

Association between the Use of Folic Acid Supplements during Pregnancy and Children’s Cognitive Function at 7–9 Years of Age in the INMA Cohort Study
 , , ,
, , ,  , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
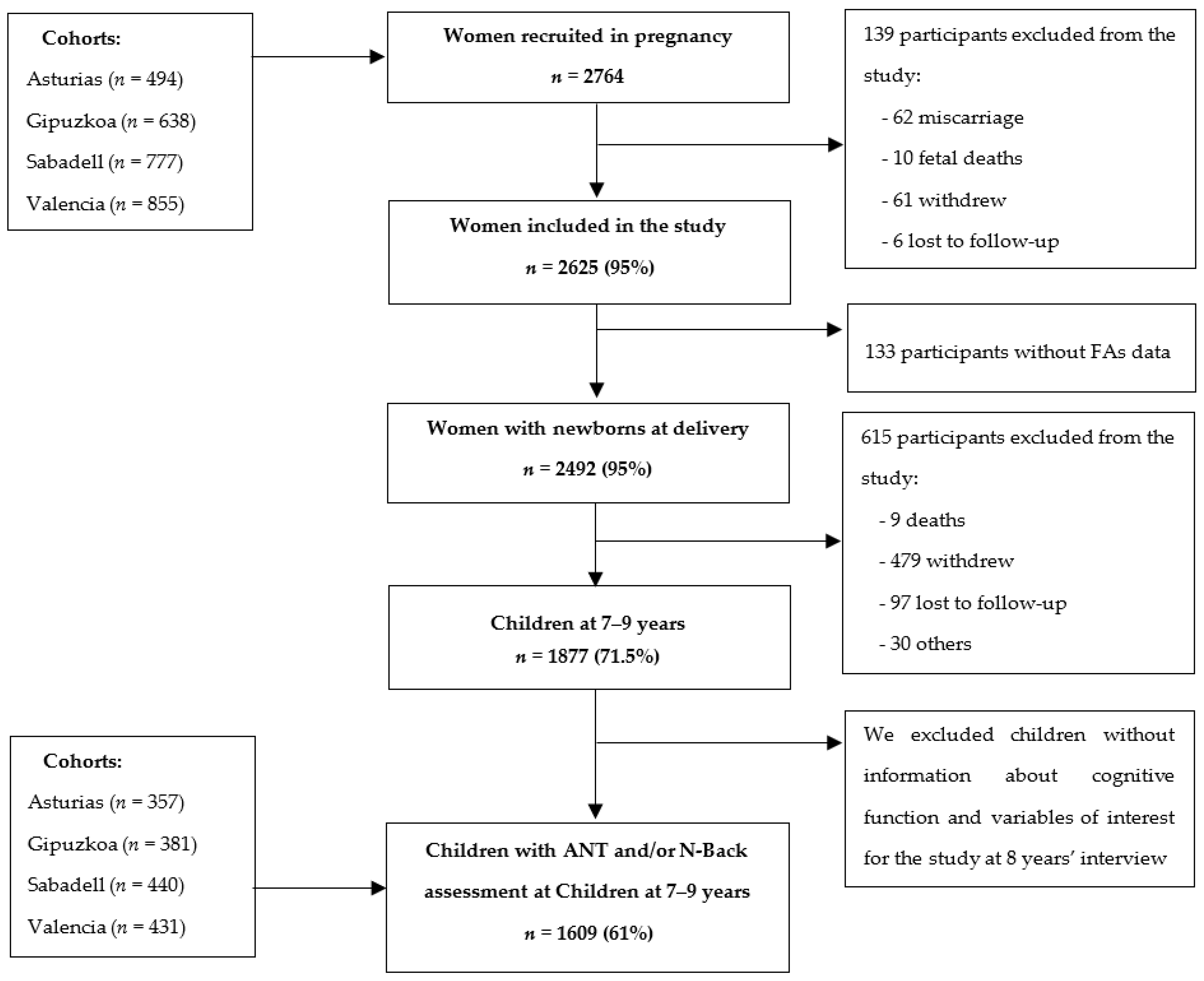
2.1. Study Desing and Population
2.2. FAs Assessment
2.3. Working Memory Assessment in Children
2.4. Attentional Function Assessment in Children
2.5. Other Variables
2.6. Statistical Analysis
3. Results
3.1. Study Population Characteristics
3.2. FAs Use during Pregnancy and Cognitive Outcomes in Children
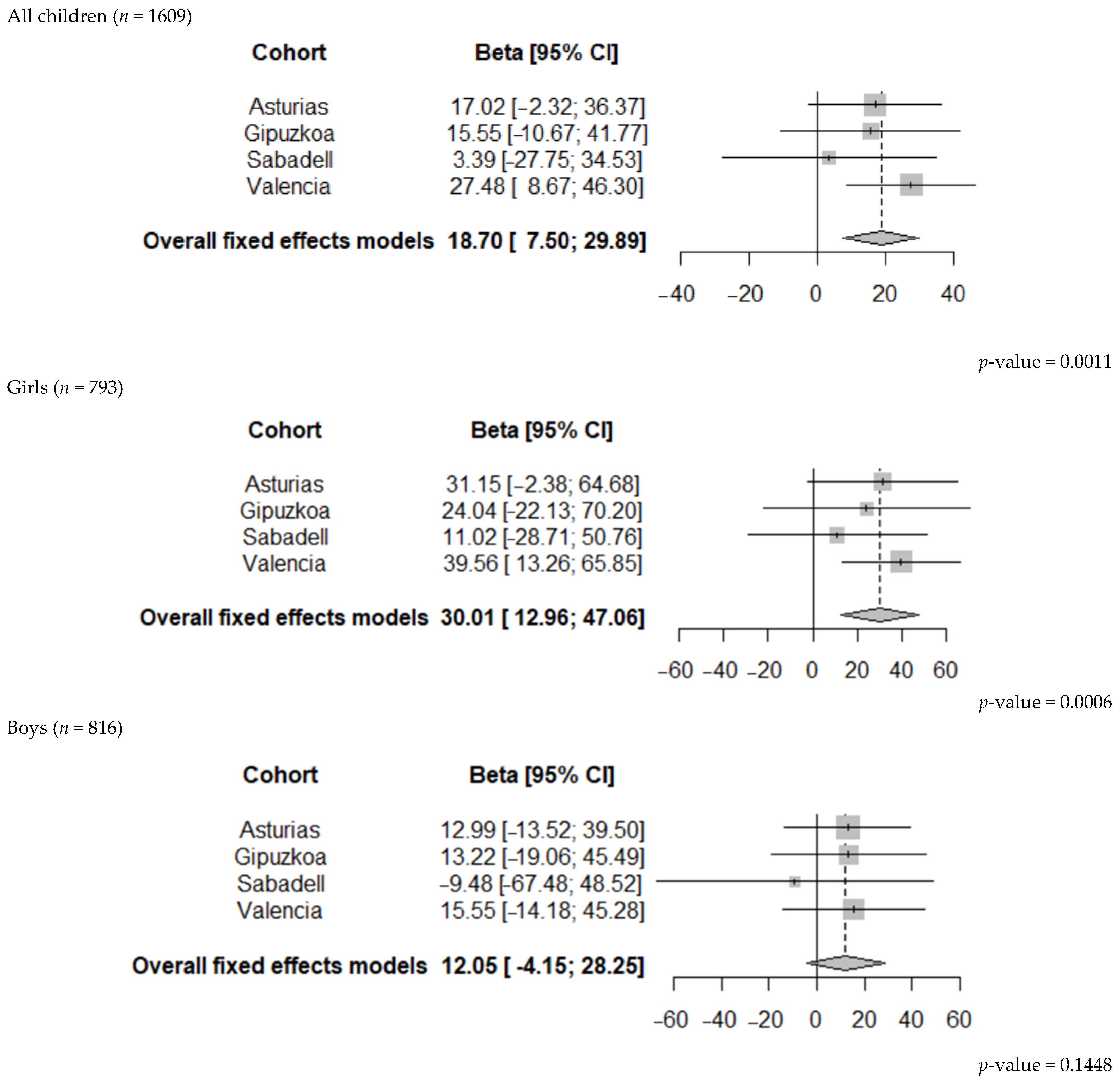
3.3. FAs Use during Pregnancy and Cognitive Outcomes in Children by Sex
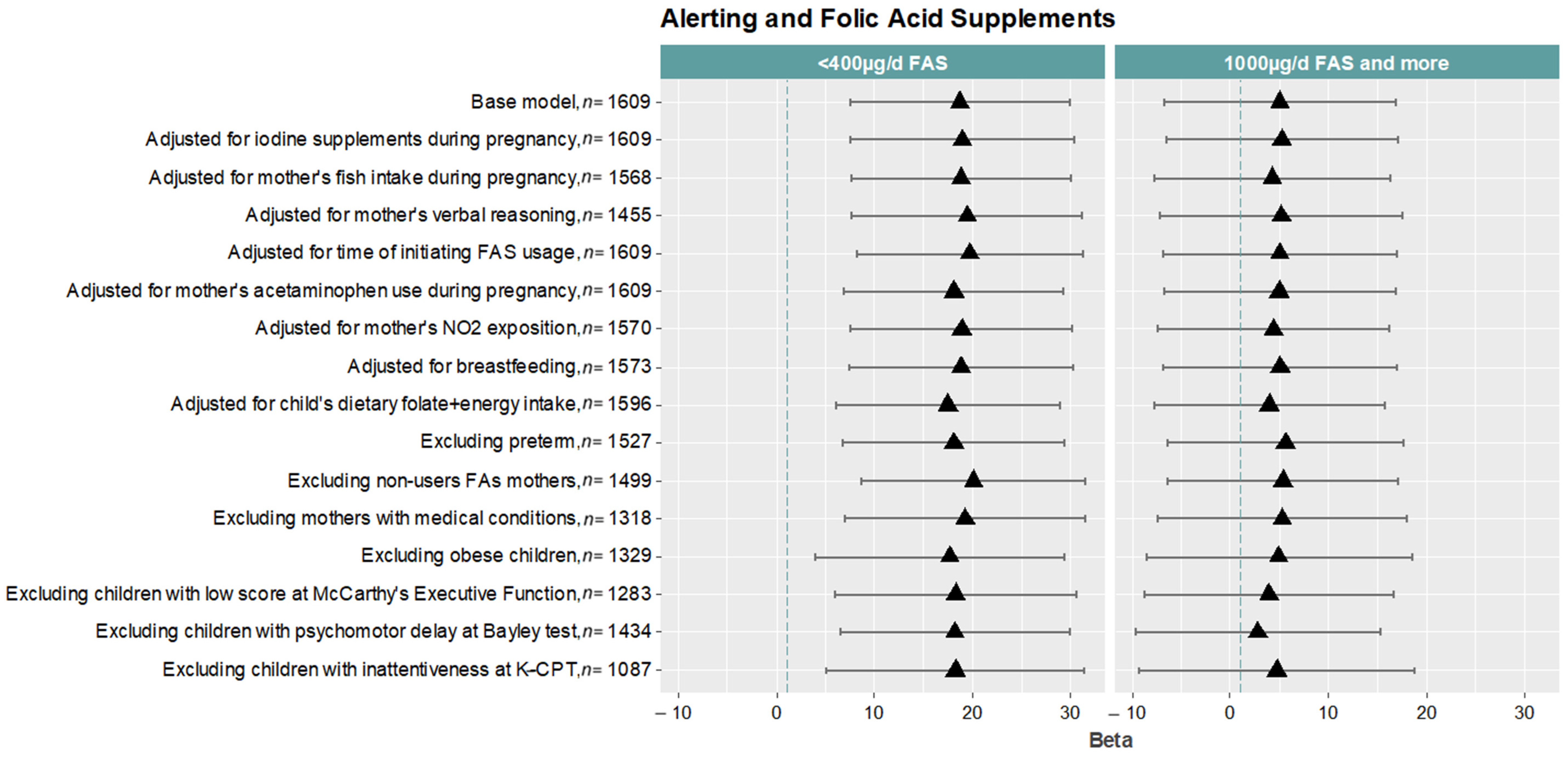
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Czeizel, A.E.; Dudás, I. Prevention of the First Occurrence of Neural-Tube Defects by Periconceptional Vitamin Supplementation. N. Engl. J. Med. 1992, 327, 1832–1835. [Google Scholar] [CrossRef]
- MRC Vitamin Study Research Group. Prevention of Neural Tube Defects: Results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory, J.F.; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development-Folate Review. J. Nutr. 2015, 145, 1636S–1680S. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Salam, R.A.; Haider, B.A.; Bhutta, Z.A. Folic Acid Supplementation during Pregnancy for Maternal Health and Pregnancy Outcomes. Cochrane Database Syst. Rev. 2013, 3, CD006896. [Google Scholar] [CrossRef]
- Desai, A.; Sequeira, J.M.; Quadros, E.V. The Metabolic Basis for Developmental Disorders Due to Defective Folate Transport. Biochimie 2016, 126, 31–42. [Google Scholar] [CrossRef]
- Clare, C.E.; Brassington, A.H.; Kwong, W.Y.; Sinclair, K.D. One-Carbon Metabolism: Linking Nutritional Biochemistry to Epigenetic Programming of Long-Term Development. Annu. Rev. Anim. Biosci. 2019, 7, 263–287. [Google Scholar] [CrossRef]
- Mastrototaro, G.; Zaghi, M.; Sessa, A. Epigenetic Mistakes in Neurodevelopmental Disorders. J. Mol. Neurosci. MN 2017, 61, 590–602. [Google Scholar] [CrossRef]
- Rubini, E.; Baijens, I.M.M.; Horánszky, A.; Schoenmakers, S.; Sinclair, K.D.; Zana, M.; Dinnyés, A.; Steegers-Theunissen, R.P.M.; Rousian, M. Maternal One-Carbon Metabolism during the Periconceptional Period and Human Foetal Brain Growth: A Systematic Review. Genes 2021, 12, 1634. [Google Scholar] [CrossRef]
- Freedman, R.; Hunter, S.K.; Law, A.J.; Clark, A.M.; Roberts, A.; Hoffman, M.C. Choline, Folic Acid, Vitamin D, and Fetal Brain Development in the Psychosis Spectrum. Schizophr. Res. 2021, 247, 16–25. [Google Scholar] [CrossRef]
- Ars, C.L.; Nijs, I.M.; Marroun, H.E.; Muetzel, R.; Schmidt, M.; Steenweg-de Graaff, J.; van der Lugt, A.; Jaddoe, V.W.; Hofman, A.; Steegers, E.A.; et al. Prenatal Folate, Homocysteine and Vitamin B12 Levels and Child Brain Volumes, Cognitive Development and Psychological Functioning: The Generation R Study. Br. J. Nutr. 2019, 122, S1–S9. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (U.S.) (Ed.) Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B₆, Folate, Vitamin B₁₂, Pantothenic Acid, Biotin, and Choline; National Academy Press: Washington, DC, USA, 1998; ISBN 978-0-309-06554-2. [Google Scholar]
- Wojtowicz, A.; Babczyk, D.; Galas, A.; Skalska-Swistek, M.; Gorecka, M.; Witkowski, R.; Huras, H. Evaluation of the Prevalence of Folic Acid Supplementation before Conception and through the First 12 Weeks of Pregnancy in Polish Women at High Risk of Fetal Anomalies. Ginekol. Pol. 2022, 93, 489–495. [Google Scholar] [CrossRef]
- Shields, R.; Khan, O.; Lim Choi Keung, S.; Hawkes, A.J.; Barry, A.; Devall, A.J.; Quinn, S.D.; Keay, S.D.; Arvanitis, T.N.; Bick, D.; et al. Quantitative Assessment of Pregnancy Outcome Following Recurrent Miscarriage Clinic Care: A Prospective Cohort Study. BMJ Open 2022, 12, e052661. [Google Scholar] [CrossRef]
- Missanelli, A.; Lombardi, N.; Bettiol, A.; Lanzi, C.; Rossi, F.; Pacileo, I.; Donvito, L.; Garofalo, V.; Ravaldi, C.; Vannacci, A.; et al. Birth Outcomes in Women Exposed to Diagnostic Radiology Procedures during First Trimester of Pregnancy: A Prospective Cohort Study. Clin. Toxicol. 2022, 60, 175–183. [Google Scholar] [CrossRef]
- Compañ Gabucio, L.M.; García de la Hera, M.; Torres Collado, L.; Fernández-Somoano, A.; Tardón, A.; Guxens, M.; Vrijheid, M.; Rebagliato, M.; Murcia, M.; Ibarluzea, J.; et al. The Use of Lower or Higher Than Recommended Doses of Folic Acid Supplements during Pregnancy Is Associated with Child Attentional Dysfunction at 4–5 Years of Age in the INMA Project. Nutrients 2021, 13, 327. [Google Scholar] [CrossRef]
- Valera-Gran, D.; García de la Hera, M.; Navarrete-Muñoz, E.M.; Fernandez-Somoano, A.; Tardón, A.; Julvez, J.; Forns, J.; Lertxundi, N.; Ibarluzea, J.M.; Murcia, M.; et al. Folic Acid Supplements during Pregnancy and Child Psychomotor Development after the First Year of Life. JAMA Pediatr. 2014, 168, e14261. [Google Scholar] [CrossRef]
- Valera-Gran, D.; Navarrete-Muñoz, E.M.; Garcia de la Hera, M.; Fernández-Somoano, A.; Tardón, A.; Ibarluzea, J.; Balluerka, N.; Murcia, M.; González-Safont, L.; Romaguera, D.; et al. Effect of Maternal High Dosages of Folic Acid Supplements on Neurocognitive Development in Children at 4–5 y of Age: The Prospective Birth Cohort Infancia y Medio Ambiente (INMA) Study. Am. J. Clin. Nutr. 2017, 106, 878–887. [Google Scholar] [CrossRef]
- Tamura, T.; Goldenberg, R.L.; Chapman, V.R.; Johnston, K.E.; Ramey, S.L.; Nelson, K.G. Folate Status of Mothers During Pregnancy and Mental and Psychomotor Development of Their Children at Five Years of Age. Pediatrics 2005, 116, 703–708. [Google Scholar] [CrossRef]
- Gilmore, J.H.; Knickmeyer, R.C.; Gao, W. Imaging Structural and Functional Brain Development in Early Childhood. Nat. Rev. Neurosci. 2018, 19, 123–137. [Google Scholar] [CrossRef]
- Roffman, J.L. Neuroprotective Effects of Prenatal Folic Acid Supplementation: Why Timing Matters. JAMA Psychiatry 2018, 75, 747. [Google Scholar] [CrossRef]
- Naninck, E.F.G.; Stijger, P.C.; Brouwer-Brolsma, E.M. The Importance of Maternal Folate Status for Brain Development and Function of Offspring. Adv. Nutr. 2019, 10, 502–519. [Google Scholar] [CrossRef]
- McNulty, B.; McNulty, H.; Marshall, B.; Ward, M.; Molloy, A.M.; Scott, J.M.; Dornan, J.; Pentieva, K. Impact of Continuing Folic Acid after the First Trimester of Pregnancy: Findings of a Randomized Trial of Folic Acid Supplementation in the Second and Third Trimesters. Am. J. Clin. Nutr. 2013, 98, 92–98. [Google Scholar] [CrossRef]
- McNulty, H.; Rollins, M.; Cassidy, T.; Caffrey, A.; Marshall, B.; Dornan, J.; McLaughlin, M.; McNulty, B.A.; Ward, M.; Strain, J.J.; et al. Effect of Continued Folic Acid Supplementation beyond the First Trimester of Pregnancy on Cognitive Performance in the Child: A Follow-up Study from a Randomized Controlled Trial (FASSTT Offspring Trial). BMC Med. 2019, 17, 196. [Google Scholar] [CrossRef]
- Caffrey, A.; McNulty, H.; Rollins, M.; Prasad, G.; Gaur, P.; Talcott, J.B.; Witton, C.; Cassidy, T.; Marshall, B.; Dornan, J.; et al. Effects of Maternal Folic Acid Supplementation during the Second and Third Trimesters of Pregnancy on Neurocognitive Development in the Child: An 11-Year Follow-up from a Randomised Controlled Trial. BMC Med. 2021, 19, 73. [Google Scholar] [CrossRef]
- Guxens, M.; Ballester, F.; Espada, M.; Fernández, M.F.; Grimalt, J.O.; Ibarluzea, J.; Olea, N.; Rebagliato, M.; Tardón, A.; Torrent, M.; et al. Cohort Profile: The INMA—INfancia y Medio Ambiente—(Environment and Childhood) Project. Int. J. Epidemiol. 2012, 41, 930–940. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Guxens, M.; Vrijheid, M.; Torrent, M.; Ibarluzea, J.; Fano, E.; Llop, S.; Ballester, F.; Fernández, M.F.; Tardón, A.; et al. The INMA—INfancia y Medio Ambiente—(Environment and Childhood) Project: More than 10 Years Contributing to Environmental and Neuropsychological Research. Int. J. Hyg. Environ. Health 2017, 220, 647–658. [Google Scholar] [CrossRef]
- Gonzalez-Palacios, S.; Navarrete-Muñoz, E.-M.; García-de-la-Hera, M.; Torres-Collado, L.; Santa-Marina, L.; Amiano, P.; Lopez-Espinosa, M.-J.; Tardon, A.; Riano-Galan, I.; Vrijheid, M.; et al. Sugar-Containing Beverages Consumption and Obesity in Children Aged 4–5 Years in Spain: The INMA Study. Nutrients 2019, 11, 1772. [Google Scholar] [CrossRef]
- Vioque, J.; Navarrete-Muñoz, E.-M.; Gimenez-Monzó, D.; García-de-la-Hera, M.; Granado, F.; Young, I.S.; Ramón, R.; Ballester, F.; Murcia, M.; Rebagliato, M.; et al. Reproducibility and Validity of a Food Frequency Questionnaire among Pregnant Women in a Mediterranean Area. Nutr. J. 2013, 12, 26. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture (USDA). Agriculture Research Service 2010 USDA National Nutrient Database for Standard Reference; Release 23; Nutrient Data Laboratory: Washington, DC, USA, 2010.
- Palma Linares, I.; Farran, A.; Cantós, D. Tablas de Composición de Alimentos por Medidas Caseras de Consumo Habitual en España=Taules de Composició d’aliments per Mesures Casolanes de Consum Habitual a Espanya; Universitat de Barcelona; McGraw-Hill-Interamericana: Barcelona, Madrid, 2008; ISBN 978-84-481-6090-6. [Google Scholar]
- Owen, A.M.; McMillan, K.M.; Laird, A.R.; Bullmore, E. N-Back Working Memory Paradigm: A Meta-Analysis of Normative Functional Neuroimaging Studies. Hum. Brain Mapp. 2005, 25, 46–59. [Google Scholar] [CrossRef]
- Forns, J.; Esnaola, M.; López-Vicente, M.; Suades-González, E.; Alvarez-Pedrerol, M.; Julvez, J.; Grellier, J.; Sebastián-Gallés, N.; Sunyer, J. The N-Back Test and the Attentional Network Task as Measures of Child Neuropsychological Development in Epidemiological Studies. Neuropsychology 2014, 28, 519–529. [Google Scholar] [CrossRef]
- Sunyer, J.; Esnaola, M.; Alvarez-Pedrerol, M.; Forns, J.; Rivas, I.; López-Vicente, M.; Suades-González, E.; Foraster, M.; Garcia-Esteban, R.; Basagaña, X.; et al. Association between Traffic-Related Air Pollution in Schools and Cognitive Development in Primary School Children: A Prospective Cohort Study. PLoS Med. 2015, 12, e1001792. [Google Scholar] [CrossRef] [Green Version]
- Deserno, L.; Sterzer, P.; Wustenberg, T.; Heinz, A.; Schlagenhauf, F. Reduced Prefrontal-Parietal Effective Connectivity and Working Memory Deficits in Schizophrenia. J. Neurosci. 2012, 32, 12–20. [Google Scholar] [CrossRef]
- Rueda, M.R.; Fan, J.; McCandliss, B.D.; Halparin, J.D.; Gruber, D.B.; Lercari, L.P.; Posner, M.I. Development of Attentional Networks in Childhood. Neuropsychologia 2004, 42, 1029–1040. [Google Scholar] [CrossRef]
- Thomason, M.E.; Race, E.; Burrows, B.; Whitfield-Gabrieli, S.; Glover, G.H.; Gabrieli, J.D.E. Development of Spatial and Verbal Working Memory Capacity in the Human Brain. J. Cogn. Neurosci. 2009, 21, 316–332. [Google Scholar] [CrossRef]
- Suades-González, E.; Forns, J.; García-Esteban, R.; López-Vicente, M.; Esnaola, M.; Álvarez-Pedrerol, M.; Julvez, J.; Cáceres, A.; Basagaña, X.; López-Sala, A.; et al. A Longitudinal Study on Attention Development in Primary School Children with and without Teacher-Reported Symptoms of ADHD. Front. Psychol. 2017, 8, 655. [Google Scholar] [CrossRef]
- Arija, V.; Hernández-Martínez, C.; Tous, M.; Canals, J.; Guxens, M.; Fernández-Barrés, S.; Ibarluzea, J.; Babarro, I.; Soler-Blasco, R.; Llop, S.; et al. Association of Iron Status and Intake During Pregnancy with Neuropsychological Outcomes in Children Aged 7 Years: The Prospective Birth Cohort Infancia y Medio Ambiente (INMA) Study. Nutrients 2019, 11, 2999. [Google Scholar] [CrossRef]
- Gignac, F.; Solé, C.; Barrera-Gómez, J.; Persavento, C.; Tena, È.; López-Vicente, M.; Júlvez, J.; Sunyer, J.; Couso, D.; Basagaña, X. Identifying Factors Influencing Attention in Adolescents with a Co-Created Questionnaire: A Citizen Science Approach with Secondary Students in Barcelona, Spain. Int. J. Environ. Res. Public. Health 2021, 18, 8221. [Google Scholar] [CrossRef]
- Antón, E.; Duñabeitia, J.A.; Estévez, A.; Hernández, J.A.; Castillo, A.; Fuentes, L.J.; Davidson, D.J.; Carreiras, M. Is There a Bilingual Advantage in the ANT Task? Evidence from Children. Front. Psychol. 2014, 5, 398. [Google Scholar] [CrossRef]
- Yu, C.; Yao, W. Robust Linear Regression: A Review and Comparison. Commun. Stat. Simul. Comput. 2017, 46, 6261–6282. [Google Scholar] [CrossRef]
- Nikoloulopoulos, A.K.; Karlis, D. On Modeling Count Data: A Comparison of Some Well-Known Discrete Distributions. J. Stat. Comput. Simul. 2008, 78, 437–457. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Wu, K.; Taki, Y.; Sato, K.; Hashizume, H.; Sassa, Y.; Takeuchi, H.; Thyreau, B.; He, Y.; Evans, A.C.; Li, X.; et al. Topological Organization of Functional Brain Networks in Healthy Children: Differences in Relation to Age, Sex, and Intelligence. PLoS ONE 2013, 8, e55347. [Google Scholar] [CrossRef]
- Wheelock, M.D.; Hect, J.L.; Hernandez-Andrade, E.; Hassan, S.S.; Romero, R.; Eggebrecht, A.T.; Thomason, M.E. Sex Differences in Functional Connectivity during Fetal Brain Development. Dev. Cogn. Neurosci. 2019, 36, 100632. [Google Scholar] [CrossRef]
- Vioque, J.; Garcia-de-la-Hera, M.; Gonzalez-Palacios, S.; Torres-Collado, L.; Notario-Barandiaran, L.; Oncina-Canovas, A.; Soler-Blasco, R.; Lozano, M.; Beneito, A.; Navarrete-Muñoz, E.-M. Reproducibility and Validity of a Short Food Frequency Questionnaire for Dietary Assessment in Children Aged 7–9 Years in Spain. Nutrients 2019, 11, 933. [Google Scholar] [CrossRef]
- Liu, H.-Y.; Liu, S.-M.; Zhang, Y.-Z. Maternal Folic Acid Supplementation Mediates Offspring Health via DNA Methylation. Reprod. Sci. 2020, 27, 963–976. [Google Scholar] [CrossRef]
- Irwin, R.E.; Pentieva, K.; Cassidy, T.; Lees-Murdock, D.J.; McLaughlin, M.; Prasad, G.; McNulty, H.; Walsh, C.P. The Interplay between DNA Methylation, Folate and Neurocognitive Development. Epigenomics 2016, 8, 863–879. [Google Scholar] [CrossRef]
- del Río Garcia, C.; Torres-Sánchez, L.; Chen, J.; Schnaas, L.; Hernández, C.; Osorio, E.; Portillo, M.G.; López-Carrillo, L. Maternal MTHFR 677C>T Genotype and Dietary Intake of Folate and Vitamin B 12: Their Impact on Child Neurodevelopment. Nutr. Neurosci. 2009, 12, 13–20. [Google Scholar] [CrossRef]
- Federico, F.; Marotta, A.; Martella, D.; Casagrande, M. Development in Attention Functions and Social Processing: Evidence from the Attention Network Test. Br. J. Dev. Psychol. 2017, 35, 169–185. [Google Scholar] [CrossRef]
- Mullane, J.C.; Lawrence, M.A.; Corkum, P.V.; Klein, R.M.; McLaughlin, E.N. The Development of and Interaction among Alerting, Orienting, and Executive Attention in Children. Child Neuropsychol. 2016, 22, 155–176. [Google Scholar] [CrossRef] [PubMed]
- Vuontela, V.; Carlson, S.; Troberg, A.-M.; Fontell, T.; Simola, P.; Saarinen, S.; Aronen, E.T. Working Memory, Attention, Inhibition, and Their Relation to Adaptive Functioning and Behavioral/Emotional Symptoms in School-Aged Children. Child Psychiatry Hum. Dev. 2013, 44, 105–122. [Google Scholar] [CrossRef]
- Anderson, P. Assessment and Development of Executive Function (EF) During Childhood. Child Neuropsychol. 2002, 8, 71–82. [Google Scholar] [CrossRef]
- Vuontela, V.; Steenari, M.-R.; Aronen, E.T.; Korvenoja, A.; Aronen, H.J.; Carlson, S. Brain Activation and Deactivation during Location and Color Working Memory Tasks in 11–13-Year-Old Children. Brain Cogn. 2009, 69, 56–64. [Google Scholar] [CrossRef] [PubMed]
- López-Vicente, M.; Forns, J.; Suades-González, E.; Esnaola, M.; García-Esteban, R.; Álvarez-Pedrerol, M.; Júlvez, J.; Burgaleta, M.; Sebastián-Gallés, N.; Sunyer, J. Developmental Trajectories in Primary Schoolchildren Using N-Back Task. Front. Psychol. 2016, 7, 716. [Google Scholar] [CrossRef] [PubMed]
- Veena, S.R.; Krishnaveni, G.V.; Srinivasan, K.; Wills, A.K.; Muthayya, S.; Kurpad, A.V.; Yajnik, C.S.; Fall, C.H.D. Higher Maternal Plasma Folate but Not Vitamin B-12 Concentrations during Pregnancy Are Associated with Better Cognitive Function Scores in 9-to 10-Year-Old Children in South India. J. Nutr. 2010, 140, 1014–1022. [Google Scholar] [CrossRef]
- Caffrey, A.; Irwin, R.E.; McNulty, H.; Strain, J.J.; Lees-Murdock, D.J.; McNulty, B.A.; Ward, M.; Walsh, C.P.; Pentieva, K. Gene-Specific DNA Methylation in Newborns in Response to Folic Acid Supplementation during the Second and Third Trimesters of Pregnancy: Epigenetic Analysis from a Randomized Controlled Trial. Am. J. Clin. Nutr. 2018, 107, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Deoni, S.C.L.; Dean, D.C.; O’Muircheartaigh, J.; Dirks, H.; Jerskey, B.A. Investigating White Matter Development in Infancy and Early Childhood Using Myelin Water Faction and Relaxation Time Mapping. NeuroImage 2012, 63, 1038–1053. [Google Scholar] [CrossRef] [PubMed]
- Vuontela, V.; Steenari, M.-R.; Carlson, S.; Koivisto, J.; Fjällberg, M.; Aronen, E.T. Audiospatial and Visuospatial Working Memory in 6–13 Year Old School Children. Learn. Mem. 2003, 10, 74–81. [Google Scholar] [CrossRef]
- Pelegrina, S.; Lechuga, M.T.; García-Madruga, J.A.; Elosúa, M.R.; Macizo, P.; Carreiras, M.; Fuentes, L.J.; Bajo, M.T. Normative Data on the N-Back Task for Children and Young Adolescents. Front. Psychol. 2015, 6, 1544. [Google Scholar] [CrossRef]
- Maruvada, P.; Stover, P.J.; Mason, J.B.; Bailey, R.L.; Davis, C.D.; Field, M.S.; Finnell, R.H.; Garza, C.; Green, R.; Gueant, J.-L.; et al. Knowledge Gaps in Understanding the Metabolic and Clinical Effects of Excess Folates/Folic Acid: A Summary, and Perspectives, from an NIH Workshop. Am. J. Clin. Nutr. 2020, 112, 1390–1403. [Google Scholar] [CrossRef]
- Balart, P.; Oosterveen, M. Females Show More Sustained Performance during Test-Taking than Males. Nat. Commun. 2019, 10, 3798. [Google Scholar] [CrossRef]
- Navarrete-Muñoz, E.M.; Valera-Gran, D.; Garcia-de-la-Hera, M.; Gonzalez-Palacios, S.; Riaño, I.; Murcia, M.; Lertxundi, A.; Guxens, M.; Tardón, A.; Amiano, P.; et al. High Doses of Folic Acid in the Periconceptional Period and Risk of Low Weight for Gestational Age at Birth in a Population Based Cohort Study. Eur. J. Nutr. 2019, 58, 241–251. [Google Scholar] [CrossRef]
- Pastor-Valero, M.; Navarrete-Muñoz, E.M.; Rebagliato, M.; Iñiguez, C.; Murcia, M.; Marco, A.; Ballester, F.; Vioque, J. Periconceptional Folic Acid Supplementation and Anthropometric Measures at Birth in a Cohort of Pregnant Women in Valencia, Spain. Br. J. Nutr. 2011, 105, 1352–1360. [Google Scholar] [CrossRef]
- Husebye, E.S.N.; Wendel, A.W.K.; Gilhus, N.E.; Riedel, B.; Bjørk, M.H. Plasma Unmetabolized Folic Acid in Pregnancy and Risk of Autistic Traits and Language Impairment in Antiseizure Medication-Exposed Children of Women with Epilepsy. Am. J. Clin. Nutr. 2022, nqab436. [Google Scholar] [CrossRef]
- Papadopoulou, E.; Stratakis, N.; Roumeliotaki, T.; Sarri, K.; Merlo, D.F.; Kogevinas, M.; Chatzi, L. The Effect of High Doses of Folic Acid and Iron Supplementation in Early-to-Mid Pregnancy on Prematurity and Fetal Growth Retardation: The Mother–Child Cohort Study in Crete, Greece (Rhea Study). Eur. J. Nutr. 2013, 52, 327–336. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Vereczkey, A.; Szabó, I. Folic Acid in Pregnant Women Associated with Reduced Prevalence of Severe Congenital Heart Defects in Their Children: A National Population-Based Case-Control Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 193, 34–39. [Google Scholar] [CrossRef]
- Mavrogenis, S.; Urban, R.; Czeizel, A.E.; Ács, N. Possible Preventive Effect of High Doses of Folic Acid for Isolated Hypospadias: A National Population-Based Case-Control Study. Am. J. Med. Genet. A 2014, 164, 3108–3114. [Google Scholar] [CrossRef]
- Chatzi, L.; Papadopoulou, E.; Koutra, K.; Roumeliotaki, T.; Georgiou, V.; Stratakis, N.; Lebentakou, V.; Karachaliou, M.; Vassilaki, M.; Kogevinas, M. Effect of High Doses of Folic Acid Supplementation in Early Pregnancy on Child Neurodevelopment at 18 Months of Age: The Mother-Child Cohort “Rhea” Study in Crete, Greece. Public Health Nutr. 2012, 15, 1728–1736. [Google Scholar] [CrossRef]
- Julvez, J.; López-Vicente, M.; Warembourg, C.; Maitre, L.; Philippat, C.; Gützkow, K.B.; Guxens, M.; Evandt, J.; Andrusaityte, S.; Burgaleta, M.; et al. Early Life Multiple Exposures and Child Cognitive Function: A Multi-Centric Birth Cohort Study in Six European Countries. Environ. Pollut. Barking Essex 1987 2021, 284, 117404. [Google Scholar] [CrossRef]
- Sagiv, S.K.; Thurston, S.W.; Bellinger, D.C.; Altshul, L.M.; Korrick, S.A. Neuropsychological Measures of Attention and Impulse Control among 8-Year-Old Children Exposed Prenatally to Organochlorines. Environ. Health Perspect. 2012, 120, 904–909. [Google Scholar] [CrossRef]
- Herzog, A.G.; MacEachern, D.B.; Mandle, H.B.; Cahill, K.E.; Fowler, K.M.; Davis, A.R.; Allen Hauser, W. Folic Acid Use by Women with Epilepsy: Findings of the Epilepsy Birth Control Registry. Epilepsy Behav. 2017, 72, 156–160. [Google Scholar] [CrossRef]
- Cai, S.; Quan, S.; Yang, G.; Chen, M.; Ye, Q.; Wang, G.; Yu, H.; Wang, Y.; Qiao, S.; Zeng, X. Nutritional Status Impacts Epigenetic Regulation in Early Embryo Development: A Scoping Review. Adv. Nutr. 2021, 12, 1877–1892. [Google Scholar] [CrossRef]
- Li, M.; Francis, E.; Hinkle, S.N.; Ajjarapu, A.S.; Zhang, C. Preconception and Prenatal Nutrition and Neurodevelopmental Disorders: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1628. [Google Scholar] [CrossRef]
- Clare, C.E.; Pestinger, V.; Kwong, W.Y.; Tutt, D.A.R.; Xu, J.; Byrne, H.M.; Barrett, D.A.; Emes, R.D.; Sinclair, K.D. Interspecific Variation in One-Carbon Metabolism within the Ovarian Follicle, Oocyte, and Preimplantation Embryo: Consequences for Epigenetic Programming of DNA Methylation. Int. J. Mol. Sci. 2021, 22, 1838. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Cohorts, n = 1609 | Valencia, n = 431 | Sabadell, n = 440 | Asturias, n = 357 | Gipuzkoa, n = 381 | p-Value 1 | |
|---|---|---|---|---|---|---|
| Mother’s age, y | 31 (28; 34) | 30 (28; 33) | 30 (28; 33) | 32 (29; 35) | 31 (29; 33) | <0.001 |
| Mother’s education | <0.001 | |||||
| Primary or less | 300 (18.7) | 111 (25.8) | 102 (23.2) | 48 (13.4) | 39 (10.2) | |
| Secondary | 671 (41.7) | 186 (43.2) | 191 (43.4) | 160 (44.8) | 134 (35.2) | |
| University | 638 (39.7) | 134 (31.1) | 147 (33.4) | 149 (41.7) | 208 (54.6) | |
| Mother’s social class | <0.001 | |||||
| I + II (high) | 406 (25.2) | 89 (20.6) | 100 (22.7) | 88 (24.6) | 129 (33.9) | |
| III | 450 (28.0) | 117 (27.1) | 144 (32.7) | 76 (21.3) | 113 (29.7) | |
| IV + V (low) | 753 (46.8) | 225 (52.2) | 196 (44.5) | 193 (54.1) | 139 (36.5) | |
| Parity ≥ 1 | 680 (42.3) | 189 (43.9) | 188 (42.7) | 137 (38.4) | 166 (43.6) | 0.398 |
| Overall tobacco exposition during pregnancy, yes | 934 (58.1) | 315 (73.1) | 260 (59.1) | 156 (43.7) | 203 (53.3) | <0.001 |
| Missing values | 41 (2.6) | 5 (1.2) | 8 (1.8) | 18 (5.0) | 10 (2.6) | |
| Prepregnancy mother’s BMI, kg/m2 | 0.008 | |||||
| <25 | 1183 (73.5) | 311 (72.2) | 317 (72.0) | 248 (69.5) | 307 (80.6) | |
| ≥25–30 | 311 (19.3) | 85 (19.7) | 84 (19.1) | 84 (23.5) | 58 (15.2) | |
| ≥30 | 115 (7.2) | 35 (8.1) | 39 (8.9) | 25 (7.0) | 16 (4.2) | |
| Prepregnancy father’s BMI, kg/m2 | <0.001 | |||||
| <25 | 687 (42.7) | 187 (43.4) | 204 (46.4) | 114 (31.9) | 182 (47.8) | |
| ≥25–30 | 704 (43.6) | 199 (46.2) | 170 (38.6) | 175 (49.0) | 160 (42.0) | |
| ≥30 | 189 (11.8) | 45 (10.4) | 60 (13.6) | 55 (15.4) | 29 (7.6) | |
| Missing values | 29 (1.8) | 0 (0.0) | 6 (1.4) | 13 (3.6) | 10 (2.6) | |
| Dietary folate, µg/d | ||||||
| In 1st period of pregnancy | 297 (239; 364) | 292 (231; 359) | 283 (230; 347) | 313 (247; 382) | 306 (255; 367) | <0.001 |
| In 2nd period of pregnancy | 297 (241; 358) | 274 (219; 349) | 291 (237; 345) | 302 (245; 367) | 312 (266; 370) | <0.001 |
| FAs µg/d, in 1st period of pregnancy | <0.001 | |||||
| 400–999 | 233 (14.5) | 68 (15.8) | 45 (10.2) | 64 (17.9) | 56 (14.7) | |
| <400 | 874 (54.3) | 249 (57.8) | 287 (65.2) | 164 (45.9) | 174 (45.7) | |
| ≥1000 | 502 (31.2) | 114 (26.5) | 108 (24.5) | 129 (36.1) | 151 (39.6) | |
| FAs µg/d, in 2nd period of pregnancy | <0.001 | |||||
| 400–999 | 426 (26.5) | 200 (46.4) | 52 (11.8) | 133 (37.3) | 41 (10.8) | |
| <400 | 907 (56.4) | 144 (33.4) | 366 (83.2) | 100 (28.0) | 297 (78.0) | |
| ≥1000 | 276 (17.2) | 87 (20.2) | 22 (5.0) | 124 (34.7) | 43 (11.3) | |
| Child’s sex | 0.631 | |||||
| Boys | 816 (50.7) | 210 (48.7) | 229 (52.0) | 188 (52.7) | 189 (49.6) | |
| Girls | 793 (49.3) | 221 (51.3) | 211 (48.0) | 169 (47.3) | 192 (50.4) | |
| Child’s age 2, in years | 7.7 (7.3; 8.0) | 7.6 (7.4; 7.6) | 6.8 (6.6; 7.1) | 8.3 (8.1; 8.4) | 7.9 (7.8; 8.0) | <0.001 |
| ANT outcomes | ||||||
| HRT-SE, ms | 305.6 (245; 364) | 323.2 (266; 382) | 320.3 (260; 369) | 260.8 (196; 329) | 304.3 (259; 356) | <0.001 |
| Accuracy | 1.0 (1.0; 1.0) | 1.0 (0.9; 1.0) | 1.0 (0.9; 1.0) | 1.0 (1.0; 1.0) | 1.0 (1.0; 1.0) | <0.001 |
| Comission errors, num | 3 (1; 5) | 4 (2; 7) | 4 (2; 7) | 1 (0; 3) | 2 (1; 4) | <0.001 |
| Omission errors, num | 2 (0; 5) | 3 (1; 7) | 2 (1; 5) | 0 (0; 2) | 2 (0; 4) | <0.001 |
| Alerting | 45 (−3.5; 100.5) | 52 (0.8; 101.8) | 39 (−10.6; 100.9) | 45 (4.0; 90.5) | 48.5 (−6.0; 108.0) | 0.314 |
| Orienting | 38.5 (−14.0; 85.0) | 40.0 (−15.5; 88.5) | 30.5 (−17.5; 81.3) | 41.5 (0.0; 83.0) | 38.0 (−17.0; 85.5) | 0.358 |
| Conflict, ms | 71 (32.5; 115) | 68.5 (28.5; 111) | 75.5 (35.9; 122) | 63.0 (33.5; 101) | 78.0 (36.0; 128) | 0.004 |
| N-back outcomes | ||||||
| d’ numbers 1-back | 3.9 (3.4; 3.9) | 3.9 (2.8; 3.9) | 3.9 (2.6; 3.9) | 3.9 (3.9; 3.9) | 3.9 (3.9; 3.9) | <0.001 |
| d’ numbers 2-back | 1.9 (1.1; 2.6) | 1.7 (1.0; 2.5) | 1.7 (1.0; 2.3) | 2.3 (1.5; 3.9) | 2.0 (1.3; 2.7) | <0.001 |
| d’ numbers 3-back | 1.1 (0.6; 1.7) | 1.0 (0.3; 1.7) | 1.0 (0.3; 1.4) | 1.4 (1.0; 2.2) | 1.4 (1.0; 1.9) | <0.001 |
| Periconceptional Period a | Second Period a | Entire Pregnancy a | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Attentional Network Test (n = 1609) | FAS (µg/d) | n | β b | (95% CI) | n | β b | (95% CI) | n | β b | (95% CI) |
| HRT-SE (ms) c | 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | |||
| <400 | 874 | −4.07 | (−15.86; 7.73) | 907 | −5.02 | (−16.21; 6.17) | 885 | −4.64 | (−15.85; 6.56) | |
| ≥1000 | 502 | −6.52 | (−19.09; 6.04) | 276 | −7.98 # | (−29.37; 13.41) | 425 | −10.96 | (−23.23; 1.31) | |
| Accuracy | 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | |||
| <400 | 874 | 0.00 | (−0.00; 0.00) | 907 | −0.00 | (−0.00; 0.00) | 885 | −0.00 | (−0.01; 0.00) | |
| ≥1000 | 502 | 0.00 | (−0.00; 0.00) | 276 | 0.00 | (−0.00; 0.01) | 425 | 0.00 | (−0.00; 0.01) | |
| Commission errors (num) c | 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | |||
| <400 | 874 | 0.94 | (0.82; 1.08) | 907 | 1.02 | (0.89; 1.14) | 885 | 1.05 | (0.92; 1.19) | |
| ≥1000 | 502 | 0.90 | (0.77; 1.04) | 276 | 1.00 | (0.87; 1.16) | 425 | 0.99 | (0.86; 1.14) | |
| Omission errors (num) c | 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | |||
| <400 | 874 | 1.08 | (0.90; 1.30) | 907 | 0.96 # | (0.74; 1.25) | 885 | 0.96 | (0.81; 1.14) | |
| ≥1000 | 502 | 0.94 | (0.77; 1.15) | 276 | 0.87 | (0.71; 1.06) | 425 | 0.85 | (0.70; 1.04) | |
| Alerting c | 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | |||
| <400 | 874 | −7.83 | (−21.56; 5.90) | 907 | 18.70 * | (7.51; 29.89) | 885 | 6.27 | (−5.56; 18.11) | |
| ≥1000 | 502 | −8.33 | (−22.52; 5.86) | 276 | 5.03 | (−6.72; 16.77) | 425 | −1.05 | (−13.29; 11.20) | |
| 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | ||||
| Orienting c | <400 | 874 | −5.95 # | (−29.52; 17.62) | 907 | 1.03 | (−9.38; 11.44) | 885 | 2.23 | (−9.03; 13.48) |
| ≥1000 | 502 | −8.25 # | (−27.26; 10.77) | 276 | −0.91 | (−13.66; 11.84) | 425 | −0.86 | (−13.29; 11.54) | |
| 400–999 | 233 | Ref. | 426 | Ref. | 299 | Ref. | ||||
| Conflict (ms) c | <400 | 874 | 3.78 | (−5.65; 13.21) | 907 | −0.62 | (−8.99; 7.76) | 885 | −1.71 | (−10.63; 7.21) |
| ≥1000 | 502 | 6.51 | (−3.47; 16.49) | 276 | 1.69 | (−7.80; 11.18) | 425 | −2.81 | (−12.57; 6.95) | |
| N-back task (n = 1312) | ||||||||||
| d’ number 2-back | 400–999 | 193 | Ref. | 346 | Ref. | 238 | Ref. | |||
| <400 | 703 | −0.04 | (−0.23; 0.14) | 721 | −0.14 | (−0.31; 0.03) | 709 | 0.10 | (−0.08; 0.28) | |
| ≥1000 | 416 | −0.05 | (−0.24; 0.15) | 245 | −0.03 | (−0.22; 0.16) | 365 | 0.15 | (−0.04; 0.34) | |
| d’ number 3-back | 400–999 | 276 | Ref. | 346 | Ref. | 238 | Ref. | |||
| <400 | 829 | 0.05 | (−0.11; 0.21) | 721 | 0.06 | (−0.09; 0.20) | 709 | 0.03 | (−0.12; 0.19) | |
| ≥1000 | 398 | 0.03 | (−0.13; 0.20) | 245 | 0.00 | (−0.16; 0.16) | 365 | 0.05 | (−0.12; 0.21) | |
| Periconceptional Period a | Second Period a | Entire Pregnancy a | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Attentional Network Test (n = 793) | FAS (µg/d) | n | β b | (95% CI) | n | β b | (95% CI) | n | β b | (95% CI) |
| HRT-SE (ms) c | 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | |||
| <400 | 425 | −3.33 | (−18.37; 11.62) | 437 | −14.25 | (−29.15; 0.64) | 215 | −15.85 | (−32.61; 0.91) | |
| ≥1000 | 239 | −3.22 # | (−30.25; 23.81) | 140 | −7.49 # | (−42.23; 27.25) | 133 | −20.38 * | (−39.12; −1.63) | |
| Accuracy | 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | |||
| <400 | 425 | −0.00 | (−0.01; 0.01) | 437 | 0.00 | (−0.00; 0.01) | 215 | −0.00 | (−0.01; 0.00) | |
| ≥1000 | 239 | 0.00 | (−0.00; 0.01) | 140 | 0.00 | (−0.00; 0.01) | 133 | −0.00 | (−0.01; 0.01) | |
| Commission errors (num) c | 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | |||
| <400 | 425 | 1.00 # | (0.64; 1.35) | 437 | 0.88 | (0.75; 1.04) | 215 | 0.98 | (0.82; 1.18) | |
| ≥1000 | 239 | 0.93 | (0.76; 1.14) | 140 | 0.88 | (0.72; 1.08) | 133 | 0.97 | (0.79; 1.19) | |
| Omission errors (num) c | 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | |||
| <400 | 425 | 1.21 | (0.95; 1.54) | 437 | 1.03 # | (0.58; 1.84) | 215 | 0.85 | (0.66; 1.09) | |
| ≥1000 | 239 | 0.93 | (0.72; 1.22) | 140 | 0.97 # | (0.46; 2.03) | 133 | 0.75 | (0.49; 1.16) | |
| Alerting c | 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | |||
| <400 | 425 | −17.93 | (−39.81; 3.95) | 437 | 30.01 | (12.96; 47.01) * | 215 | 8.96 | (−11.55; 29.48) | |
| ≥1000 | 239 | −16.14 | (−38.53; 6.25) | 140 | 6.23 | (−10.86; 23.32) | 133 | −0.41 | (−21.04; 20.23) | |
| 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | ||||
| Orienting c | <400 | 425 | −18.07 # | (−42.59; 6.44) | 437 | 4.37 | (−11.06; 19.80) | 215 | 3.80 | (−14.72; 22.31) |
| ≥1000 | 239 | −12.47 | (−29.91; 4.97) | 140 | 13.27 | (−4.56; 31.10) | 133 | 7.65 | (−11.74; 27.04) | |
| 400–999 | 129 | Ref. | 216 | Ref. | 445 | Ref. | ||||
| Conflict (ms) c | <400 | 425 | 7.88 | (−5.98; 21.73) | 437 | 1.74 | (−11.32; 14.81) | 215 | 5.06 | (−9.98; 20.11) |
| ≥1000 | 239 | 11.60 | (−3.51; 26.71) | 140 | 1.77 | (−12.15; 15.69) | 133 | 3.70 | (−12.04; 19.44) | |
| N-back task (n = 639) | ||||||||||
| d’ number 2-back | 400–999 | 107 | Ref. | 168 | Ref. | 106 | Ref. | |||
| <400 | 336 | −0.01 | (−0.25; 0.23) | 343 | −0.06 | (−0.29; 0.18) | 351 | 0.21 | (−0.05; 0.46) | |
| ≥1000 | 196 | 0.00 | (−0.26; 0.26) | 128 | 0.09 | (−0.18; 0.36) | 182 | 0.28 * | (0.01; 0.56) | |
| d’ number 3-back | 400–999 | 107 | Ref. | 168 | Ref. | 106 | Ref. | |||
| <400 | 336 | −0.06 | (−0.27; 0.16) | 343 | 0.14 | (−0.07; 0.34) | 351 | 0.12 | (−0.11; 0.34) | |
| ≥1000 | 196 | 0.09 | (−0.14; 0.32) | 128 | 0.14 | (−0.10; 0.37) | 182 | 0.32 * | (0.08; 0.56) | |
| Periconceptional Period a | Second Period a | Entire Pregnancy a | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Attentional Network Test (n = 816) | FAS (µg/d) | n | β b | (95% CI) | n | β b | (95% CI) | n | β b | (95% CI) |
| HRT-SE (ms) c | 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | |||
| <400 | 449 | −8.92 | (−27.00; 9.16) | 470 | 7.19 | (−10.05; 24.43) | 440 | 5.15 | (−10.20; 20.50) | |
| ≥1000 | 263 | −8.59 | (−27.10; 9.92) | 136 | −3.20 | (−23.69; 17.28) | 210 | −2.35 | (−19.44; 14.73) | |
| Accuracy | 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | |||
| <400 | 449 | 0.01 | (−0.00; 0.01) | 470 | −0.00 | (−0.01; 0.00) | 440 | 0.00 | (−0.00; 0.01) | |
| ≥1000 | 263 | 0.01 | (−0.00; 0.01) | 136 | −0.00 | (−0.01; 0.01) | 210 | 0.00 | (−0.00; 0.01) | |
| Commission errors (num) c | 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | |||
| <400 | 449 | 0.88 | (0.72; 1.07) | 470 | 1.15 | (0.97; 1.37) | 440 | 1.04 | (0.87; 1.23) | |
| ≥1000 | 263 | 0.84 | (0.68; 1.03) | 136 | 1.06 | (0.86; 1.29) | 210 | 0.94 | (0.78; 1.14) | |
| Omission errors (num) c | 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | |||
| <400 | 449 | 1.05 | (0.79; 1.39) | 470 | 1.02 | (0.80; 1.30) | 440 | 1.10 | (0.87; 1.40) | |
| ≥1000 | 263 | 1.05 | (0.79; 1.41) | 136 | 0.99 | (0.74; 1.31) | 210 | 1.00 # | (0.61; 1.61) | |
| Alerting c | 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | |||
| <400 | 449 | 2.08 | (−16.12; 20.28) | 470 | 12.05 | (−4.15; 28.25) | 440 | 2.75 | (−12.31; 17.81) | |
| ≥1000 | 263 | 1.16 | (−18.37; 20.70) | 136 | 7.84 | (−9.81; 25.49) | 210 | 0.52 | (−15.97; 17.02) | |
| 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | ||||
| Orienting c | <400 | 449 | 9.27 | (−7.58; 26.12) | 470 | −0.20 | (−15.00; 14.61) | 440 | 1.12 # | (−23.82; 26.05) |
| ≥1000 | 263 | −1.66 | (−19.91; 16.59) | 136 | −14.31 | (−32.49; 3.88) | 210 | −6.17 | (−22.30; 9.95) | |
| 400–999 | 104 | Ref. | 210 | Ref. | 166 | Ref. | ||||
| Conflict (ms) c | <400 | 449 | 2.44 | (−11.16; 16.05) | 470 | −2.25 | (−14.45; 9.96) | 440 | −5.38 | (−17.30; 6.53) |
| ≥1000 | 263 | 2.22 | (−11.48; 15.91) | 136 | 0.48 | (−13.18; 14.14) | 210 | −5.78 | (−18.74; 7.18) | |
| N-back task (n = 673) | ||||||||||
| d’ number 2-back | 400–999 | 86 | Ref. | 178 | Ref. | 132 | Ref. | |||
| <400 | 367 | −0.10 | (−0.38; 0.17) | 378 | −0.25 * | (−0.49; 0.01) | 358 | 0.07 | (−0.17; 0.31) | |
| ≥1000 | 220 | −0.07 | (−0.36; 0.21) | 117 | −0.13 | (−0.40; 0.13) | 183 | 0.12 | (0.14; 0.37) | |
| d’ number 3-back | 400–999 | 86 | Ref. | 178 | Ref. | 132 | Ref. | |||
| <400 | 367 | 0.15 | (−0.09; 0.39) | 378 | 0.00 | (−0.24; 0.24) | 358 | −0.01 | (−0.21; 0.20) | |
| ≥1000 | 220 | −0.03 | (−0.27; 0.22) | 117 | −0.15 | (−0.42; 0.11) | 183 | −0.19 | (−0.41; 0.03) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Compañ-Gabucio, L.M.; Torres-Collado, L.; Garcia-de la Hera, M.; Fernández-Somoano, A.; Tardón, A.; Julvez, J.; Sunyer, J.; Rebagliato, M.; Murcia, M.; Ibarluzea, J.; et al. Association between the Use of Folic Acid Supplements during Pregnancy and Children’s Cognitive Function at 7–9 Years of Age in the INMA Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 12123. https://doi.org/10.3390/ijerph191912123
Compañ-Gabucio LM, Torres-Collado L, Garcia-de la Hera M, Fernández-Somoano A, Tardón A, Julvez J, Sunyer J, Rebagliato M, Murcia M, Ibarluzea J, et al. Association between the Use of Folic Acid Supplements during Pregnancy and Children’s Cognitive Function at 7–9 Years of Age in the INMA Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12123. https://doi.org/10.3390/ijerph191912123
Chicago/Turabian StyleCompañ-Gabucio, Laura María, Laura Torres-Collado, Manuela Garcia-de la Hera, Ana Fernández-Somoano, Adonina Tardón, Jordi Julvez, Jordi Sunyer, Marisa Rebagliato, Mario Murcia, Jesús Ibarluzea, and et al. 2022. "Association between the Use of Folic Acid Supplements during Pregnancy and Children’s Cognitive Function at 7–9 Years of Age in the INMA Cohort Study" International Journal of Environmental Research and Public Health 19, no. 19: 12123. https://doi.org/10.3390/ijerph191912123
APA StyleCompañ-Gabucio, L. M., Torres-Collado, L., Garcia-de la Hera, M., Fernández-Somoano, A., Tardón, A., Julvez, J., Sunyer, J., Rebagliato, M., Murcia, M., Ibarluzea, J., Santa-Marina, L., & Vioque, J. (2022). Association between the Use of Folic Acid Supplements during Pregnancy and Children’s Cognitive Function at 7–9 Years of Age in the INMA Cohort Study. International Journal of Environmental Research and Public Health, 19(19), 12123. https://doi.org/10.3390/ijerph191912123