8, 17–29. [Google Scholar] [CrossRef]
- Higashi, Y.; Kihara, Y.; Noma, K. Endothelial dysfunction and hypertension in aging. Hypertens. Res. 2012, 35, 1039–1047. [Google Scholar] [CrossRef]
- Zuchi, C.; Tritto, I.; Carluccio, E.; Mattei, C.; Cattadori, G.; Ambrosio, G. Role of endothelial dysfunction in heart failure. Heart Fail Rev. 2020, 25, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, M.W.; Goodfellow, J.; Jones, C.J.; Luddington, L.A.; Lewis, M.J.; Henderson, A.H. Endothelial control of arterial distensibility is impaired in chronic heart failure. Circulation 1995, 92, 3212–3219. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.D.; Hryniewicz, K.; Hriljac, I.; Balidemaj, K.; Dimayuga, C.; Hudaihed, A.; Yasskiy, A. Vascular endothelial dysfunction and mortality risk in patients with chronic heart failure. Circulation 2005, 111, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Kubo, S.H.; Rector, T.S.; Bank, A.J.; Williams, R.E.; Heifetz, S.M. Endothelium-dependent vasodilation is attenuated in patients with heart failure. Circulation 1991, 84, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Hadi, H.A.; Carr, C.S.; Al Suwaidi, J. Endothelial dysfunction: Cardiovascular risk factors, therapy, and outcome. Vasc. Health Risk Manag. 2005, 1, 183–198. [Google Scholar] [PubMed]
- Herrera, M.D.; Mingorance, C.; Rodríguez-Rodríguez, R.; Alvarez de Sotomayor, M. Endothelial dysfunction and aging: An update. Ageing Res. Rev. 2010, 9, 142–152. [Google Scholar] [CrossRef]
- Meyrelles, S.S.; Peotta, V.A.; Pereira, T.M.; Vasquez, E.C. Endothelial dysfunction in the apolipoprotein E-deficient mouse: Insights into the influence of diet, gender and aging. Lipids Health Dis. 2011, 10, 211. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Spiegelhalter, D.J.; Georgakopoulos, D.; Robinson, J.; Deanfield, J.E. Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women. J. Am. Coll. Cardiol. 1994, 24, 471–476. [Google Scholar] [CrossRef]
- Moreau, K.L.; Hildreth, K.L.; Meditz, A.L.; Deane, K.D.; Kohrt, W.M. Endothelial function is impaired across the stages of the menopause transition in healthy women. J. Clin. Endocrinol. Metab. 2012, 97, 4692–4700. [Google Scholar] [CrossRef]
- Stanhewicz, A.E.; Wenner, M.M.; Stachenfeld, N.S. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am. J. Physiol. Heart. Circ. Physiol. 2018, 315, H1569–H1588. [Google Scholar] [CrossRef]
- Mannino, D.M.; Buist, A.S. Global burden of COPD: Risk factors, prevalence, and future trends. Lancet 2007, 370, 765–773. [Google Scholar] [CrossRef]
- Løkke, A.; Lange, P.; Scharling, H.; Fabricius, P.; Vestbo, J. Developing COPD: A 25 year follow up study of the general population. Thorax 2006, 61, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xu, J.; Yang, L.; Xu, Y.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; Shen, H.; Wen, F.; et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): A national cross-sectional study. Lancet 2018, 391, 1706–1717. [Google Scholar] [CrossRef]
- Burney, P.; Patel, J.; Minelli, C.; Gnatiuc, L.; Amaral, A.F.; Kocabaş, A.; Cherkaski, H.H.; Gulsvik, A.; Nielsen, R.; Bateman, E.; et al. Prevalence and population attributable risk for chronic airflow obstruction in a large multinational study. Am. J. Respir. Crit. Care Med. 2020, 203, 1353–1365. [Google Scholar] [CrossRef]
- Wang, S.; Xu, L.; Jonas, J.B.; You, Q.S.; Wang, Y.X.; Yang, H. Prevalence and associated factors of dyslipidemia in the adult Chinese population. PLoS ONE 2011, 6, e17326. [Google Scholar] [CrossRef]
- Li, C.H.; Chen, W.C.; Liao, W.C.; Tu, C.Y.; Lin, C.L.; Sung, F.C.; Chen, C.H.; Hsu, W.H. The association between chronic obstructive pulmonary disease and Parkinson’s disease: A nationwide population-based retrospective cohort study. Qjm 2015, 108, 39–45. [Google Scholar] [CrossRef]
- Chen, S.J.; Yeh, C.M.; Chao, T.F.; Liu, C.J.; Wang, K.L.; Chen, T.J.; Chou, P.; Wang, F.D. The use of benzodiazepine receptor agonists and risk of respiratory failure in patients with chronic obstructive pulmonary disease: A nationwide population-based case-control study. Sleep 2015, 38, 1045–1050. [Google Scholar] [CrossRef]
- Huang, H.H.; Chen, S.J.; Chao, T.F.; Liu, C.J.; Chen, T.J.; Chou, P.; Wang, F.D. Influenza vaccination and risk of respiratory failure in patients with chronic obstructive pulmonary disease: A nationwide population-based case-cohort study. J. Microbiol. Immunol. Infect. 2019, 52, 22–29. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Data | Patients with Hyperlipidemia | Patients without Hyperlipidemia | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age, year * | 42.54 (13.26) | 42.54 (13.26) | |||
| ≥65 | 1571 | 8.0 | 7004 | 8.0 | 0.999 |
| <65 | 20,039 | 92.0 | 80,156 | 92.0 | |
| Sex | |||||
| Male | 12,938 | 59.4 | 51,752 | 59.4 | 0.999 |
| Female | 8852 | 40.6 | 35,408 | 40.6 | |
| Comorbidities | |||||
| Diabetes mellitus | 3278 | 15.0 | 3471 | 4.0 | <0.001 |
| Hypertension | 5536 | 25.4 | 7865 | 9.0 | <0.001 |
| Nephropathy | 2052 | 9.4 | 4216 | 4.8 | <0.001 |
| Depression | 297 | 1.4 | 653 | 0.7 | <0.001 |
| Cirrhosis | 218 | 1.0 | 636 | 0.7 | <0.001 |
| Autoimmune disease | 540 | 2.5 | 1112 | 1.3 | <0.001 |
| Congestive heart failure | 266 | 1.2 | 516 | 0.6 | <0.001 |
| Alcoholism | 490 | 2.2 | 945 | 1.1 | <0.001 |
| Obesity | 292 | 1.3 | 164 | 0.2 | <0.001 |
| Degree of urbanization | <0.001 | ||||
| Urban | 13,856 | 63.6 | 54,089 | 62.1 | |
| Suburban | 6621 | 30.4 | 27,736 | 31.8 | |
| Rural | 1313 | 6.0 | 5335 | 6.1 | |
| Income | <0.001 | ||||
| High income | 3667 | 16.8 | 12,028 | 13.8 | |
| Medium income | 4642 | 21.3 | 17,451 | 20.0 | |
| Low income | 10,009 | 45.9 | 43,761 | 50.2 | |
| No income | 3472 | 15.9 | 13,920 | 16.0 | |
| Follow-up, years * | 8.88 (4.00) | 9.42 (3.74) | <0.001 | ||
| Patients with Hyperlipidemia | Patients without Hyperlipidemia | RR (95% CI) * | p Value | |||
|---|---|---|---|---|---|---|
| No. of COPD | Incidence † | No. of COPD | Incidence † | |||
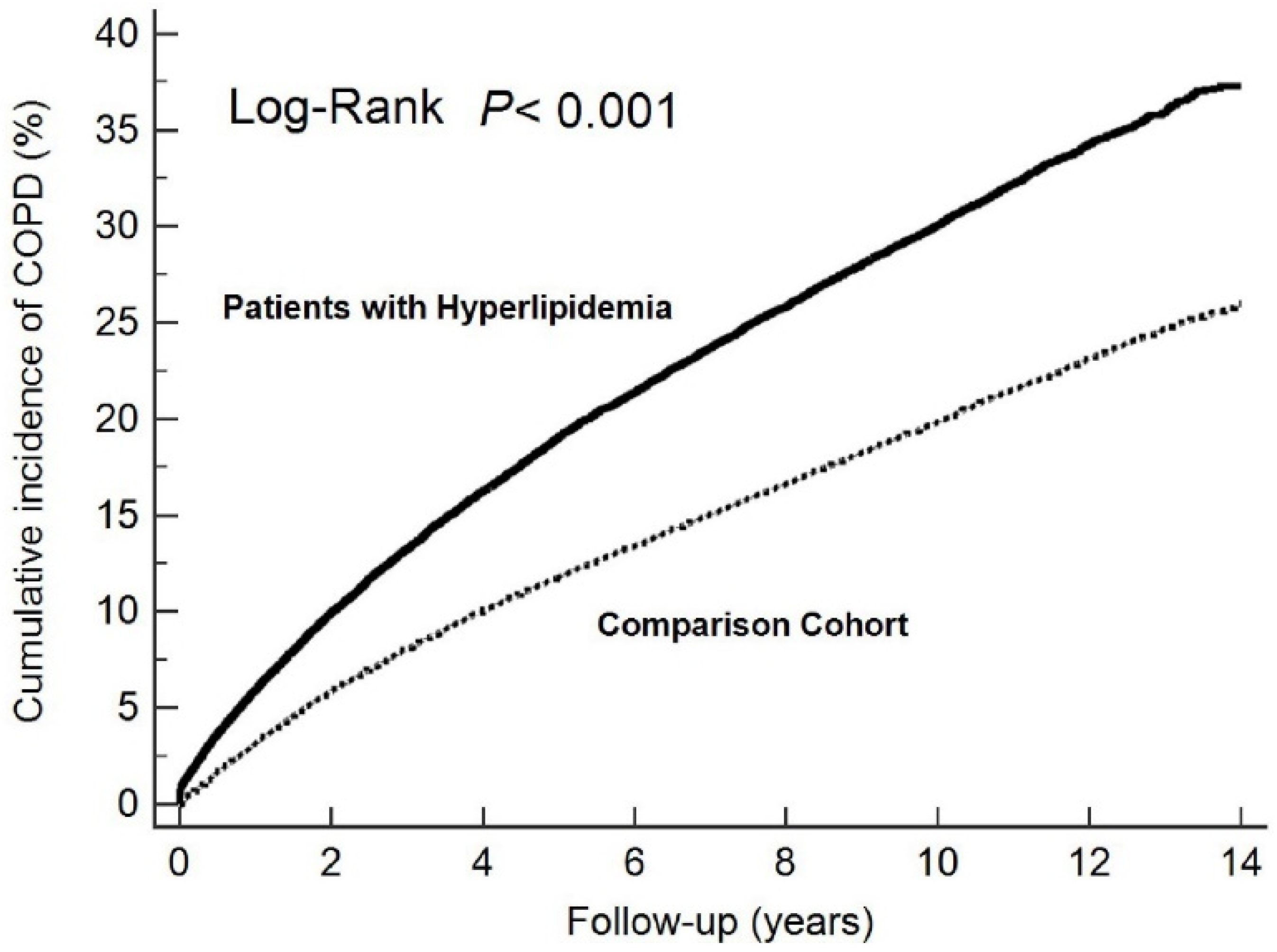
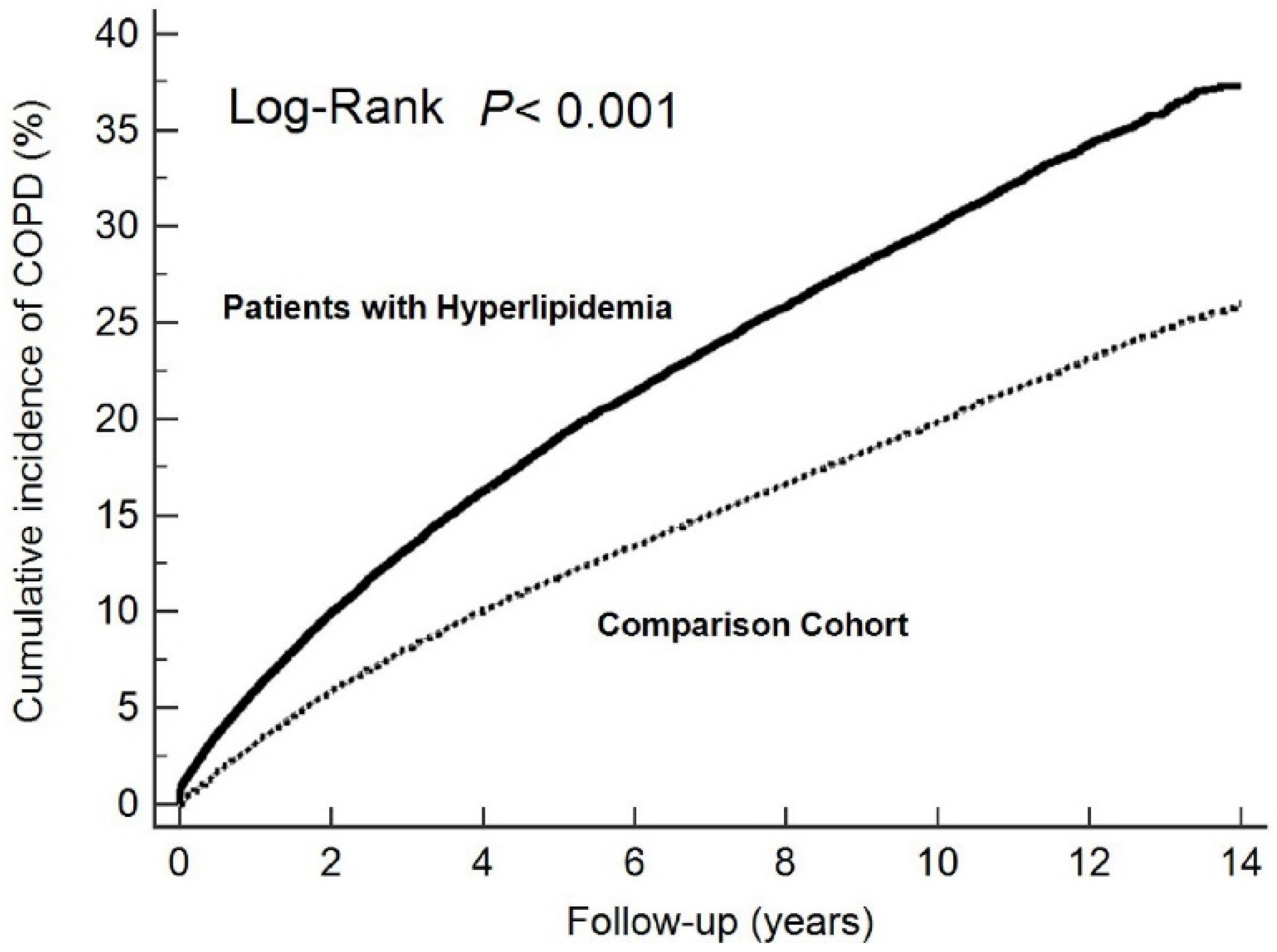
| Total | 6995 | 36.14 | 18,295 | 22.29 | 1.61 (1.57–1.66) | <0.001 |
| Age, year | ||||||
| ≥65 | 900 | 81.98 | 2999 | 69.33 | 1.19 (1.10–1.28) | <0.001 |
| <65 | 6095 | 33.38 | 15,296 | 19.67 | 1.69 (1.64–1.74) | <0.001 |
| Sex | ||||||
| Male | 4021 | 35.12 | 10,607 | 21.96 | 1.59 (1.53–1.65) | <0.001 |
| Female | 2974 | 37.62 | 7688 | 22.75 | 1.64 (1.58–1.72) | <0.001 |
| Follow-up, years | ||||||
| 0–1 | 1286 | 2276.50 | 2722 | 1344.67 | 1.72 (1.61–1.84) | <0.001 |
| 1–5 | 2829 | 310.19 | 7256 | 257.26 | 1.16 (1.11–1.21) | <0.001 |
| 5–10 | 2248 | 42.83 | 6381 | 30.67 | 1.45 (1.38–1.52) | <0.001 |
| ≥10 | 632 | 4.81 | 1936 | 3.32 | 1.46 (1.33–1.59) | <0.001 |
| Predictive Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Hyperlipidemia | 1.61 (1.57–1.66) | <0.001 | 1.48 (1.44–1.53) | <0.001 |
| Age (<65 = 0, ≥65 = 1) | 3.09 (2.99–3.20) | <0.001 | 2.63 (2.52–2.73) | <0.001 |
| Sex (male = 0, female = 1) | 1.05 (1.02–1.07) | <0.001 | 1.05 (1.02–1.08) | <0.001 |
| Comorbidities | ||||
| Diabetes mellitus | 1.70 (1.63–1.78) | <0.001 | 1.08 (1.03–1.13) | 0.001 |
| Hypertension | 2.07 (2.00–2.13) | <0.001 | 1.32 (1.28–1.37) | <0.001 |
| Nephropathy | 1.61 (1.54–1.69) | <0.001 | 1.25 (1.20–1.31) | <0.001 |
| Depression | 1.26 (1.11–1.42) | <0.001 | 1.15 (1.02–1.30) | 0.026 |
| Cirrhosis | 1.71 (1.51–1.94) | <0.001 | 1.31 (1.15–1.49) | <0.001 |
| Autoimmune disease | 1.33 (1.21–1.45) | <0.001 | 1.15 (1.05–1.26) | 0.004 |
| Congestive heart failure | 2.63 (2.36–2.94) | <0.001 | 1.29 (1.15–1.45) | <0.001 |
| Alcoholism | 1.35 (1.22–1.50) | <0.001 | 1.15 (1.03–1.27) | 0.011 |
| Obesity | 1.49 (1.27–1.75) | <0.001 | 1.22 (1.04–1.44) | 0.015 |
| Degree of urbanization | ||||
| Urban | Reference | Reference | ||
| Suburban | 1.09 (1.06–1.12) | <0.001 | 1.06 (1.03–1.08) | <0.001 |
| Rural | 1.36 (1.30–1.43) | <0.001 | 1.24 (1.18–1.30) | <0.001 |
| Income | ||||
| High income | Reference | Reference | ||
| Medium income | 1.04 (1.00–1.09) | 0.075 | 1.05 (1.00–1.10) | 0.033 |
| Low income | 1.16 (1.12–1.21) | <0.001 | 1.02 (0.98–1.06) | 0.322 |
| No income | 1.26 (1.21–1.32) | <0.001 | 0.98 (0.94–1.03) | 0.479 |
| Predictive Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (<65 = 0, ≥65 = 1) | 2.34 (2.18–2.51) | <0.001 | 2.07 (1.91–2.24) | <0.001 |
| Sex (male = 0, female = 1) | 1.07 (1.02–1.13) | 0.004 | 1.07 (1.01–1.12) | 0.011 |
| Comorbidities | ||||
| Diabetes mellitus | 1.18 (1.11–1.26) | <0.001 | 1.01 (0.95–1.08) | 0.735 |
| Hypertension | 1.41 (1.34–1.48) | <0.001 | 1.19 (1.13–1.26) | <0.001 |
| Nephropathy | 1.33 (1.23–1.43) | <0.001 | 1.21 (1.12–1.30) | <0.001 |
| Depression | 1.13 (0.93–1.37) | 0.226 | ||
| Cirrhosis | 1.20 (0.95–1.51) | 0.129 | ||
| Autoimmune disease | 1.18 (1.03–1.37) | 0.022 | 1.11 (0.96–1.28) | 0.179 |
| Congestive heart failure | 1.94 (1.62–2.33) | <0.001 | 1.36 (1.13–1.63) | 0.001 |
| Alcoholism | 1.09 (0.93–1.28) | 0.280 | ||
| Obesity | 1.15 (0.94–1.39) | 0.171 | ||
| Degree of urbanization | ||||
| Urban | Reference | Reference | ||
| Suburban | 1.06 (1.01–1.12) | 0.024 | 1.03 (0.98–1.09) | 0.230 |
| Rural | 1.22 (1.11–1.34) | <0.001 | 1.14 (1.04–1.26) | 0.006 |
| Income | ||||
| High income | Reference | Reference | ||
| Medium income | 1.16 (1.07–1.25) | <0.001 | 1.15 (1.06–1.24) | 0.001 |
| Low income | 1.33 (1.24–1.42) | <0.001 | 1.18 (1.10–1.27) | <0.001 |
| No income | 1.32 (1.21–1.43) | <0.001 | 1.06 (0.97–1.16) | 0.191 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.-Y.; Hu, L.-Y.; Chen, H.-J.; Chen, R.-Y.; Hu, C.-K.; Shen, C.-C. Increased Risk of Chronic Obstructive Pulmonary Disease in Patients with Hyperlipidemia: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 12331. https://doi.org/10.3390/ijerph191912331
Yang H-Y, Hu L-Y, Chen H-J, Chen R-Y, Hu C-K, Shen C-C. Increased Risk of Chronic Obstructive Pulmonary Disease in Patients with Hyperlipidemia: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12331. https://doi.org/10.3390/ijerph191912331
Chicago/Turabian StyleYang, Hao-Yu, Li-Yu Hu, Hon-Jhe Chen, Ru-Yih Chen, Chang-Kuo Hu, and Cheng-Che Shen. 2022. "Increased Risk of Chronic Obstructive Pulmonary Disease in Patients with Hyperlipidemia: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 19: 12331. https://doi.org/10.3390/ijerph191912331
APA StyleYang, H.-Y., Hu, L.-Y., Chen, H.-J., Chen, R.-Y., Hu, C.-K., & Shen, C.-C. (2022). Increased Risk of Chronic Obstructive Pulmonary Disease in Patients with Hyperlipidemia: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 19(19), 12331. https://doi.org/10.3390/ijerph191912331