
Mathematical Modeling of the Evolution of Absenteeism in a University Hospital over 12 Years


 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Judgment Criteria
2.4. Statistics
3. Results
3.1. Description of the Population
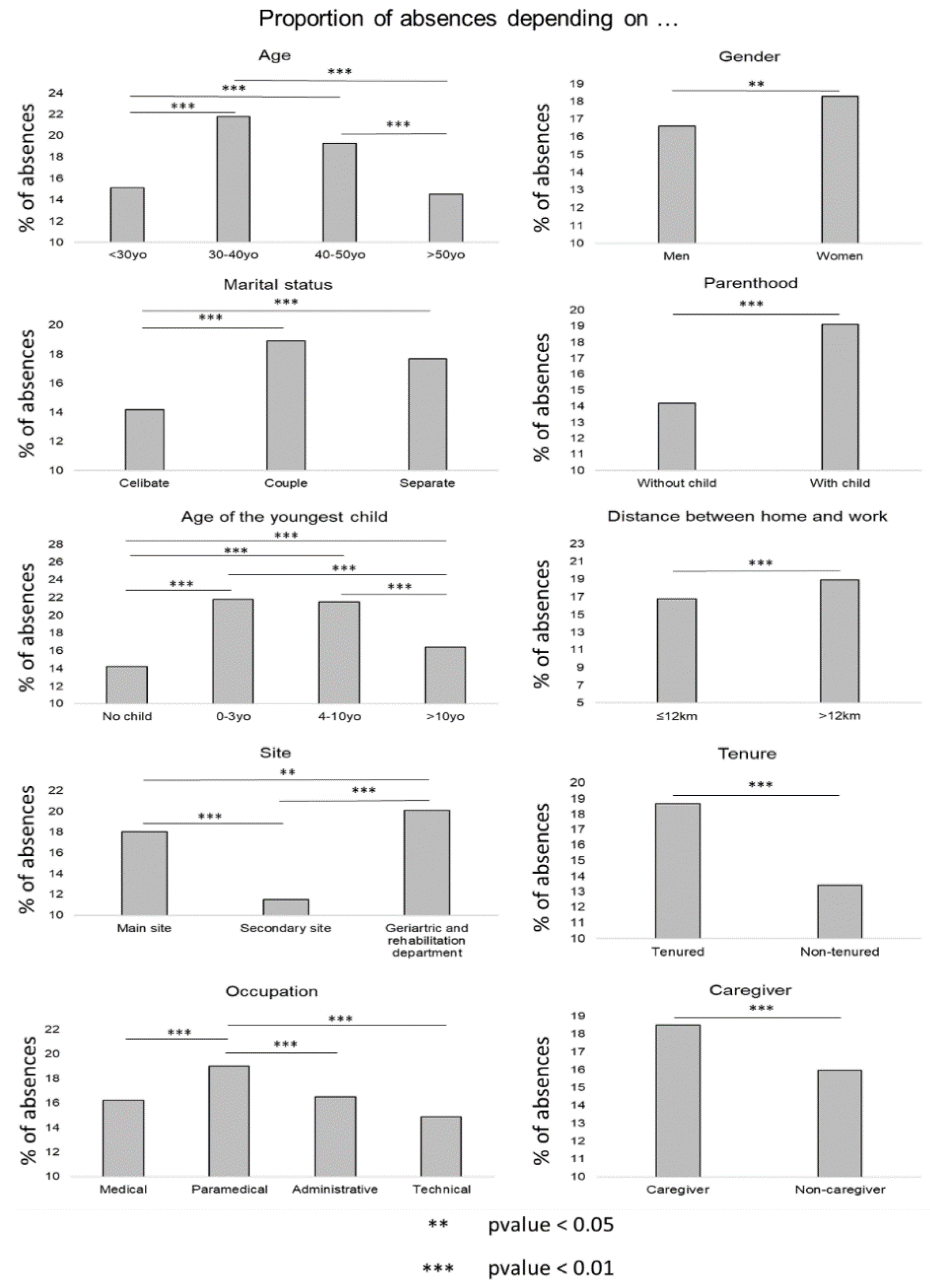
3.2. Descriptive Analysis
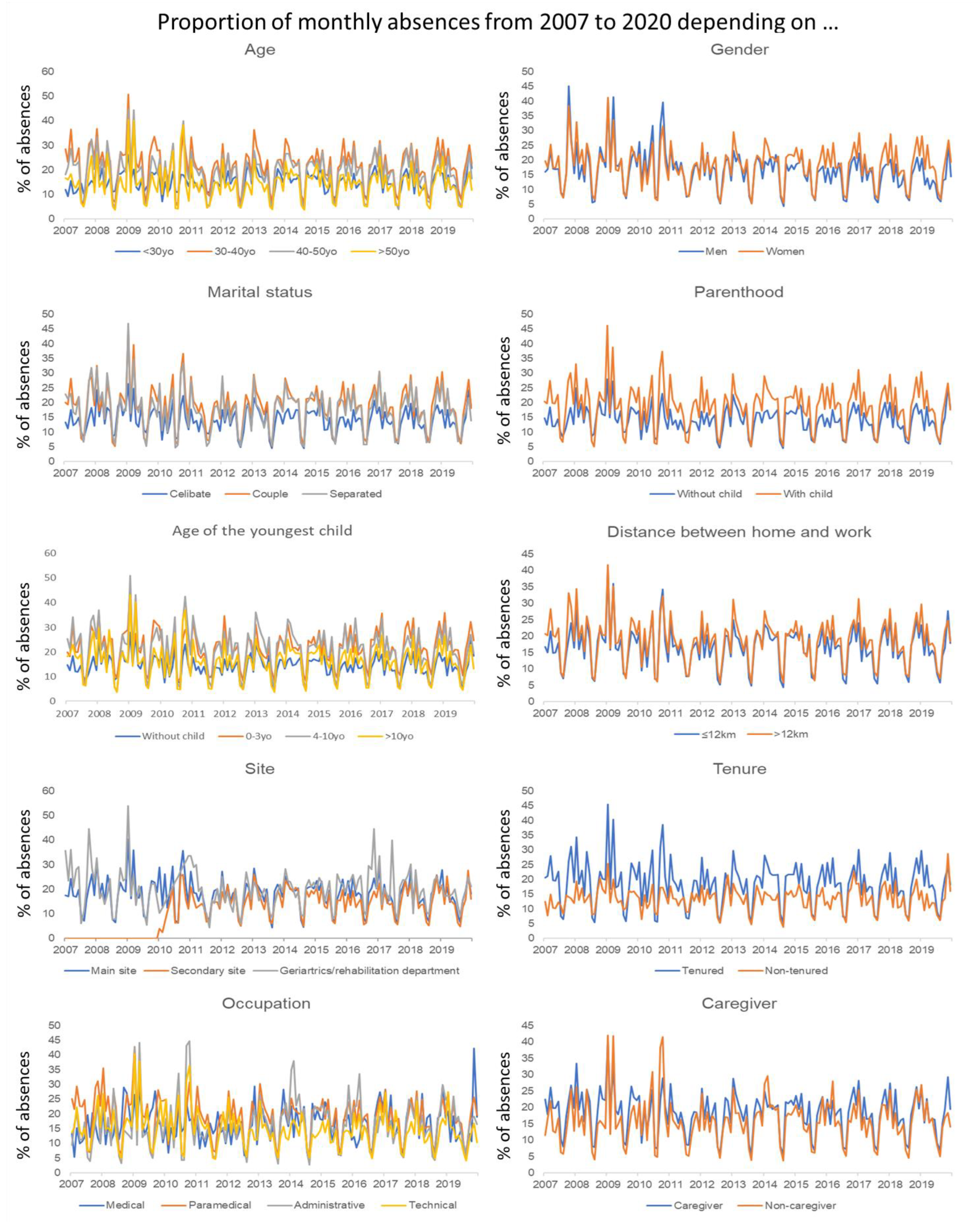
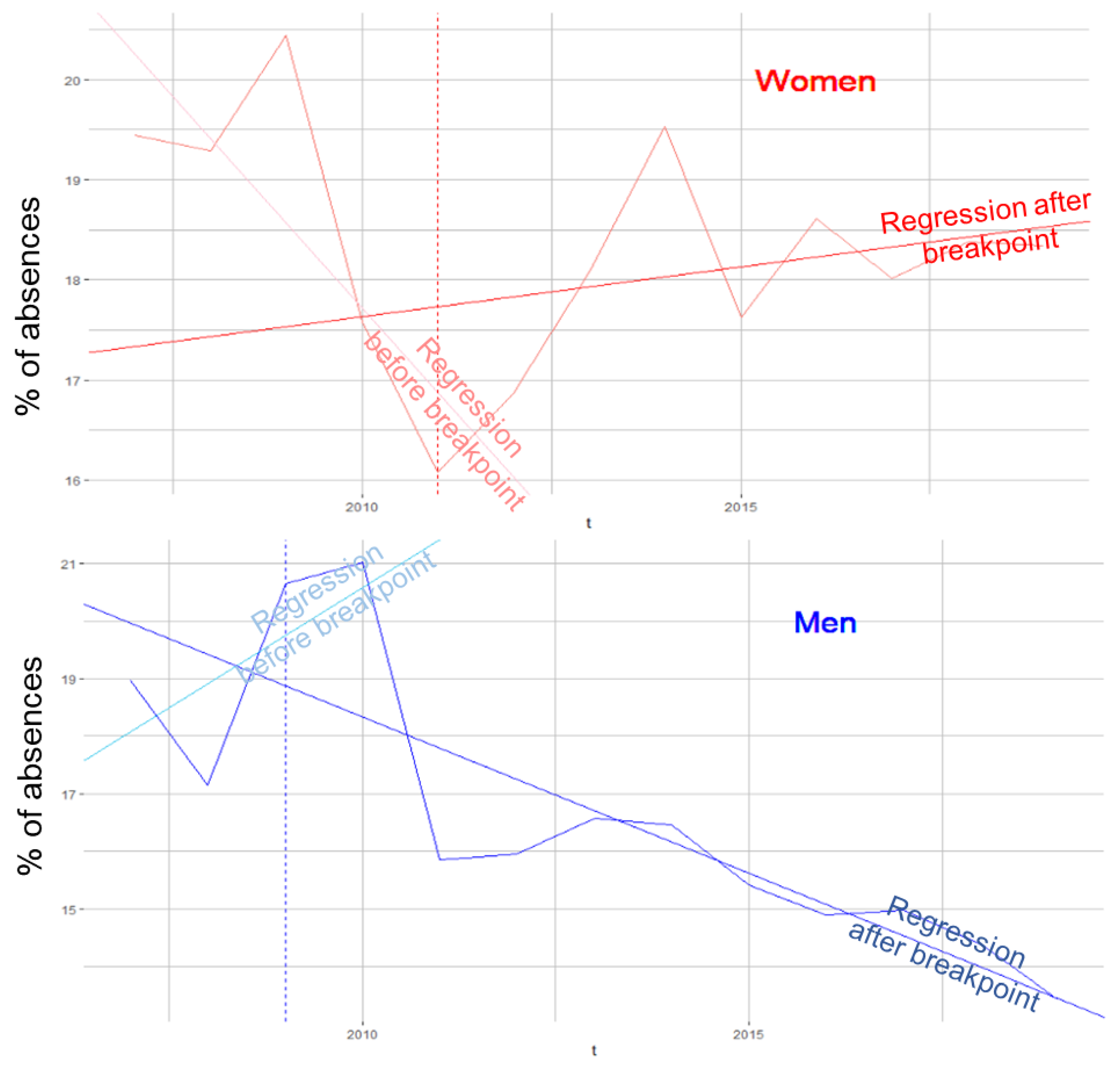
3.3. Time Series
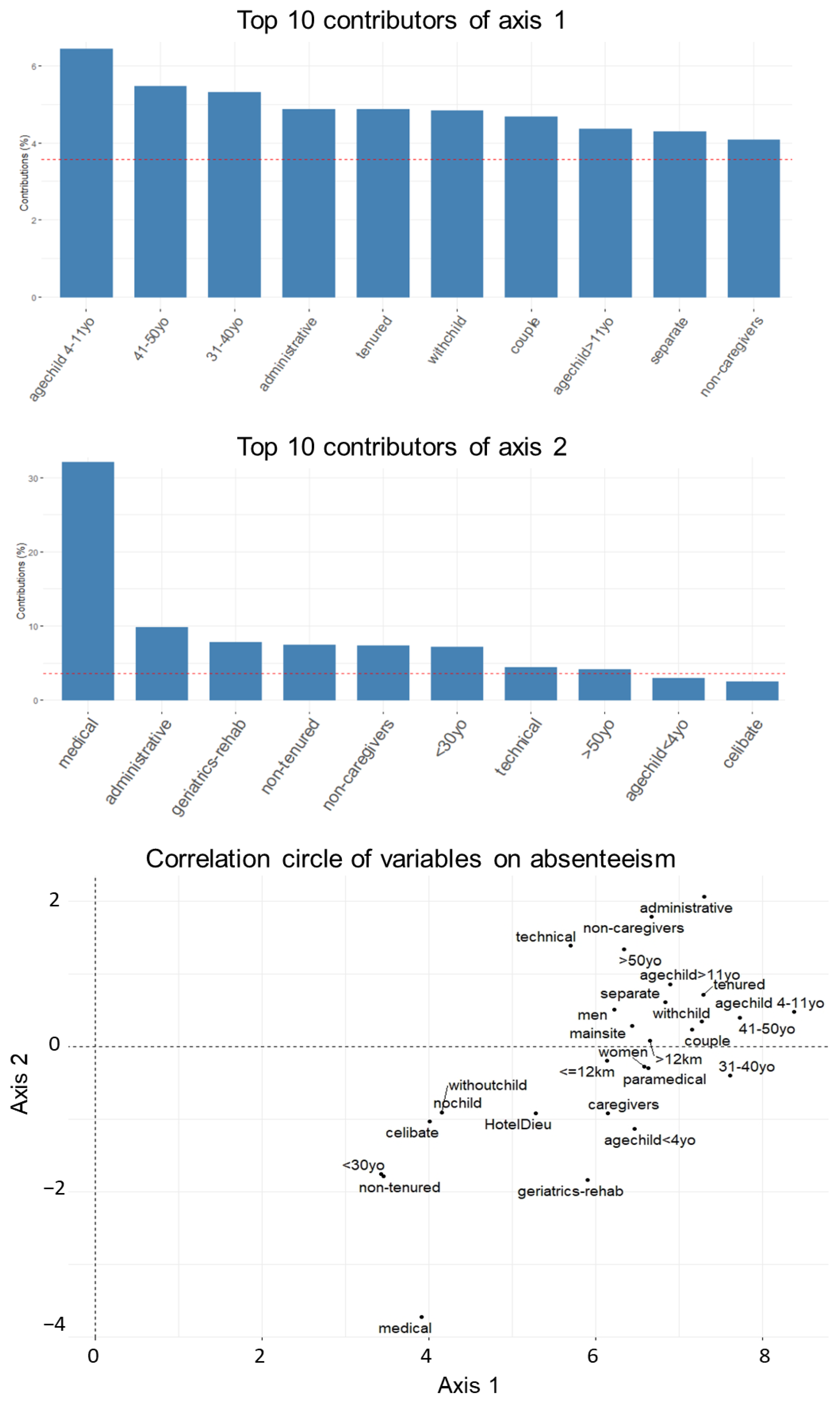
3.4. Principal Components Aanalysis
3.5. Principal Component Analysis by Period
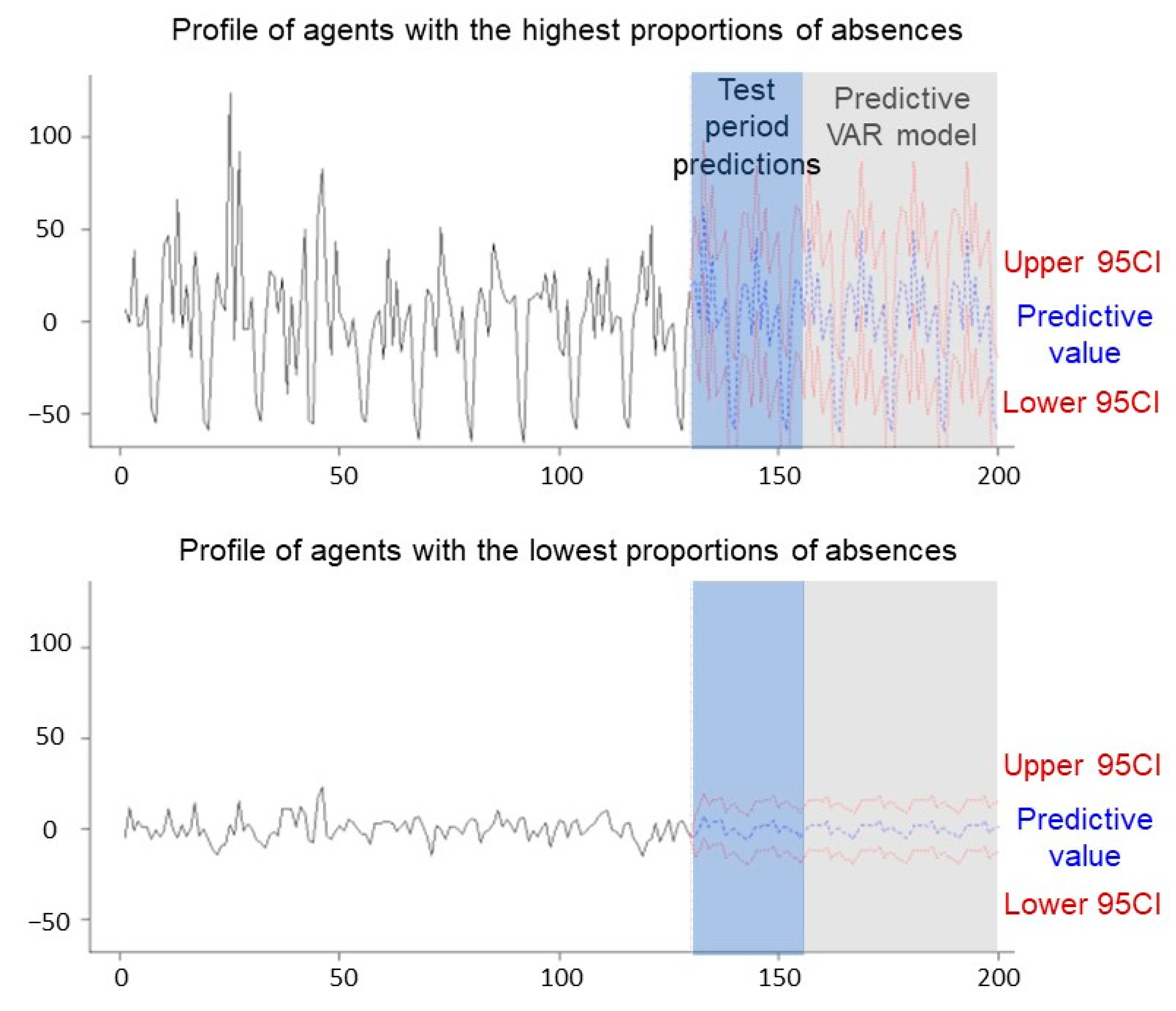
3.6. Autoregressive Vector
4. Discussion
4.1. Sociodemographic and Occupational Factors Influencing Absences
4.2. The VAR Model
4.3. Solutions to Reduce the Major Problem of Absenteeism
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Randon, S.; Baret, C.; Prioul, C. La prévention de l’absentéisme du personnel soignant en gériatrie: Du savoir académique à l’action managériale. Manag. Avenir 2011, 49, 133–149. [Google Scholar] [CrossRef]
- Thévenet, M. Impliquer les Personnes dans l’Entreprise; Éd. Liaisons: Paris, France, 1992; pp. 25–205. [Google Scholar]
- Brami, L.; Damart, S.; Kletz, F. Santé au travail et travail en santé. La performance des établissements de santé face à l’absentéisme et au bien-être des personnels soignants. Manag. Avenir 2013, 61, 168–189. [Google Scholar] [CrossRef]
- Duclay, E.; Hardouin, J.B.; Sébille, V.; Anthoine, E.; Moret, L. Exploring the impact of staff absenteeism on patient satisfaction using routine databases in a university hospital. J. Nurs. Manag. 2015, 23, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Kletz, F.; Brami, L.; Damart, S.; Detchessahar, M.; Devigne, M.; Habib, J.; Krohmer, C. L’Absentéisme des Personnels Soignants à l’Hôpital: Comprendre et Agir; Presses des Mines: Paris, France, 2016; p. 156. Available online: http://books.openedition.org/pressesmines/2310 (accessed on 28 April 2021).
- Brami, L.; Damart, S.; Kletz, F. Réformes de l’hôpital, crise à l’hôpital: Une étude des liens entre réformes hospitalières et absentéisme des personnels soignants. Polit. Manag. Public 2012, 29, 541–661. [Google Scholar] [CrossRef]
- Agence Nationale Pour L’Amélioration des Conditions de Travail (Anact). Available online: https://www.anact.fr/ (accessed on 28 April 2021).
- Forssman, D.S. L’Absentéisme dans l’Industrie. 1955, p. 8. Available online: https://apps.who.int/iris/bitstream/handle/10665/265633/PMC2538116.pdf?sequence=1&isAllowed=y (accessed on 28 April 2021).
- Ministère du Travail. Les Absences au Travail des Salariés pour Raisons de Santé: Un Rôle Important des Conditions de Travail. 2013. Available online: https://travail-emploi.gouv.fr/IMG/pdf/2013-009.pdf (accessed on 28 April 2021).
- Strömberg, C.; Aboagye, E.; Hagberg, J.; Bergström, G.; Lohela-Karlsson, M. Estimating the Effect and Economic Impact of Absenteeism, Presenteeism, and Work Environment-Related Problems on Reductions in Productivity from a Managerial Perspective. Value Health 2017, 20, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Howard, K.J.; Howard, J.T.; Smyth, A.F. The Problem of Absenteeism and Presenteeism in the Workplace. In Handbook of Occupational Health and Wellness; Gatchel, R.J., Schultz, I.Z., Eds.; Springer: Boston, MA, USA, 2012; pp. 151–179. [Google Scholar] [CrossRef]
- Mickaël, B. Absentéisme: De la Nécessité de Lutter Contre un Tabou Hospitalier. La Réduction de l’Absentéisme de Courte Durée du Personnel Non Médical à l’Hôpital Necker—Enfants Malades (AP-HP); Ecole des hautes études en Santé Publique: Rennes, France, 2009; p. 73. Available online: https://documentation.ehesp.fr/memoires/2009/edh/battesti.pdf (accessed on 23 April 2021).
- Gallois, P. L’Absentéisme: Comprendre et Agir; Editions Liaisons: Paris, France, 2005; Available online: https://www.lgdj.fr/l-absenteisme-comprendre-et-agir-9782878807837.html (accessed on 28 April 2021).
- Dumas, M. Absentéisme Maladie et Santé au Travail: Cause Démographique et Remèdes. Santé au Travail et Travail de Santé; Presses de l’EHESP: Rennes, France, 2008; Available online: https://www.cairn.info/sante-au-travail-et-travail-de-sante--9782859529680-page-131.html (accessed on 28 April 2021).
- Barometre-Absenteisme-2020-Ayming. 2020. Available online: https://www.ayming.fr/wp-content/uploads/sites/11/2020/09/Barometre-absenteisme-2020-Ayming.pdf (accessed on 28 April 2021).
- 13ème édition du Panorama du Risque en Etablissements de Santé, Sociaux et Médico-Sociaux—Édition 2017. 2017. Available online: https://www.relyens.eu/sites/default/files/2018-01/efd42d49ffb683e3829e623d449c7979.pdf (accessed on 28 April 2021).
- DREES. Rapport-ESPF-2017.pdf. 2017. Available online: https://drees.solidarites-sante.gouv.fr/sites/default/files/2021-01/Rapport-ESPF-2017.pdf (accessed on 29 April 2021).
- Motet, L.; Béguin, F.; Gittus, S.; Dedier, E.; Dumas, E. Infirmiers, Aides-Soignants… A l’Hôpital, les Arrêts Maladie s’Allongent chez les Personnels Non Médicaux. Le Monde.fr. 16 December 2019. Available online: https://www.lemonde.fr/societe/article/2019/12/16/infirmiers-aides-soignants-a-l-hopital-les-arrets-maladie-s-allongent-chez-les-personnels-non-medicaux_6023086_3224.html (accessed on 29 April 2021).
- Kaiser, C.P. Absenteeism, Presenteeism, and Workplace Climate: A Taxonomy of Employee Attendance Behaviors. Econ. Bus. J. Inq. Perspect. 2018, 9, 19. [Google Scholar]
- Toque, C. For the Identification of Time-Series Models. Application to Arma Pocesses. Available online: https://pastel.archives-ouvertes.fr/pastel-00001966/document (accessed on 22 June 2021).
- Larif, M.; Soulaymani, A.; Elmidaoui, A. Evaluation spatio-temporelle du degré de la pollution industrielle oléicole sur les cours d’eaux de l’oued Boufekrane dans la région de Meknès-Tafilalt (Maroc) [Spatio-temporal assessment of the degree of industrial pollution on Olive waterways of the Boufekrane river in the region of Meknès-Tafilalt (Morocco)]. J. Mater. Environ. Sci. 2013, 4, 432–441. [Google Scholar]
- NCSS Statistical Software. Principal Components Analysis. In Multivariate Analysis in NCSS; NCSS, LLC: Kaysville, UT, USA, 2022; p. 41. Available online: https://ncss-wpengine.netdna-ssl.com/wp-content/themes/ncss/pdf/Procedures/NCSS/Principal_Components_Analysis.pdf (accessed on 21 June 2022).
- Lütkepohl, H. Vector Autoregressive Models. Handbook of Research Methods and Applications in Empirical Macroeconomics. 30 July 2013. Available online: https://www.elgaronline.com/view/edcoll/9780857931016/9780857931016.00012.xml (accessed on 22 June 2021).
- Zivot, E.; Wang, J. (Eds.) Vector Autoregressive Models for Multivariate Time Series. In Modeling Financial Time Series with S-PLUS®; Springer: New York, NY, USA, 2006; pp. 385–429. [Google Scholar] [CrossRef]
- Dolan, S.L.; Arsenault, A.; Lizotte, J.P.; Abenhaim, L. L’absentéisme hospitalier au Québec: Aspects culturels et socio-démographiques. Relat. Ind. 1983, 38, 14. [Google Scholar] [CrossRef][Green Version]
- Pollak, C.; Ricroch, L. Les disparités d’absentéisme à l’hôpital sont-elles associées à des différences de conditions de travail? Rev. Fr. D’economie 2016, 31, 181–220. [Google Scholar] [CrossRef]
- Lipszyc, B.; Laurent, S. L’Absentéisme Dans Une Institution Hospitalière: Les Facteurs Déterminants. 2000. Available online: http://www.timberlake-consultancy.com/slaurent/pdf/ber-1041.pdf (accessed on 18 May 2022).
- Côté, D.; Haccoun, R.R. L’absentéisme des femmes et des hommes: Une méta-analyse. Can. J. Adm. Sci. Rev. Can. Sci. L’Adm. 1991, 8, 130–139. [Google Scholar] [CrossRef]
- Chaupain-Guillot, S.; Guillot, O. Les déterminants individuels de l’absentéisme au travail. Rev. Econ. 2011, 62, 419–427. [Google Scholar] [CrossRef]
- Tchuinguem, G. Ampleur, Coûts, Facteurs Personnels et Occupationnels de L’Absentéisme Dans la Fonction Publique Hospitalière au Cameroun. 2009. Available online: https://papyrus.bib.umontreal.ca/xmlui/handle/1866/3205 (accessed on 18 May 2021).
- Huver, B.; Richard, S.; Vaneecloo, N.; Bierla, I. Âge, absence-maladie et présentéisme au travail: Le cas d’un établissement de santé régional. Manag. Avenir 2014, 70, 97–114. [Google Scholar] [CrossRef]
- Isah, E.C.; Omorogbe, V.E.; Orji, O.; Oyovwe, L. Self-reported absenteeism among hospital workers in benin city, Nigeria. Ghana Med J. Mars 2008, 42, 2–7. [Google Scholar]
- Lim, A.; Chongsuvivatwong, V.; Geater, A.; Chayaphum, N.; Thammasuwan, U. Influence of Work Type on Sickness Absence among Personnel in a Teaching Hospital. J. Occup. Health 2002, 44, 254–263. [Google Scholar] [CrossRef]
- Borda, R.G.; Norman, I.J. Testing a model of absence and intent to stay in employment: A study of registered nurses in Malta. Int. J. Nurs. Stud. 1997, 34, 375–384. [Google Scholar] [CrossRef]
- Dilasser, A.; Huet, S.; Lavenu, G.; le Guyader, Y.; Prudent, L.; Vuillin, P.; Hellie, J.; Joyeux, J.; Leroy, C.; Millet, P. Analyser et Prévenir l’Absentéisme Dysfonctionnel dans le Secteur de la Santé; Ecole des hautes études en Santé Publique: Rennes, France, 2017; p. 74. Available online: https://documentation.ehesp.fr/memoires/2017/mip/groupe%2011.pdf (accessed on 23 April 2021).
- Absentéisme: Première Cause, Une Mauvaise Organisation du Travail. Available online: https://www.techopital.com/absenteisme---premiere-cause,-une-mauvaise-organisation-du-travail-NS_1199.html (accessed on 18 May 2021).
- Stock, J.H.; Watson, M.W. Vector Autoregressions. J. Econ. Perspect. 2001, 15, 101–115. [Google Scholar] [CrossRef]
- Les Œufs Geslin Identifie les Causes de son Absentéisme et Met en Place des Actions de Prévention|Agence Pationale pour l’Amélioration des Conditions de Travail (Anact). Available online: https://www.anact.fr/cas/les-oeufs-geslin-identifie-les-causes-de-son-absenteisme-et-met-en-place-des-actions-de (accessed on 28 April 2021).
- Patton, E. The devil is in the details: Judgments of responsibility and absenteeism from work. J. Occup. Organ. Psychol. 2011, 84, 759–779. [Google Scholar] [CrossRef]
- Commeiras, N.; Achmet, V. La Gestion de l’Absentéisme à l’Hôpital Public: Les Effets Délétères de Solutions Trop Fragiles. The Conversation. Available online: http://theconversation.com/la-gestion-de-labsenteisme-a-lhopital-public-les-effets-deleteres-de-solutions-trop-fragiles-154596 (accessed on 21 April 2021).
- Cohen, A.; Golan, R. Predicting absenteeism and turnover intentions by past absenteeism and work attitudes: An empirical examination of female employees in long term nursing care facilities. Career Dev. Int. 2007, 12, 416–432. [Google Scholar] [CrossRef]
- Burmeister, E.A.; Kalisch, B.J.; Xie, B.; Doumit, M.A.A.; Lee, E.; Ferraresion, A.; Terzioglu, F.; Bragadóttir, H. Determinants of nurse absenteeism and intent to leave: An international study. J. Nurs. Manag. 2019, 27, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Eshoj, P.; Jepsen, J.R.; Nielsen, C.V. Long-term sickness absence—Risk indicators among occupationally active residents of a Danish county. Occup. Med. 2001, 51, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Derros, E. L’hôpital Malade de l’absentéisme santé: Evaluation Socio-Economique des Congés «“Maladie”» non Ordinaires Chez Les Personnels Non Médicaux Dans Trois Etablissements Publics d’Auvergne; Université d’Auvergne Clermont I: Clermont-Ferrand, France, 2012; Available online: https://tel.archives-ouvertes.fr/tel-01168277/document (accessed on 1 June 2021).
- Baccelli, L. Comment Calculer le Coût de l’Absentéisme en Entreprise? Culture RH. 2020. Available online: https://culture-rh.com/comment-calculer-cout-absenteisme-entreprise/ (accessed on 20 May 2021).
- Barometre Absenteisme 2015 Ayming. 2015. Available online: https://goodwill-management.com/wp-content/uploads/2020/01/Barometre_Absenteisme_2015_ayming-goodwill-management.pdf (accessed on 1 June 2021).





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vialatte, L.; Pereira, B.; Guillin, A.; Miallaret, S.; Baker, J.S.; Colin-Chevalier, R.; Yao-Lafourcade, A.-F.; Azzaoui, N.; Clinchamps, M.; Bouillon-Minois, J.-B.; et al. Mathematical Modeling of the Evolution of Absenteeism in a University Hospital over 12 Years. Int. J. Environ. Res. Public Health 2022, 19, 8236. https://doi.org/10.3390/ijerph19148236
Vialatte L, Pereira B, Guillin A, Miallaret S, Baker JS, Colin-Chevalier R, Yao-Lafourcade A-F, Azzaoui N, Clinchamps M, Bouillon-Minois J-B, et al. Mathematical Modeling of the Evolution of Absenteeism in a University Hospital over 12 Years. International Journal of Environmental Research and Public Health. 2022; 19(14):8236. https://doi.org/10.3390/ijerph19148236
Chicago/Turabian StyleVialatte, Luc, Bruno Pereira, Arnaud Guillin, Sophie Miallaret, Julien Steven Baker, Rémi Colin-Chevalier, Anne-Françoise Yao-Lafourcade, Nourddine Azzaoui, Maëlys Clinchamps, Jean-Baptiste Bouillon-Minois, and et al. 2022. "Mathematical Modeling of the Evolution of Absenteeism in a University Hospital over 12 Years" International Journal of Environmental Research and Public Health 19, no. 14: 8236. https://doi.org/10.3390/ijerph19148236
APA StyleVialatte, L., Pereira, B., Guillin, A., Miallaret, S., Baker, J. S., Colin-Chevalier, R., Yao-Lafourcade, A.-F., Azzaoui, N., Clinchamps, M., Bouillon-Minois, J.-B., & Dutheil, F. (2022). Mathematical Modeling of the Evolution of Absenteeism in a University Hospital over 12 Years. International Journal of Environmental Research and Public Health, 19(14), 8236. https://doi.org/10.3390/ijerph19148236