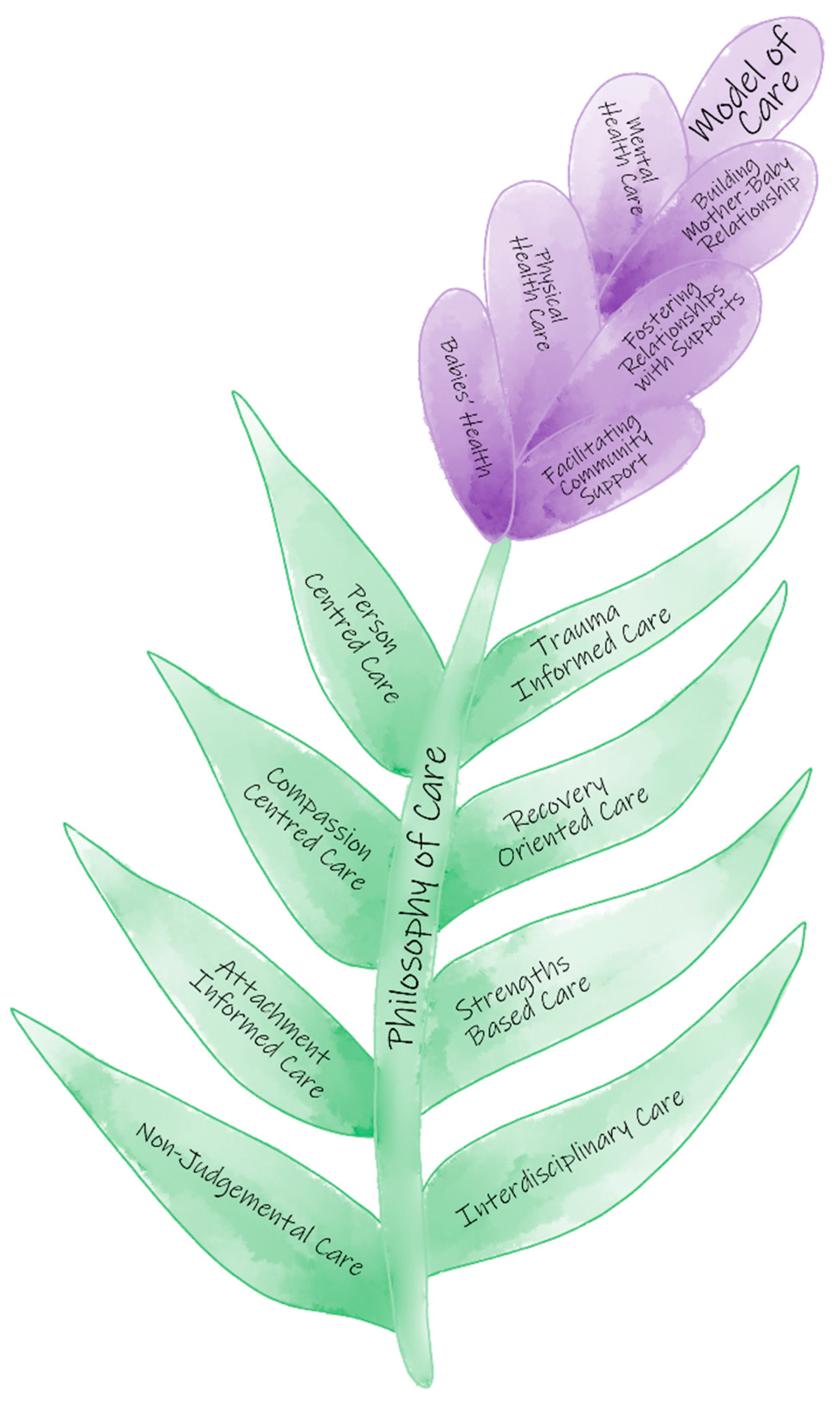
3.1. Lavender Model of Care
The Lavender Model of Care is a six-dimensional model based on participants’ views of their services, responsibilities, and experiences of working at the mother-baby unit (MBU), including: mental health care, physical health care, looking after baby, mother-baby relationship, fostering relationships, and community support.
3.1.1. Mental Health Care
Providing mental health care to patients was identified to be the primary goal of admission at the MBU: “the key admission goals for mums would be to improve their mental health” (Lauren, Community Registrar).
Mental health care commenced with a comprehensive perinatal mental health assessment which included exploration of a consumer’s trauma history, including experiences during childhood and obstetric history. Clinicians sought to understand: “…what their childhood was like, the experiences they had, and things they’d like to change for their babies” (Quella, Psychologist).
Kate (Psychiatrist) further suggested that assessing for psychosocial risk factors was important to consider during assessment. “It is important for MBU professionals to be able to sort of have the conversation with women about the domestic and family violence, and to have the skills to identify it and ask about it.”
Having a thorough knowledge of perinatal mental health disorders, their underlying causes, associated symptoms, and presentation were identified to be essential attributes for working in an MBU: “…to work at a mother-baby unit, it is necessary to have the knowledge of what are the common mental health conditions that can happen. So having the knowledge base of what are the features of depression, antenatal postnatal depression, all the anxiety disorders. How to identify postpartum psychosis, bipolar disorder, and schizophrenia” (Kate, Psychiatrist).
“If they (healthcare professionals) understand mum and her diagnosis well, then it’s easy to be able to give her the best care that you can because you are aware of what borderline is, how they present; or the presentations of schizophrenia, how they present; or how a postnatal depression looks like” (Amy, Clinical Nurse).
Understanding the impact of a mother’s mental health on her relationship and interactions with her baby was also important, and indicated the level of acuity of her mental illness. “Each person’s intervention is different because the situation is different. For example, we had a lady who had OCD traits, she was very cautious and apprehensive initially because of some compulsion that she felt during baby’s bath time. So, we provided her support and assistance with bathing her baby, just so she doesn’t feel alone and compelled to complete” (Amy, Nurse). Amy furthered “Somebody comes in unwell, that they are feeling that they want to adopt their babies out because they feel that they are not coping because they are unwell. And to see that person even three weeks later to be shocked by their own thoughts, that they even thought that.”
Participants further highlighted that MBU patients may present in times of crisis, so being able to assess for capacity and manage emotional dysregulation was important. “A good understanding of mental health is critical, and the capacity factor in understanding that within mental health acute crisis situations, there is a specific time when our patients will actually have the capacity and the ability to have insight into addressing their needs, so being quite sensitive to when would be appropriate to be addressing specifically identified needs, identified through the psychosocial screening process” (Hanna, Social Worker). “If a woman with a personality disorder experiences emotional dysregulation, we will have one to one intervention with the woman and develop a management plan specific to her” (Tanya, Nurse Team Leader).
Given that a range of individual and group interventions (e.g., sensory modulation, psychological strategies) were offered to patients, having proficiency in executing diverse interventions was deemed to be critical. “We do a lot of sensory work as we get a lot of postnatal depression, anxiety, and personality disorder cases. And sensory modulation is amazing for that population” (Natasha, OT).
“As a psychologist we have to be well versed in a number of interventions such as ACT [Acceptance and Commitment Therapy], CBT [Cognitive Behavioral Therapy], and DBT [Dialectical Behavioral Therapy] and even the relationship like Gottman work is a necessity… We do exposure response prevention for OCD [Obsessive Compulsive Disorder] patients, help with some depression support and anxiety support … to do with cognition diffusion. We do behavioral activation stuff minimizing self-harm or providing safer alternatives. Also do kind of red zone distress and tolerance stuff…Having good understanding of trauma and trauma interventions is important to work at a mother-baby unit. Groups that we run are for managing thoughts, mindfulness, diffusion of thoughts, mindful eating, emotional regulation, distress tolerance” (Quella, Psychologist).
From a nursing perspective, a range of emotional, practical and recreational interventions were conducted to improve mental health. “We do art therapies that they show interest in or something we got equipment for, like we do pampering sessions. Take them for a walk. Sit in the courtyard with them, mainly listening to their concerns and showing them that their feelings are validated” (Amy, Nurse). “In groups, we target advocacy for patients especially those who are under the Act [Mental Health Act 2016], like helping people understand their rights and services that we can provide. We do crisis counselling, grounding strategies or mindfulness strategies. I suppose assessing if people need that sensory support, like if they have done sensory toolkit with OT” (Erika, Nurse).
Staff reported that embedding interventions that other health professionals had recommended, and using both pharmacological and psychosocial interventions were important. “Our main focus becomes like a psychotropic management but there are other non-psychotropic interventions that we use in terms of monitoring or supporting patients. For example, sometimes I tell patients not to use medication for anxiety but to use other non-pharmacological therapy like use a fidget when distressed” (Josh, Pharmacist).
“In order to prepare consumers [patients] to feel comfortable with recommendations, we need to involve a lot of psychoeducation and sometimes do a brief CBT. As well as some mindfulness… and sometimes recommend medications too” (Maya, Community psychiatric registrar).
3.1.2. Physical Health Care
Assessment and treatment of patients’ physical needs was reported to be an important aspect as “physical health is often a big issue with them” (Lauren, Community Nurse). The physiotherapists, Osha and Penny, both affirmed that they assessed post-birth issues related to pelvic floor, bowel and bladder difficulties, and exercise engagement, as well as pain that may affect their mental health.
“We normally go over the pregnancy and how that might have impacted the patient, we focus on their return to exercises, the importance of exercise for their mental and physical health and their pelvic floor…I would normally do a detailed physical assessment on everybody, so check their bladder and bowel, their delivery, their exercise history, their musculoskeletal history” (Osha, Physiotherapist).
“There is a lot of pain, there is a lot of chronic pain, vaginal, incontinence itself, debilitating, there is a lot of emotion that goes with that, there is also a lot of pain that goes hand in hand often with mental health” (Penny, Physiotherapist).
Physiotherapists provided a range of interventions based on the consumer’s interest and stage of recovery to target these physical health issues and promote positive mental health recovery, such as through walking, mother-baby exercise, pilates exercise, psychoeducation and starting a morning routine with exercises.
“We get them back into things they used to enjoy as…they just lock themselves at home and don’t go out, so even though a walk seems very simple, that is very beneficial. Obviously, there is a huge benefit of getting them out and exercising on their mood and so we try to do it every day and try to get them into that pattern of starting the day and waking up, or ending the day. We do a healthy lifestyle group with the dietitian. Regarding return to exercise, the importance of exercise for their mental and physical health, and their pelvic floor.” (Osha, Physiotherapist).
Dietitians focused on supporting the dietary aspects of recovery and providing management of underlying medical comorbidities, such as eating disorders, diabetes, or coeliac disease. “I do dietary assessment which involves looking at nutritional profiles of mother…Depending on the stage of recovery, we look into eating disorders and look into medical complication or food allergies. And we also do nutrition restoration, so if there’s any undernutrition, we do dietary planning” (Finn, Dietitian). Dietitians worked in collaboration with the OT to conduct cooking groups; where the OT will focus on the skills of cooking (e.g., peeling, safety, budgeting) and the dietitian will focus on the nutritional aspects.
Sleep support was also provided to promote favorable mental health. “If needed, we provide protected sleep for the first few days. If they come in and they’re really fatigued and busted, we stand beside them and support them” (Diane, Registered Nurse). Post-caesarean recommendations in line with obstetric direction were also reinforced by the nursing staff, such as “not able to lift baby” or “use a hospital bed” (Lauren, Community Nurse) as mothers may be admitted within the first six weeks post-birth.
3.1.3. Babies’ Care
Participants highlighted that caring for babies was a central element of care as participants “don’t just switch off from babies” (Erika, Nurse). Given the link between poor maternal mental health and difficulties with child health (e.g., sleeping, settling, feeding), nursing staff focused on providing support with these child health issues. “A lot of babies have had reflux and colic, a reason, perhaps, that their babies being so unsettled, and that’s contributed to their mental health decline” (Victoria, Registered Nurse).
“We need an awareness around child health issues because you know often, that can be a precipitating factor in a woman’s current mental health presentation, and so it’s important that we as nurses are able to… offer that advice and guidance. Obviously making sure that it’s evidence based” (Tanya, Nurse Unit Manager).
Interventions related to sleep and settling, such as education around sleep cycles, responsive settling, understanding baby cues, settling strategies and following the baby’s lead, were important aspects of babies’ care. To ensure the safety of the baby when sleeping, co-sleeping is prohibited on the unit. “One agreement that we recently created was the safe sleep agreement regarding mothers and babies not co-sleeping together. We don’t allow that because of sudden infant death syndrome, mothers being medicated and highly sedated, and as mothers may have thoughts of harm towards baby” (Samantha, Research and Service Development Coordinator).
Both allied health and nursing staff highlighted the importance of feeding. “First and foremost, assessment is safety, assessing if baby is getting fed properly and regularly” (Diane, Nurse).
“Ninety percent of child health problems are dietary, often its weaning solids or feeding difficulties” (Jenny, Child Health Nurse). They described the need for educating mothers on breastfeeding, particularly surrounding medication intake, bottle-feeding and introduction of solids. Mothers often seek guidance on when to breastfeed after taking medications. “Mums are guided for things like medication and their interactions with breastfeeding. We have to assess how bubs (babies) are going developmentally in regard to feeding… breastfeeding, formula feeding or introduction to solids” (Finn, Dietitian).
Nursing staff also taught mother-crafting skills to those who lacked confidence. “Some of them have never had anything to do with babies, so the basics, like breastfeeding, sterilizing bottles, interacting with their babies, even baby cares like giving the baby a bath, some of them don’t feel confident with doing that” (Victoria, Nurse). The OT (Natasha) also explained that assessing the safety and quality of activities of daily living, that mother and baby participate in, was an important part of her role. “We do functional task assessment, we go into community with babies, look at, you know, parent’s occupations in the community, public transport, shopping, cooking, or that kind of support”.
As most staff were adult mental health staff, responding to baby physical deterioration and escalating appropriately was also highlighted. “Other core competencies include knowing how to do resuscitation of babies…and to be aware of deterioration and wellbeing in babies, and knowledge of who to contact in such situations” (Kate, Psychiatrist).
Staff identified that assessment of infant development and providing strategies to mothers to promote favorable development, such as through play and baby massage, were crucial interventions. “We look into normal baby development: their physical, emotional, social, language development” (Kate, Psychiatrist).
“My job is to look at developmental assessments. So, I’m concerned about baby’s behavior. I do Ages and Stages, and look into their social and emotional development” (Jenny, Child Health Nurse). Physiotherapists and OTs also described focusing on developmental assessment, play ideas, and tummy time.
Protecting children was reported to be a critical aspect. “We follow Queensland Health guidelines on liaising with Child Safety as we have the sanctuary obligation as mandatory reporting of potential harm to infants” (Tanya, Nurse Unit Manager). Nursing staff played a key role in assessing mother-baby interactions: “With assessments, we realize if mum is being unsafe with the baby, then the Child Safety process is followed” (Diane, Nurse). As the social worker, Hannah highlighted that her role was to educate mothers involved with Child Safety around processes and interventions. “If the infant goes into Child Safety, we arrange conversations with those mothers around the concerns and help the mothers understand the process of Child Safety so they know the focus is of them being reunified and so empowering and advocating for the mum, to basically effect the changes that Child Safety are requesting in order for them to be reunited”.
3.1.4. Building Mother-Baby Relationship
Developing the mother-baby relationship was found to be an important dimension of care. Foundational in their clinical practice was that staff focused on the relationship between the dyad, conceptualizing the mother and baby to be one unit. “There is a lot more at stake in terms of working with two within the one... right at the core, is trying to figure out how they work together. They face difficulties getting to know each other, so we need to work together and help them develop a relationship [with their baby], so we need to nurture that” (Georgia, Dietitian).
Many mothers had difficulty forming loving and warm attachments to their baby due to their mental illness and previous trauma. “Mothers come in with reporting no attachment or very little attachment or highly avoidant of their baby, or express intrusive harm, thoughts and thinking that, well in the words of a patient, that they’re monsters…Their presentation gets in the way of attachment or bonding or normalizing to motherhood, thus having a good understanding and skills to deal with how trauma impacts attachment is important to work at an MBU” (Quella, Psychologist).
“A lot of them [mothers] expressed that they don’t feel anything when they look at their babies, maybe they love their babies, but they don’t feel it…I find it challenging when mums perhaps put themselves first before their babies to the point that baby will be hungry, but they will see their needs first” (Victoria, Registered Nurse).
The multidisciplinary team at the Unit strived to improve the mother-baby relationship: “Sometimes they stay on the unit longer than they might on an acute unit because we’re working on the relationship between Mums and Bubs” (Erika, Clinical Nurse). Quella (Psychologist) stated that, “Mothers are really anxious. At the start, they don’t know how to care for babies, they come in low in confidence. So, we work on improving attachment, developing a loving bond, and closeness between them”.
Nursing staff utilized a range of mother-baby oriented interventions to build the mother-baby relationship, such as: role modelling and coaching of mothercraft skills; play time; providing the voice of the baby to the mothers; encouraging attachment building exercises (e.g., art therapy); and helping mothers understand baby cues during daily activities. “We do role modelling, like settling the bub or feeding or like engaging with babies. We do art therapy where mothers make baby footprints, for example” (Erika, Nurse).
Similarly, allied health professionals employed a range of strategies to help foster maternal-infant attachment, such as “group sessions on attachment and bonding, so touching on Circle of Security concepts” (Hanna, Social Worker), and providing “psychological strategies and tools to build relationship with their babies” (Quella, Psychologist). The Physiotherapist (Penny) encouraged mothers to engage in exercises with their baby as a way to develop a warm attachment.
The OT (Natasha) shared that, as mothers are easily overwhelmed and bothered by things that they can see, hear and touch, she used sensory modulation approaches to help mothers understand their sensory preferences and, in turn, bond with their baby: “The Sensory Profile that I see most in Lavender, is mothers who have sensory sensitivity and particularly to auditory input, visual input, and sometimes touch as well. So, mothers then struggle to connect with babies as the sensory input provided by a baby and their activities is quite overwhelming. Just think about the auditory input of babies crying and the visual input when playing with bright and colorful toys. But by understanding their Sensory Profile, this helps them understand themselves better and then they interact better.”
3.1.5. Fostering Relationships with Supports
Fostering social support from their partners, family, and friends was a pivotal dimension of care, as “we look into the important role that family plays” (Diane, Registered Nurse). “Because mother and infant dyads don’t exist in isolation, they are a part of a much bigger whole. Of course, that whole is those key support people around them, whether that be a partner or family or friend or community” (Hanna, Social Worker).
Family members and other social supports were engaged throughout “admission and care planning, discharge planning, to ensure a holistic and realistic care plan” (Hanna, Social worker). They were also supported with education and resources. “We speak about family members from the very beginning, so from pre-admission we start gathering all the information about family members or supportive people around the woman, and then incorporate them in treatment and strengthen their relationships…We also include family members in, or create, discharge meetings as well; whether based on site or on the phone, we provide them with psychoeducation, resources or like websites” (Tanya, Nurse Unit Manager).
Families and partners were also involved in therapy approaches to support the implementation and awareness of strategies: “We do discuss in meetings the component of why she’s finding things difficult, it is probably because of the way that she processes the sensory information or because of their [partner’s] own sensory processing. It’s just very powerful when they understand this about themselves. It is important for partners to look from the other person’s point of view as to why they are struggling or what are the challenges; this helps them in understanding each other. So, it’s not always about Dad doing everything to make sure the environment is clean and quiet, but it’s also mum figuring out what dad’s needs are as well” (Natasha, OT). Lavender utilized counselling as an important strategy to foster patients’ relationship with their partners. “Mothers are counselled about father’s situation and journey to parenthood; how fathers were impacted by their wives’ mental health condition, how she should communicate about her mental health with dad’s and think about broader family structure” (Kate, Psychiatrist).
“We do modelling with mum and dad of what it looks like to play with their child, engage with their child and build that social emotional connection when they are eating” (Jenny, Child Health Nurse). Recreational family activities are encouraged to foster family relationships: “On weekends where there are mums and dads, they play with their babies and chat with each other. We are hoping to arrange family barbeques” (Victoria, Nurse).
3.1.6. Facilitating Community Support
Facilitating community support was reported to be an important dimension of care to help “set them up for their whole life” (Lauren, Nurse). This included supporting mothers and linkages with community services for transition back to home post-discharge. “We help support the transition to community services or we keep supporting that woman through consultation and liaison, and provide umbrella support for up to three months post-discharge” (Tanya, Nurse Unit Manager).
“I do discharge planning and follow-up in the community to make sure they’re engaged post-discharge as well. I do consultation and liaison with community services state-wide. Can be, for example, writing a letter and advocating for childcare as it is free for 10 weeks post-discharge, or other individual programs for mothers and babies care as they might need physio sometimes” (Isabel, Social Worker).
As a range of needs are identified during admission that cannot be addressed in the limited admission, and require ongoing support, community services are referred to. “Some things can be addressed during the acute admission phase; other things are identified and then recommendations are made for post discharge care, to then facilitate and support the woman or partners or significant others to link in with relevant services down the track” (Hanna, Social worker).
As a Statewide service, telehealth services were utilized as an important tool to connect patients with different services and improve access. “We do seven-day follow-up and also connect them to other services, sometimes we do face-to-face or do telehealth, especially in far areas of the state” (Isabel, Social Worker).
As mothers admitted had complex needs, patients required support from a range of different services (e.g., allied health professionals, non-governmental organizations, mother-infant therapy, domestic violence services, Child Safety, and refugee/migrant women’s services) and were supported to link up with these services.
“We have to link them with a community dietitian if they have an eating disorder. But to find a dietitian, they [the mothers] get triaged, but the dieticians at a public service isn’t always available state-wide, so we have to utilize other avenues such as contacting health precincts in certain catchment areas. We have to make sure that there will be dietitians available in their local community that might be linked with a certain GP” (Finn, Dietitian).
“Sometimes we need private practitioners such as mother-infant therapists, governmental day programs such as Together in Mind and non-government organizations who run peer support programs and Circle of Security. Sometimes other psychological programs, domestic violence prevention services or women’s legal services, a refugee or migrant women’s resource centers, and trauma services need to be arranged” (Isabel, Social Worker).
“We help patients in identifying the community support around them, improving their access to community support, and how to navigate legal systems, in relation to family law, mediation etc., looking at Child Safety and facilitating and liaising with them” (Hana, Social Worker).
Community support services and relevant external stakeholders were also reported to be included in multidisciplinary care reviews and other meetings, and invited to take part in collaborative care planning. “Most of the time we do care planning jointly with other service case managers when we handover patients. We invite them for care reviews and ask them what their role would be post-discharge and we also keep them in the loop post-discharge” (Isabel, Social Worker).
3.2. Philosophy of Care
The Philosophy of Care Principles were underpinned by clinical practice and their attitudes towards patients and families. These included: Person-centered care, Trauma-informed care, Compassion-centered care, Recovery-oriented care, Attachment- and family-focused care, Strengths-based care, Non-judgmental care, and Interdisciplinary care.
3.2.1. Person-Centered Care
The treatment and therapeutic programs were guided by patients’ preferences and goals: “…it’s about what client wants…I look at the person and tailoring what it is I have to say to the person’s personality and style rather than being prescriptive” (Jenny, Child Health Nurse).
“Some mothers are really active in their adult life, they want to go to gym, in that case I take them to gym and design gym program for them” (Penny, Physiotherapist).
“We take in consideration consumers’ [patients’] goals and practices and our job is to make them achieve those goals” (Tanya, Nurse Unit Manager).
3.2.2. Trauma-Informed Care
Understanding the mother’s experience with trauma, such as during childhood, recent pregnancy-related difficulties, and other stressors, was highlighted as vital. “We look into the trauma history from the past. It can be very sensitive and that can be very triggering to people, how their childhood was like, if they were happy with their childhood, and whether there were things they’d like to change because it often impacts on how they perceive their goals with parenting…What’s happened in the past with them, how has their pregnancy experience been like for you, and you break that down into trimesters first, second, and 3rd trimester. Did they have any miscarriage, termination, stillbirths?” (Lauren, Nurse).
Recognizing the signs of trauma in the mother’s behaviors and how they interact with their baby was also viewed as significant. “You need to understand the mother’s background and her previous attachment trauma as it helps explain her behavior. For example, a mother may push someone away because they’ve been rejected a lot in the past and they want to protect themselves” (Samantha, Research and Service Development Officer).
Additionally, adopting interventions to address trauma was perceived to be foundational. “Having a good understanding of trauma, and trauma interventions, such as avoiding re-traumatization, is important to work at MBU. And understanding those trauma responses, such as dissociation and avoidance, are important” (Quella, Psychologist).
3.2.3. Compassion-Centered Care
A key philosophy of care was to show compassion and empathy towards every patient, particularly as the patients had been through difficult situations, and to support optimal outcomes in the therapeutic relationship. “With mental health patients we have to be kind, compassionate, and understanding” (Amy, Nurse).
“When you hear their background, you become more compassionate and think, wow, that must be really hard” (Osha, Physiotherapy).
“I try to be very sensitive and always kind because in my 30 years’ experience, I have learned kindness, compassion, and rapport building makes a lot of differences in other people’s lives” (Jenny, Child Health Nurse).
3.2.4. Recovery-Oriented Care
Clinical care was recovery-oriented, as staff held hope for the patients in improving their mental state, maternal-infant attachment, and overall functioning. Staff voiced that they played a role in the recovery process and were heartened by the difference they could observe from start to end of admission. “We become part of that recovery-based journey and you see big differences in patients. They come in depressed and leave functioning and continuing on the road of recovery” (Claire, Nurse).
Staff also noted the positive change in the relationship between the mother and her baby over the course of the admission. “It’s amazing when you see new mums coming in, struggling with having no feelings of love, or no feelings of that real mother-child bond, and then seeing that build in confidence before they leave. They get so organized and recover so much when you look at them at discharge” (Diane, Nurse).
To support recovery, staff focused on the transition back into the community after discharge. “From the physio’s perspective, I focus on getting them back into things they used to enjoy, and things mums want to do post-discharge” (Osha, Physiotherapist).
3.2.5. Attachment-Informed Care
A foundational principle was to “think about mother and baby together, and keeping in mind who is around them to provide support” (Quella, Psychologist), such as the partner, grandmother of the baby, friends and other key support people. “Thinking about the dyad, that mother-infant relationship, and in the context of the family, is imperative to the work we do within a mother-baby unit” (Tania, Nurse Unit Manager). Consideration of the mother, baby and the dyad together was identified as crucial, with staff reporting: “I guess the challenge or difference is that we are working with mother-baby dyad and we have to be mindful of that, we have to consider them both while designing appropriate interventions” (Georgia, Dietitian).
“Within Lavender, I think it is that mother-baby dyad that is unique, so you have to consider both together” (Osha, Physio).
Strengthening the attachment relationship between mother and family was highlighted by Hanna (Social worker) when she explained, “We look into patient’s attachment history and how it is impacting on their current mental health and relationship with their infant and partners, and how it impacts their current health and what interventions could basically improve and strengthen their attachment.”
Staff were also upskilled in working with families through recognized programs: “What we’ve done is, with particularly the nursing staff, they’re all gradually going through, attending the Family Partnership Training through Child Health, and which they’ve said is very beneficial” (Tanya, Nurse Unit Manager).
3.2.6. Non-Judgmental Care
Being non-judgmental was highlighted to be a core attribute for clinicians when interacting with mothers struggling with parenting and who had difficult backgrounds that affected their presentation. “It requires us to be non-judgmental, especially in this unit. It’s the hardest unit because there are babies involved and you do feel protectiveness towards them…They come from all different backgrounds, all different childhoods, different mothers, crafting abilities and you have to be non-judgmental in meeting them, treating them and caring for them” (Claire, Nurse). Another nurse (Victoria) also acknowledged that “definitely, being non-judgmental is a big thing because we see mums from all walks of life”. Clinicians also responded to mothers during individual and group therapy sessions in a non-judgmental manner. “In group settings we discuss a series of topics of interests and encourage them to ask questions and give them answers in a non-judgmental way” (Josh, Pharmacist).
3.2.7. Strengths-Based Care
The Lavender Model of Care was found to be strength-based, where patients’ strengths were harnessed to facilitate recovery. “We look at their strengths and what they do well and try to exploit that towards their recovery rather than focusing on their deficits” (Diane, Nurse).
Staff also felt it was important to support women in their mothering role: the “goal is to empower mums to see their potential as a mother, as a lot of women come in with a lack self-esteem and confidence, so our job is to make them stronger” (Yvette, Nurse).
Women were empowered to manage their mental illness to support their recovery. “How do I live with mental illness and how can I parent with mental illness and so to give them that empowerment, to give them that knowledge and to watch them grow from their mental condition” (Claire, Nurse).
3.2.8. Interdisciplinary Care
The model of care was revealed to be underpinned by an interdisciplinary approach, where professionals from different backgrounds brought their unique knowledge and skills together towards the single goal of a patient’s recovery. Adopting an interdisciplinary way of working was also perceived to be more effective than working in a silo.
“At Lavender, we follow a multidisciplinary team approach, which is really positive. There is lots of sharing, assessments, discussions or working together with the other members of the MDT. Say, for example, combining with the physio for a healthy lifestyle type approach or combining with the OT for functional assessments and community engagement or with social worker, child health nurse, pharmacist, psychiatrist…What we could do together as a team is lot more than what we could do as an individual” (Georgia, Dietitian).
“We basically have a service therapeutic model where all the staff skill set adds on and works much efficiently than what an individual professional can offer” (Hanna, Social Worker).
In particular, the allied health team collaborated closely together. “We have got the whole allied team that works together as a unit across different facets of patient’s recovery” (Claire, Nurse).
A key forum in which staff communicated with each other regarding the care plan, were the community and inpatient case reviews. “Community case reviews happens twice a week, that’s the intake multidisciplinary meeting, attended by consultants, team leaders for the social worker, me, nursing team leader. We discuss case review and intake assessments” (Lauren, Community Nurse).
Regarding inpatient case reviews: “we do case review as well, so you get discussion with the multidisciplinary team. So, after that meeting is finished, I would generally go down and do a mutual help meeting, so that also runs in conjunction with our other Allied Health members” (Penny, Physiotherapist).




{kind=link}