

Managing the Wellbeing of Elite Rugby Union Players from an Occupational Safety and Health Perspective



Abstract
1. Introduction
Theoretical Framework
Safety Culture from OSH Perspective
2. Materials and Methods
2.1. Participants
2.2. Study Chronology
2.2.1. Data Collection
2.2.2. Data Analysis
2.3. Trustworthiness
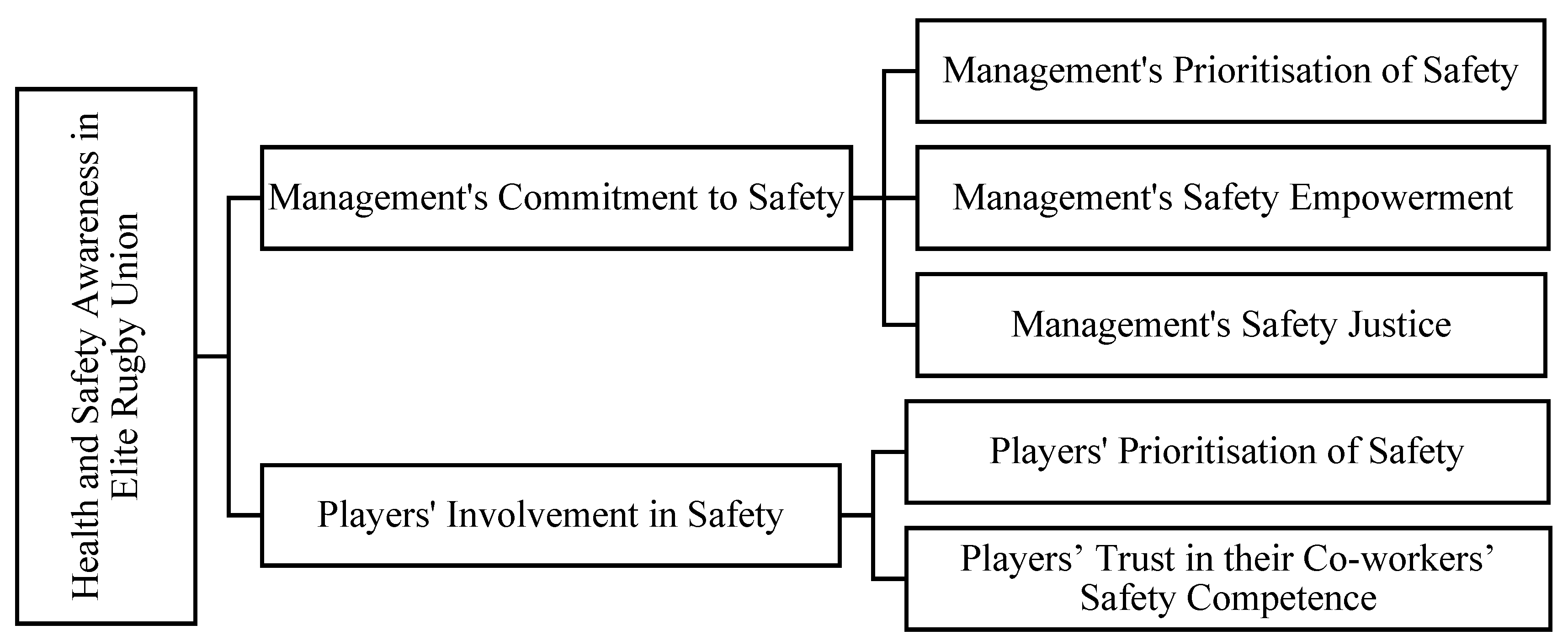
3. Results
3.1. Management’s Commitment to Safety
3.1.1. Management’s Prioritization of Safety
“It’s monitored, say somebody’s appetite is always 10 out of 10, and suddenly drops to six; an alert will pop up. If their sit-and-reach is normally 10 centimetres and suddenly drops to five, an alert pops up and physios are called straight over. Maybe we’ll look at them [the player] to try to pre-empt injury.”(Med12)
“At the start of the season, our doctors and physios hold a meeting to decide on the procedures that will be implemented in different situations, then communicated between coaches”.
“IRFU try to manage somebody across the whole season, and say nobody can play every game. ‘How many games can we get this person to play, so they are healthy at the end of it?’ I think that’s something very important that other countries and unions don’t necessarily do”.
“Then, after games, I go chat to the players who played, see if anyone’s picked up any knocks [injuries] that they didn’t mention, during the game”.
“Obviously, the pressure of sports probably gets rugby coaches to put the medical staff under a bit of pressure, especially with the one-of-a-kind main player that they need in the squad on a certain weekend. But I think that’s probably natural, in this sport.”(Coach6)
3.1.2. Management’s Safety Empowerment
“If I substituted every player with any sign of injury, there would be a lot of changes during a game. But, I’m giving them opportunity to prove they’re okay to continue to play. And they respect that, when it comes to making big decisions”.
“We try and maintain that relationship, and have professional interactions with them so that they see that we are professionals, not just some friends, we are trained professional people giving you what we believe is good advice”.
“It’s a tricky area. Obviously, player-to-coach is a critical relationship in terms of building a team. It’s different because, you’re thinking, ‘if I say this to the coach, will he think that I’m soft?’ Or ‘will he think that I’m weak?’ Or, ‘will he think that this is a real injury or that I’m looking for an easy way out?’”(Coach11)
3.1.3. Management’s Safety Justice
“From a referee’s perspective, one of our primary concerns is the health, safety, and wellbeing of a player. If something happens within the game, the correct reaction must be taken; even stopping the game in certain circumstances. If a referee doesn’t spot in advance, if an act of foul play is committed, depending on the severity of the act of foul play, the referee should react in an appropriate way by either sanctioning a yellow card or sanctioning a red card. And although that doesn’t stop the event taking place, we can prevent further events taking place.”(Mgt10)
“Refereeing in rugby is hugely challenging, be it amateur or professional. It’s a hugely intelligent game, because the laws, in some instances… are quite black-and-white, but in other instances, grey. The challenge for referees is to find the black-and-white in… a grey situation.”(Mgt10)
“The perfect case is Danny Cipriani, playing for Gloucester against Munster two months ago. So there are a lot of decisions that the referees are trying to make… but the changes are hard to make”.
3.2. Players’ Involvement in Safety
3.2.1. Players’ Prioritisation of Safety
“Injury has a bigger impact than just missing a couple of training days. You’ve got the mental side of it too. Because it troubles you, makes you think… if you’re going to feel down, you’re not going to be happy about things, and it’ll affect you in other ways.”(Coach11)
“Someone has a niggling injury… may not be comfortable playing with it. Others maybe have a higher pain threshold or are prepared to train with a little bit of discomfort”.
“You develop mutual trust… when you know players, they are honest with you and tell you how it is. When you don’t have that relationship with players, with health and safety, it’s very difficult to figure out whether that person is okay”.
“instead of relying solely on players and physiotherapists to ensure health and safety-awareness, all staff in the organisation should contribute to decisions regarding players”.
“I think part of that is the culture of the club. Outcomes can take a second place to player welfare for us. I think some of the barriers to implementing health and safety or welfare, I suppose the pressure on outcomes might be greater, there’s a player-welfare-focussed or performance-focussed judgement. If there’s pressure to perform, player welfare can be put to one side or pushed away.”(Mgt2)
“they don’t want to be seen to be the weak one. They want to be seen to be as good or as healthy as the next guy.”(Mgt7)
“I think it’s just the pressure, like the pressure to keep your position and contract. You’re publicly exposed, it’s a competitive situation. People out there, they might have been in the same year in college, and they’re becoming qualified accountants, and they’re starting to make some money, but you’re not.”(Coach6)
“I think it’s because it’s sports, and your decision to play is by your contract, might actually be if you’re getting closer to contract negotiations, and you know you can play through injury, and cover up an injury as much as possible.”(Coach6)
“The more competitions you win, the bigger the cash bonus or wage bonus is. Now, a lot of those players will say they love playing the game, and they’re not really worried about the cash. That’s not true, because their career is only 15 years at most, it’s probably less. They only have that period of time to amass as much income as they can. Earnings would be in the region of €300,000. Basically, that’s a lot of money for a 22- or 23-year-old player.”(Mgt7)
“A player might have a career that’s 10, 15 years, whereas I might have a career in an office job for 40 or 50 years. So, missing time through ill-health is much more significant for players”.
3.2.2. Players’ Trust in Their Co-Workers’ Safety Competence
“I suppose, if you take contact as a major issue, I think tackle technique is important. If you see someone tackling with their head across, and the person is hit… that can be a disaster. And you may see a lot of shoulder injuries by someone who is actually tackling passively.”(Med5)
“It’s quite unique in a situation when those players come in, because they may be playing, passing the ball, to someone who’s never played rugby like that before. So you’ve got the elite of the elite, and… amateurs play with them”.
“Players, who know each other will often be more brave, be very aggressive with someone. But, if they don’t know the other person that well on a foreign team or another club, they might be a little bit reserved and sometimes coaches will have a small part of a training session during the week of a big game. They will say, ‘we’re going to go full metal jacket’. And that means that there are very few rules and people just get barbaric.”(Coach15)
“Every week you have rugby players play for Ireland, but next week in the league they’re playing on opposite teams, so they play against each other all the time. So, it’s difficult to be overly aggressive with your team, with your Ireland teammates. Your teammate is there, but the following week [he] could be your opposition, the opposition player.”(Mgt7)
“I don’t think any of those players would want to injure another player. But I have seen in Irish training sessions where one group of forwards will go against another group of forwards, and some of the players will almost try to injure their own teammates because they might get selected.”(Coach15)
4. Managerial Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Protocol

References
- Schroeder, P. A model for assessing organizational culture in intercollegiate athletics. J. Issues Intercoll. Athl. 2010, 3, 98–118. [Google Scholar]
- Chen, Y.; Kelly, S.; Buggy, C. Evaluating safety and risk awareness in contact sports: Development of a quantitative survey for elite rugby. Int. J. Occup. Environ. Saf. 2022, 6, 26–40. [Google Scholar] [CrossRef]
- Williams, S.; Trewartha, G.; Kemp, S.; Stokes, K. A Meta-Analysis of Injuries in Senior Men’s Professional Rugby Union. Sports Med. 2013, 43, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, R.; Liston, M.; Comyns, T.; Kenny, I.; Cahalan, R.; Campbell, M.; Glynn, L.; Harrison, D.; Hayes, K.; Lyons, M.; et al. The Irish Rugby Injury Surveillance Project All-Ireland League Rugby. 2018. [Google Scholar]
- Chen, Y.; Buggy, C.; Kelly, S. Winning at all costs: A review of risk-taking behaviour and sporting injury from an occupational safety and health perspective. Sports Med.—Open 2019, 5, 15. [Google Scholar] [CrossRef]
- Nixon, H.L. A Social Network Analysys of Influences on Athletes to Play with Pain and Injuries. J. Sport Soc. Issues 1992, 16, 127–135. [Google Scholar] [CrossRef]
- Nixon, H.L. Social Network Analysis of Sport: Emphasizing Social Structure in Sport Sociology. Sociol. Sport J. 2016, 10, 315–321. [Google Scholar] [CrossRef]
- Maxwell, J.P.; Visek, A.J. Unsanctioned aggression in rugby union: Relationships among aggressiveness, anger, athletic identity, and professionalization. Aggress. Behav. 2009, 35, 237–243. [Google Scholar] [CrossRef]
- Haslam, C.; O’Hara, J.; Kazi, A.; Twumasi, R.; Haslam, R. Proactive occupational safety and health management: Promoting good health and good business. Saf. Sci. 2016, 81, 99–108. [Google Scholar] [CrossRef]
- Piggin, J.; Pollock, A. World Rugby’s erroneous and misleading representation of Australian sports’ injury statistics. Br. J. Sports Med. 2016, 51, 1108. [Google Scholar] [CrossRef]
- Lisinskiene, A.; Lochbaum, M. The Coach–Athlete–Parent Relationship: The Importance of the Sex, Sport Type, and Family Composition. Int. J. Environ. Res. Public Health 2022, 19, 4821. [Google Scholar] [CrossRef]
- Chen, Y.; Kelly, S.; Buggy, C.J. Considering Occupational Safety Awareness in Elite Rugby: A Game of Near- Misses. J. Interdiscip. Sci. 2021, 5, 1–31. [Google Scholar]
- Li, F.; Adrien, N.; He, Y. Biomechanical Risks Associated with Foot and Ankle Injuries in Ballet Dancers: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 4916. [Google Scholar] [CrossRef] [PubMed]
- Gamble, P. Physical Preparation for Elite-Level Rugby Union Football. Strength Cond. J. 2004, 26, 10–23. [Google Scholar] [CrossRef]
- Quarrie, K.L.; Hopkins, W.G. Tackle Injuries in Professional Rugby Union. Am. J. Sports Med. 2008, 36, 1705–1716. [Google Scholar] [CrossRef] [PubMed]
- Malcolm, D. Unprofessional Practice? The Status and Power of Sport Physicians. Sociol. Sport J. 2006, 23, 376–395. [Google Scholar] [CrossRef]
- Howe, P.D. An ethnography of pain and injury in professional rugby union: The Case of Pontypridd RFC. Int. Rev. Sociol. Sport 2001, 36, 289–303. [Google Scholar] [CrossRef]
- Kroshus, E.; Garnett, B.; Hawrilenko, M.; Baugh, C.M.; Calzo, J.P. Concussion under-reporting and pressure from coaches, teammates, fans, and parents. Soc. Sci. Med. 2015, 134, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Jackson, S. Competing loyalties in sports medicine: Threats to medical professionalism in elite, commercial sport. Int. Rev. Sociol. Sport 2013, 48, 238–256. [Google Scholar] [CrossRef]
- De Bosscher, V.; Shilbury, D.; Theeboom, M.; Van Hoecke, J.; De Knop, P. Effectiveness of National Elite Sport Policies: A Multidimensional Approach Applied to the Case of Flanders. Eur. Sport Manag. Q. 2011, 11, 115–141. [Google Scholar] [CrossRef]
- Sotiriadou, P.; De Bosscher, V. Managing high-performance sport: Introduction to past, present and future considerations. Eur. Sport Manag. Q. 2017, 18, 1–7. [Google Scholar] [CrossRef]
- Kearney, P.E.; See, J. Misunderstandings of concussion within a youth rugby population. J. Sci. Med. Sport 2017, 20, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Posthumus, M.; Viljoen, W. BokSmart: Safe and effective techniques in rugby union. S. Afr. J. Sports Med. 2008, 20, 64–69. [Google Scholar] [CrossRef]
- Van Mechelen, W.; Hlobil, H.; Kemper, H.C.G. Incidence, Severity, Aetiology and Prevention of Sports Injuries. A review of concepts. Sports Med. 1992, 14, 82–99. [Google Scholar] [CrossRef]
- Donaldson, A.; Borys, D.; Finch, C.F. Understanding safety management system applicability in community sport. Saf. Sci. 2013, 60, 95–104. [Google Scholar] [CrossRef]
- Coffey, N.; Lawless, M.; Kelly, S.; Buggy, C. Frequency of self-reported concussion amongst professional and semi-professional footballers in Ireland during the 2014 season: A cross-sectional study. Sports Med.-Open 2018, 4, 1–8. [Google Scholar] [CrossRef]
- Guldenmund, F.W. (Mis)understanding Safety Culture and Its Relationship to Safety Management. Risk Anal. 2010, 30, 1466–1480. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, J.; Alvesson, M. Ways of constructing research questions: Gap-spotting or problematization? Organization 2011, 18, 23–44. [Google Scholar] [CrossRef]
- Cooper, M. Towards a model of safety culture. Saf. Sci. 2000, 36, 111–136. [Google Scholar] [CrossRef]
- Zohar, D. Safety climate in industrial organizations: Theoretical and applied implications. J. Appl. Psychol. 1980, 65, 96–102. [Google Scholar] [CrossRef]
- Cox, S.; Flin, R. Safety culture: Philosopher’s stone or man of straw? Work Stress 1998, 12, 189–201. [Google Scholar] [CrossRef]
- Brown, R.; Holmes, H. The use of a factor-analytic procedure for assessing the validity of an employee safety climate model. Accid. Anal. Prev. 1986, 18, 455–470. [Google Scholar] [CrossRef]
- Pousette, A.; Larsson, S.; Törner, M. Safety climate cross-validation, strength and prediction of safety behaviour. Saf. Sci. 2008, 46, 398–404. [Google Scholar] [CrossRef]
- Reason, J. Managing the Risks of Organizational Accidents, 1st ed.; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar] [CrossRef]
- Clarke, S.; Ward, K. The Role of Leader Influence Tactics and Safety Climate in Engaging Employees’ Safety Participation. Risk Anal. 2006, 26, 1175–1185. [Google Scholar] [CrossRef]
- Törner, M.; Pousette, A. Safety in construction—A comprehensive description of the characteristics of high safety standards in construction work, from the combined perspective of supervisors and experienced workers. J. Saf. Res. 2009, 40, 399–409. [Google Scholar] [CrossRef]
- Kines, P.; Lappalainen, J.; Mikkelsen, K.L.; Olsen, E.; Pousette, A.; Tharaldsen, J.; Tómasson, K.; Törner, M. Nordic Safety Climate Questionnaire (NOSACQ-50): A new tool for diagnosing occupational safety climate. Int. J. Ind. Ergon. 2011, 41, 634–646. [Google Scholar] [CrossRef]
- Alsarve, D. The need for a violence prevention programme in ice hockey: A case study on how hegemonic masculinity supports and challenges violent behaviour in Swedish ice hockey. Eur. Sport Manag. Q. 2020, 21, 218–236. [Google Scholar] [CrossRef]
- Malcom, N.L. “Shaking It Off” and “Toughing It Out”. J. Contemp. Ethnogr. 2006, 35, 495–525. [Google Scholar] [CrossRef]
- Coupland, C. Organizing masculine bodies in rugby league football: Groomed to fail. Organization 2014, 22, 793–809. [Google Scholar] [CrossRef]
- Curry, T.J. A Little Pain Never Hurt Anyone: Athletic Career Socialization and the Normalization of Sports Injury. Symb. Interact. 1993, 16, 273–290. [Google Scholar] [CrossRef]
- Hughes, R.; Coakley, J. Positive Deviance among Athletes: The Implications of Overconformity to the Sport Ethic. Sociol. Sport J. 1991, 8, 307–325. [Google Scholar] [CrossRef]
- Malcolm, D. Cricket and Civilizing Processes: A Response to Stokvis. Int. Rev. Sociol. Sport 2002, 37, 37–57. [Google Scholar] [CrossRef]
- Safai, P. Healing the Body in the “Culture of Risk”: Examining the Negotiation of Treatment between Sport Medicine Clinicians and Injured Athletes in Canadian Intercollegiate Sport. Sociol. Sport J. 2003, 20, 127–146. [Google Scholar] [CrossRef]
- Walk, S.R. Peers in Pain: The Experiences of Student Athletic Trainers. Sociol. Sport J. 1997, 14, 22–56. [Google Scholar] [CrossRef]
- Waddington, I. Ethical Problems in the Medical Management of Sports Injuries: A Case Study of English Professional Football. In Pain and Injury in Sport: Social and Ethical Analysis; Loland, S., Skirstad, B., Waddington, I., Eds.; Routledge: London, UK; New York, NY, USA,, 2006; pp. 182–199. [Google Scholar]
- Safai, P. Negotiating with Risk: Exploring the Role of the Sport Medicine Clinician. In Sports Bodies, Damaged Selves: Sociological Studies of Sports-Related Injury; Young, K., Ed.; Elsevier: Oxford, UK, 2004; pp. 269–286. [Google Scholar] [CrossRef]
- Malcolm, D. Medical Uncertainty and Clinician–Athlete Relations: The Management of Concussion Injuries in Rugby Union. Sociol. Sport J. 2009, 26, 191–210. [Google Scholar] [CrossRef]
- Roderick, M.; Waddington, I.; Parker, G. PLAYING HURT: Managing Injuries in English Professional Football. Int. Rev. Sociol. Sport 2000, 35, 165–180. [Google Scholar] [CrossRef]
- Theberge, N. The Gendering of Sports Injury: A Look at ‘Progress’ in Women’s Sport through a Case Study of the Biomedical Discourse on the Injured Athletic Body. Sport Soc. 2006, 9, 634–648. [Google Scholar] [CrossRef]
- Murray, I.R.; Murray, A.D.; Robson, J. Sports Concussion. Clin. J. Sport Med. 2015, 25, 75–77. [Google Scholar] [CrossRef]
- Fraas, M.R.; Coughlan, G.F.; Hart, E.C.; McCarthy, C. Concussion knowledge and management practices among coaches and medical staff in Irish professional rugby teams. Ir. J. Med Sci. 2015, 184, 425–430. [Google Scholar] [CrossRef]
- Yung, K.K.; Ardern, C.L.; Serpiello, F.R.; Robertson, S. A Framework for Clinicians to Improve the Decision-Making Process in Return to Sport. Sports Med.—Open 2022, 8, 52. [Google Scholar] [CrossRef]
- Smith, B. Generalizability in qualitative research: Misunderstandings, opportunities and recommendations for the sport and exercise sciences. Qual. Res. Sport Exerc. Health 2017, 10, 137–149. [Google Scholar] [CrossRef]
- Sparkes, A.C.; Smith, B. Qualitative Research Methods in Sport, Exercise and Health: From Process to Product; Routledge: London, UK, 2013. [Google Scholar] [CrossRef]
- Skinner, J.; Edwards, A.; Smith, A.C. Qualitative Research in Sport Management; Routledge: London, UK, 2020. [Google Scholar] [CrossRef]
- Parry, A. Handbook of Qualitative Research, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2000. [Google Scholar] [CrossRef]
- Fletcher, A.J. Applying critical realism in qualitative research: Methodology meets method. Int. J. Soc. Res. Methodol. 2016, 20, 181–194. [Google Scholar] [CrossRef]
- Baker, J.F.; Devitt, B.M.; Green, J.; McCarthy, C. Concussion among under 20 rugby union players in Ireland: Incidence, attitudes and knowledge. Ir. J. Med Sci. 2013, 182, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Noy, C. Sampling Knowledge: The Hermeneutics of Snowball Sampling in Qualitative Research. Int. J. Soc. Res. Methodol. 2008, 11, 327–344. [Google Scholar] [CrossRef]
- Skinner, J.; Smith, A.C.T. Introduction: Sport and COVID-19: Impacts and challenges for the future (Volume 1). Eur. Sport Manag. Q. 2021, 21, 323–332. [Google Scholar] [CrossRef]
- Smith, B.; McGannon, K. Developing rigor in qualitative research: Problems and opportunities within sport and exercise psychology. Int. Rev. Sport Exerc. Psychol. 2016, 11, 101–121. [Google Scholar] [CrossRef]
- Chen, Y.; Kelly, S.; Buggy, C.J. Protecting the Health and Wellbeing of Rugby Players and Support Staff from an Occupational Safety and Health Perspective during Return to Play in A Global Pandemic. J. Sports Med. Orthop. Adv. 2021, 1, 5–13. Available online: https://researchrepository.ucd.ie/handle/10197/12141 (accessed on 15 August 2022).
- Eeckelaert, L.; Starren, A.; van Scheppingen, A.; Fox, D.; Bruck, C. Occupational Safety and Health Culture Assessment—A Review of main Approaches and Selected Tools; European Agency for Safety and Health at Work: Brussels, Belgium, 2011; pp. 1–79. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Tuckett, A.G. Applying thematic analysis theory to practice: A researcher’s experience. Contemp. Nurse 2005, 19, 75–87. [Google Scholar] [CrossRef]
- McGrath, C.; Palmgren, P.J.; Liljedahl, M. Twelve tips for conducting qualitative research interviews. Med Teach. 2018, 41, 1002–1006. [Google Scholar] [CrossRef]
- Downward, P.; Mearman, A. Critical Realism and Econometrics: Constructive Dialogue with Post Keynesian Economics. Metroeconomica 2002, 53, 391–415. [Google Scholar] [CrossRef]
- Huang, Y.-H.; Sinclair, R.R.; Lee, J.; McFadden, A.C.; Cheung, J.H.; Murphy, L.A. Does talking the talk matter? Effects of supervisor safety communication and safety climate on long-haul truckers’ safety performance. Accid. Anal. Prev. 2018, 117, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Drew, M.K.; Cook, J.; Finch, C.F. Sports-related workload and injury risk: Simply knowing the risks will not prevent injuries: Narrative review. Br. J. Sports Med. 2016, 50, 1306–1308. [Google Scholar] [CrossRef] [PubMed]
- Mooney, A. (Ed.) Contemporary Developments in Games Teaching; Routledge: New York, NY, USA; London, UK, 2013. [Google Scholar] [CrossRef]
- Collins, C.L.; Fields, S.K.; Comstock, R.D. When the rules of the game are broken: What proportion of high school sports-related injuries are related to illegal activity? Inj. Prev. 2008, 14, 34–38. [Google Scholar] [CrossRef]
- Fuller, C.W.; Ashton, T.; Brooks, J.H.M.; Cancea, R.J.; Hall, J.; Kemp, S. Injury risks associated with tackling in rugby union. Br. J. Sports Med. 2008, 44, 159–167. [Google Scholar] [CrossRef]
- Beardmore, A.L.; Handcock, P.J.; Rehrer, N.J. Return-to-play after injury: Practices in New Zealand rugby union. Phys. Ther. Sport 2005, 6, 24–30. [Google Scholar] [CrossRef]
- Fuller, C.W.; Molloy, M.G.; Bagate, C.; Bahr, R.; Brooks, J.H.M.; Donson, H.; Kemp, S.P.T.; McCrory, P.; McIntosh, A.S.; Meeuwisse, W.H.; et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br. J. Sports Med. 2007, 41, 328–331. [Google Scholar] [CrossRef]
- Gianotti, S.M.; Quarrie, K.L.; Hume, P.A. Evaluation of RugbySmart: A rugby union community injury prevention programme. J. Sci. Med. Sport 2009, 12, 371–375. [Google Scholar] [CrossRef]
- Trewartha, G.; Preatoni, E.; England, M.E.; Stokes, K.A. Injury and biomechanical perspectives on the rugby scrum: A review of the literature. Br. J. Sports Med. 2014, 49, 425–433. [Google Scholar] [CrossRef]
- Clutterbuck, D.A.; Kochan, F.K.; Lunsford, L. (Eds.) Mentoring Irish Rugby Players for Life After Rugby; SAGE: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Green, M.; Oakley, B. Elite sport development systems and playing to win: Uniformity and diversity in international approaches. Leis. Stud. 2001, 20, 247–267. [Google Scholar] [CrossRef]
- Sun, Y.; Xu, L.; Shao, H.; Wang, H. China’s laws, rights, and administrative structures in occupational safety and health: A comparison with the United States. J. Public Health Policy 2014, 35, 455–469. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Participant Pseudonym | Position Involved | Team Level (Highest) | Employment Type | Age Group | Gender | Elite Playing Experience |
|---|---|---|---|---|---|---|
| Mgt1 | Management | Provincial | Full-time | 50–60 | M | Yes |
| Mgt2 | Management | Provincial | Full-time | 30–40 | M | Yes |
| Med3 | Medical staff | National | Full-time | 30–40 | M | No |
| Med4 | Medical staff | AIL 1A | Part-time | 20–30 | M | Yes |
| Med5 | Medical staff | AIL 1A | Part-time | 30–40 | M | No |
| Coach6 | Coaching staff | Provincial | Part-time | 20–30 | M | Yes |
| Mgt7 | Management | AIL 1A | Full-time | 50–60 | M | Yes |
| Coach8 | Coaching staff | AIL 1A | Part-time | 20–30 | M | Yes |
| Coach9 | Coaching staff | AIL 1A | Part-time | 40–50 | M | Yes |
| Mgt10 | Management | National | Full-time | 40–50 | M | No |
| Coach11 | Coaching staff | National | Full-time | 20–30 | M | Yes |
| Med12 | Medical staff | National | Full-time | 30–40 | F | No |
| Med13 | Medical staff | National | Full-time | 50–60 | M | No |
| Coach14 | Coaching staff | National | Full-time | 30–40 | M | Yes |
| Coach15 | Coaching staff | National | Full-time | 40–50 | M | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Buggy, C.; Kelly, S. Managing the Wellbeing of Elite Rugby Union Players from an Occupational Safety and Health Perspective. Int. J. Environ. Res. Public Health 2022, 19, 12229. https://doi.org/10.3390/ijerph191912229
Chen Y, Buggy C, Kelly S. Managing the Wellbeing of Elite Rugby Union Players from an Occupational Safety and Health Perspective. International Journal of Environmental Research and Public Health. 2022; 19(19):12229. https://doi.org/10.3390/ijerph191912229
Chicago/Turabian StyleChen, Yanbing, Conor Buggy, and Seamus Kelly. 2022. "Managing the Wellbeing of Elite Rugby Union Players from an Occupational Safety and Health Perspective" International Journal of Environmental Research and Public Health 19, no. 19: 12229. https://doi.org/10.3390/ijerph191912229
APA StyleChen, Y., Buggy, C., & Kelly, S. (2022). Managing the Wellbeing of Elite Rugby Union Players from an Occupational Safety and Health Perspective. International Journal of Environmental Research and Public Health, 19(19), 12229. https://doi.org/10.3390/ijerph191912229