
Developing a Cold-Related Mortality Database in Bangladesh



Abstract
:1. Introduction
- develop a comprehensive database on division-wise cold-related mortality in Bangladesh during the winter months of 2009–2021 using information from online national newspapers and available reports;
- find a relationship between mortality and the drift of winter temperatures; and
- determine the spatiotemporal variability and demographic dynamics of cold-related mortality in Bangladesh.
2. Materials and Methods
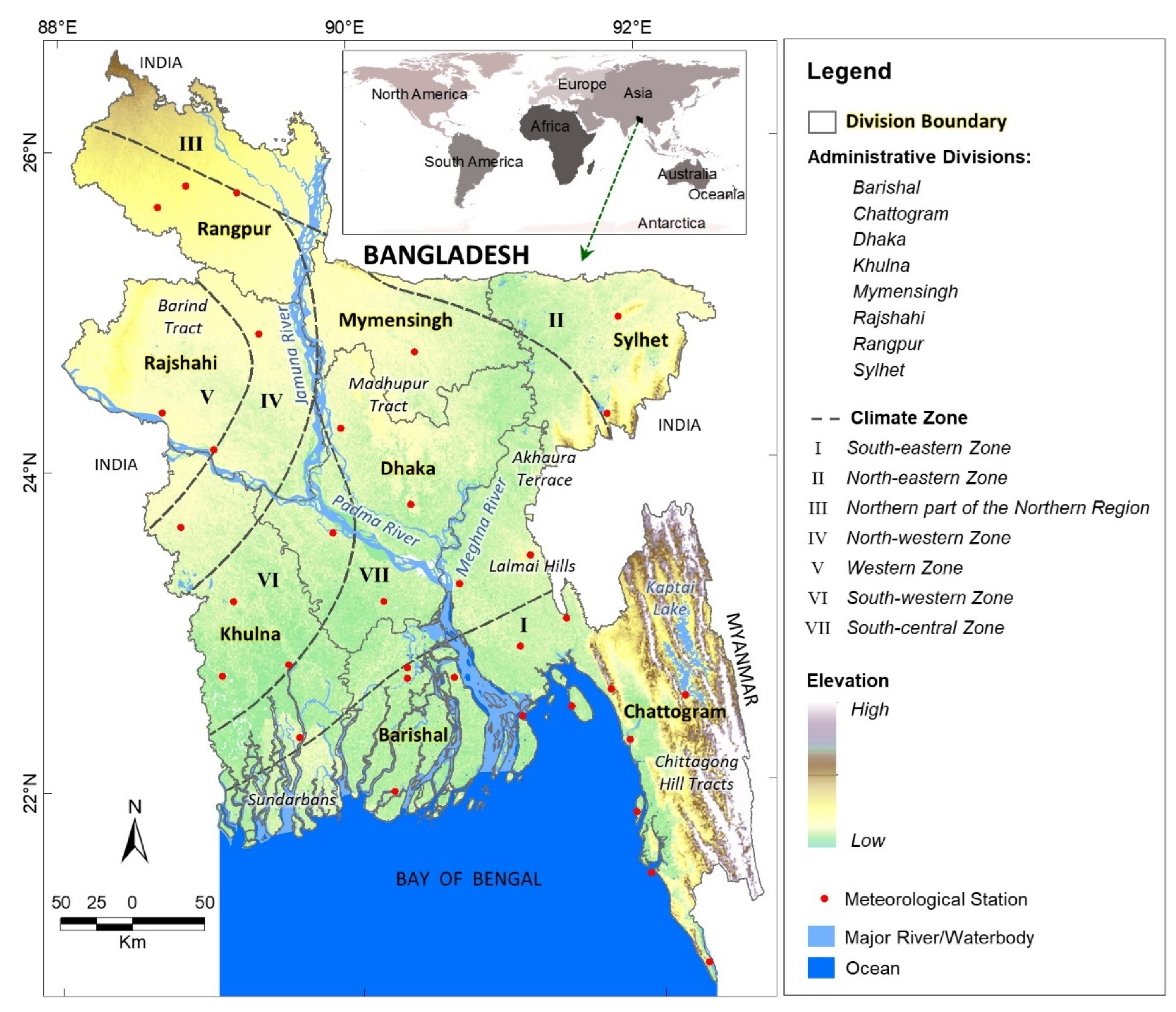
2.1. Study Area
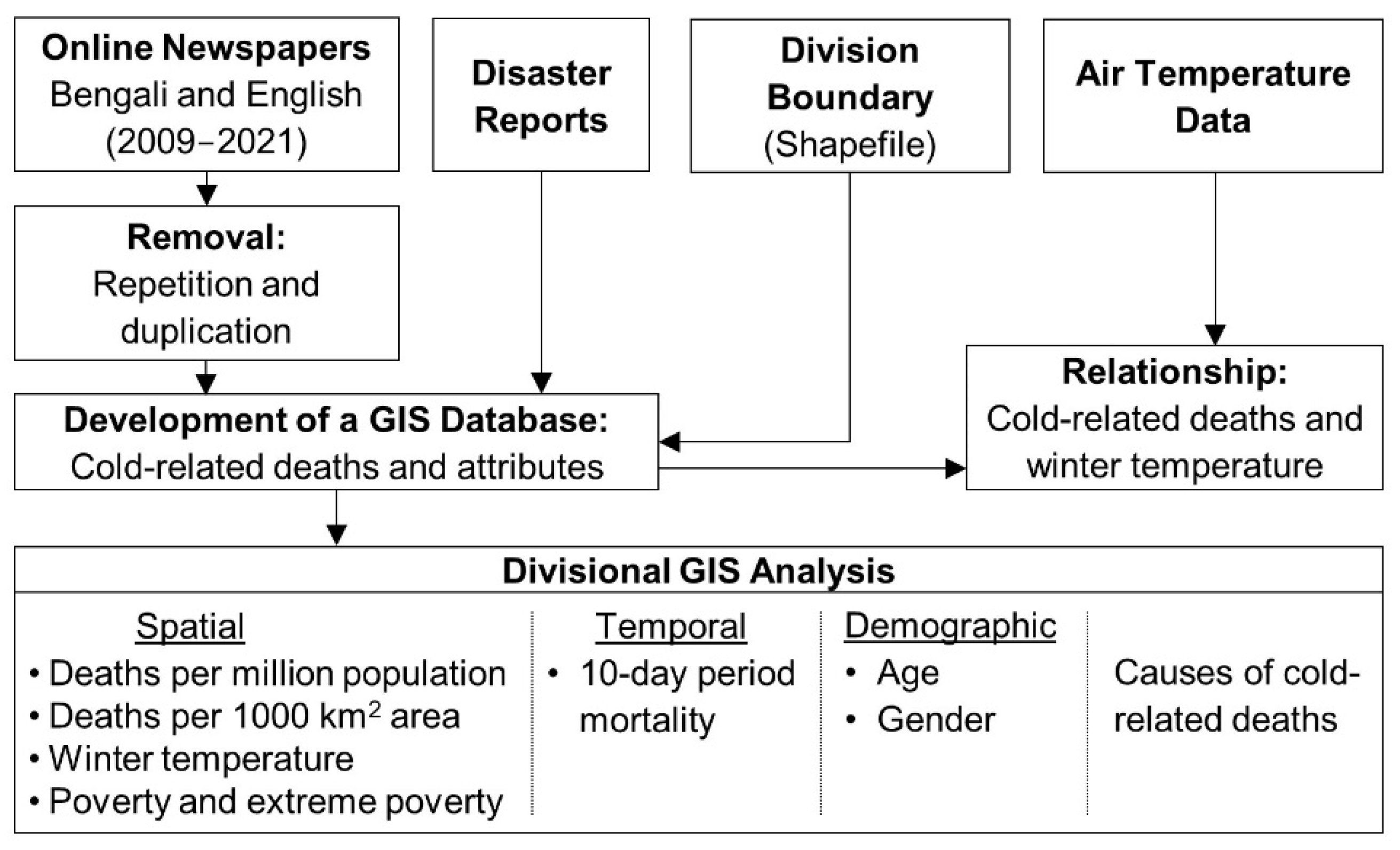
2.2. Data and Methods
3. Results
3.1. Spatial Distribution of Cold-Related Mortality and Its Associated Factors
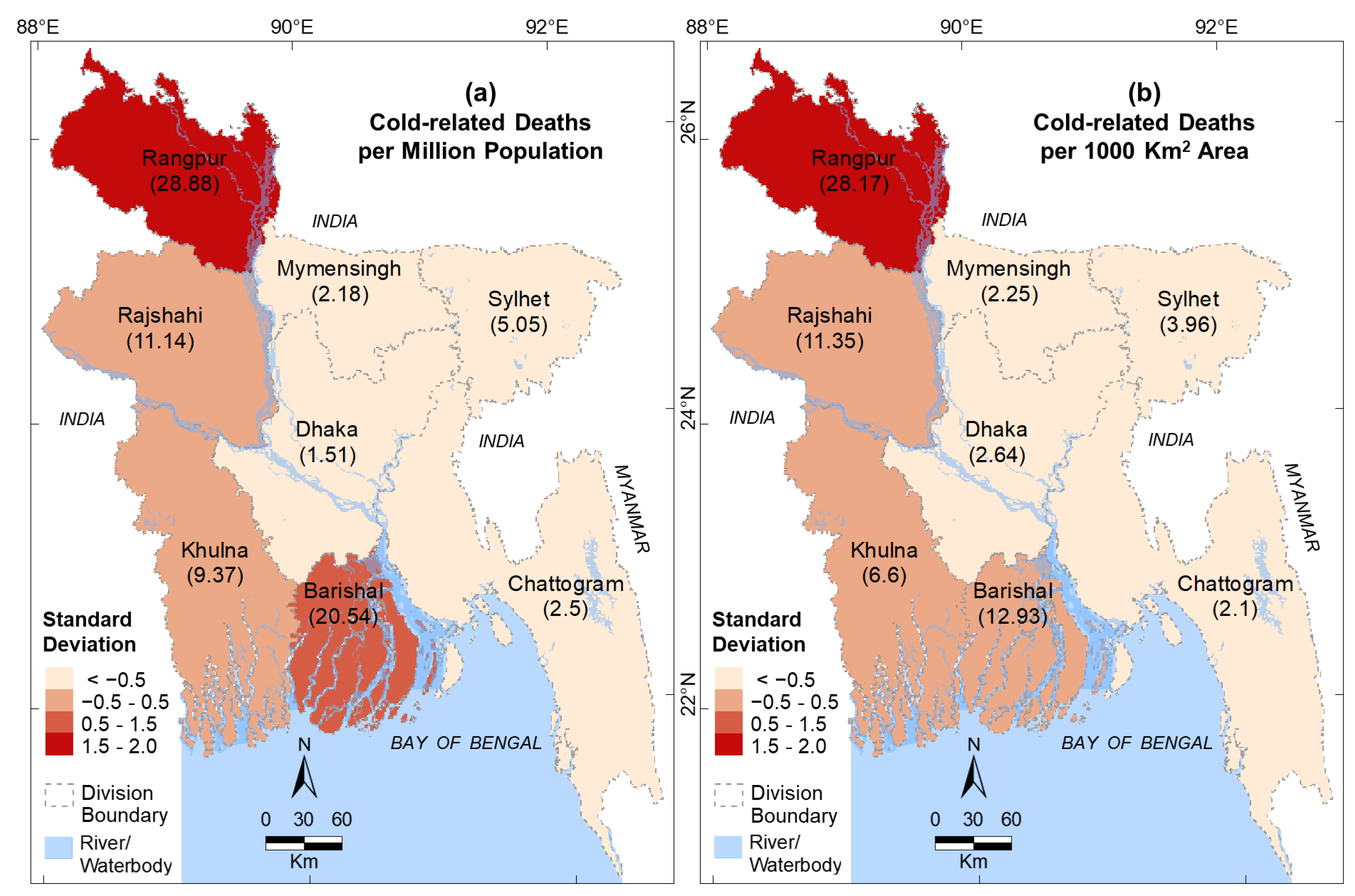
3.1.1. Cold-Related Deaths
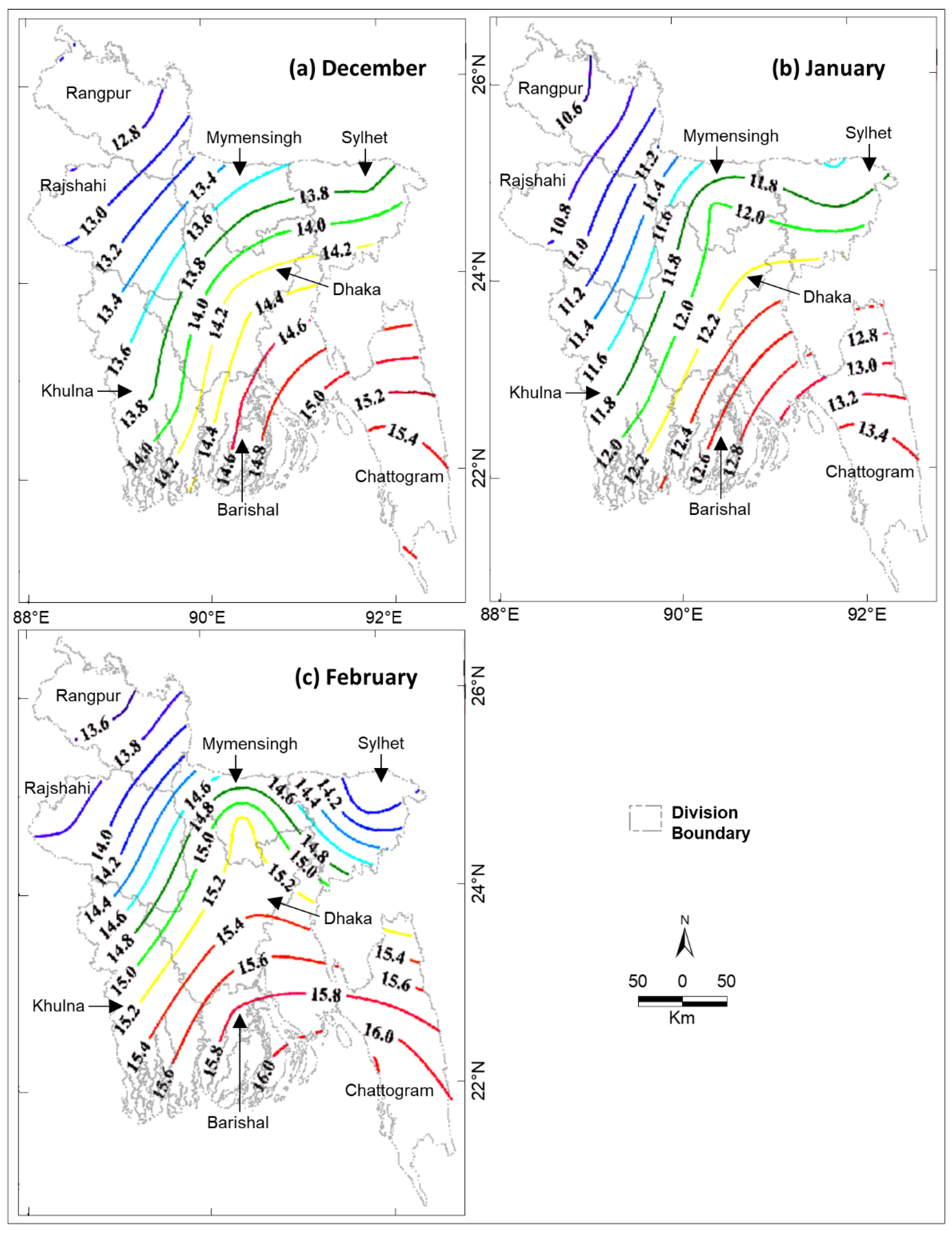
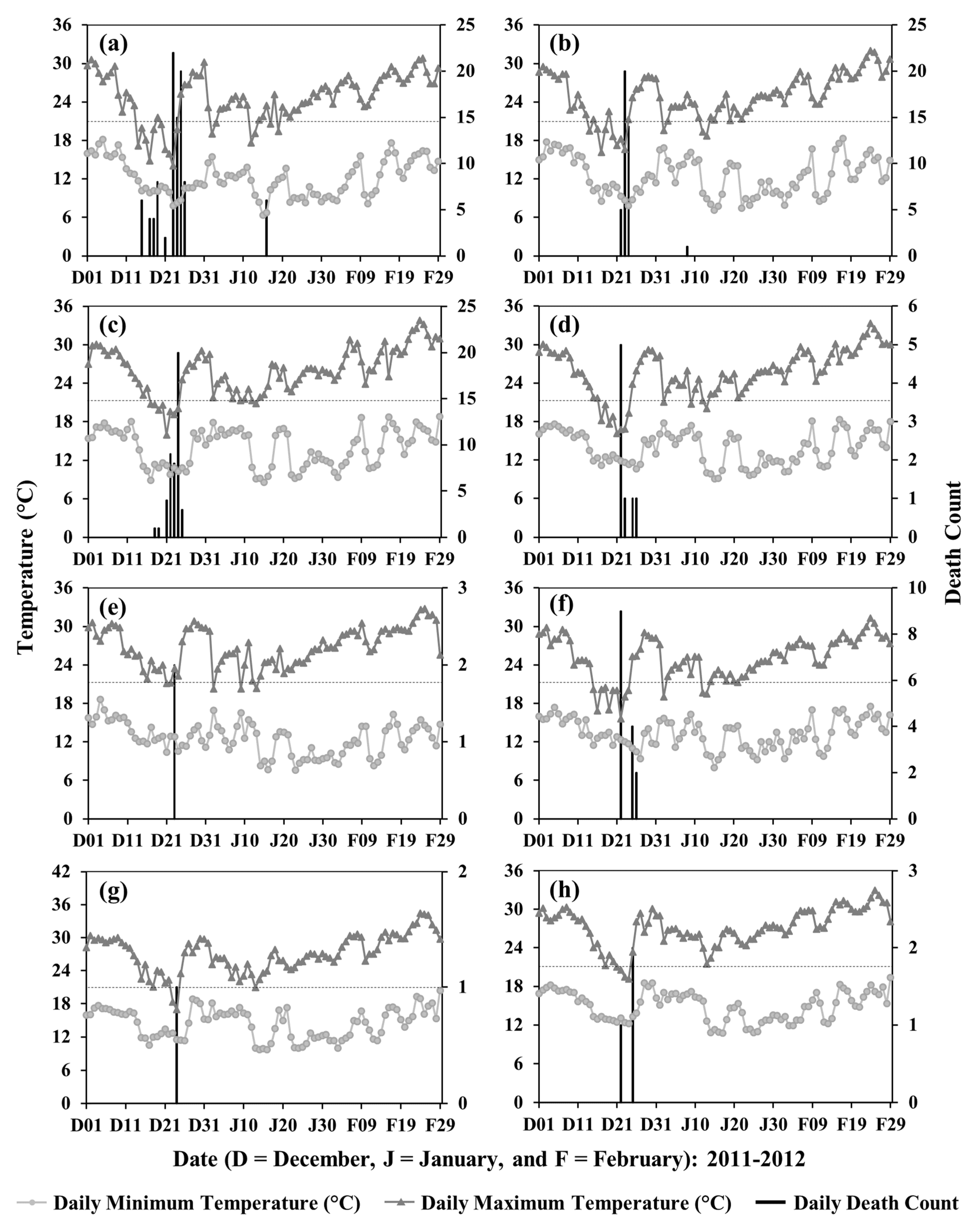
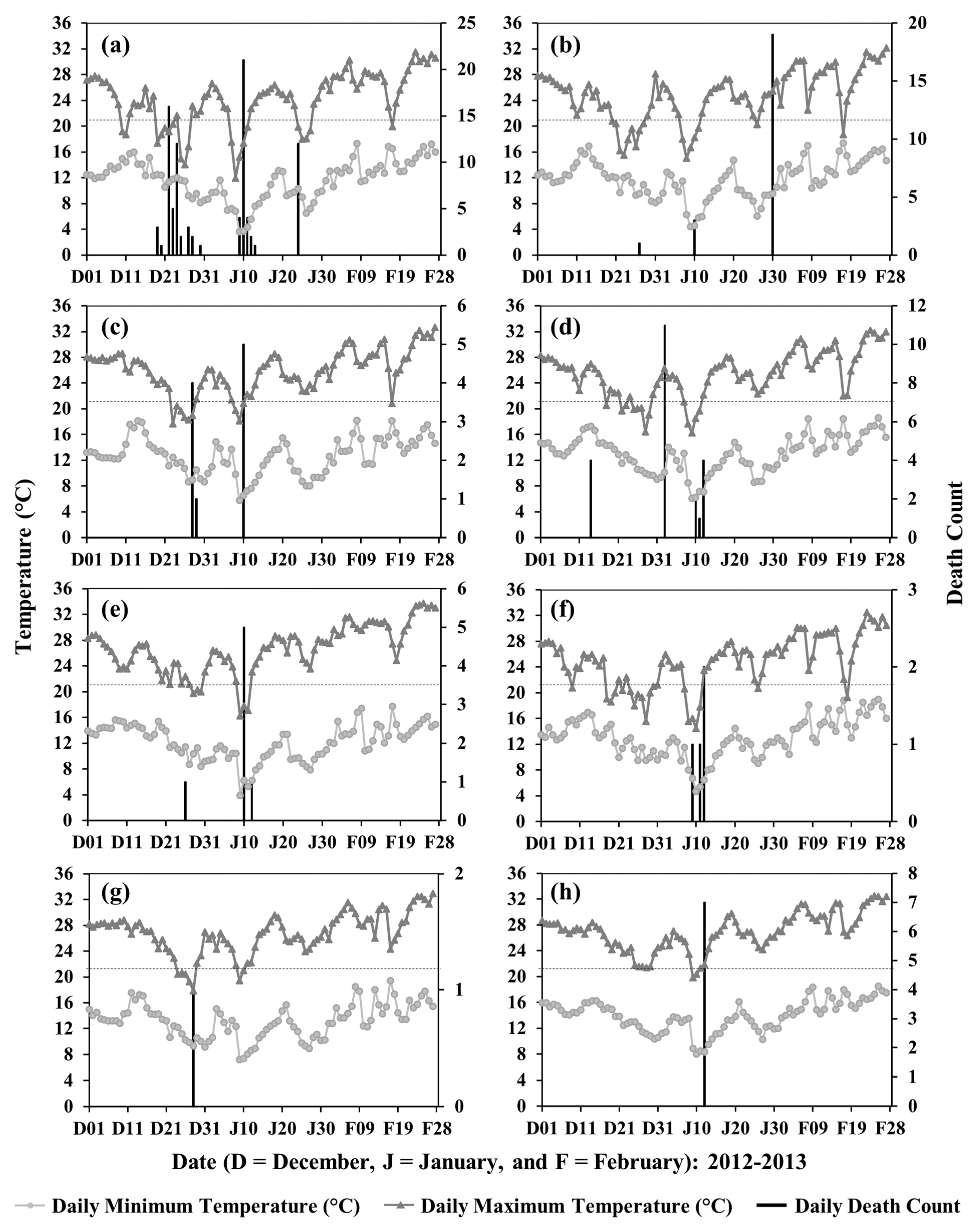
3.1.2. Winter Temperature
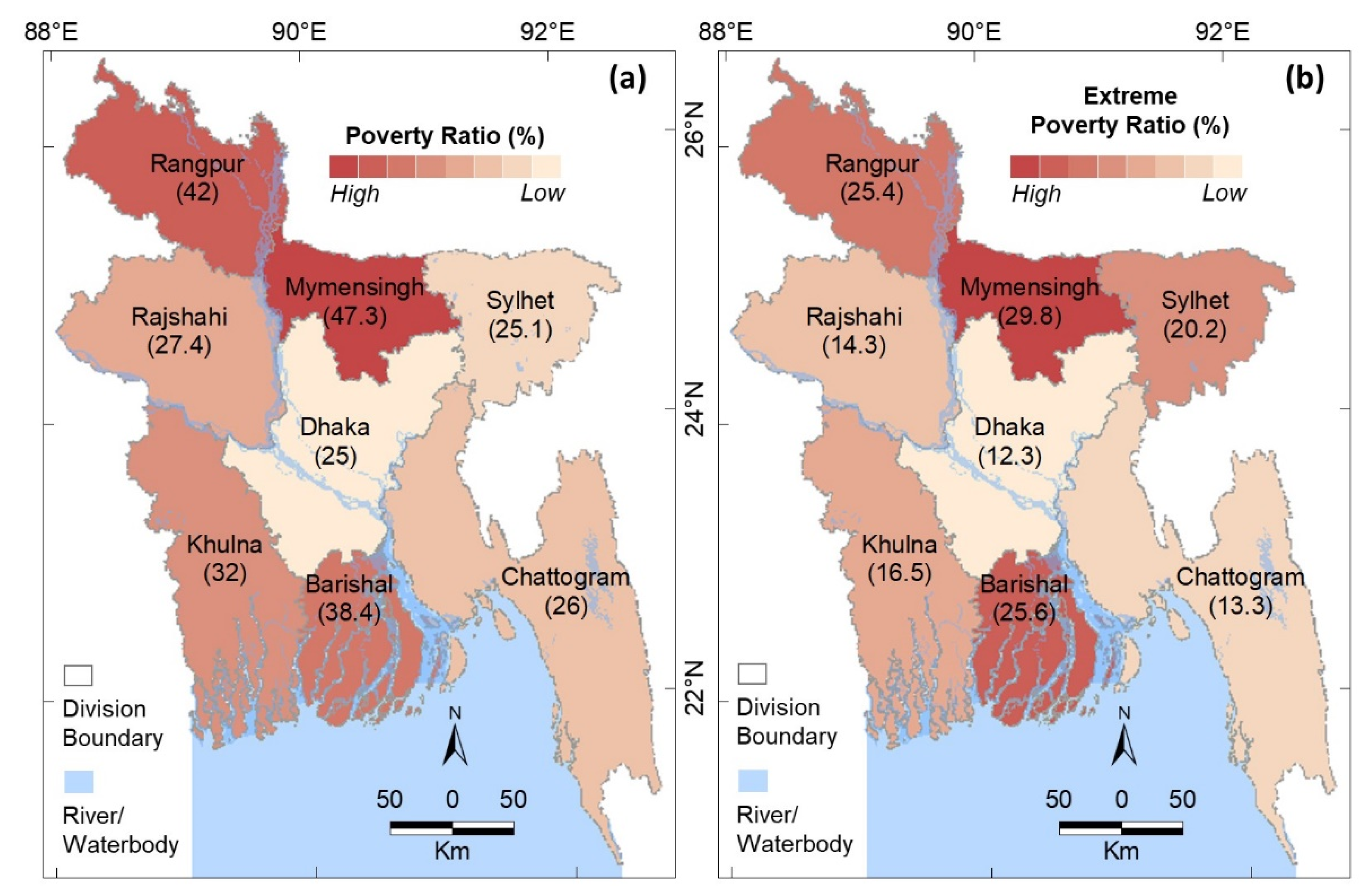
3.1.3. Poverty and Extreme Poverty
3.2. Temporal Variations in Cold-Related Mortality
3.3. Demographic Dynamics of Cold-Related Mortality
3.4. Causes of Cold-Related Mortality
4. Discussion
4.1. Socioeconomic Dimension and Environmental Consequences
4.2. Institutional Framework for Mitigating Cold-Related Deaths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Division | 2009–2010 | 2010–2011 | 2011–2012 | 2012–2013 | 2013–2014 | 2014–2015 | 2015–2016 | 2016–2017 | 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Division | Gender | ||||||||||||||
| Male | Barishal | 4 | 4 | 256 | |||||||||||
| Chattogram | 4 | 5 | 1 | 1 | 2 | 13 | |||||||||
| Dhaka | 4 | 1 | 3 | 12 | 1 | 3 | 24 | ||||||||
| Khulna | 18 | 5 | 18 | 5 | 1 | 6 | 3 | 2 | 58 | ||||||
| Mymensingh | 6 | 1 | 2 | 9 | |||||||||||
| Rajshahi | 5 | 5 | 16 | 3 | 6 | 1 | 3 | 39 | |||||||
| Rangpur | 6 | 11 | 50 | 13 | 4 | 1 | 2 | 4 | 3 | 94 | |||||
| Sylhet | 1 | 1 | 1 | 5 | 3 | 1 | 3 | 15 | |||||||
| Female | Barishal | 1 | 1 | 174 | |||||||||||
| Chattogram | 2 | 2 | 2 | 6 | |||||||||||
| Dhaka | 1 | 3 | 2 | 1 | 4 | 1 | 12 | ||||||||
| Khulna | 10 | 4 | 14 | 4 | 1 | 1 | 3 | 1 | 2 | 40 | |||||
| Mymensingh | 5 | 0 | 5 | ||||||||||||
| Rajshahi | 2 | 2 | 16 | 0 | 2 | 1 | 23 | ||||||||
| Rangpur | 3 | 6 | 19 | 8 | 8 | 2 | 1 | 1 | 25 | 2 | 4 | 3 | 82 | ||
| Sylhet | 2 | 1 | 2 | 5 | |||||||||||
| Children | Barishal | 1 | 3 | 39 | 2 | 117 | 162 | 633 | |||||||
| Chattogram | 35 | 1 | 2 | 6 | 44 | ||||||||||
| Dhaka | 2 | 7 | 9 | ||||||||||||
| Khulna | 1 | 13 | 21 | 3 | 1 | 1 | 40 | ||||||||
| Mymensingh | 3 | 4 | 7 | ||||||||||||
| Rajshahi | 3 | 20 | 23 | 65 | 4 | 115 | |||||||||
| Rangpur | 3 | 24 | 25 | 45 | 38 | 17 | 3 | 7 | 6 | 1 | 38 | 207 | |||
| Sylhet | 1 | 5 | 4 | 5 | 6 | 4 | 5 | 30 | |||||||
| Across BD * | 19 | 19 | |||||||||||||
| Gender not mentioned | Barishal | 1 | 3 | 4 | 186 | ||||||||||
| Chattogram | 8 | 8 | |||||||||||||
| Dhaka | 2 | 1 | 3 | 4 | 10 | ||||||||||
| Khulna | 2 | 1 | 1 | 2 | 3 | 9 | |||||||||
| Mymensingh | 3 | 3 | |||||||||||||
| Rajshahi | 1 | 5 | 23 | 29 | |||||||||||
| Rangpur | 17 | 2 | 1 | 23 | 9 | 8 | 4 | 3 | 6 | 73 | |||||
| Across BD * | 4 | 20 | 7 | 19 | 50 | ||||||||||
| Annual Total | 114 | 75 | 214 | 183 | 87 | 125 | 114 | 18 | 76 | 129 | 62 | 52 | 1249 | 1249 | |
| Age (Year) | Division | 2009–2010 | 2010–2011 | 2011–2012 | 2012–2013 | 2013–2014 | 2014–2015 | 2015–2016 | 2016–2017 | 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Division | Age Group | ||||||||||||||
| 6 and below | Barisal | 1 | 3 | 39 | 2 | 117 | 162 | 633 | |||||||
| Chattogram | 35 | 1 | 2 | 6 | 44 | ||||||||||
| Dhaka | 2 | 7 | 9 | ||||||||||||
| Khulna | 1 | 13 | 21 | 3 | 1 | 1 | 40 | ||||||||
| Mymensingh | 3 | 4 | 7 | ||||||||||||
| Rajshahi | 3 | 20 | 23 | 65 | 4 | 115 | |||||||||
| Rangpur | 3 | 24 | 25 | 45 | 38 | 17 | 3 | 7 | 6 | 1 | 38 | 207 | |||
| Sylhet | 1 | 5 | 4 | 5 | 6 | 4 | 5 | 30 | |||||||
| Across BD * | 19 | 19 | |||||||||||||
| 7–14 | Chattogram | 1 | 1 | 7 | |||||||||||
| Khulna | 1 | 1 | |||||||||||||
| Rajshahi | 1 | 1 | 2 | ||||||||||||
| Rangpur | 2 | 1 | 3 | ||||||||||||
| 15–64 | Barisal | 1 | 1 | 166 | |||||||||||
| Chattogram | 1 | 1 | 3 | 1 | 1 | 7 | |||||||||
| Dhaka | 2 | 4 | 8 | 2 | 3 | 2 | 21 | ||||||||
| Khulna | 6 | 4 | 11 | 2 | 1 | 2 | 1 | 1 | 28 | ||||||
| Mymensingh | 4 | 2 | 6 | ||||||||||||
| Rajshahi | 5 | 3 | 8 | 2 | 18 | ||||||||||
| Rangpur | 2 | 5 | 20 | 7 | 7 | 2 | 21 | 2 | 3 | 3 | 72 | ||||
| Sylhet | 1 | 3 | 4 | 1 | 4 | 13 | |||||||||
| 65 and above | Barisal | 4 | 4 | 255 | |||||||||||
| Chattogram | 4 | 1 | 4 | 2 | 11 | ||||||||||
| Dhaka | 3 | 2 | 2 | 5 | 1 | 1 | 1 | 15 | |||||||
| Khulna | 24 | 5 | 19 | 6 | 1 | 5 | 3 | 3 | 3 | 69 | |||||
| Mymensingh | 4 | 1 | 5 | ||||||||||||
| Rajshahi | 2 | 4 | 24 | 3 | 7 | 2 | 1 | 43 | |||||||
| Rangpur | 7 | 12 | 46 | 14 | 5 | 1 | 1 | 3 | 8 | 4 | 101 | ||||
| Sylhet | 1 | 1 | 4 | 1 | 7 | ||||||||||
| Age not mentioned | Barisal | 1 | 3 | 4 | 188 | ||||||||||
| Chattogram | 8 | 8 | |||||||||||||
| Dhaka | 1 | 2 | 3 | 4 | 10 | ||||||||||
| Khulna | 2 | 2 | 2 | 3 | 9 | ||||||||||
| Mymensingh | 3 | 3 | 6 | ||||||||||||
| Rajshahi | 1 | 4 | 23 | 28 | |||||||||||
| Rangpur | 17 | 2 | 2 | 22 | 9 | 8 | 4 | 3 | 6 | 73 | |||||
| Across BD * | 4 | 20 | 7 | 19 | 50 | ||||||||||
| Annual Total | 114 | 75 | 214 | 183 | 87 | 125 | 114 | 18 | 76 | 129 | 62 | 52 | 1249 | 1249 | |
References
- Lu, L.; Wang, Z.; Shi, P. Mapping Cold Wave Risk of the World. In World Atlas of Natural Disaster Risk; Shi, P., Kasperson, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 189–207. ISBN 978-3-662-45430-5. [Google Scholar]
- Federal Emergency Management Agency (US) Cold Wave. Available online: https://hazards.fema.gov/nri/cold-wave#:~:text=A%20Cold%20Wave%20is%20a,(NWS)%20weather%20forecast%20office (accessed on 20 September 2022).
- Karmakar, S. Patterns of Climate Change and Its Impacts in Northwestern Bangladesh. J. Eng. Sci. 2019, 10, 33–48. [Google Scholar]
- Roy, U.; Singh, A.; Rahman, M.W.; Chowdhury, M.T. To Date Situation of Highly Pathogenic Avian Influenza (HPAI) H5N1 in Bangladesh: A Review. In Proceedings of the 3rd International Conference on Environmental Aspects of Bangladesh [ICEAB 2012], Fukuoka, Japan, 13–14 October 2012; pp. 84–86. [Google Scholar]
- Akhter, A.; Rahim, A. Bangladesh Cold Wave Leaves at Least 50 Dead. Available online: https://www.japantimes.co.jp/news/2019/12/29/world/bangladesh-cold-wave-leaves-least-50-dead/ (accessed on 12 January 2022).
- Akhter, A. Dozens Dead as Cold Wave Sweeps through Bangladesh. Available online: https://www.aljazeera.com/news/2019/12/29/dozens-dead-as-cold-wave-sweeps-through-bangladesh (accessed on 12 January 2022).
- Encyclopaedia Britannica Mortality. Available online: https://www.britannica.com/science/mortality-demography (accessed on 12 January 2022).
- Merriam-Webster Mortality. Available online: https://www.merriam-webster.com/dictionary/mortality (accessed on 12 March 2022).
- Cambridge Dictionary Mortality. Available online: https://dictionary.cambridge.org/dictionary/english/mortality (accessed on 12 March 2022).
- Oxford Learner’s Dictionaries Mortality. Available online: https://www.oxfordlearnersdictionaries.com/definition/american_english/mortality#:~:text=noun-,noun,aware%20of%20her%20own%20mortality (accessed on 12 March 2022).
- Top, F.H. Mortality, fatality, and morbidity (proper use of terms). Pediatrics 1972, 50, 976. [Google Scholar] [CrossRef] [PubMed]
- Almendra, R.; Perelman, J.; Vasconcelos, J.; Santana, P. Excess winter mortality and morbidity before, during, and after the Great Recession: The Portuguese case. Int. J. Biometeorol. 2019, 63, 873–883. [Google Scholar] [CrossRef] [PubMed]
- Pascal, M.; Wagner, V.; Corso, M.; Laaidi, K.; Ung, A.; Beaudeau, P. Heat and cold related-mortality in 18 French cities. Environ. Int. 2018, 121, 189–198. [Google Scholar] [CrossRef]
- Paschalidou, A.K.; Kassomenos, P.A.; McGregor, G.R. Analysis of the synoptic winter mortality climatology in five regions of England: Searching for evidence of weather signals. Sci. Total Environ. 2017, 598, 432–444. [Google Scholar] [CrossRef]
- Montero, J.C.; Mirón, I.J.; Criado-Álvarez, J.J.; Linares, C.; Díaz, J. Mortality from cold waves in Castile—La Mancha, Spain. Sci. Total Environ. 2010, 408, 5768–5774. [Google Scholar] [CrossRef]
- Analitis, A.; Katsouyanni, K.; Biggeri, A.; Baccini, M.; Forsberg, B.; Bisanti, L.; Kirchmayer, U.; Ballester, F.; Cadum, E.; Goodman, P.G.; et al. Effects of cold weather on mortality: Results from 15 European cities within the PHEWE project. Am. J. Epidemiol. 2008, 168, 1397–1408. [Google Scholar] [CrossRef]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Eric Lavigne, A.Z.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; Leone, M.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 14, 464–465. [Google Scholar] [CrossRef]
- Nation Master Cold Countries: Statistical Profile. Available online: https://www.nationmaster.com/country-info/groups/Cold-countries#:~:text=DEFINITION%3A%20Countries%20where%20the%20mean,%2439.12%20trillion (accessed on 20 September 2022).
- Davie, G.S.; Baker, M.G.; Hales, S.; Carlin, J.B. Trends and determinants of excess winter mortality in New Zealand: 1980 to 2000. BMC Public Health 2007, 7, 263. [Google Scholar] [CrossRef]
- Schwartz, J. Who is sensitive to extremes of temperature? A case-only analysis. Epidemiology 2005, 16, 67–72. [Google Scholar] [CrossRef]
- Wilkinson, P.; Pattenden, S.; Armstrong, B.; Fletcher, A.; Kovats, R.S.; Mangtani, P.; McMichael, A.J. Vulnerability to winter mortality in elderly people in Britain: Population based study. Br. Med. J. 2004, 329, 647–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asif, M.; Nawaz, K.; Zaheer, Z.; Thygesen, H.; AbuShaheen, A.; Riaz, M. Seasonality of deaths with respect to age and cause in Chitral District Pakistan. PLoS ONE 2019, 14, e0225994. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.H.; Gasparrini, A.; Rodriguez, P.S.; Jha, P. Mortality attributable to hot and cold ambient temperatures in India: A nationally representative case-crossover study. PLoS Med. 2018, 15, e1002619. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Liu, T.; Hu, M.; Zeng, W.; Zhang, Y.; Rutherford, S.; Lin, H.; Xiao, J.; Yin, P.; Liu, J.; et al. The impact of cold spells on mortality and effect modification by cold spell characteristics. Sci. Rep. 2016, 6, 38380. [Google Scholar] [CrossRef]
- Zhou, M.G.; Wang, L.J.; Liu, T.; Zhang, Y.H.; Lin, H.L.; Luo, Y.; Xiao, J.P.; Zeng, W.L.; Zhang, Y.W.; Wang, X.F.; et al. Health impact of the 2008 cold spell on mortality in subtropical China: The climate and health impact national assessment study (CHINAs). Environ. Health 2014, 13, 60. [Google Scholar] [CrossRef]
- Ou, C.Q.; Song, Y.F.; Yang, J.; Chau, P.Y.K.; Yang, L.; Chen, P.Y.; Wong, C.M. Excess Winter Mortality and Cold Temperatures in a Subtropical City, Guangzhou, China. PLoS ONE 2013, 8, e77150. [Google Scholar] [CrossRef]
- Goggins, W.B.; Chan, E.Y.; Yang, C.; Chong, M. Associations between mortality and meteorological and pollutant variables during the cool season in two Asian cities with sub-tropical climates: Hong Kong and Taipei. Environ. Health A Glob. Access Sci. Source 2013, 12, 59. [Google Scholar] [CrossRef]
- Pandey, K. Cold Waves Killed More Indians than Heat Waves Since 1980: IMD. Available online: https://www.downtoearth.org.in/news/cold-waves-killed-more-indians-than-heat-waves-since-1980-imd-68606 (accessed on 23 September 2021).
- Marchand, I.; Johnson, D.; Montgomery, D.; Brisson, G.R.; Perrault, H. Gender differences in temperature and vascular characteristics during exercise recovery. Can. J. Appl. Physiol. 2001, 26, 425–441. [Google Scholar] [CrossRef]
- Mahapatra, B.; Walia, M.; Saggurti, N. Extreme weather events induced deaths in India 2001–2014: Trends and differentials by region, sex and age group. Weather Clim. Extrem. 2018, 21, 110–116. [Google Scholar] [CrossRef]
- Burkart, K.; Khan, M.H.; Krämer, A.; Breitner, S.; Schneider, A.; Endlicher, W.R. Seasonal variations of all-cause and cause-specific mortality by age, gender, and socioeconomic condition in urban and rural areas of Bangladesh. Int. J. Equity Health 2011, 10, 32. [Google Scholar] [CrossRef]
- Hashizume, M.; Wagatsuma, Y.; Hayashi, T.; Saha, S.K.; Streatfield, K.; Yunus, M. The effect of temperature on mortality in rural Bangladesh-a population-based time-series study. Int. J. Epidemiol. 2009, 38, 1689–1697. [Google Scholar] [CrossRef] [Green Version]
- Babalola, O.; Razzaque, A.; Bishai, D. Temperature extremes and infant mortality in Bangladesh: Hotter months, lower mortality. PLoS ONE 2018, 13, e0189252. [Google Scholar] [CrossRef]
- DF Foundation For Disaster Forum. A National Network on Disaster Preparedness and Risk Reduction. Available online: https://disasterforum.org/publications/ (accessed on 5 August 2021).
- NIRAPAD Hazard Situation Report. Available online: https://www.nirapad.org.bd/home/resources/hazardSituation (accessed on 5 August 2021).
- OCHA United Nations Office for the Coordination of Humanitarian Affairs. About ReliefWeb. Available online: https://www.reliefweb.int/report/bangladesh/bangladesh-cold-wave-information-bulletin/ (accessed on 5 August 2021).
- IFRC International Federation of Red Cross and Red Crescent Societies. Available online: https://media.ifrc.org/ifrc/where-we-work/asia-pacific/ (accessed on 5 August 2021).
- CRED Centre for Research on the Epidemiology of Disasters. EM-DAT: The International Disaster Database. Available online: https://www.emdat.be/ (accessed on 5 August 2021).
- The Daiy Star The Daily Star on Friday. Available online: https://epaper.thedailystar.net/Home/ArticleView?eid=1&edate=31/07/2020&pgid=16371 (accessed on 5 August 2021).
- Rabbi, A.R. Fire fatalities: Lack of awareness leads to higher casualties in winter. DhakaTribute 2018. Available online: https://archive.dhakatribune.com/bangladesh/nation/2018/01/28/fire-fatalities-lack-awareness-leads-higher-casualties-winter (accessed on 5 August 2021).
- Banglapedia National Encyclopedia of Bangladesh. Bangladesh Geography. Available online: https://en.banglapedia.org/index.php?title=Bangladesh_Geography (accessed on 5 August 2021).
- BBS Statistics 2019. Bangladesh Bureau of Statistics, Statistics and Informatics Division, Ministry of Planning; Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2019.
- BBS Population & Housing Census-2011. Bangladesh Bureau of Statistics, Statistics and Informatics Division, Ministry of Planning; Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2014; Volume 2.
- Rashid, H.E. Geography of Bangladesh. Available online: https://en.wikipedia.org/wiki/Geography_of_Bangladesh (accessed on 10 January 2022).
- Brammer, H. Bangladesh’s diverse and complex physical geography: Implications for agricultural development. Int. J. Environ. Stud. 2017, 74, 1–27. [Google Scholar] [CrossRef]
- Wikipedia People’s Republic of Bangladesh. Available online: https://apps.who.int/iris/bitstream/handle/10665/254275/WHO-HSE-GCR-2016.23-eng.pdf;jsessionid=D11D81B590B207358388321280541148?sequence=1 (accessed on 18 August 2021).
- Alamgir, M.; Ahmed, K.; Homsi, R.; Dewan, A.; Wang, J.J.; Shahid, S. Downscaling and Projection of Spatiotemporal Changes in Temperature of Bangladesh. Earth Syst. Environ. 2019, 3, 381–398. [Google Scholar] [CrossRef]
- Sarker, M.A.R.; Alam, K.; Gow, J. Performance of rain-fed Aman rice yield in Bangladesh in the presence of climate change. Renew. Agric. Food Syst. 2019, 34, 304–312. [Google Scholar] [CrossRef]
- The Daily Star The cold facts. The Daily Star on Friday: 12 January 2018. Available online: https://epaper.thedailystar.net/Home/ArticleView?eid=1&edate=12/01/2018&pgid=76230 (accessed on 1 August 2021).
- Shahid, S. Spatial and temporal characteristics of droughts in the western part of Bangladesh. Hydrol. Process. 2008, 22, 2235–2247. [Google Scholar] [CrossRef]
- Shahid, S.; Khairulmaini, O.S. Spatio-Temporal Variability of Rainfall over Bangladesh During the Time Period 1969-2003. Asia-Pac. J. Atmos. Sci. 2009, 45, 375–389. [Google Scholar]
- Prothom–alo Bengali News paper. Available online: www.prothomalo.com (accessed on 5 August 2021).
- Ittefaq Bengali News Paper. Available online: www.ittefaq.com.bd (accessed on 5 August 2021).
- The Daily Star Today’s News. Available online: https://www.thedailystar.net/ (accessed on 5 August 2021).
- Daily Observer Latest News. Available online: www.observerbd.com (accessed on 5 August 2021).
- DhakaTribune Today’s Paper. Available online: www.dhakatribune.com (accessed on 5 August 2021).
- Holle, R.L.; Dewan, A.; Said, R.; Brooks, W.A.; Hossain, M.F.; Rafiuddin, M. Fatalities related to lightning occurrence and agriculture in Bangladesh. Int. J. Disaster Risk Reduct. 2019, 41, 101264. [Google Scholar] [CrossRef]
- Dewan, A.; Hossain, M.F.; Rahman, M.M.; Yamane, Y.; Holle, R.L. Recent lightning-related fatalities and injuries in Bangladesh. Weather. Clim. Soc. 2017, 9, 575–589. [Google Scholar] [CrossRef]
- The World Bank DataBank. Available online: https://databank.worldbank.org/home.aspx (accessed on 2 September 2021).
- Bugmann, G.; Lister, J.B.; Stockar, U.V. The Standard Deviation Method: Data analysis by classical means and by neural networks. In International Conference on Recent Development in Statistical Data Analysis and Inference; Ecole Polytechnique Federale De Lausanne: Neuchdtel, Switzerland, 1989; p. 18. [Google Scholar]
- World Bank. Bangladesh Poverty Assessment: Facing Old and New Frontiers in Poverty Reduction; World Bank: Washington, DC, USA, 2019. [Google Scholar]
- Pradhan, B.; Sharma, P.; Pradhan, P.K. Impact of Cold Wave on Vulnerable People of Tarai Region, Nepal. In Climate Change and Global Warming; IntechOpen: London, UK, 2019; pp. 143–156. [Google Scholar]
- Malik, P.; Bhardwaj, P.; Singh, O. Distribution of Cold Wave Mortalities over India: 1978–2014. Int. J. Disaster Risk Reduct. 2020, 51, 101841. [Google Scholar] [CrossRef]
- BMD Bangladesh Meteorological Department: Climate Data Library. Available online: http://datalibrary.bmd.gov.bd/ (accessed on 21 September 2021).
- Rettner, R. How Does a Person Freeze to Death? Available online: https://www.livescience.com/6008-person-freeze-death.html (accessed on 12 January 2022).
- Garner, J.M.; Iwasko, W.C.; Jewel, T.D.; Charboneau, B.R.; Dodd, A.A.; Zontos, K.M. A multihazard assessment of age-related weather vulnerabilities. Weather. Clim. Soc. 2020, 12, 367–386. [Google Scholar] [CrossRef]
- The Daily Star SBMCH in Barishal: 110 Infants Dies of Dold-Related Diseases in Dec. Available online: https://epaper.thedailystar.net/Home/ArticleView?eid=1&edate=14/01/2019&pgid=86797 (accessed on 16 September 2021).
- Wardlaw, T.; Salama, P.; Johansson, E.W.; Mason, E. Pneumonia: The leading killer of children. Lancet 2006, 368, 1048–1050. [Google Scholar] [CrossRef]
- Staff Correspondent Burn Units to be Set Up in Every District Hospital. Available online: https://m.daily-bangladesh.com/english/Burn-units-to-be-set-up-in-every-district-hospital/63685 (accessed on 11 January 2022).







| Period | Division | 2009–2010 | 2010–2011 | 2011–2012 | 2012–2013 | 2013–2014 | 2014–2015 | 2015–2016 | 2016–2017 | 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | Total | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Division | Period | Month | |||||||||||||||
| December | 1–10 | Chattogram | 1 | 1 | 2 | 568 | |||||||||||
| Dhaka | 1 | 1 | |||||||||||||||
| 11–20 | Chattogram | 9 | 1 | 10 | 57 | ||||||||||||
| Dhaka | 4 | 4 | |||||||||||||||
| Khulna | 2 | 2 | 4 | ||||||||||||||
| Rangpur | 22 | 4 | 26 | ||||||||||||||
| Sylhet | 4 | 5 | 9 | ||||||||||||||
| Across BD * | 4 | 4 | |||||||||||||||
| 21–31 | Barishal | 1 | 1 | 21 | 110 | 133 | 509 | ||||||||||
| Chattogram | 3 | 3 | 6 | ||||||||||||||
| Dhaka | 8 | 1 | 9 | ||||||||||||||
| Khulna | 15 | 44 | 5 | 22 | 5 | 91 | |||||||||||
| Mymensingh | 15 | 2 | 17 | ||||||||||||||
| Rajshahi | 39 | 1 | 23 | 63 | |||||||||||||
| Rangpur | 67 | 41 | 26 | 1 | 3 | 5 | 1 | 144 | |||||||||
| Sylhet | 2 | 1 | 5 | 8 | |||||||||||||
| Across BD * | 38 | 38 | |||||||||||||||
| January | 1–10 | Barishal | 1 | 1 | 174 | 669 | |||||||||||
| Chattogram | 5 | 1 | 3 | 9 | |||||||||||||
| Dhaka | 5 | 13 | 3 | 21 | |||||||||||||
| Khulna | 8 | 1 | 5 | 1 | 15 | ||||||||||||
| Mymensingh | 1 | 1 | |||||||||||||||
| Rajshahi | 4 | 1 | 3 | 1 | 6 | 15 | |||||||||||
| Rangpur | 10 | 15 | 25 | 15 | 25 | 9 | 2 | 101 | |||||||||
| Sylhet | 5 | 6 | 11 | ||||||||||||||
| 11–20 | Barishal | 3 | 7 | 10 | 287 | ||||||||||||
| Chattogram | 24 | 8 | 7 | 6 | 45 | ||||||||||||
| Dhaka | 3 | 5 | 2 | 3 | 3 | 16 | |||||||||||
| Khulna | 7 | 9 | 1 | 4 | 5 | 26 | |||||||||||
| Mymensingh | 3 | 3 | |||||||||||||||
| Rajshahi | 4 | 7 | 7 | 2 | 1 | 21 | |||||||||||
| Rangpur | 19 | 28 | 6 | 7 | 14 | 2 | 3 | 21 | 6 | 6 | 19 | 131 | |||||
| Sylhet | 1 | 1 | 1 | 5 | 8 | ||||||||||||
| Across BD * | 20 | 7 | 27 | ||||||||||||||
| 21–31 | Barishal | 21 | 6 | 27 | 208 | ||||||||||||
| Dhaka | 4 | 4 | |||||||||||||||
| Khulna | 2 | 6 | 2 | 10 | |||||||||||||
| Rajshahi | 19 | 88 | 107 | ||||||||||||||
| Rangpur | 12 | 2 | 3 | 7 | 27 | 51 | |||||||||||
| Sylhet | 4 | 5 | 9 | ||||||||||||||
| February | 1–10 | Khulna | 1 | 1 | 12 | 12 | |||||||||||
| Mymensingh | 3 | 3 | |||||||||||||||
| Rangpur | 2 | 1 | 3 | ||||||||||||||
| Sylhet | 5 | 5 | |||||||||||||||
| Annual Total | 114 | 75 | 214 | 183 | 87 | 125 | 114 | 18 | 76 | 129 | 62 | 52 | 1249 | 1249 | 1249 | ||
| Cause of Death | 2009–2010 | 2010–2011 | 2011–2012 | 2012–2013 | 2013–2014 | 2014–2015 | 2015–2016 | 2016–2017 | 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | Total | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cold | 107 | 70 | 208 | 145 | 41 | 113 | 51 | 13 | 19 | 127 | 6 | 43 | 943 | 943 | |
| Disease | Pneumonia | 5 | 5 | 3 | 23 | 6 | 6 | 2 | 11 | 61 | 133 | ||||
| Diarrhoea | 2 | 3 | 30 | 35 | |||||||||||
| Asthma | 2 | 14 | 5 | 2 | 14 | 37 | |||||||||
| Burn | 1 | 3 | 1 | 1 | 2 | 5 | 37 | 2 | 12 | 9 | 73 | 73 | |||
| Unknown | 12 | 25 | 56 | 7 | 100 | 100 | |||||||||
| Annual Total | 114 | 75 | 214 | 183 | 87 | 125 | 114 | 18 | 76 | 129 | 62 | 52 | 1249 | 1249 | |
| Division | Death | Hospitalization | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (Year) | Gender | Age and Gender Not Mentioned | Age (Year) | Age and Gender Not Mentioned | |||||||||
| 6 and below | 7–14 | 15–64 | 65 and above | Male | Female | Children | 6 and below | 7–14 | 15–64 | 65 and above | |||
| Barishal | 1 | 1 | |||||||||||
| Chittagong | 3 | 2 | 1 | ||||||||||
| Dhaka | 2 | 2 | 1 | 3 | 4 | ||||||||
| Khulna | 2 | 1 | 1 | 1 | 1 | 2 | |||||||
| Mymensingh | 2 | 20 | |||||||||||
| Rajshahi | 1 | 3 | 1 | 3 | |||||||||
| Rangpur | 1 | 23 | 12 | 5 | 30 | 1 | 15 | 11 | 02 | 132 | |||
| Total | 3 | 31 | 18 | 10 | 39 | 3 | 21 | 11 | 02 | 152 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.M.; Mahtab, A.S.M.; Ahmed, M.R.; Hassan, Q.K. Developing a Cold-Related Mortality Database in Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 12175. https://doi.org/10.3390/ijerph191912175
Alam MM, Mahtab ASM, Ahmed MR, Hassan QK. Developing a Cold-Related Mortality Database in Bangladesh. International Journal of Environmental Research and Public Health. 2022; 19(19):12175. https://doi.org/10.3390/ijerph191912175
Chicago/Turabian StyleAlam, Md. Mahbub, A.S.M. Mahtab, M. Razu Ahmed, and Quazi K. Hassan. 2022. "Developing a Cold-Related Mortality Database in Bangladesh" International Journal of Environmental Research and Public Health 19, no. 19: 12175. https://doi.org/10.3390/ijerph191912175
APA StyleAlam, M. M., Mahtab, A. S. M., Ahmed, M. R., & Hassan, Q. K. (2022). Developing a Cold-Related Mortality Database in Bangladesh. International Journal of Environmental Research and Public Health, 19(19), 12175. https://doi.org/10.3390/ijerph191912175