
Using Convolutional Neural Networks to Derive Neighborhood Built Environments from Google Street View Images and Examine Their Associations with Health Outcomes


 ,
,  ,
, 
Abstract
:1. Introduction
Study Aims and Hypotheses
2. Materials and Methods
2.1. Google Street View Image Collection
2.1.1. Data Collection
2.1.2. Data Processing
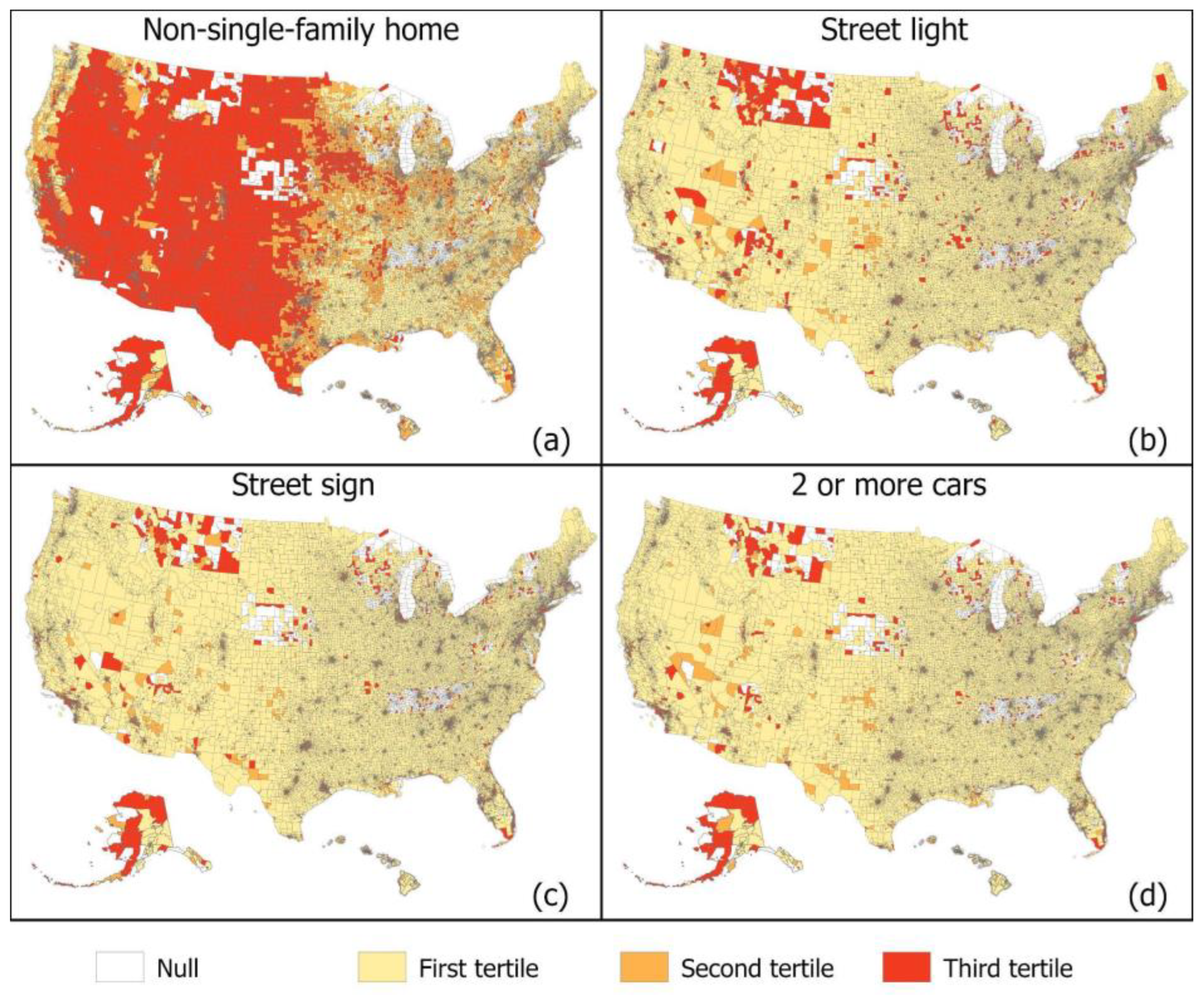
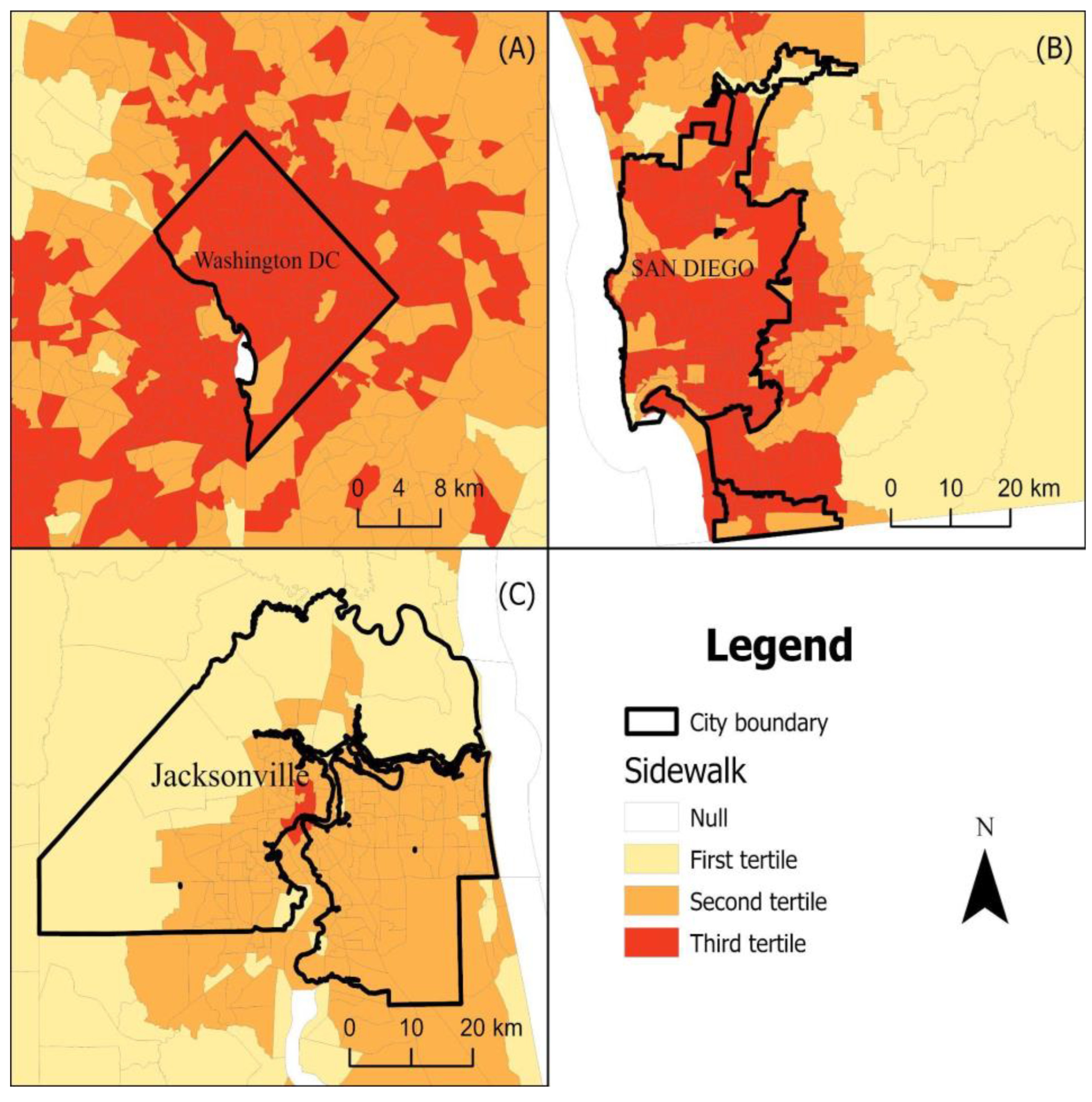
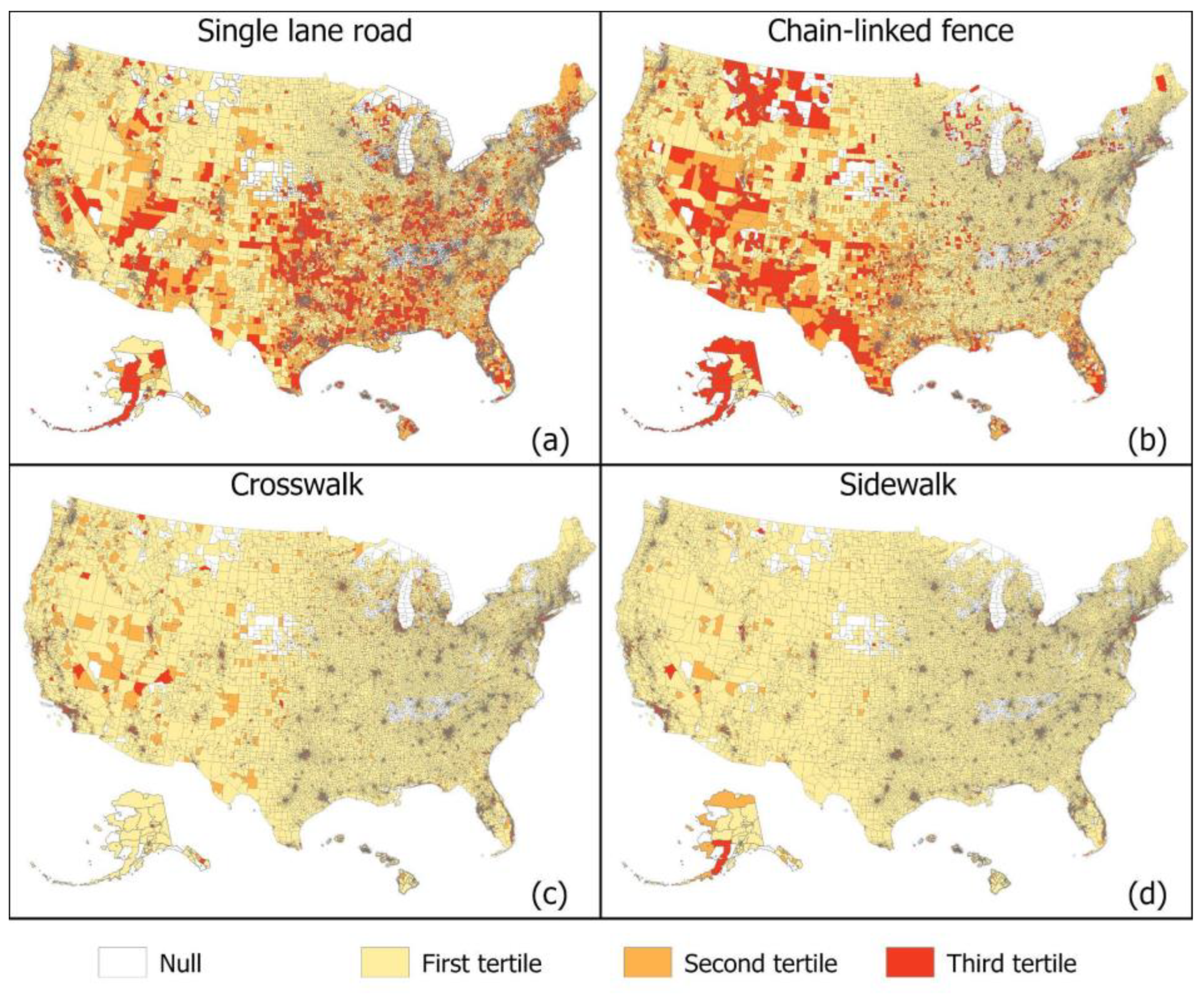
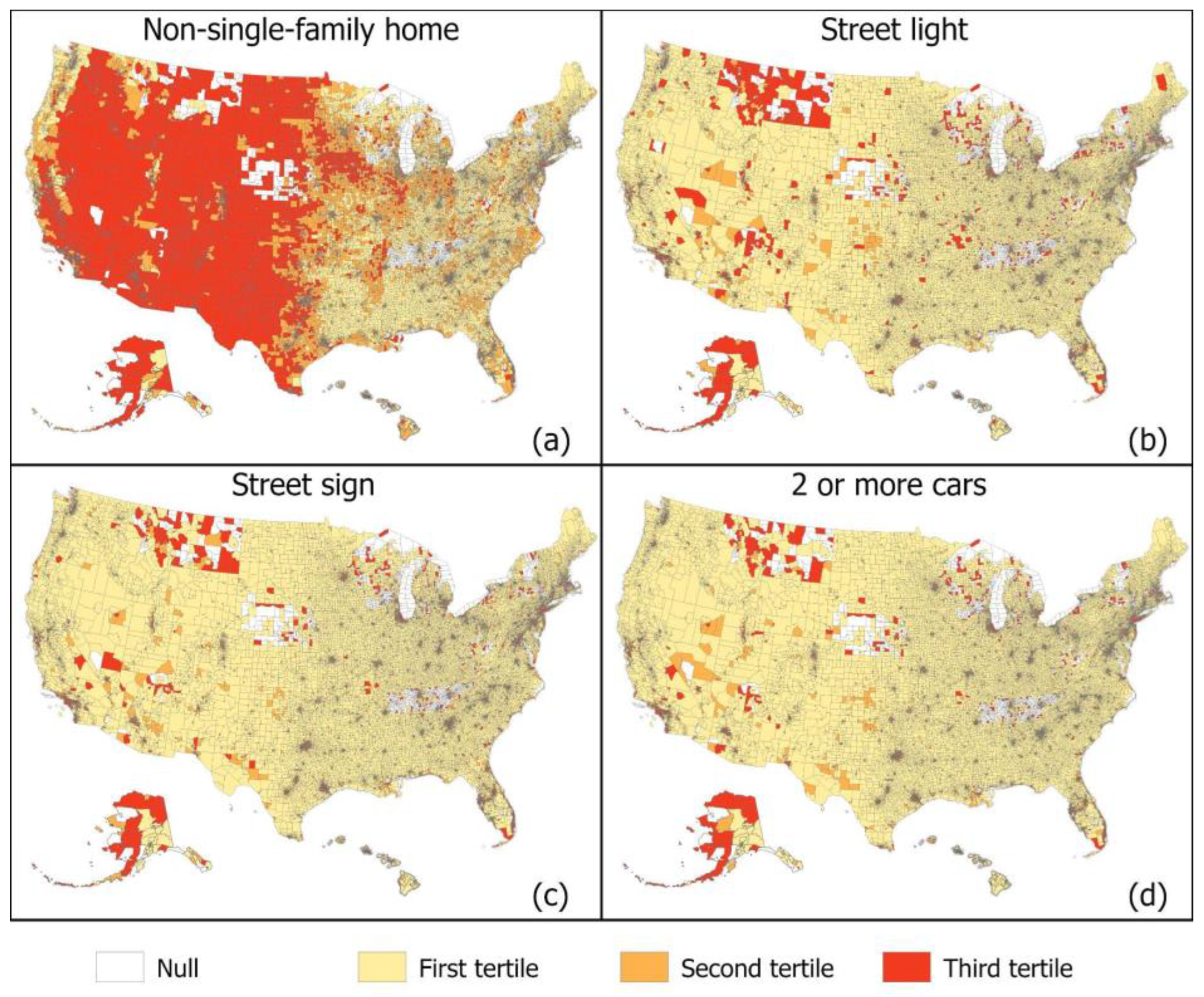
2.1.3. Built Environment Indicators
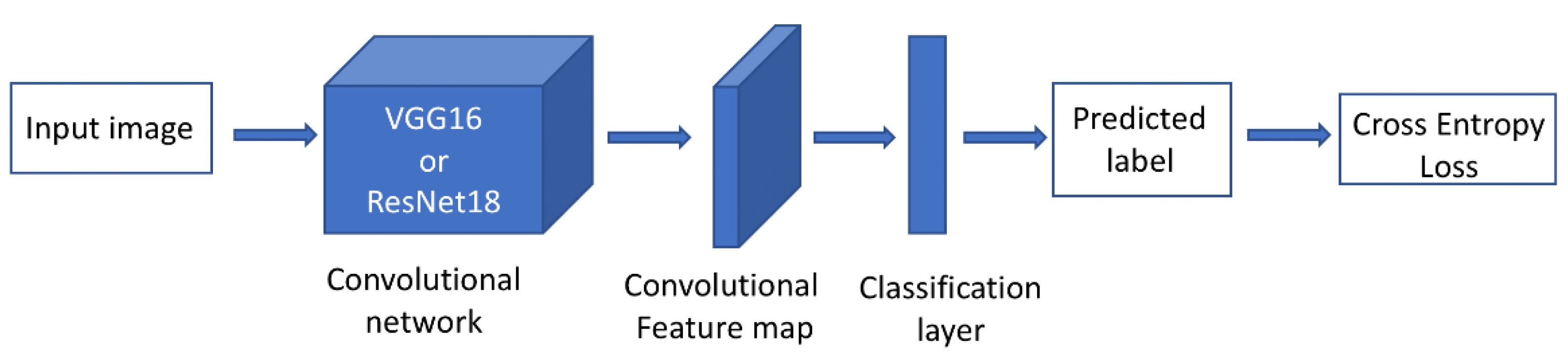
2.1.4. Computer Vision Model Building and Validation Results
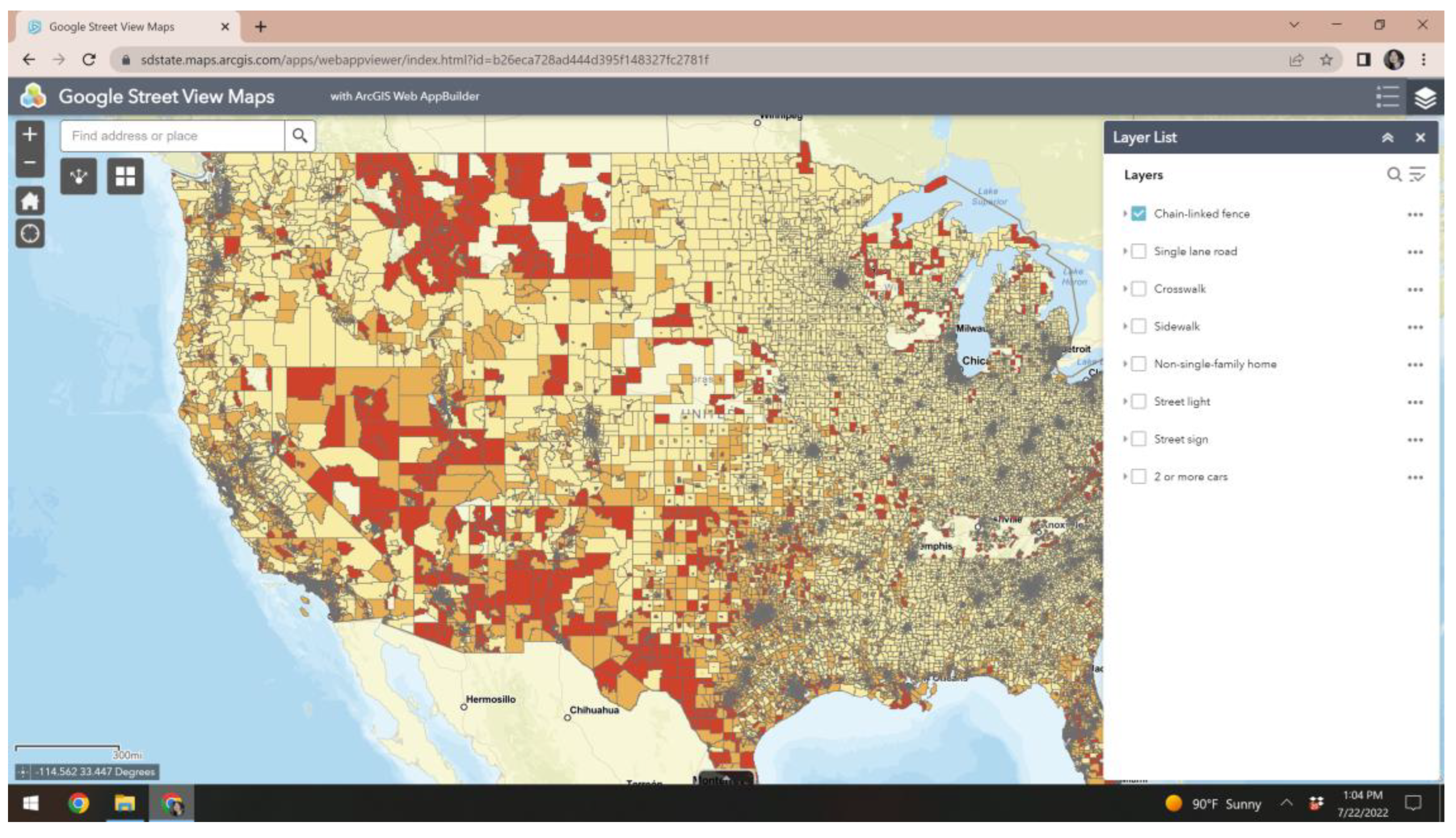
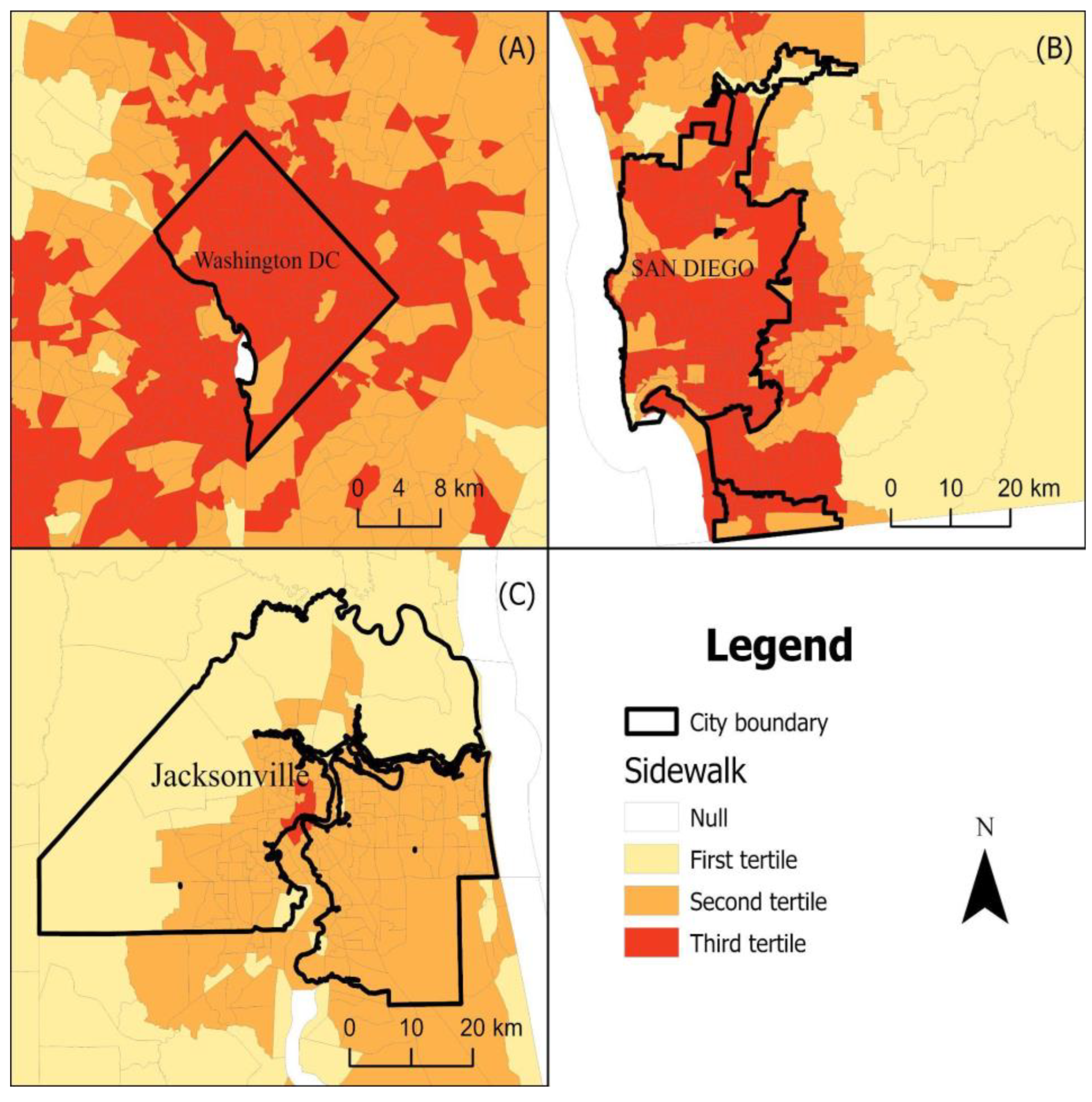
2.2. Geoportal
- Select the GSV variable to display (e.g., sidewalk);
- Type a location or address in the search bar and the map will zoom to that area
- Darker colors signal higher prevalence of neighborhood feature
2.3. Demographic and Socioeconomic Data
2.4. Health Outcome Data
2.5. Statistical Analyses
3. Results
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cagney, K.A.; Browning, C.R. Exploring Neighborhood-Level Variation in Asthma and Other Respiratory Diseases: The Contribution of Neighborhood Social Context. J. Gen. Intern. Med. 2004, 19, 229–236. [Google Scholar] [CrossRef]
- Malambo, P.; Kengne, A.P.; De Villiers, A.; Lambert, E.V.; Puoane, T. Built Environment, Selected Risk Factors and Major Cardiovascular Disease Outcomes: A Systematic Review. PLoS ONE 2016, 11, e0166846. [Google Scholar] [CrossRef] [PubMed]
- Grigsby-Toussaint, D.S.; Lipton, R.; Chavez, N.; Handler, A.; Johnson, T.P.; Kubo, J. Neighborhood Socioeconomic Change and Diabetes RiskFindings from the Chicago Childhood Diabetes Registry. Diabetes Care 2010, 33, 1065–1068. [Google Scholar] [CrossRef]
- Eames, M.; Ben-Shlomo, Y.; Marmot, M.G. Social Deprivation and Premature Mortality: Regional Comparison across England. Br. Med. J. 1993, 307, 1097–1102. [Google Scholar] [CrossRef]
- Cohen, D.A.; Mason, K.; Bedimo, A.; Scribner, R.; Basolo, V.; Farley, T.A. Neighborhood Physical Conditions and Health. Am. J. Public Health 2003, 93, 467. [Google Scholar] [CrossRef]
- Brown, S.C.; Mason, C.A.; Lombard, J.L.; Martinez, F.; Plater-Zyberk, E.; Spokane, A.R.; Newman, F.L.; Pantin, H.; Szapocznik, J. The Relationship of Built Environment to Perceived Social Support and Psychological Distress in Hispanic Elders: The Role of “Eyes on the Street”. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2009, 64B, 234. [Google Scholar] [CrossRef]
- CDC Designing Activity-Friendly Communities. Available online: https://www.cdc.gov/nccdphp/dnpao/features/walk-friendly-communities/index.html (accessed on 1 August 2022).
- Adams, M.A.A.-P.; Christine, B. AU-Patel, AksharAU-Middel, ArianeTI-Training Computers to See the Built Environment Related to Physical Activity: Detection of Microscale Walkability Features Using Computer Vision Training Computers to See the Built Environment Related to Physical Activity: Detection of Microscale Walkability Features Using Computer Vision. Int. J. Environ. Res. Public. Health 2022, 19, 4548. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, J. Health Impacts of Nonmotorized Travel Behavior and the Built Environment: Evidence from the 2017 National Household Travel Survey. J. Transp. Health 2022, 26, 101404. [Google Scholar] [CrossRef]
- Sullivan, W.; Chang, C.-Y. Mental Health and the Built Environment. In Making Healthy Places; Island Press: Washington, DC, USA, 2011; pp. 106–116. ISBN 978-1-61091-036-1. [Google Scholar]
- Eyler, A.A.; Blanck, H.M.; Gittelsohn, J.; Karpyn, A.; McKenzie, T.L.; Partington, S.; Slater, S.J.; Winters, M. Physical Activity and Food Environment Assessments. Am. J. Prev. Med. 2015, 48, 639–645. [Google Scholar] [CrossRef]
- Schmidt, N.M.; Tchetgen Tchetgen, E.J.; Ehntholt, A.; Almeida, J.; Nguyen, Q.C.; Molnar, B.E.; Azrael, D.; Osypuk, T.L. Does neighborhood collective efficacy for families change over time? the boston neighborhood survey: Stability of Neighborhood Collective Efficacy for Families. J. Community Psychol. 2014, 42, 61–79. [Google Scholar] [CrossRef]
- National Archive of Criminal Justice Project on Human Development in Chicago Neighborhoods. 2012. Available online: http://icpsr.umich.edu/web/pages/NACJD/ (accessed on 3 February 2013).
- Bader, M.D.M.; Mooney, S.J.; Lee, Y.J.; Sheehan, D.; Neckerman, K.M.; Rundle, A.G.; Teitler, J.O. Development and Deployment of the Computer Assisted Neighborhood Visual Assessment System (CANVAS) to Measure Health-Related Neighborhood Conditions. Health Place 2015, 31, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Peng, L.; Wu, C.; Zhang, J. Street View Imagery (SVI) in the Built Environment: A Theoretical and Systematic Review. Buildings 2022, 12, 1167. [Google Scholar] [CrossRef]
- Rundle, A.G.; Bader, M.D.M.; Richards, C.A.; Neckerman, K.M.; Teitler, J.O. Using Google Street View to Audit Neighborhood Environments. Am. J. Prev. Med. 2011, 40, 94. [Google Scholar] [CrossRef] [PubMed]
- Giles, W.H.; Holmes-Chavez, A.; Collins, J.L. Cultivating Healthy Communities: The CDC Perspective. Health Promot. Pract. 2009, 10, 86S–87S. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.H. Feature Extraction and Image Recognition with Convolutional Neural Networks. J. Phys. Conf. Ser. 2018, 1087, 062032. [Google Scholar] [CrossRef]
- Liu, Y.; Pu, H.; Sun, D.-W. Efficient Extraction of Deep Image Features Using Convolutional Neural Network (CNN) for Applications in Detecting and Analysing Complex Food Matrices. Trends Food Sci. Technol. 2021, 113, 193–204. [Google Scholar] [CrossRef]
- Lawrence, S.; Giles, C.L.; Tsoi, A.C.; Back, A.D. Back Face Recognition: A Convolutional Neural-Network Approach. IEEE Trans. Neural Netw. 1997, 8, 98–113. [Google Scholar] [CrossRef]
- Liu, Y.; Racah, E.; Prabhat; Correa, J.; Khosrowshahi, A.; Lavers, D.; Kunkel, K.; Wehner, M.; Collins, W. Application of Deep Convolutional Neural Networks for Detecting Extreme Weather in Climate Datasets. arXiv 2016, arXiv:1605.01156. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. In Proceedings of the Advances in Neural Information Processing Systems, Lake Tahoe, NV, USA, 3–6 December 2012; Pereira, F., Burges, C.J., Bottou, L., Weinberger, K.Q., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2012; Volume 25. [Google Scholar]
- Hentschel, C.; Wiradarma, T.P.; Sack, H. Fine Tuning CNNS with Scarce Training Data—Adapting Imagenet to Art Epoch Classification. In Proceedings of the 2016 IEEE International Conference on Image Processing (ICIP), Phoenix, AZ, USA, 25 September 2016; pp. 3693–3697. [Google Scholar]
- Odgers, C.L.; Caspi, A.; Bates, C.J.; Sampson, R.J.; Moffitt, T.E. Systematic Social Observation of Children’s Neighborhoods Using Google Street View: A Reliable and Cost-Effective Method: SSO in Street View. J. Child Psychol. Psychiatry 2012, 53, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would You Be Happier Living in a Greener Urban Area? A Fixed-Effects Analysis of Panel Data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.K.; Sessions, J.; Board, T. Logging Truck Speeds on Curves and Favorable Grades of Single-Lane Roads. Transp. Res. Rec. 1987, 1106, 112–118. [Google Scholar]
- Yamada, I.; Brown, B.B.; Smith, K.R.; Zick, C.D.; Kowaleski-Jones, L.; Fan, J.X. Mixed Land Use and Obesity: An Empirical Comparison of Alternative Land Use Measures and Geographic Scales. Prof. Geogr. J. Assoc. Am. Geogr. 2012, 64, 157–177. [Google Scholar] [CrossRef] [PubMed]
- Neckerman, K.M.; Lovasi, G.S.; Davies, S.; Purciel, M.; Quinn, J.; Feder, E.; Raghunath, N.; Wasserman, B.; Rundle, A. Disparities in Urban Neighborhood Conditions: Evidence from GIS Measures and Field Observation in New York City. J. Public Health Policy 2009, 30, S264–S285. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B. Socioeconomic Status Differences in Recreational Physical Activity Levels and Real and Perceived Access to a Supportive Physical Environment. Prev. Med. 2002, 35, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Galanis, A.; Eliou, N. Evaluation of the Pedestrian Infrastructure Using Walkability Indicators. WSEAS Trans. Environ. Dev. 2011, 7, 385–394. [Google Scholar]
- Remigio, R.V.; Zulaika, G.; Rabello, R.S.; Bryan, J.; Sheehan, D.M.; Galea, S.; Carvalho, M.S.; Rundle, A.; Lovasi, G.S. A Local View of Informal Urban Environments: A Mobile Phone-Based Neighborhood Audit of Street-Level Factors in a Brazilian Informal Community. J. Urban Health 2019, 96, 537–548. [Google Scholar] [CrossRef]
- Kenner, A.; Nobles, E.; Stalcup, S. Cultivating a Politics of Sight for Vacant Land Use in Cities. Anthropol. Q. 2022, 95, 387–415. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar] [CrossRef]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. TensorFlow: A System for Large-Scale Machine Learning. In Proceedings of the 12th USENIX Symposium on Operating Systems Design and Implementation (OSDI 16), Savannah, GA, USA, 2–4 November 2016; pp. 265–283. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. arXiv 2015, arXiv:1512.03385. [Google Scholar] [CrossRef]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An Imperative Style, High-Performance Deep Learning Library. In Proceedings of the Advances in Neural Information Processing Systems, Vancouver, BC, Canada, 8–14 December 2019; Wallach, H., Larochelle, H., Beygelzimer, A., Alché-Buc, F.d’., Fox, E., Garnett, R., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2019; Volume 32. [Google Scholar]
- Quinn, J.W.; Mooney, S.J.; Sheehan, D.M.; Teitler, J.O.; Neckerman, K.M.; Kaufman, T.K.; Lovasi, G.S.; Bader, M.D.M.; Rundle, A.G. Neighborhood Physical Disorder in New York City. J. Maps 2016, 12, 53–60. [Google Scholar] [CrossRef]
- Mayne, S.; Jose, A.; Mo, A.; Vo, L.; Rachapalli, S.; Ali, H.; Davis, J.; Kershaw, K. Neighborhood Disorder and Obesity-Related Outcomes among Women in Chicago. Int. J. Environ. Res. Public. Health 2018, 15, 1395. [Google Scholar] [CrossRef] [PubMed]
- Auler, M.M.; Lopes, C.d.S.; Cortes, T.R.; Bloch, K.V.; Junger, W.L. Neighborhood Physical Disorder and Common Mental Disorders in Adolescence. Int. Arch. Occup. Environ. Health 2021, 94, 631–638. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Neighborhood Disadvantage, Disorder, and Health. J. Health Soc. Behav. 2001, 42, 258–276. [Google Scholar] [CrossRef]
- Nguyen, Q.C.; Khanna, S.; Dwivedi, P.; Huang, D.; Huang, Y.; Tasdizen, T.; Brunisholz, K.D.; Li, F.; Gorman, W.; Nguyen, T.T.; et al. Using Google Street View to Examine Associations between Built Environment Characteristics and U.S. Health Outcomes. Prev. Med. Rep. 2019, 14, 100859. [Google Scholar] [CrossRef] [PubMed]
- Keralis, J.M.; Javanmardi, M.; Khanna, S.; Dwivedi, P.; Huang, D.; Tasdizen, T.; Nguyen, Q.C. Health and the Built Environment in United States Cities: Measuring Associations Using Google Street View-Derived Indicators of the Built Environment. BMC Public Health 2020, 20, 215. [Google Scholar] [CrossRef]
- Halperin, D. Environmental Noise and Sleep Disturbances: A Threat to Health? Sleep Sci. 2014, 7, 209. [Google Scholar] [CrossRef]
- Garcia, M.C.; Faul, M.; Dowling, N.F.; Thomas, C.C.; Iademarco, M.F. Bridging the Gap in Potentially Excess Deaths Between Rural and Urban Counties in the United States. Public Health Rep. 2020, 135, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and Access to Healthy Food in the United States: A Review of Food Deserts Literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef]
- Kegler, M.C.; Gauthreaux, N.; Hermstad, A.; Arriola, K.J.; Mickens, A.; Ditzel, K.; Hernandez, C.; Haardörfer, R. Inequities in Physical Activity Environments and Leisure-Time Physical Activity in Rural Communities. Prev. Chronic. Dis. 2022, 19, 210417. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.A.; Weinberger, A.H.; Eggers, E.M.; Parker, E.S.; Villanti, A.C. Trends in Rural and Urban Cigarette Smoking Quit Ratios in the US From 2010 to 2020. JAMA Netw. Open 2022, 5, e2225326. [Google Scholar] [CrossRef] [PubMed]
- Doogan, N.J.; Roberts, M.E.; Wewers, M.E.; Stanton, C.A.; Keith, D.R.; Gaalema, D.E.; Kurti, A.N.; Redner, R.; Cepeda-Benito, A.; Bunn, J.Y.; et al. A Growing Geographic Disparity: Rural and Urban Cigarette Smoking Trends in the United States. Prev. Med. 2017, 104, 79–85. [Google Scholar] [CrossRef]
- Gaffney, A.W.; Hawks, L.; White, A.C.; Woolhandler, S.; Himmelstein, D.; Christiani, D.C.; McCormick, D. Health Care Disparities Across the Urban-Rural Divide: A National Study of Individuals with COPD. J. Rural Health 2022, 38, 207–216. [Google Scholar] [CrossRef]
- Matthews, K.A.; Croft, J.B.; Liu, Y.; Lu, H.; Kanny, D.; Wheaton, A.G.; Cunningham, T.J.; Khan, L.K.; Caraballo, R.S.; Holt, J.B.; et al. Health-Related Behaviors by Urban-Rural County Classification—United States, 2013. MMWR Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef]
- Li, J.; Yao, Y.; Dong, Q.; Dong, Y.; Liu, J.; Yang, L.; Huang, F. Characterization and Factors Associated with Sleep Quality among Rural Elderly in China. Arch. Gerontol. Geriatr. 2013, 56, 237–243. [Google Scholar] [CrossRef]
- Jones, V.N.; Bucchio, J. The Sleep Gap: Advancing Healthy Sleep among Youth in Rural Communities. Contemp. Rural. Soc. Work. J. 2018, 10, 3. [Google Scholar]
- Sarkar, C.; Webster, C.; Gallacher, J. Neighbourhood Walkability and Incidence of Hypertension: Findings from the Study of 429,334 UK Biobank Participants. Int. J. Hyg. Environ. Health 2018, 221, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Lovasi, G.S.; Moudon, A.V.; Pearson, A.L.; Hurvitz, P.M.; Larson, E.B.; Siscovick, D.S.; Berke, E.M.; Lumley, T.; Psaty, B.M. Using Built Environment Characteristics to Predict Walking for Exercise. Int. J. Health Geogr. 2008, 7, 10. [Google Scholar] [CrossRef]
- Chen, B.-I.; Hsueh, M.-C.; Rutherford, R.; Park, J.-H.; Liao, Y. The Associations between Neighborhood Walkability Attributes and Objectively Measured Physical Activity in Older Adults. PLoS ONE 2019, 14, e0222268. [Google Scholar] [CrossRef]
- Ki, M.; Shim, H.-Y.; Lim, J.; Hwang, M.; Kang, J.; Na, K.-S. Preventive Health Behaviors among People with Suicide Ideation Using Nationwide Cross-Sectional Data in South Korea. Sci. Rep. 2022, 12, 11615. [Google Scholar] [CrossRef] [PubMed]
- Pj, C.; Se, L.; Sm, C. Exercise for the Treatment of Depression and Anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [Google Scholar] [CrossRef]
- Em, B.; Lm, G.; Av, M.; Eb, L. Protective Association between Neighborhood Walkability and Depression in Older Men. J. Am. Geriatr. Soc. 2007, 55, 526–533. [Google Scholar] [CrossRef]
- van den Berg, P.; Kemperman, A.; de Kleijn, B.; Borgers, A. Ageing and Loneliness: The Role of Mobility and the Built Environment. Plan. Qual. Life 2016, 5, 48–55. [Google Scholar] [CrossRef]
- Phan, L.; Yu, W.; Keralis, J.M.; Mukhija, K.; Dwivedi, P.; Brunisholz, K.D.; Javanmardi, M.; Tasdizen, T.; Nguyen, Q.C. Google Street View Derived Built Environment Indicators and Associations with State-Level Obesity, Physical Activity, and Chronic Disease Mortality in the United States. Int. J. Environ. Res. Public. Health 2020, 17, 3659. [Google Scholar] [CrossRef]
- Nguyen, Q.C.; Keralis, J.; Dwivedi, P.; Ng, A.E.; Javanmardi, M.; Khanna, S.; Huang, Y.; Brunisholz, K.D.; Kumar, A.; Tasdizen, T. Leveraging 31 Million Google Street View Images to Characterize Built Environments and Examine County Health Outcomes. Public Health Rep. 2021, 136, 201–211. [Google Scholar] [CrossRef]
- Hunter, J.C.; Hayden, K.M. The Association of Sleep with Neighborhood Physical and Social Environment. Public Health 2018, 162, 126–134. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Mean (SD) | |
|---|---|---|
| Built environment characteristics | ||
| Crosswalks | 70,359 | 3.63 (4.37) |
| Sidewalks | 70,359 | 43.96 (30.72) |
| Single lane road | 70,359 | 67.11 (14.57) |
| Presence of apartment/commercial building | 70,359 | 29.80 (23.69) |
| Streetlights | 70,319 | 15.66 (14.96) |
| Street signs | 70,344 | 24.28 (15.08) |
| 2 or more cars | 70,288 | 36.10 (20.53) |
| Chain Link fence | 70,311 | 7.63 (13.79) |
| Census tract characteristics | ||
| Population size | 72,864 | 4237.29 (1972.52) |
| Percent 65 years+ | 72,578 | 13.63 (7.39) |
| Percent male | 72,578 | 49.18 (4.05) |
| Percent Black | 72,578 | 13.83 (22.29) |
| Percent Hispanic | 72,578 | 15.27 (20.82) |
| Percent single female headed households | 72,472 | 13.65 (8.17) |
| Percent owner-occupied housing | 72,472 | 64.32 (22.50) |
| Percent college educated | 72,436 | 27.67 (18.50) |
| Median household income | 72,048 | 67,432.68 (32,960.44) |
| Percent unemployed | 72,330 | 10.36 (6.34) |
| Child opportunity index, range 0 to 100 | 72,213 | 49.15 (28.61) |
| Adult health outcomes | ||
| Obesity | 70,338 | 32.63 (6.82) |
| Diabetes | 70,338 | 10.96 (3.73) |
| High Blood Pressure | 70,338 | 32.49 (7.36) |
| High Cholesterol | 70,338 | 31.83 (4.79) |
| Cancer | 70,338 | 6.73 (1.94) |
| Poor mental health days | 70,338 | 15.21 (3.57) |
| Depression | 72,337 | 36.77 (5.23) |
| Sleep less than 7 h a night | 70,338 | 17.61 (3.45) |
| Current Smoking | 70,338 | 17.98 (5.76) |
| Obese | High Blood Pressure | High Cholesterol | Diabetes | Cancer | |
|---|---|---|---|---|---|
| Built Environment Characteristics | Crude Odds Ratio (95% CI) | Crude Odds Ratio (95% CI) | Crude Odds Ratio (95% CI) | Crude Odds Ratio (95% CI) | Crude Odds Ratio (95% CI) |
| Single lane road | |||||
| 3rd tertile (highest) | 2.19 (2.06, 2.31) | 3.23 (3.09, 3.36) | 2.18 (2.09, 2.26) | 0.75 (0.69, 0.82) | 0.69 (0.66, 0.73) |
| 2nd tertile | 1.11 (0.99, 1.24) | 1.71 (1.58, 1.84) | 1.41 (1.33, 1.50) | 0.21 (0.14, 0.28) | 0.50 (0.46, 0.53) |
| 2 or more cars | |||||
| 3rd tertile (highest) | −1.97 (−2.09, −1.84) | −3.46 (−3.60, −3.33) | −4.43 (−4.51, −4.34) | 0.34 (0.27, 0.40) | −1.80 (−1.84, −1.77) |
| 2nd tertile | −1.46 (−1.58, −1.33) | −2.15 (−2.29, −2.02) | −2.20 (−2.28, −2.12) | −0.33 (−0.40, −0.26) | −0.71 (−0.75, −0.68) |
| Street signs | |||||
| 3rd tertile (highest) | −2.44 (−2.56, −2.31) | −4.45 (−4.58, −4.32) | −4.68 (−4.76, −4.60) | −0.05 (−0.12, 0.02) | −1.96 (−2.00, −1.93) |
| 2nd tertile | −1.02 (−1.14, −0.89) | −2.04 (−2.17, −1.91) | −2.55 (−2.63, −2.47) | −0.27 (−0.34, −0.20) | −0.81 (−0.84, −0.77) |
| Street lights | |||||
| 3rd tertile (highest) | −1.49 (−1.62, −1.37) | −3.04 (−3.17, −2.91) | −3.89 (−3.97, −3.81) | 0.35 (0.28, 0.42) | −1.64 (−1.68, −1.61) |
| 2nd tertile | −0.86 (−0.99, −0.74) | −2.74 (−2.87, −2.60) | −2.82 (−2.91, −2.74) | −0.54 (−0.61, −0.47) | −0.89 (−0.92, −0.86) |
| Non-single family home | |||||
| 3rd tertile (highest) | −1.58 (−1.70, −1.45) | −3.56 (−3.70, −3.43) | −3.77 (−3.85, −3.69) | 0.12 (0.05, 0.19) | −1.60 (−1.63, −1.56) |
| 2nd tertile | −0.08 (−0.21, 0.04) | −1.20 (−1.33, −1.07) | −1.43 (−1.51, −1.34) | 0.06 (−0.01, 0.13) | −0.59 (−0.62, −0.55) |
| Sidewalks | |||||
| 3rd tertile (highest) | −4.09 (−4.21, −3.96) | −5.83 (−5.95, −5.70) | −5.06 (−5.13, −4.98) | −0.94 (−1.01, −0.87) | −1.82 (−1.85, −1.79) |
| 2nd tertile | −2.33 (−2.45, −2.21) | −3.23 (−3.36, −3.10) | −2.85 (−2.92, −2.77) | −0.78 (−0.85, −0.71) | −0.77 (−0.81, −0.74) |
| Crosswalks | |||||
| 3rd tertile (highest) | −4.49 (−4.61, −4.37) | −5.99 (−6.12, −5.86) | −4.86 (−4.94, −4.78) | −1.25 (−1.32, −1.18) | −1.57 (−1.61, −1.54) |
| 2nd tertile | −1.84 (−1.96, −1.72) | −2.68 (−2.81, −2.55) | −2.40 (−2.48, −2.32) | −0.58 (−0.65, −0.51) | −0.68 (−0.71, −0.65) |
| N | 67,445 | 67,445 | 67,445 | 67,445 | 67,445 |
| Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b | |
| Single lane road | |||||
| 3rd tertile (highest) | 1.34 (1.26, 1.42) | 1.15 (1.08, 1.21) | 0.65 (0.60, 0.70) | 0.34 (0.31, 0.38) | 0.11 (0.10, 0.12) |
| 2nd tertile | 0.76 (0.68, 0.83) | 0.67 (0.60, 0.73) | 0.35 (0.30, 0.40) | 0.14 (0.11, 0.18) | 0.08 (0.07, 0.09) |
| 2 or more cars | |||||
| 3rd tertile (highest) | −3.39 (−3.48, −3.30) | −2.90 (−2.98, −2.82) | −1.67 (−1.74, −1.61) | −1.23 (−1.28, −1.19) | −0.37 (−0.38, −0.36) |
| 2nd tertile | −0.98 (−1.06, −0.90) | −1.55 (−1.61, −1.48) | −1.05 (−1.10, −0.99) | −0.72 (−0.76, −0.69) | −0.18 (−0.19, −0.17) |
| Street signs | |||||
| 3rd tertile (highest) | −2.71 (−2.81, −2.62) | −2.34 (−2.42, −2.26) | −1.32 (−1.39, −1.26) | −0.92 (−0.97, −0.88) | −0.31 (−0.32, −0.30) |
| 2nd tertile | −1.11 (−1.19, −1.03) | −1.44 (−1.51, −1.38) | −0.87 (−0.92, −0.81) | −0.68 (−0.72, −0.65) | −0.15 (−0.16, −0.14) |
| Street lights | |||||
| 3rd tertile (highest) | −1.56 (−1.65, −1.48) | −0.83 (−0.87, −0.80) | −1.99 (−2.07, −1.92) | −1.36 (−1.42, −1.30) | −0.28 (−0.29, −0.27) |
| 2nd tertile | −0.69 (−0.77, −0.61) | −0.62 (−0.65, −0.58) | −1.37 (−1.44, −1.30) | −1.00 (−1.05, −0.94) | −0.15 (−0.16, −0.14) |
| Non-single family home | |||||
| 3rd tertile (highest) | −1.90 (−1.99, −1.81) | −1.59 (−1.67, −1.52) | −1.00 (−1.06, −0.94) | −0.60 (−0.64, −0.56) | −0.19 (−0.20, −0.18) |
| 2nd tertile | −0.38 (−0.46, −0.31) | −0.67 (−0.74, −0.61) | −0.45 (−0.50, −0.40) | −0.27 (−0.30, −0.23) | −0.09 (−0.10, −0.08) |
| Sidewalks | |||||
| 3rd tertile (highest) | −3.07 (−3.16, −2.97) | −3.12 (−3.20, −3.04) | −1.85 (−1.91, −1.79) | −1.13 (−1.17, −1.09) | −0.34 (−0.35, −0.32) |
| 2nd tertile | −1.07 (−1.15, −0.98) | −1.71 (−1.78, −1.64) | −1.20 (−1.25, −1.14) | −0.75 (−0.79, −0.71) | −0.14 (−0.15, −0.13) |
| Crosswalks | |||||
| 3rd tertile (highest) | −2.99 (−3.08, −2.90) | −1.29 (−1.33, −1.25) | −3.07 (−3.14, −2.99) | −1.85 (−1.91, −1.79) | −0.28 (−0.29, −0.27) |
| 2nd tertile | −0.80 (−0.88, −0.72) | −0.63 (−0.67, −0.60) | −1.46 (−1.52, −1.39) | −0.96 (−1.01, −0.90) | −0.10 (−0.11, −0.09) |
| N | 67,167 | 67,167 | 67,167 | 67,167 | 67,167 |
| Poor Mental Health Days | Depression | Inadequate Sleep (<7 h a Night) | Current Smoking | |
|---|---|---|---|---|
| Built Environment Characteristics | Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b | Adjusted Odds Ratio (95% CI) b |
| Single lane road | ||||
| 3rd tertile (highest) | 0.51 (0.48, 0.55) | 0.82 (0.78, 0.87) | 0.19 (0.13, 0.24) | 0.82 (0.76, 0.87) |
| 2nd tertile | 0.32 (0.28, 0.35) | 0.60 (0.55, 0.64) | −0.19 (−0.25, −0.14) | 0.35 (0.30, 0.41) |
| Chain-linked fence | ||||
| 3rd tertile (highest) | 0.17 (0.12, 0.21) | 0.43 (0.37, 0.48) | −0.30 (−0.37, −0.24) | −0.58 (−0.65, −0.52) |
| 2nd tertile | −0.14 (−0.17, −0.10) | 0.10 (0.05, 0.14) | −0.40 (−0.45, −0.35) | −0.80 (−0.85, −0.75) |
| Crosswalks | ||||
| 3rd tertile (highest) | −0.80 (−0.84, −0.76) | −1.29 (−1.35, −1.23) | −0.56 (−0.62, −0.49) | −2.04 (−2.10, −1.97) |
| 2nd tertile | −0.16 (−0.19, −0.12) | −0.35 (−0.40, −0.30) | −0.15 (−0.21, −0.09) | −0.68 (−0.74, −0.63) |
| Sidewalks | ||||
| 3rd tertile (highest) | −0.89 (−0.93, −0.85) | −1.46 (−1.52, −1.40) | 0.51 (0.44, 0.57) | −1.68 (−1.74, −1.61) |
| 2nd tertile | −0.19 (−0.23, −0.16) | −0.37 (−0.42, −0.32) | 0.01 (−0.05, 0.07) | −0.65 (−0.71, −0.60) |
| Non-single family home | ||||
| 3rd tertile (highest) | −0.68 (−0.72, −0.64) | −1.37 (−1.43, −1.32) | −0.67 (−0.73, −0.60) | −1.11 (−1.17, −1.04) |
| 2nd tertile | −0.31 (−0.35, −0.28) | −0.44 (−0.48, −0.39) | −0.82 (−0.88, −0.77) | −0.51 (−0.56, −0.45) |
| Street lights | ||||
| 3rd tertile (highest) | −0.28 (−0.32, −0.25) | −0.80 (−0.86, −0.75) | −0.01 (−0.07, 0.05) | −1.02 (−1.09, −0.96) |
| 2nd tertile | −0.18 (−0.21, −0.14) | −0.25 (−0.30, −0.20) | −0.11 (−0.16, −0.05) | −0.57 (−0.63, −0.52) |
| Street signs | ||||
| 3rd tertile (highest) | −0.42 (−0.46, −0.38) | −0.81 (−0.87, −0.75) | 0.57 (0.50, 0.64) | −1.23 (−1.30, −1.16) |
| 2nd tertile | 0.18 (−0.22, −0.15) | −0.30 (−0.35, −0.25) | −0.02 (−0.07, 0.04) | −0.72 (−0.77, −0.66) |
| 2 or more cars | ||||
| 3rd tertile (highest) | −0.67 (−0.72, −0.63) | −1.18 (−1.24, −1.12) | 0.17 (0.10, 0.24) | −1.69 (−1.75, −1.62) |
| 2nd tertile | −0.17 (−0.20, −0.13) | −0.34 (−0.39, −0.29) | 0.04 (−0.02, 0.09) | −0.64 (−0.69, −0.58) |
| N | 67,167 | 67,167 | 67,167 | 67,167 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yue, X.; Antonietti, A.; Alirezaei, M.; Tasdizen, T.; Li, D.; Nguyen, L.; Mane, H.; Sun, A.; Hu, M.; Whitaker, R.T.; et al. Using Convolutional Neural Networks to Derive Neighborhood Built Environments from Google Street View Images and Examine Their Associations with Health Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 12095. https://doi.org/10.3390/ijerph191912095
Yue X, Antonietti A, Alirezaei M, Tasdizen T, Li D, Nguyen L, Mane H, Sun A, Hu M, Whitaker RT, et al. Using Convolutional Neural Networks to Derive Neighborhood Built Environments from Google Street View Images and Examine Their Associations with Health Outcomes. International Journal of Environmental Research and Public Health. 2022; 19(19):12095. https://doi.org/10.3390/ijerph191912095
Chicago/Turabian StyleYue, Xiaohe, Anne Antonietti, Mitra Alirezaei, Tolga Tasdizen, Dapeng Li, Leah Nguyen, Heran Mane, Abby Sun, Ming Hu, Ross T. Whitaker, and et al. 2022. "Using Convolutional Neural Networks to Derive Neighborhood Built Environments from Google Street View Images and Examine Their Associations with Health Outcomes" International Journal of Environmental Research and Public Health 19, no. 19: 12095. https://doi.org/10.3390/ijerph191912095
APA StyleYue, X., Antonietti, A., Alirezaei, M., Tasdizen, T., Li, D., Nguyen, L., Mane, H., Sun, A., Hu, M., Whitaker, R. T., & Nguyen, Q. C. (2022). Using Convolutional Neural Networks to Derive Neighborhood Built Environments from Google Street View Images and Examine Their Associations with Health Outcomes. International Journal of Environmental Research and Public Health, 19(19), 12095. https://doi.org/10.3390/ijerph191912095