
Gestational and Neonatal Outcomes in Cities in the Largest Coal Mining Region in Brazil



Abstract
:1. Introduction
2. Materials and Methods
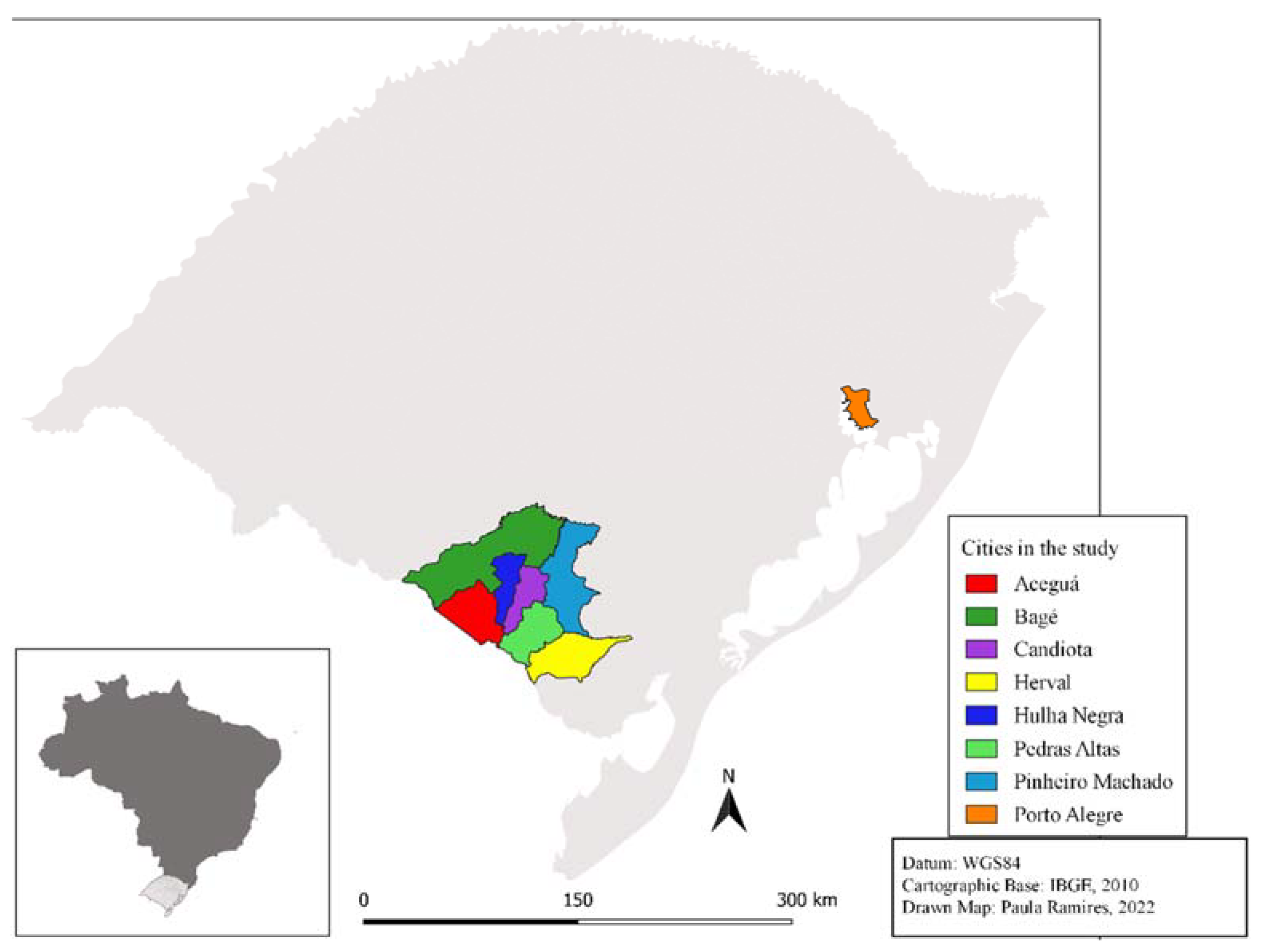
2.1. Study Area
2.2. Analysis of Air Pollutants
2.3. Data Collection
2.4. Variables
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- EPA Agency Environmental Protection. National Emissions Inventory. 2016. Available online: https://www.epa.gov/ (accessed on 15 June 2022).
- Da Silva Júnior, F.M.R.; Tavella, R.A.; Fernandes, C.L.F.; Soares, M.C.F.; de Almeida, K.A.; Garcia, E.M.; da Silva Pinto, E.A.; Baisch, A.L.M. Genotoxicity in Brazilian coal miners and its associated factors. Hum. Exp. Toxicol. 2018, 37, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Epstein, M.B.; Bates, M.N.; Arora, N.K.; Balakrishnan, K.; Jack, D.W.; Smith, K.R. Household fuels, low birth weight, and neonatal death in India: The separate impacts of biomass, kerosene, and coal. Int. J. Hyg. Environ. Health 2013, 216, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Ahern, M.; Mullett, M.; MacKay, K.; Hamilton, C. Residence in coal-mining areas and low-birth-weight outcomes. Matern. Child Health J. 2011, 15, 974–979. [Google Scholar] [CrossRef]
- World Coal Association. Energy Poverty and Sustainable Development Policy Statement. 2011. Available online: https://www.worldcoal.org/ (accessed on 9 June 2022).
- Brasil Agência Nacional de Energia Elétrica. Atlas de Energia Elétrica do Brasil, 2nd ed.; ANEEL: Brasília, Brazil, 2002; p. 243. [Google Scholar]
- De Santana, E.R.R.; Sampaio, C.H.; Teixeira, E.C.; Andréani, P.-A.; Benezet, J.-C.; Adamiec, P.; Benhassaine, A.; Schütz, R. Sulfated coal ashes characterization aiming its utilization in cement industry-mineralogical reconstruction of Candiota coal (Brazil). Rev. Bras. Geocienc. 2011, 41, 220–227. [Google Scholar] [CrossRef]
- Ramgrab, G.; Holz, M.; De Ros, L. Principais recursos minerais do Rio Grande do Sul. In Geologia Do Rio Grande Do Sul; CIGO/UFRGS, Ed.; UFRGS: Porto Alegre, Brazil, 2000; pp. 407–440. [Google Scholar]
- Pereira, V.C.; Almeida, J. Relações entre a Atividade Carbonífera e o Rural em Candiota, RS, Brasil: Análises sobre representações sociais em um contexto de dilemas sobre a energia. Rev. Econ. Sociol. Rural. 2015, 53, 127–142. [Google Scholar] [CrossRef]
- Pires, M.; Querol, X. Characterization of Candiota (South Brazil) coal and combustion by-product. Int. J. Coal Geol. 2004, 60, 57–72. [Google Scholar] [CrossRef]
- Da Silva Júnior, F.M.R.; Ramires, P.F.; Dos Santos, M.; Seus, E.R.; Soares, M.C.F.; Muccillo-Baisch, A.L.; Mirlean, N.; Baisch, P.R.M. Distribution of potentially harmful elements in soils around a large coal-fired power plant. Environ. Geochem. Health 2019, 41, 2131–2143. [Google Scholar] [CrossRef]
- Kvitko, K.; Bandinelli, E.; Henriques, J.A.P.; Heuser, V.D.; Rohr, P.; Silva, F.R.; Schneider, N.B.; Fernandes, S.; Ancines, C.; Silva, J. Susceptibility to DNA damage in workers occupationally exposed to pesticides, to tannery chemicals and to coal dust during mining. Genet. Mol. Biol. 2012, 35, 1060–1068. [Google Scholar] [CrossRef]
- Cortes-Ramirez, J.; Naish, S.; Sly, P.D.; Jagals, P. Mortality and morbidity in populations in the vicinity of coal mining: A systematic review. BMC Public Health 2018, 18, 721. [Google Scholar] [CrossRef]
- Melody, S.M.; Ford, J.; Wills, K.; Venn, A.; Johnston, F.H. Maternal exposure to fi ne particulate matter from a coal mine fi re and birth outcomes in Victoria, Australia. Environ. Int. 2019, 127, 233–242. [Google Scholar] [CrossRef]
- Mohorovic, L. First two months of pregnancy—Critical time for preterm delivery and low birthweight caused by adverse effects of coal combustion toxics. Early Hum. Dev. 2004, 80, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Ahern, M.; Hendryx, M.; Conley, J.; Fedorko, E.; Ducatman, A.; Zullig, K.J. The association between mountaintop mining and birth defects among live births in central Appalachia, 1996–2003. Environ. Res. 2011, 111, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Hu, H.; Roth, J.; Kan, H.; Xu, X. Associations between residential proximity to power plants and adverse birth outcomes. Am. J. Epidemiol. 2015, 182, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Rückerl, R.; Schneider, A.; Breitner, S.; Cyrys, J.; Peters, A. Health effects of particulate air pollution: A review of epidemiological evidence. Inhal. Toxicol. 2011, 23, 555–592. [Google Scholar] [CrossRef]
- Xu, Y.; Huang, H.; Zeng, Q.; Yu, C.; Yao, M.; Hong, F.; Luo, P.; Pan, X.; Zhang, A. The effect of elemental content on the risk of dental fluorosis and the exposure of the environment and population to fluoride produced by coal-burning. Environ. Toxicol. Pharmacol. 2017, 56, 329–339. [Google Scholar] [CrossRef]
- Trasande, L.; Liu, Y. Reducing the staggering costs of environmental disease in children, estimated at $76.6 billion in 2008. Health Aff. 2011, 30, 863–870. [Google Scholar] [CrossRef]
- Fernández-Navarro, P.; García-Pérez, J.; Ramis, R.; Boldo, E.; López-Abente, G. Science of the Total Environment Proximity to mining industry and cancer mortality. Sci. Total Environ. 2012, 435–436, 66–73. [Google Scholar] [CrossRef]
- Júnior, F.M.R.D.S.; Honscha, L.C.; Brum, R.D.L.; Ramires, P.F.; Tavella, R.A.; Fernandes, C.L.F.; Pentado, J.O.; Bonifácio, A.D.S.; Volcão, L.M.; Dos Santos, M.; et al. Air quality in cities of the extreme south of Brazil. Ecotoxicol. Environ. Contam. 2020, 15, 61–67. [Google Scholar] [CrossRef]
- Dos Santos, M.; Ramires, P.F.; Gironés, M.C.R.; Armendáriz, M.D.C.R.; Montelongo, S.P.; Muccillo-Baisch, A.L.; da Silva Junior, F.M.R. Multiple exposure pathways and health risk assessment of selenium for children in a coal mining area. Environ. Sci. Pollut. Res. 2021, 28, 13562–13569. [Google Scholar] [CrossRef]
- Müller, L.; Ramires, P.F.; dos Santos, M.; Coronas, M.V.; Lima, J.V.; Dias, D.; Muccillo-Baisch, A.L.; Baisch, P.R.M.; da Silva Júnior, F.M.R. Human health risk assessment of arsenic in a region influenced by a large coal-fired power plant. Int. J. Environ. Sci. Technol. 2022, 19, 281–288. [Google Scholar] [CrossRef]
- Bonifácio, A.S.; de Lima Brum, R.; Tavella, R.A.; Ramires, P.F.; Lessa, I.M.; Dos Santos, M.; da Silva Júnior, F.M.R. Human health risk assessment of metals and anions in surface water from a mineral coal region in Brazil. Environ. Monit. Assess. 2021, 193, 567. [Google Scholar] [CrossRef] [PubMed]
- Ramires, P.F.; Dos Santos, M.; Paz-Montelongo, S.; Rubio-Armendáriz, C.; Adamatti, D.; Fiasconaro, M.L.; da Silva Júnior, F.M.R. Multiple exposure pathways and health risk assessment of potentially harmful elements for children and adults living in a coal region in Brazil. Environ. Geochem. Health 2022. [Google Scholar] [CrossRef]
- Pinto, E.A.D.S.; Garcia, E.M.; De Almeida, K.A.; Fernandes, C.F.L.; Tavella, R.A.; Soares, M.C.F.; Baisch, P.R.M.; Muccillo-Baisch, A.L.; da Silva Júnior, F.M.R. Genotoxicity in adult residents in mineral coal region—A cross-sectional study. Environ. Sci. Pollut. Res. 2017, 24, 16806–16814. [Google Scholar] [CrossRef]
- Dos Santos, M.; Soares, M.C.F.; Baisch, P.R.M.; Baisch, A.L.M.; da Silva Júnior, F.M.R. Biomonitoring of trace elements in urine samples of children from a coal-mining region. Chemosphere 2018, 197, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Bigliardi, A.P.; Fernandes, C.L.F.; Pinto, E.A.; Dos Santos, M.; Garcia, E.M.; Baisch, P.R.M.; Soares, M.C.F.; Muccillo-Baisch, A.L.; da Silva Júnior, F.M.R. Blood markers among residents from a coal mining area. Environ. Sci. Pollut. Res. 2021, 28, 1409–1416. [Google Scholar] [CrossRef] [PubMed]
- Bigliardi, A.P.; Dos Santos, M.; Fernandes, C.L.F.; Garcia, E.M.; Dos Santos, M.E.T.; Jones, M.H.; Soares, M.C.F.; Baisch, A.L.M.; da Silva Júnior, F.M.R. Lung function among residents from the largest coal region in Brazil. Environ. Sci. Pollut. Res. 2022, 29, 46803–46812. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, M.; da Silva Júnior, F.M.R.; Zurdo, D.V.; Baisch, P.R.M.; Muccillo-Baisch, A.L.; Madrid, Y. Selenium and mercury concentration in drinking water and food samples from a coal mining area in Brazil. Environ. Sci. Pollut. Res. 2019, 26, 15510–15517. [Google Scholar] [CrossRef] [PubMed]
- Honscha, L.C.; Penteado, J.O.; de Sá Gama, V.; da Silva Bonifácio, A.; Aikawa, P.; Dos Santos, M.; Baisch, P.R.M.; Muccillo-Baisch, A.L.; da Silva Júnior, F.M.R. Health impact assessment of air pollution in an area of the largest coal mine in Brazil. Environ. Sci. Pollut. Res. 2021, 29, 14176–14184. [Google Scholar] [CrossRef]
- Honscha, L.C.; de Moura, R.R.; Baisch, P.R.M.; Júnior, F.M.R.D.S. Increasingly distant from Eden—a look at the soils of protected areas using ecotoxicological tests and chemical analysis. Water Air Soil Pollut. 2019, 230, 162. [Google Scholar] [CrossRef]
- Dos Santos, M.; Penteado, J.O.; Baisch, P.R.M.; Soares, B.M.; Muccillo-Baisch, A.L.; da Silva Júnior, F.M.R. Selenium dietary intake, urinary excretion, and toxicity symptoms among children from a coal mining area in Brazil. Environ. Geochem. Health 2021, 43, 65–75. [Google Scholar] [CrossRef]
- Dupont-Soares, M.; Dos Santos, M.; Garcia, E.M.; Soares, M.C.F.; Muccillo-Baisch, A.L.; da Silva Júnior, F.M.R. Maternal, neonatal and socio-economic factors associated with intellectual development among children from a coal mining region in Brazil. Environ. Geochem. Health 2021, 43, 3055–3066. [Google Scholar] [CrossRef] [PubMed]
- Silva-Junior, D.; Rodrigues, F.M.; Oleinski, R.M.; Azevedo, A.E.; Monroe, K.C.; Dos Santos, M.; Da Silveira, T.B.; De Oliveira, A.M.N.; Soares, M.C.F.; Pereira, T.D.S. Vulnerability associated with “symptoms similar to those of mercury poisoning” in communities from Xingu River, Amazon basin. Environ. Geochem. Health 2018, 40, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Amster, E.; Levy, C.L. Impact of Coal-fired Power Plant Emissions on Children’s Health: A Systematic Review of the Epidemiological Literature. Int. J. Environ. Res. Public Health 2019, 16, 2008. [Google Scholar] [CrossRef] [PubMed]
- Casey, J.A.; Karasek, D.; Ogburn, E.L.; Goin, D.E.; Dang, K.; Braveman, P.A.; Morello-Frosch, R. Retirements of Coal and Oil Power Plants in California: Association With Reduced Preterm Birth Among Populations Nearby. Am. J. Epidemiol. 2018, 187, 1586–1594. [Google Scholar] [CrossRef] [PubMed]
- Diniz, D.; Medeiros, M.; Madeiro, A. Pesquisa Nacional de Aborto 2016. Ciên. Saúde Colet. 2017, 22, 653–660. [Google Scholar] [CrossRef]
- Grippo, A.; Myneni, A.A.; Mu, L. Air pollution exposure during pregnancy and spontaneous abortion and stillbirth. Rev. Environ. Health 2018, 33, 247–264. [Google Scholar] [CrossRef] [PubMed]
- Mohorovic, L.; Petrovic, O.; Haller, H.; Micovic, V. Pregnancy loss and maternal methemoglobin levels: An indirect explanation of the association of environmental toxics and their adverse effects on the mother and the fetus. Int. J. Environ. Res. Public Health 2010, 7, 4203–4212. [Google Scholar] [CrossRef]
- Viellas, E.F.; Augusto, M.; Dias, B.; Viana, J.; Bastos, M.H. Prenatal care in Brazil. Cad. Saúde Pública 2014, 30, 85–100. [Google Scholar] [CrossRef]
- Cesar, J.A.; Mano, P.S.; Carlotto, K.; Gonzalez-Chica, D.A.; Mendoza-sassi, R.A. Público versus privado: Avaliando a assistência à gestação e ao parto no extremo sul do Brasil. Rev. Bras. Saúde Matern. Infant. 2011, 11, 257–263. [Google Scholar] [CrossRef]
- Marmitt, L.P.; Machado, A.K.F.; Cesar, J.A. Recent trends in cesarean section reduction in extreme south of Brazil: A reality only in the public sector? Ciên. Saúde Colet. 2022, 27, 3307–3381. [Google Scholar] [CrossRef]
- Eufrásio, L.S.; Souza, D.E.; Fonsêca, A.M.C.; Viana, E.S.R. Brazilian regional differences and factors associated with the prevalence of cesarean sections. Fisioter. Mov. 2018, 31, e003108. [Google Scholar] [CrossRef]
- Backes, C.H.; Nelin, T.; Gorr, M.W.; Wold, L.E. Early Life Exposure to Air Pollution: How Bad Is It? Toxicol. Lett. 2013, 216, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Luz, G.D.S.; Karam, S.M.; Dumith, S.C. Congenital anomalies in Rio Grande do Sul State: A time series analysis. Rev. Bras. Epidemiol. 2019, 22, e190040. [Google Scholar] [CrossRef] [PubMed]
- Leite, J.C.; Schuler-Faccini, L. Defeitos congenitos em uma regiao de mineracao de carvao. [Congenital defects in a coal mining region]. Rev. Saude Publica 2001, 35, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Wang, J.; Wu, J.; Driskell, L.; Wang, W.; Zhang, T.; Xue, G.; Zheng, X. Spatial analysis of neural tube defects in a rural coal mining area. Int. J. Environ. Health Res. 2010, 20, 439–450. [Google Scholar] [CrossRef]
- Victora, J.D.; Silveira, M.F.; Tonial, C.T.; Victora, C.G.; Barros, F.C.; Horta, B.L.; dos Santos, I.S.; Bassani, D.G.; Garcia, P.C.R.; Scheeren, M.; et al. Prevalence, mortality and risk factors associated with very low birth weight preterm infants: An analysis of 33 years. J. Pediatr. 2020, 96, 327–332. [Google Scholar] [CrossRef]
- do Nascimento, F.P.; de Almeida, M.F.; Gouveia, N. Individual and contextual socioeconomic status as effect modifier in the air pollution-birth outcome association. Sci. Total Environ. 2022, 803, 149790. [Google Scholar] [CrossRef]
- Cassidy-Bushrow, A.E.; Burmeister, C.; Lamerato, L.; Lemke, L.D.; Mathieu, M.; O’Leary, B.F.; Sperone, F.G.; Straughen, J.K.; Reiners, J.J., Jr. Prenatal airshed pollutants and preterm birth in an observational birth cohort study in Detroit, Michigan, USA. Environ. Res. 2020, 189, 109845. [Google Scholar] [CrossRef]
- Liu, Y.; Xu, J.; Chen, D.; Sun, P.; Ma, X. The association between air pollution and preterm birth and low birth weight in Guangdong, China. BMC Public Health 2019, 19, 3. [Google Scholar] [CrossRef]
- Karanth, S.; Vijay, C.; Mol, C.J.S.; Vijaykumar, N.; Devaraj, U.; Balakrishnan, H. Study of Maternal and Perinatal Outcomes in Pregnant Women with Respiratory Complications. J. South Asian Fed. Obstet. Gynecol. 2021, 13, 216–220. [Google Scholar] [CrossRef]
- Brasil [CONAMA] Conselho Nacional do Meio Ambiente. Resolução n° 491 de 19 de Novembro de 2018. Dispõe sobre padrões de qualidade do ar. Brasília: Diário oficial da República Federativa do Brasil. 2018. Available online: https://www.in.gov.br/materia/-/asset_publisher/Kujrw0TZC2Mb/content/id/51058895 (accessed on 20 September 2022).
- WHO-World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide: Executive Summary. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/345334/9789240034433-eng.pdf (accessed on 20 September 2022).
- Pedraza, D.F. Baixo peso ao nascer no Brasil: Revisão sistemática de estudos baseados no sistema de informações sobre nascidos vivos. Rev. Atenção Saúde 2014, 12, 37–50. [Google Scholar] [CrossRef]

{kind=link}
| Candiota Station | Pedras Altas Station | Aceguá Station | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NO | NO2 | SO2 | PM10 | NO | NO2 | SO2 | PM10 | NO | NO2 | SO2 | PM10 | |
| Minimum | 0 | 0.19 | 0.82 | 5.00 | 0.00 | 0.75 | 0.82 | 3.00 | 0.00 | 1.32 | 0.82 | 2.00 |
| 25th Percentile | 2.33 | 4.33 | 5.32 | 18.00 | 1.72 | 3.20 | 7.77 | 11.00 | 1.72 | 3.01 | 9.00 | 15.75 |
| Median | 3.19 | 6.21 | 7.77 | 24.00 | 1.96 | 4.14 | 9.82 | 16.00 | 1.96 | 4.14 | 10.63 | 21.00 |
| 75th Percentile | 4.79 | 9.03 | 12.27 | 32.00 | 2.09 | 5.08 | 11.04 | 22.00 | 2.21 | 5.27 | 12.68 | 27.00 |
| Maximum | 72.53 | 52.88 | 264.62 | 116.0 | 16.45 | 41.96 | 36.40 | 52.00 | 8.96 | 29.54 | 24.54 | 57.00 |
| Mean | 4.19 | 7.66 | 13.46 | 26.71 | 2.01 | 4.33 | 9.80 | 17.49 | 1.99 | 4.56 | 10.63 | 22.09 |
| Std. Deviation | 3.44 | 5.34 | 20.56 | 12.90 | 0.64 | 2.18 | 4.05 | 8.66 | 0.46 | 2.21 | 3.56 | 9.40 |
| n | % | |
|---|---|---|
| Age | ||
| ≤19 years | 373 | 19.1 |
| 20–34 years | 1320 | 67.7 |
| ≥35 years | 257 | 13.2 |
| Skin color declared + | ||
| Caucasian | 1424 | 73.1 |
| Black or mixed | 505 | 25.9 |
| Education level + | ||
| 1 to 3 years | 84 | 4.3 |
| 4 to 7 years | 703 | 36.1 |
| ≥8 years | 1147 | 58.8 |
| Married + | ||
| Not | 1355 | 69.5 |
| Yes | 580 | 29.7 |
| Previous pregnancies + | ||
| Zero | 868 | 44.5 |
| 1 gestation | 544 | 27.9 |
| ≥2 gestations | 533 | 27.3 |
| Previous fetal loss/abortions *+ | ||
| Zero | 791 | 73.1 |
| ≥1 loss | 290 | 26.8 |
| n | % | |
|---|---|---|
| Initiation of prenatal care + | ||
| 1–3 month | 1510 | 77.4 |
| 4–6 month | 300 | 15.4 |
| 7–9 month | 40 | 2.1 |
| Prenatal care + | ||
| Inadequate | 254 | 13.0 |
| Adequate | 1651 | 84.7 |
| Birth type + | ||
| Vaginal | 611 | 31.3 |
| Cesarean | 1337 | 68.6 |
| Gender of the newborn | ||
| Male | 980 | 50.3 |
| Female | 970 | 49.7 |
| Gestational age + | ||
| Preterm | 223 | 11.6 |
| Term | 1684 | 86.4 |
| Post-term | 31 | 1.4 |
| 5th minute Apgar score + | ||
| ≤6 | 21 | 1.1 |
| ≥7 | 1920 | 98.5 |
| Birth weight (g) + | ||
| ≤2499 | 184 | 9.5 |
| 2500–2999 | 433 | 22.2 |
| ≥3000 | 1332 | 68.3 |
| Congenital disorders + | ||
| No | 1902 | 97.5 |
| Yes | 17 | 0.9 |
| Total | Candiota | Aceguá | Bagé | Herval | Hulha Negra | Pedras Altas | Pinheiro Machado | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Gestational age (weeks) | <0.01 | ||||||||
| ≤31 | 30 (1.5) | - | 03 (5.7) | 22 (1.4) | 01 (2.4) | 01 (1.5) | 01 (4.8) | 02 (2.2) | |
| 32–33 | 35 (2.0) | 02 (1.6) | - | 28 (1.8) | 01 (2.4) | 01 (1.5) | 01 (4.8) | 02 (2.2) | |
| 34–36 | 158 (8.1) | 17 (13.3) | 03 (5.7) | 128 (8.3) | 03 (7.3) | 04 (6.2) | - | 03 (3.2) | |
| 37–41 | 1684 (86.4) | 102 (79.7) | 44 (83.0) | 1356 (87.5) | 35 (85.4) | 55 (84.6) | 16 (76.2) | 76 (87.0) | |
| ≥42 | 31 (1.6) | 06 (4.7) | 03 (5.7) | 10 (0.6) | 01 (2.4) | 03 (4.6) | 03 (14.3) | 05 (5.4) | |
| Birth weight (g) | <0.01 | ||||||||
| ≤999 | 09 (0.5) | - | 02 (3.8) | 05 (0.3) | 01 (2.4) | 01 (1.5) | - | - | |
| 1000–1499 | 16 (0.8) | - | - | 14 (0.9) | - | - | 02 (9.5) | - | |
| 1500–2499 | 159 (8.2) | 13 (10.2) | 03 (5.7) | 129 (8.3) | 01 (2.4) | 0,2 (3.1) | 01 (4.8) | 10 (10.8) | |
| 2500–2999 | 433 (22.2) | 31 (24.2) | 09 (17.0) | 350 (22.6) | 08 (19.5) | 08 (12.3) | 04 (19.0) | 23 (24.7) | |
| 3000–3999 | 1215 (62.3) | 80 (62.5) | 31 (58.5) | 958 (61.8) | 30 (73.2) | 49 (75.4) | 12 (57.1) | 55 (59.1) | |
| ≥4000 | 117 (6.0) | 04 (3.1) | 08 (15.1) | 93 (6.0) | 01 (2.4) | 05 (7.7) | 02 (9.5) | 04 (4.3) |
| Unadjusted | p-Value | Adjusted | p-Value | |
|---|---|---|---|---|
| Previous fetal loss/abortions | 0.02 | 0.01 | ||
| Zero | 1.00 | 1.00 | ||
| ≥1 loss | 1.57 (1.09–2.26) | 1.58 (1.10–2.27) | ||
| Prenatal care | <0.01 | <0.01 | ||
| Adequate | 1.00 | 1.00 | ||
| Inadequate | 2.57 (1.93–3.42) | 2.39 (1.62–3.52) | ||
| Birth type | 0.01 | 0.01 | ||
| Vaginal | 1.00 | 1.00 | ||
| Cesarean | 1.52 (1.11–2.08) | 1.87 (1.16–3.02) | ||
| PM10 in the first trimester of pregnancy | 0.99 (0.95–1.04) | 0.77 | 1.31 (1.11–1.55) | <0.01 |
| Unadjusted | p-Value | Adjusted | p-Value | |
|---|---|---|---|---|
| Skin color declared | <0.01 | 0.01 | ||
| Caucasian | 1.00 | 1.00 | ||
| Black or mixed | 1.52 (1.11–2.08) | 1.53 (1.12–2.10) | ||
| Prenatal care | <0.01 | <0.01 | ||
| Adequate | 1.00 | 1.00 | ||
| Inadequate | 3.06 (2.24–4.19) | 2.94 (2.14–4.05) | ||
| Initiation of prenatal care | 0.03 | 0.47 | ||
| 1–3 month | 1.00 | 1.00 | ||
| 4–6 month | 1.64 (1.14–2.35) | 1.01 (0.67–1.50) | ||
| 7–9 month | 1.03 (0.34–3.10) | 0.51 (0.16–1.68) | ||
| PM10 exposure in the first trimester of pregnancy | 1.01 (0.96–1.06) | 0.75 | 1.27 (1.06–1.52) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, R.D.; dos Santos, M.; de Moura, F.R.; Muccillo-Baisch, A.L.; Baisch, P.R.M.; Soares, M.C.F.; da Silva Júnior, F.M.R. Gestational and Neonatal Outcomes in Cities in the Largest Coal Mining Region in Brazil. Int. J. Environ. Res. Public Health 2022, 19, 12107. https://doi.org/10.3390/ijerph191912107
Soares RD, dos Santos M, de Moura FR, Muccillo-Baisch AL, Baisch PRM, Soares MCF, da Silva Júnior FMR. Gestational and Neonatal Outcomes in Cities in the Largest Coal Mining Region in Brazil. International Journal of Environmental Research and Public Health. 2022; 19(19):12107. https://doi.org/10.3390/ijerph191912107
Chicago/Turabian StyleSoares, Renata Dupont, Marina dos Santos, Fernando Rafael de Moura, Ana Luiza Muccillo-Baisch, Paulo Roberto Martins Baisch, Maria Cristina Flores Soares, and Flavio Manoel Rodrigues da Silva Júnior. 2022. "Gestational and Neonatal Outcomes in Cities in the Largest Coal Mining Region in Brazil" International Journal of Environmental Research and Public Health 19, no. 19: 12107. https://doi.org/10.3390/ijerph191912107
APA StyleSoares, R. D., dos Santos, M., de Moura, F. R., Muccillo-Baisch, A. L., Baisch, P. R. M., Soares, M. C. F., & da Silva Júnior, F. M. R. (2022). Gestational and Neonatal Outcomes in Cities in the Largest Coal Mining Region in Brazil. International Journal of Environmental Research and Public Health, 19(19), 12107. https://doi.org/10.3390/ijerph191912107