
Tuberculosis among Ambulatory People Living with HIV in Guangxi Province, China: A Longitudinal Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
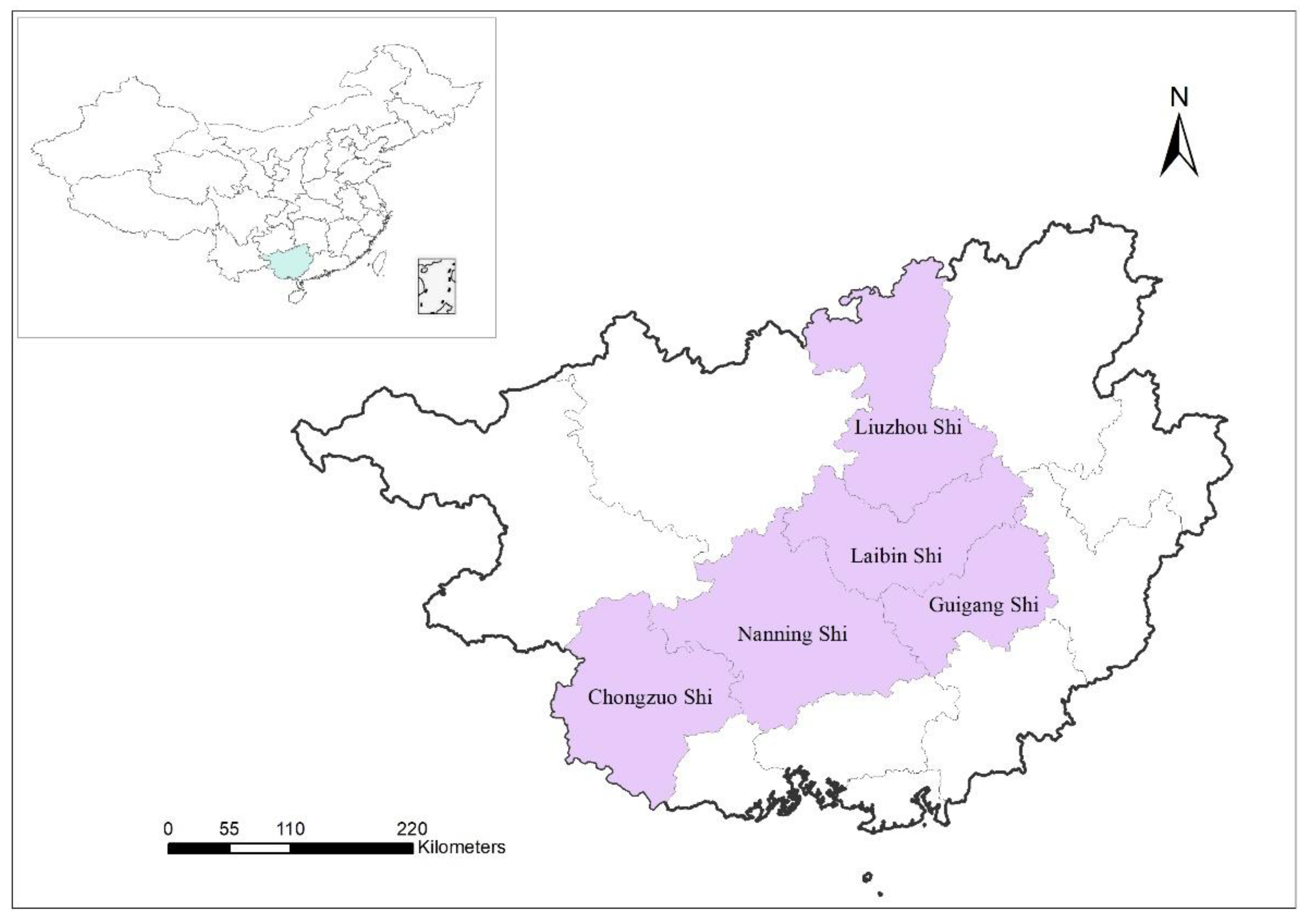
2.1. Study Design and Participants
2.2. Procedures
2.3. Statistical Analysis
2.4. Ethical Consideration
3. Results
3.1. TB Diagnosis
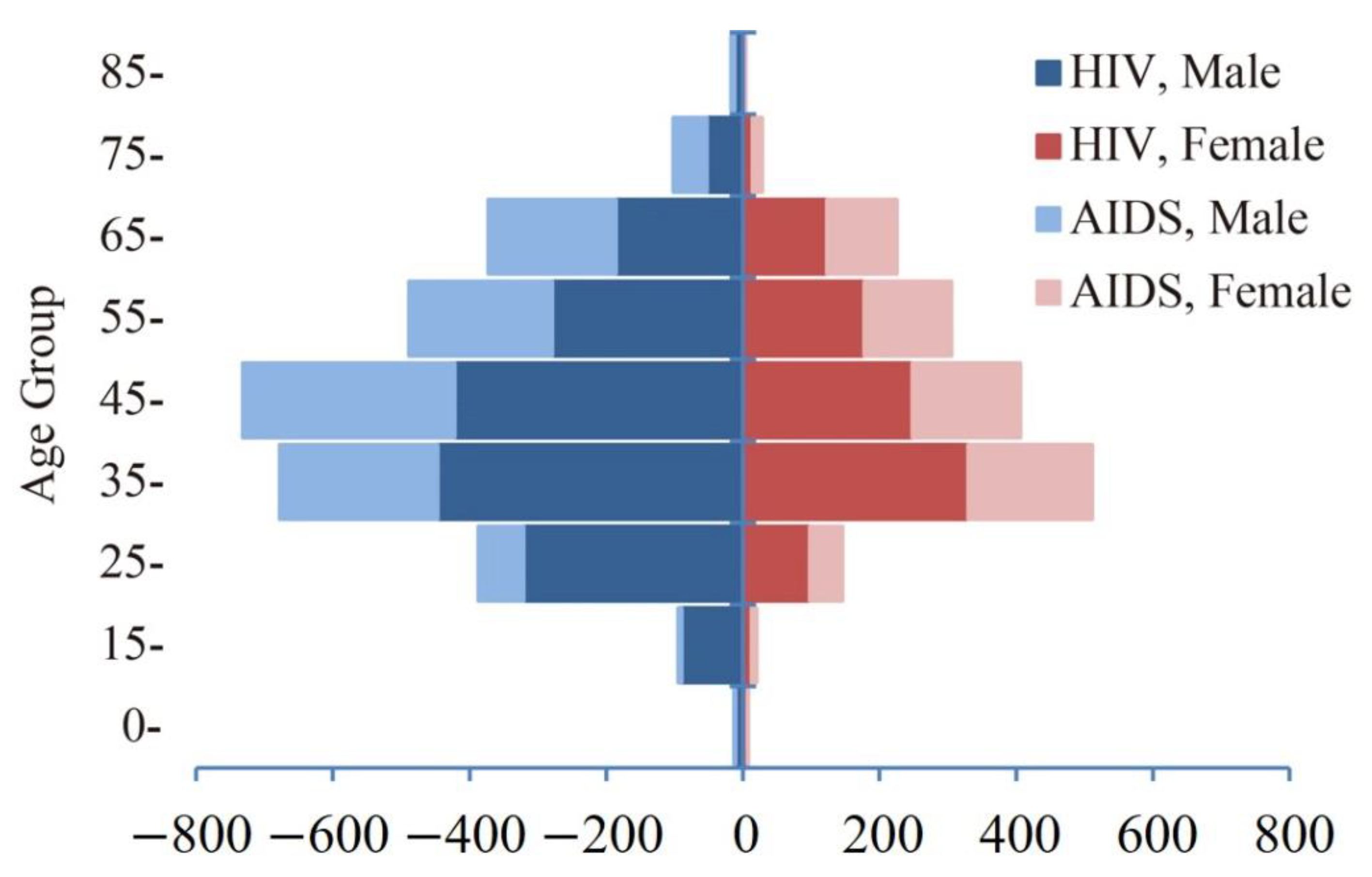
3.2. Demographics
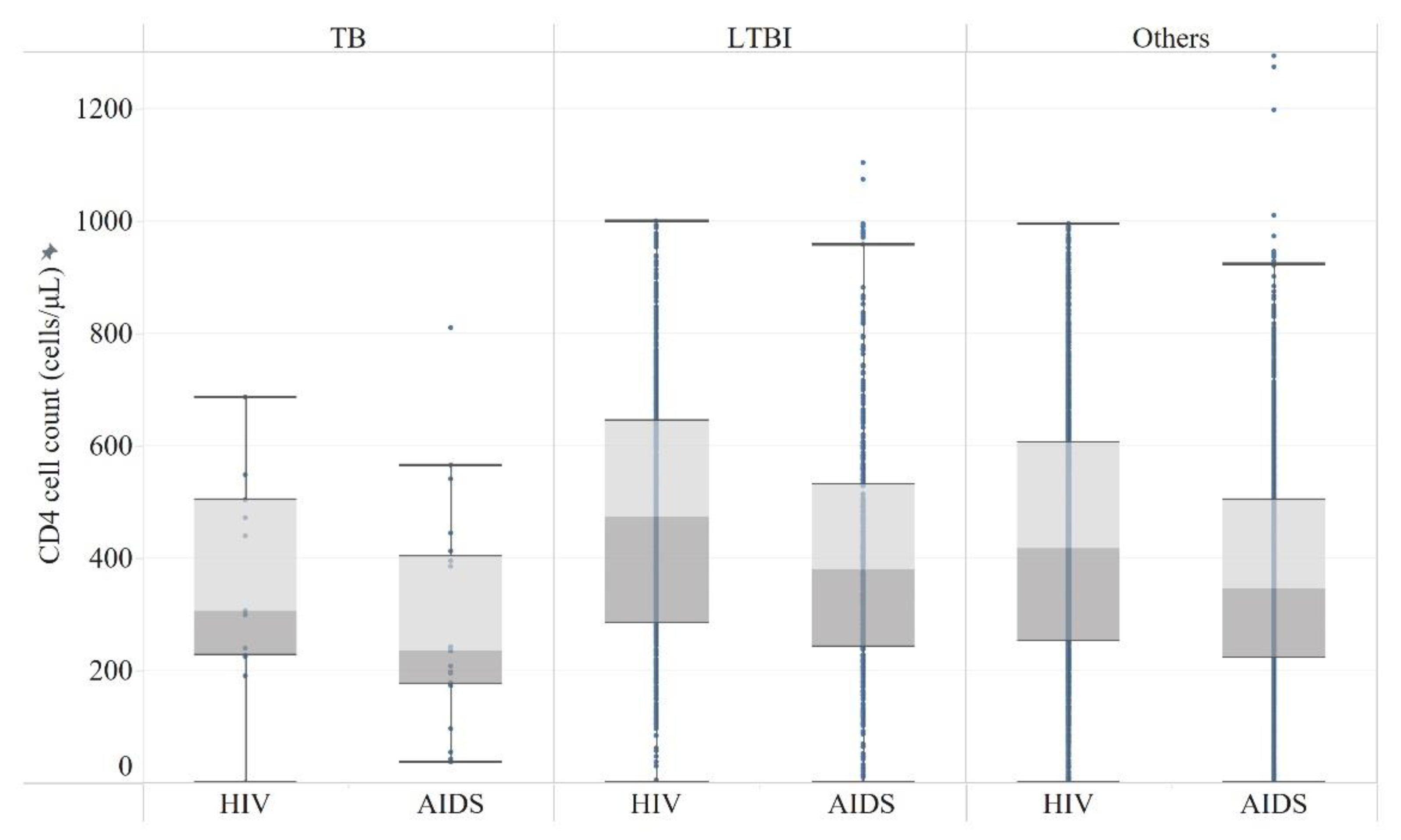
3.3. Clinical Characteristics
4. Discussion
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Age Group | HIV | AIDS | Total | |||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| 0- | 11 | 7 | 2 | 1 | 13 | 8 |
| 15- | 90 | 13 | 5 | 7 | 95 | 20 |
| 25- | 321 | 98 | 66 | 48 | 387 | 146 |
| 35- | 447 | 330 | 231 | 181 | 678 | 511 |
| 45- | 422 | 248 | 310 | 158 | 732 | 406 |
| 55- | 279 | 178 | 210 | 127 | 489 | 305 |
| 65- | 186 | 123 | 187 | 102 | 373 | 225 |
| 75- | 53 | 14 | 49 | 14 | 102 | 28 |
| 85- | 12 | 3 | 5 | 1 | 17 | 4 |
| Total | 1821 | 1014 | 1065 | 639 | 2886 | 1653 |
| Year | TB | LTBI | Others |
|---|---|---|---|
| HIV | 299 (207–487) | 475 (286–645) | 418 (251–605) |
| AIDS | 238 (177–412) | 379 (243–531) | 346 (224–504) |
| Total | 241 (183–458) | 425 (268–606) | 387 (236–568) |
References
- Makam, P.; Matsa, R. “Big Three” Infectious Diseases: Tuberculosis, Malaria and HIV/AIDS. Curr. Top. Med. Chem. 2021, 21, 2779–2799. [Google Scholar] [CrossRef] [PubMed]
- Breton, G.; Duval, X.; Estellat, C.; Poaletti, X.; Bonnet, D.; Mvondo, D.M.; Longuet, P.; Leport, C.; Vildé, J. Determinants of immune reconstitution inflammatory syndrome in HIV type 1-infected patients with tuberculosis after initiation of antiretroviral therapy. Clin. Infect. Dis. 2004, 39, 1709–1712. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.S.; Andrews, J.R.; Hatherill, M.; Hermans, S.; Martinez, L.; Schurr, E.; van der Heijden, Y.; Wood, R.; Rustomjee, R.; Kana, B.D. Advances in the understanding of Mycobacterium tuberculosis transmission in HIV-endemic settings. Lancet Infect. Dis. 2019, 19, e65–e76. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Wang, L.; Zhang, H.; Ruan, Y.; Chin, D.P.; Xia, Y.; Cheng, S.; Chen, M.; Zhao, Y.; Jiang, S.; Du, X.; et al. Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data. Lancet 2014, 383, 2057–2064. [Google Scholar] [CrossRef]
- Hou, Y.; Liu, J.; Zhao, Y.; Wu, Y.; Ma, Y.; Zhao, D.; Dou, Z.; Liu, Z.; Shi, M.; Jiao, Y.; et al. Epidemiological trends of severely immunosuppressed people living with HIV at time of starting antiretroviral treatment in China during 2005–2018. J. Infect. 2022, 84, 400–409. [Google Scholar] [CrossRef]
- Lai, J.; Jiang, Z.; Zhang, H.; Wei, W.; Li, X.; Zhou, O.; Wang, G.; Yang, Y.; Han, J.; Liang, H.; et al. Predictive factors of ART adherence in people living with HIV in Guangxi, China: A retrospective cross-sectional study. AIDS Care 2021, 1243–1248. [Google Scholar] [CrossRef]
- Zhu, Y.; Wu, J.; Feng, X.; Chen, H.; Lu, H.; Chen, L.; Luo, L.; Rui, C. Patient characteristics and perceived health status of individuals with HIV and tuberculosis coinfection in Guangxi, China. Medicine 2017, 96, e6475. [Google Scholar] [CrossRef]
- Walzl, G.; McNerney, R.; du Plessis, N.; Bates, M.; McHugh, T.D.; Chegou, N.N.; Zumla, A. Tuberculosis: Advances and challenges in development of new diagnostics and biomarkers. Lancet Infect. Dis. 2018, 18, e199–e210. [Google Scholar] [CrossRef]
- Cui, Z.; Lin, M.; Nie, S.; Lan, R. Risk factors associated with Tuberculosis (TB) among people living with HIV/AIDS: A pair-matched case-control study in Guangxi, China. PLoS ONE 2017, 12, e0173976. [Google Scholar] [CrossRef]
- Zhang, C.; Li, X.; Liu, Y.; Qiao, S.; Chen, Y.; Zhou, Y.; Shen, Z. Co-infections of tuberculosis, hepatitis B or C viruses in a cohort of people living with HIV/AIDS in China: Predictors and sequelae. AIDS Care 2017, 29, 974–977. [Google Scholar] [CrossRef]
- Maimaiti, R.; Zhang, Y.; Pan, K.; Mijiti, P.; Wubili, M.; Musa, M.; Andersson, R. High prevalence and low cure rate of tuberculosis among patients with HIV in Xinjiang, China. BMC Infect. Dis. 2017, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-F.; Song, Y.-M.; He, W.-C.; Liu, D.-X.; He, P.; Bao, J.-J.; Wang, X.-Y.; Li, Y.-M.; Zhao, Y.-L. Nontuberculous mycobacteria in China: Incidence and antimicrobial resistance spectrum from a nationwide survey. Infect. Dis. Poverty 2021, 10, 59. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Lu, W.; Bai, L.; Wang, X.; Xu, J.; Catanzaro, A.; Cárdenas, V.; Li, X.; Yang, Y.; Du, J.; et al. Latent tuberculosis infection in rural China: Baseline results of a population-based, multicentre, prospective cohort study. Lancet Infect. Dis. 2015, 15, 310–319. [Google Scholar] [CrossRef]
- Runels, T.; Ragan, E.J.; Ventura, A.S.; Winter, M.R.; White, L.F.; Horsburgh, C.R.; Samet, J.H.; Saitz, R.; Jacobson, K.R. Testing and treatment for latent tuberculosis infection in people living with HIV and substance dependence: A prospective cohort study. BMJ Open 2022, 12, e058751. [Google Scholar] [CrossRef] [PubMed]
- Pawlowski, A.; Jansson, M.; Skold, M.; Rottenberg, M.E.; Kallenius, G. Tuberculosis and HIV co-infection. PLoS Pathog. 2012, 8, e1002464. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on the Management of Latent Tuberculosis Infection; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Badje, A.; Moh, R.; Gabillard, D.; Guehi, C.; Kabran, M.; Ntakpe, J.B.; le Carrou, E.; Kouame, G.M.; Ouattara, E.; Messou, E.; et al. Effect of isoniazid preventive therapy on risk of death in west African, HIV-infected adults with high CD4 cell counts: Long-term follow-up of the Temprano ANRS 12136 trial. Lancet Glob. Health 2017, 5, e1080–e1089. [Google Scholar] [CrossRef]
- Getahun, H.; Kittikraisak, W.; Heilig, C.M.; Corbett, E.L.; Ayles, H.; Cain, K.P.; Grant, A.D.; Churchyard, G.J.; Kimerling, M.; Shah, S.; et al. Development of a standardized screening rule for tuberculosis in people living with HIV in resource-constrained settings: Individual participant data meta-analysis of observational studies. PLoS Med. 2011, 8, e1000391. [Google Scholar] [CrossRef]
- World Health Organization. Lateral Flow Urine Lipoarabinomannan Assay (LF-LAM) for the Diagnosis of Active Tuberculosis in People Living with HIV: Policy Update 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Dhana, A.; Hamada, Y.; Kengne, A.P.; Kerkhoff, A.D.; Rangaka, M.X.; Kredo, T.; Baddeley, A.; Miller, C.; Singh, S.; Hanifa, Y.; et al. Tuberculosis screening among ambulatory people living with HIV: A systematic review and individual participant data meta-analysis. Lancet Infect. Dis. 2022, 22, 507–518. [Google Scholar] [CrossRef]
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis, Module 2: Screening, Systematic Screening for Tuberculosis Disease; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Zeru, M.A. Prevalence and associated factors of HIV-TB co-infection among HIV patients: A retrospective Study. Afr. Health Sci. 2021, 21, 1003–1009. [Google Scholar] [CrossRef]
- Negussie, A.; Debalke, D.; Belachew, T.; Tadesse, F. Tuberculosis co-infection and its associated factors among People living with HIV/AIDS attending antiretroviral therapy clinic in southern Ethiopia: A facility based retrospective study. BMC Res. Notes 2018, 11, 417. [Google Scholar] [CrossRef]
- Martin-Iguacel, R.; Llibre, J.M.; Pedersen, C.; Obel, N.; Stærke, N.B.; Åhsberg, J.; Ørsted, I.; Holden, I.; Kronborg, G.; Mohey, R.; et al. Tuberculosis incidence and mortality in people living with human immunodeficiency virus: A Danish nationwide cohort study. Clin. Microbiol. Infect. 2022, 28, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L. How COVID is derailing the fight against HIV, TB and malaria. Nature 2021, 597, 314. [Google Scholar] [CrossRef] [PubMed]
- Fei, H.; Yinyin, X.; Hui, C.; Ni, W.; Xin, D.; Wei, C.; Tao, L.; Shitong, H.; Miaomiao, S.; Mingting, C.; et al. The impact of the COVID-19 epidemic on tuberculosis control in China. Lancet Reg. Health West Pac. 2020, 3, 100032. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Deng, B.; Rui, J.; Guo, S.B.; Hu, Q.; Chen, Q.; Tang, C.; Zhou, L.; Zhao, Z.; Lin, S.; et al. Epidemiological Characteristics and Transmissibility of Human Immunodeficiency Virus in Nanning City, China, 2001–2020. Front. Public Health 2021, 9, 689575. [Google Scholar] [CrossRef] [PubMed]
- Ejeta, E.; Chala, M.; Arega, G.; Ayalsew, K.; Tesfaye, L.; Birhanu, T.; Disassa, H. Outcome of tuberculosis patients under directly observed short course treatment in western Ethiopia. J. Infect. Dev. Ctries. 2015, 9, 752–759. [Google Scholar] [CrossRef]
- Giri, P.A.; Deshpande, J.D.; Phalke, D.B. Prevalence of Pulmonary Tuberculosis among HIV Positive Patients Attending Antiretroviral Therapy Clinic. N. Am. J. Med. Sci. 2013, 5, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Sabur, N.F.; Esmail, A.; Brar, M.S.; Dheda, K. Diagnosing tuberculosis in hospitalized HIV-infected individuals who cannot produce sputum: Is urine lipoarabinomannan testing the answer? BMC Infect. Dis. 2017, 17, 803. [Google Scholar] [CrossRef]
- Gupta, R.K.; Lucas, S.B.; Fielding, K.L.; Lawn, S.D. Prevalence of tuberculosis in post-mortem studies of HIV-infected adults and children in resource-limited settings: A systematic review and meta-analysis. AIDS 2015, 29, 1987–2002. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zerdali, E.; Nakir, I.Y.; Surme, S.; Sayili, U.; Yildirim, M. Predictors for tuberculosis co-infection in people living with HIV/AIDs. Afr. Health Sci. 2021, 21, 995–1002. [Google Scholar] [CrossRef]
- Suwanpimolkul, G.; Gatechompol, S.; Kawkitinarong, K.; Ueaphongsukkit, T.; Sophonphan, J.; Siriyakorn, N.; Jirajariyavej, S.; Khusuwan, S.; Panarat, P.; Wannalerdsakun, S.; et al. Incidence of active tuberculosis among people living with HIV receiving long-term antiretroviral therapy in high TB/HIV burden settings in Thailand: Implication for tuberculosis preventive therapy. J. Int. AIDS Soc. 2022, 25, e25900. [Google Scholar] [CrossRef] [PubMed]



| Year | Total | Active TB | NTM | LTBI | |||||
|---|---|---|---|---|---|---|---|---|---|
| PTB (%) | EPTB (%) | Total (%) | p Value * | Total (%) | p Value | Total (%) | p Value | ||
| 2019 | 1865 | 22 (88.0) | 3 (12.0) | 25 (1.3) | 0.0005 | 43 (2.3) | <0.0001 | 426 (22.8) | 0.0540 |
| 2020 | 675 | 4 (100.0) | 0 (0.0) | 4 (0.6) | 16 (2.4) | 185 (27.4) | |||
| 2021 | 1999 | 6 (85.7) | 1 (14.3) | 7 (0.4) | 7 (0.4) | 493 (24.7) | |||
| Total | 4539 | 32 (88.9) | 4 (11.1) | 36 (0.8) | 66 (1.5) | 1104 (24.3) | |||
| Factors | Total | Active TB | LTBI | HIV Mono-Infection | |||
|---|---|---|---|---|---|---|---|
| n | p Value | n (%) | p Value | n (%) | p Value | ||
| Gender | 0.0336 | 0.0256 | 0.0082 | ||||
| Male | 2886 (63.6) | 29 (80.6) | 733 (66.4) | 2124 (62.5) | |||
| Female | 1653 (26.4) | 7 (19.4) | 371 (33.6) | 1275 (37.5) | |||
| Age | 0.9212 | 0.8918 | 0.8388 | ||||
| 0- | 21 (0.5) | 0 (0.0) | 4 (0.4) | 17 (0.5) | |||
| 15- | 1837 (40.5) | 13 (36.1) | 440 (39.9) | 1384 (40.7) | |||
| 45- | 1608 (35.4) | 14 (38.9) | 398 (36.1) | 1196 (35.2) | |||
| 60- | 1073 (23.6) | 9 (25.0) | 262 (23.7) | 802 (23.6) | |||
| Marriage | 0.7046 | 0.4471 | 0.4045 | ||||
| Married | 2857 (62.9) | 20 (55.6) | 694 (62.9) | 2143 (63.0) | |||
| Unmarried | 996 (21.9) | 10 (27.8) | 234 (21.2) | 752 (22.1) | |||
| Divorced/widowed | 641 (14.1) | 6 (16.7) | 168 (15.2) | 467 (13.7) | |||
| Unknown | 45 (1.0) | 0 (0.0) | 8 (0.7) | 37 (1.1) | |||
| Education | 0.3496 | 0.0818 | 0.0859 | ||||
| Illiteracy | 321 (7.1) | 3 (8.3) | 77 (7.0) | 241 (7.1) | |||
| Primary school | 1564 (34.5) | 17 (47.2) | 398 (36.1) | 1149 (33.8) | |||
| Junior high school | 1597 (35.2) | 12 (33.3) | 351 (31.8) | 1234 (36.3) | |||
| High school | 586 (12.9) | 3 (8.3) | 157 (14.2) | 426 (12.5) | |||
| Junior college/above | 471 (10.4) | 1 (2.8) | 121 (11.0) | 349 (10.3) | |||
| Occupation | 0.0260 | 0.4583 | 0.5181 | ||||
| Farmer | 2766 (60.9) | 23 (63.9) | 651 (59.0) | 2092 (61.5) | |||
| Self-employed | 759 (16.7) | 2 (5.6) | 198 (17.9) | 559 (16.4) | |||
| Unemployed | 527 (11.6) | 9 (25.0) | 132 (12.0) | 386 (11.4) | |||
| Other | 487 (10.7) | 2 (5.6) | 123 (11.1) | 362 (10.7) | |||
| Factors | Total | Active TB | LTBI | HIV Mono-Infection | |||
|---|---|---|---|---|---|---|---|
| n (%) | p Value | n (%) | p Value | n (%) | p Value | ||
| HIV status | 0.0097 | 0.6446 | 0.9420 | ||||
| HIV infected | 2835 (62.5) | 15 (46.9) | 696 (61.8) | 2124 (62.8) | |||
| AIDS | 1704 (37.5) | 21 (65.6) | 408 (36.2) | 1275 (37.7) | |||
| Comorbidity | 0.0347 | 0.6675 | 0.3915 | ||||
| Yes | 421 (9.3) | 7 (19.4) | 106 (9.6) | 308 (9.1) | |||
| No | 4118 (90.7) | 29 (80.6) | 998 (90.4) | 3091 (90.9) | |||
| Close contact | 0.3555 | 0.7313 | 0.6305 | ||||
| Yes | 157 (3.5) | 2 (5.6) | 40 (3.6) | 115 (3.4) | |||
| No | 4382 (96.5) | 34 (94.4) | 1064 (96.4) | 3284 (96.6) | |||
| Nine Symptoms | 0.0052 | 0.6504 | 0.8098 | ||||
| Yes | 276 (6.1) | 7 (19.4) | 64 (5.8) | 205 (6) | |||
| No | 4263 (93.9) | 29 (80.6) | 1040 (94.2) | 3194 (94) | |||
| W4SS * | 0.0728 | 0.8812 | 0.8007 | ||||
| Yes | 201 (4.4) | 4 (11.1) | 48 (4.3) | 149 (4.4) | |||
| No | 4338 (95.6) | 32 (88.9) | 1056 (95.7) | 3250 (95.6) | |||
| Chest x-ray | <0.0001 | 0.4773 | 0.0886 | ||||
| Abnormal | 997 (22) | 20 (55.6) | 251 (22.7) | 726 (21.4) | |||
| Normal | 3542 (78) | 16 (44.4) | 853 (77.3) | 2673 (78.6) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Z.; Huang, F.; Liang, D.; Huang, Y.; Qin, H.; Ye, J.; Huang, L.; Zhou, C.; Huang, M.; Liang, X.; et al. Tuberculosis among Ambulatory People Living with HIV in Guangxi Province, China: A Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 12280. https://doi.org/10.3390/ijerph191912280
Cui Z, Huang F, Liang D, Huang Y, Qin H, Ye J, Huang L, Zhou C, Huang M, Liang X, et al. Tuberculosis among Ambulatory People Living with HIV in Guangxi Province, China: A Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12280. https://doi.org/10.3390/ijerph191912280
Chicago/Turabian StyleCui, Zhezhe, Fei Huang, Dabin Liang, Yan Huang, Huifang Qin, Jing Ye, Liwen Huang, Chongxing Zhou, Minying Huang, Xiaoyan Liang, and et al. 2022. "Tuberculosis among Ambulatory People Living with HIV in Guangxi Province, China: A Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 19: 12280. https://doi.org/10.3390/ijerph191912280
APA StyleCui, Z., Huang, F., Liang, D., Huang, Y., Qin, H., Ye, J., Huang, L., Zhou, C., Huang, M., Liang, X., Long, F., Zhao, Y., & Lin, M. (2022). Tuberculosis among Ambulatory People Living with HIV in Guangxi Province, China: A Longitudinal Study. International Journal of Environmental Research and Public Health, 19(19), 12280. https://doi.org/10.3390/ijerph191912280