
Embodied Cognition in Meditation, Yoga, and Ethics—An Experimental Single-Case Study on the Differential Effects of Four Mind–Body Treatments



Abstract
1. Introduction
2. Method
2.1. Procedure
2.2. Participants
2.3. Treatment
2.4. Measures
2.5. Data Analysis
3. Results
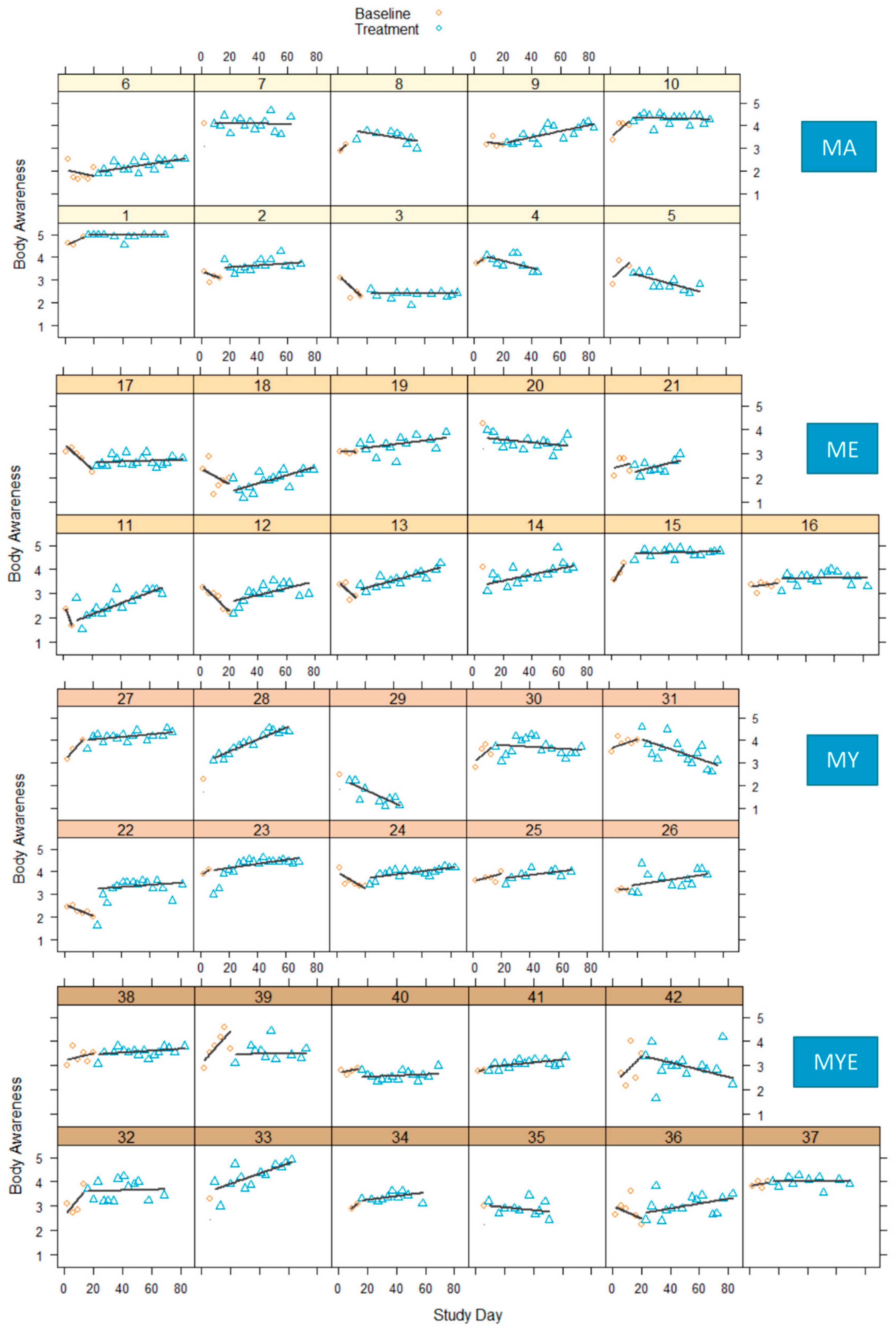
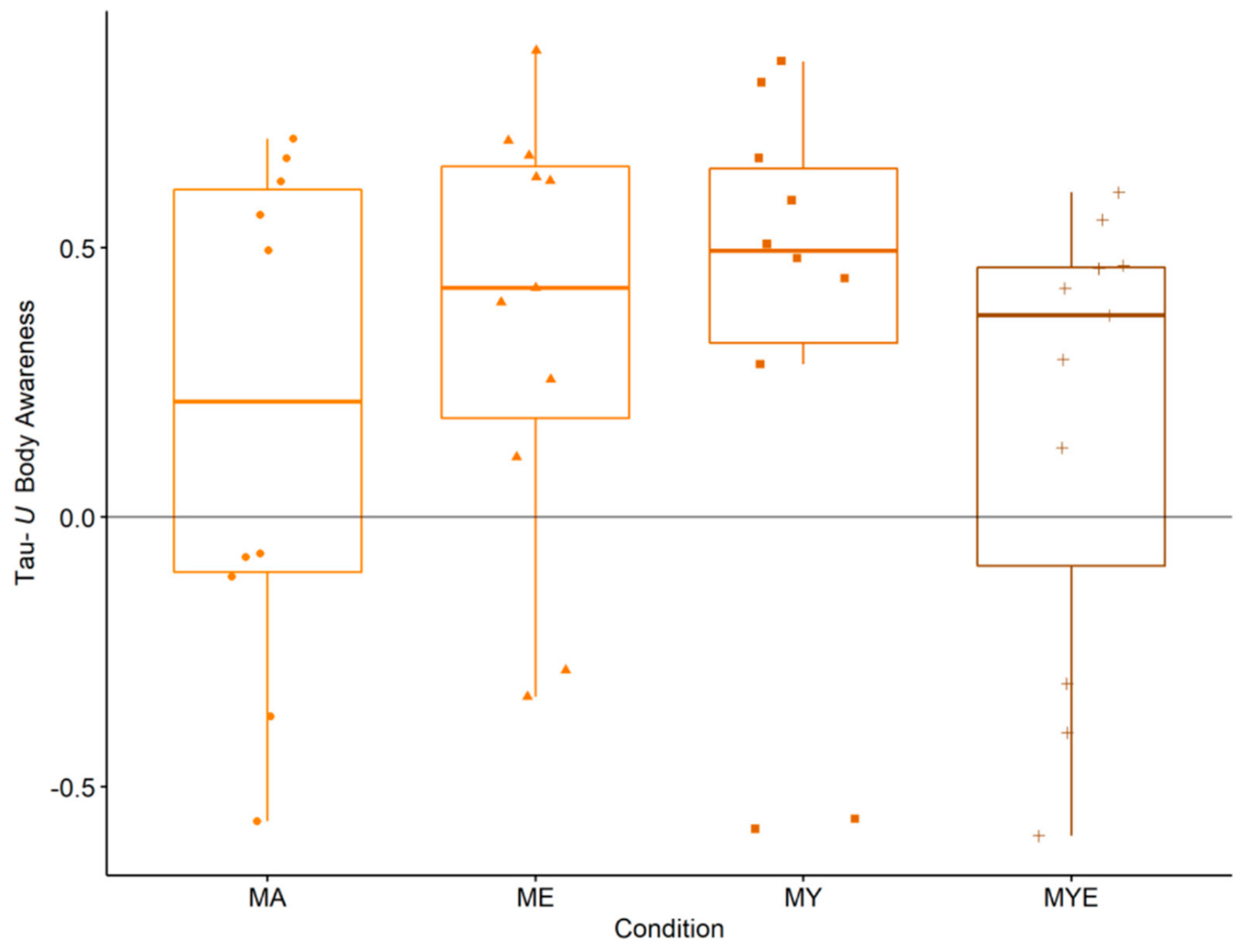
3.1. Body Awareness
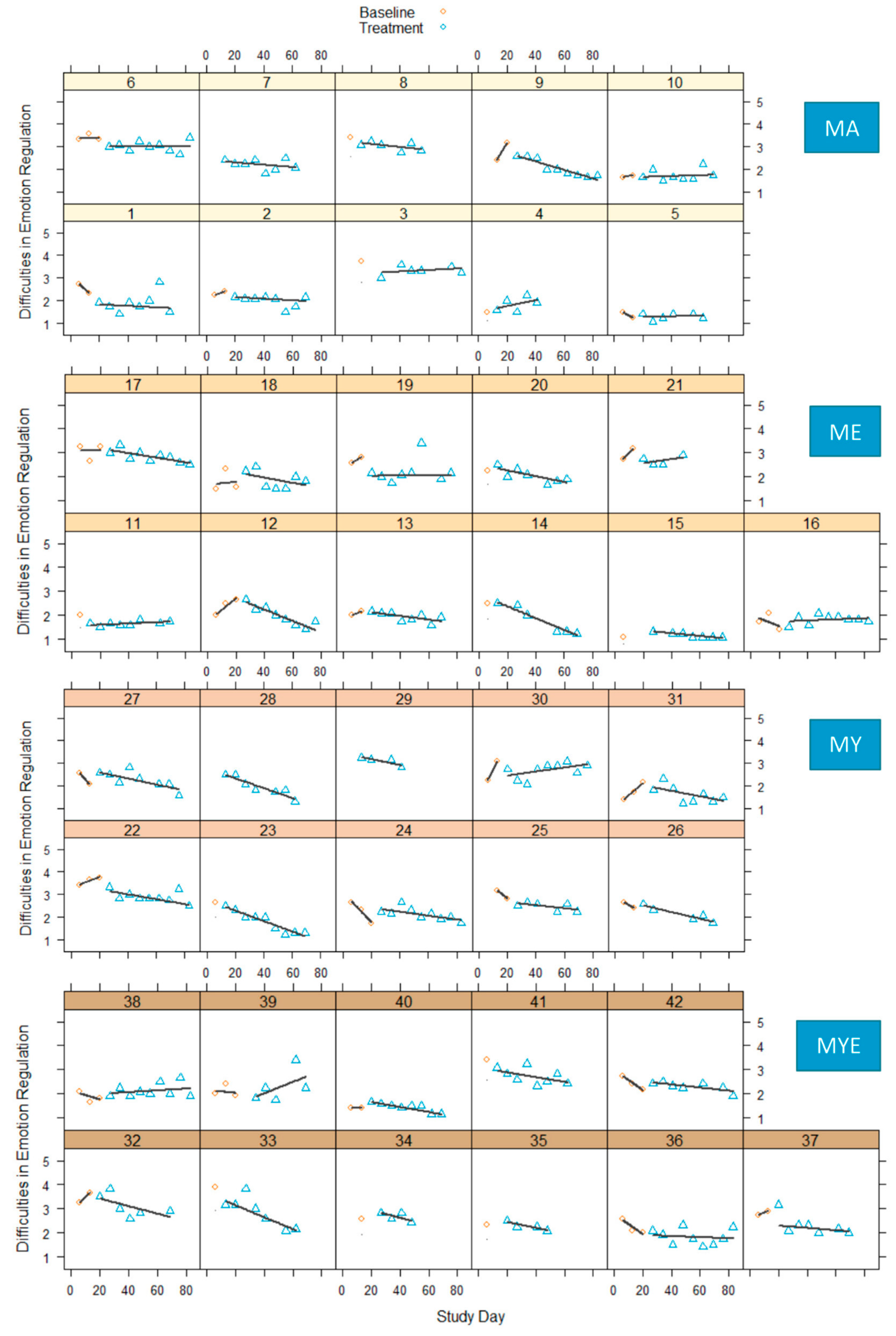
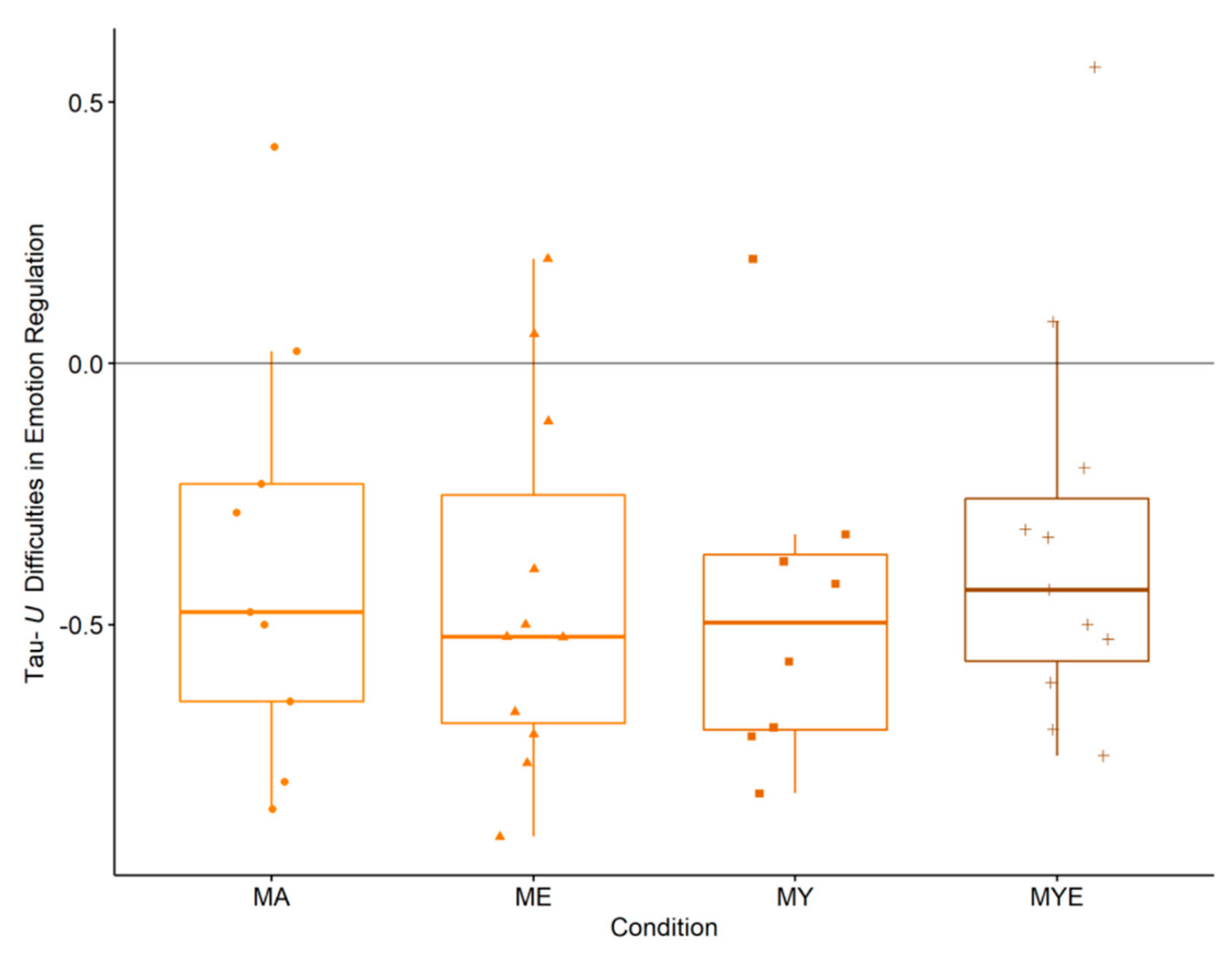
3.2. Emotion Regulation
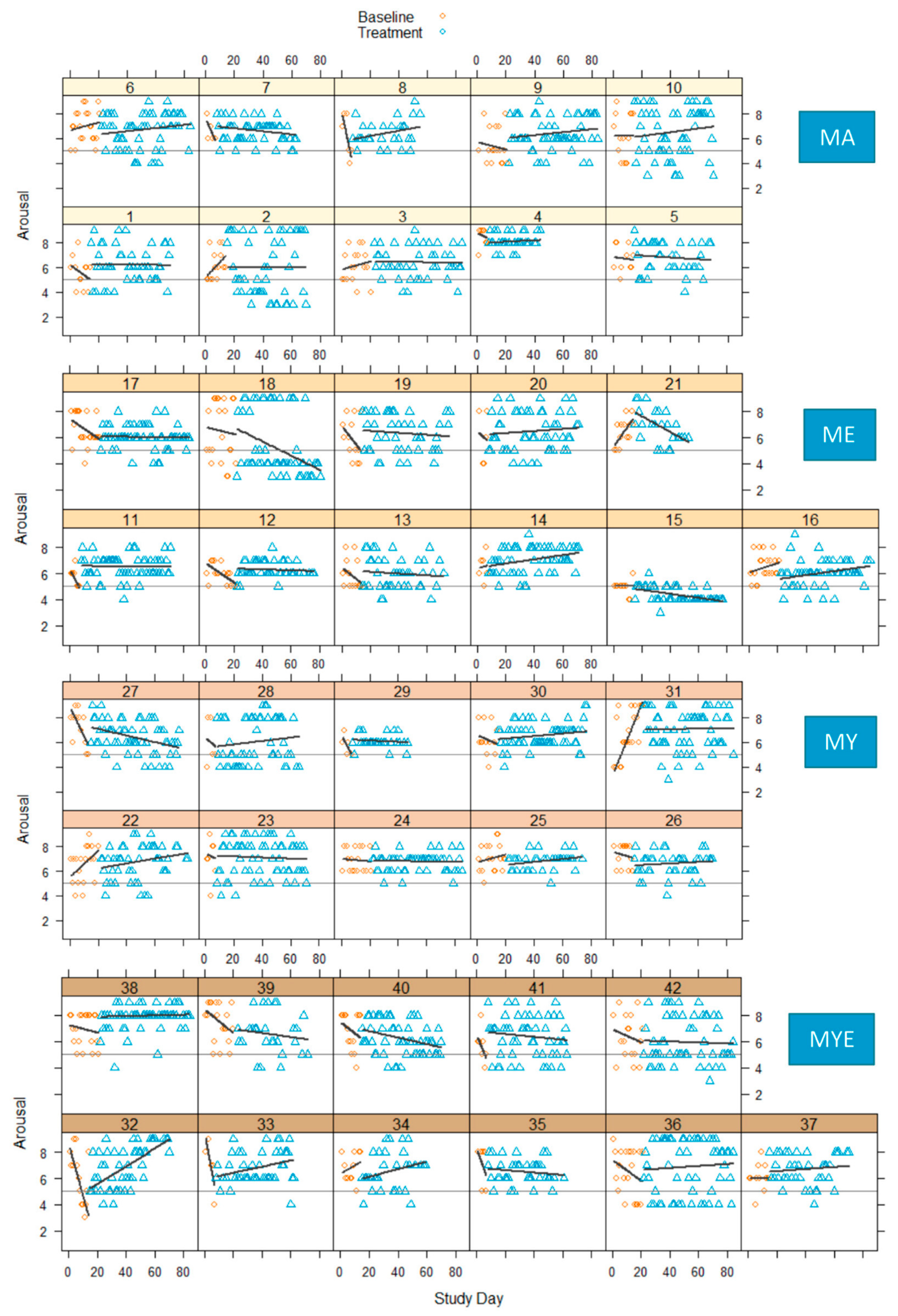
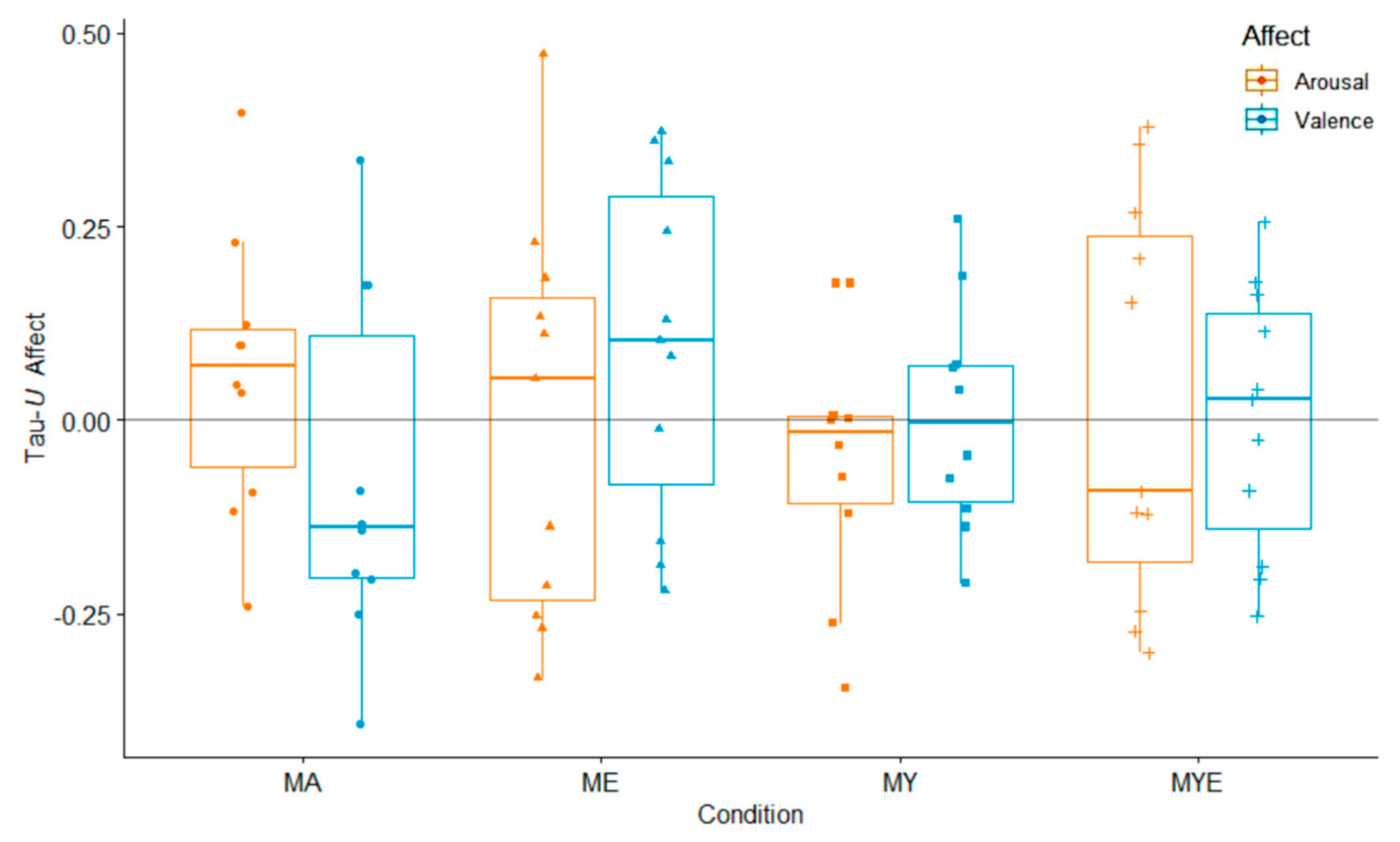
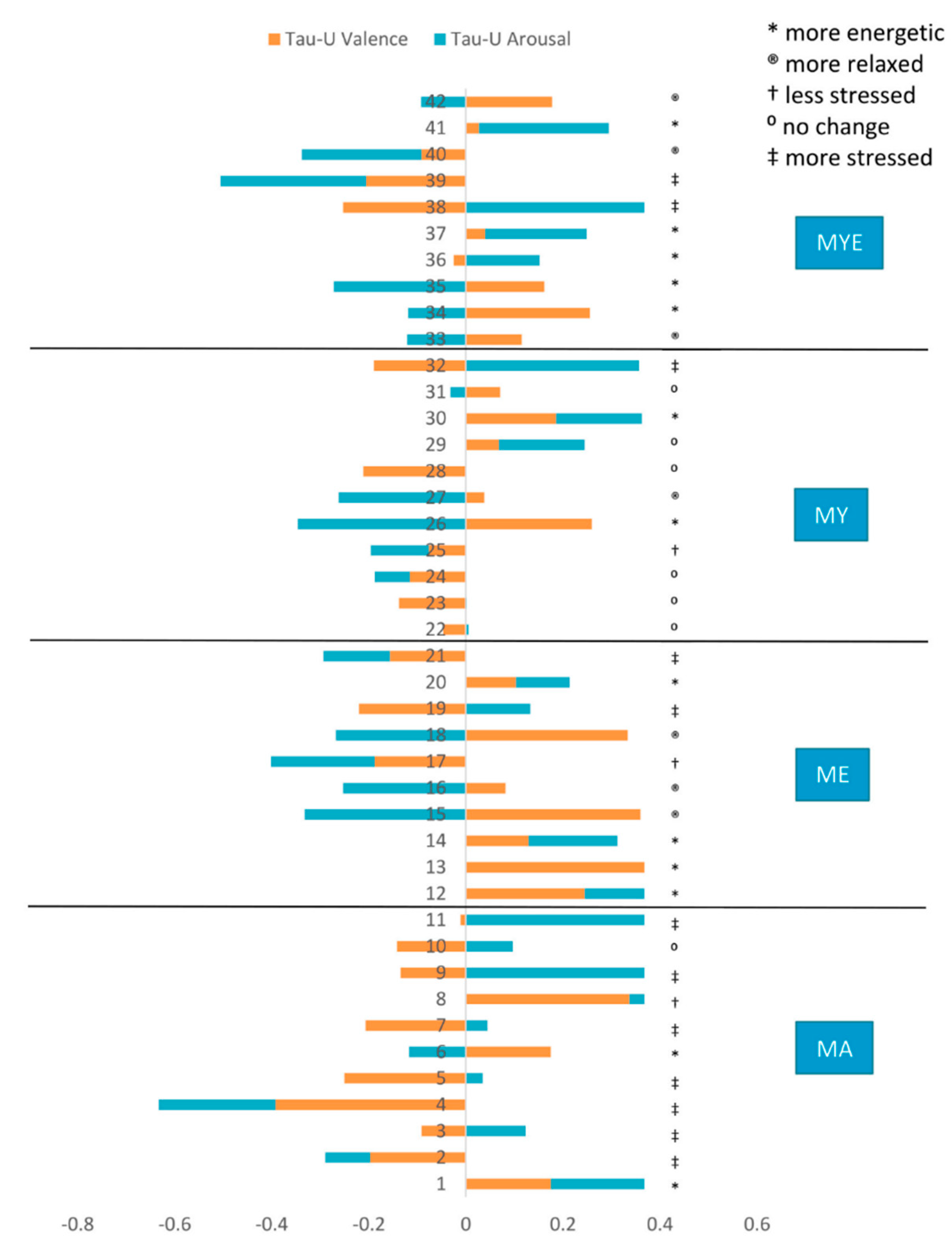
3.3. Affectivity
3.4. Relations between Affectivity, Body Awareness, and Emotion Regulation
3.5. Distress Tolerance
3.6. Self-Compassion
3.7. Changes in Home Practice
3.8. Selected Cases
4. Discussion
4.1. Mantra Meditation Might Be the Driving Force behind Subjective Improvements
4.2. Adding Yoga Components to Meditation Enhances Positive Affect
4.3. Body Awareness and Emotion Regulation Are Central Mechanisms
5. Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sullivan, M.B.; Moonaz, S.; Weber, K.; Taylor, J.N.; Schmalzl, L. Toward an Explanatory Framework for Yoga Therapy Informed by Philosophical and Ethical Perspectives. Altern. Ther. Health Med. 2017, 24, 38–47. [Google Scholar]
- Niedenthal, P.M.; Barsalou, L.W.; Winkielman, P.; Krauth-Gruber, S.; Ric, F. Embodiment in attitudes, social perception, and emotion. Personal Soc. Psychol. Rev. 2005, 9, 184–211. [Google Scholar] [CrossRef] [PubMed]
- Varela, F.J.; Thompson, E.; Rosch, E. The Embodied Mind: Cognitive Science and Human Experience; revised edition; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Winkielman, P.; Niedenthal, P.; Wielgosz, J.; Eelen, J.; Kavanagh, L.C. Embodiment of cognition and emotion. APA Handb. Personal. Soc. Psychol. 2015, 1, 151–175. [Google Scholar] [CrossRef]
- Hefferon, K. The Role of Embodiment in Optimal Functioning. In Positive Psychology in Practice: Promoting Human Flourishing in Work, Health, Education, and Everyday Life, 2nd ed.; Wiley: Hoboken, NJ, USA, 2015; pp. 789–806. [Google Scholar]
- Impett, E.A.; Daubenmier, J.J.; Hirschman, A.L. Minding the body: Yoga, embodiment, and well-being. Sex. Res. Soc. Policy 2006, 3, 39–48. [Google Scholar] [CrossRef]
- Francis, A.L.; Beemer, R.C. How does yoga reduce stress? Embodied cognition and emotion high-light the influence of the mus-culoskeletal system. Complement. Ther. Med. 2019, 43, 170–175. [Google Scholar] [CrossRef]
- Gard, T.; Noggle, J.J.; Park, C.L.; Vago, D.R.; Wilson, A. Potential self-regulatory mechanisms of yoga for psychological health. Front. Hum. Neurosci. 2014, 8, 770. [Google Scholar] [CrossRef]
- Schmalzl, L.; Powers, C.; Henje Blom, E. Neurophysiological and neurocognitive mechanisms underlying the effects of yoga-based practices: Towards a comprehensive theoretical frame-work. Front Hum. Neurosci. 2015, 9, 235. [Google Scholar] [CrossRef]
- Mehling, W.E.; Wrubel, J.; Daubenmier, J.J.; Price, C.J.; Kerr, C.E.; Silow, T.; Gopisetty, V.; Stewart, A.L. Body Awareness: A phenomenological inquiry into the common ground of mind-body therapies. Philos. Ethic-Humanit. Med. 2011, 6, 6. [Google Scholar] [CrossRef]
- Feuerstein, G. The Yoga Tradition: Its History, Literature, Philosophy and Practice, 3rd ed.; Hohm Press: Prescott, AZ, USA, 2012. [Google Scholar]
- Bringmann, H.C.; Sedlmeier, P. Effects of Different Components of Yoga: A Meta-Synthesis. OBM Integr. Complement. Med. 2021, 6, 1. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Dobos, G. Characteristics of randomized controlled trials of yoga: A bibliometric analysis. BMC Complement. Altern. Med. 2014, 14, 1–20. [Google Scholar] [CrossRef]
- Gallagher, S. Interpretations of Embodied Cognition. In The Implications of Embodiment: Cognition and Communication; Imprint Academic: Charlottesville, VA, USA, 2011; pp. 59–71. [Google Scholar]
- Niedenthal, P.M.; Maringer, M. Embodied Emotion Considered. Emot. Rev. 2009, 1, 122–128. [Google Scholar] [CrossRef]
- Pollatos, O.; Ferentzi, E. Embodiment of Emotion Regulation. In Emobiment in Psychotherapy; Springer: Berlin/Heidelberg, Germany, 2018; pp. 43–55. [Google Scholar]
- Khoury, B. Compassion: Embodied and Embedded. Mindfulness 2019, 10, 2363–2374. [Google Scholar] [CrossRef]
- Francis, A.L. The Embodied Theory of Stress: A Constructionist Perspective on the Experience of Stress. Rev. Gen. Psychol. 2018, 22, 398–405. [Google Scholar] [CrossRef]
- Fuchs, T.; Schlimme, J.E. Embodiment and psychopathology: A phenomenological perspective. Curr. Opin. Psychiatry 2009, 22, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; Muñoz, R.F. Emotion regulation and mental health. Clin. Psychol. Sci. Pract. 1995, 2, 151–164. [Google Scholar] [CrossRef]
- Phillips, M.L.; Drevets, W.C.; Rauch, S.L.; Lane, R. Neurobiology of emotion perception II: Implications for major psychiatric disorders. Biol. Psychiatry 2003, 54, 515–528. [Google Scholar] [CrossRef]
- MacBeth, A.; Gumley, A. Exploring compassion: A meta-analysis of the association between self-compassion and psycho-pathology. Clin. Psychol. Rev. 2012, 32, 545–552. [Google Scholar] [CrossRef]
- Zvolensky, M.J.; Bernstein, A.; Vujanovic, A.A. Distress Tolerance: Theory, Research, and Clinical Applications; Guilford Press: New York, NY, USA, 2011; p. 305p. [Google Scholar]
- Medina, J.; Hopkins, L.; Powers, M.; Baird, S.O.; Smits, J. The Effects of a Hatha Yoga Intervention on Facets of Distress Tolerance. Cogn. Behav. Ther. 2015, 44, 288–300. [Google Scholar] [CrossRef]
- Riley, K.E.; Park, C.L. How does yoga reduce stress? A systematic review of mechanisms of change and guide to future inquiry. Heal. Psychol. Rev. 2015, 9, 379–396. [Google Scholar] [CrossRef]
- Mehling, W.E.; Gopisetty, V.; Daubenmier, J.; Price, C.J.; Hecht, F.M.; Stewart, A. Body Awareness: Construct and Self-Report Measures. PLoS ONE 2009, 4, e5614. [Google Scholar] [CrossRef]
- Bechara, A.; Naqvi, N. Listening to your heart: Interoceptive awareness as a gateway to feeling. Nat. Neurosci. 2004, 7, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Damasio, A.R. Descartes’ Error: Emotion, Reason, and the Human Brain; Random House: London, UK, 2006. [Google Scholar]
- Füstös, J.; Gramann, K.; Herbert, B.; Pollatos, O. On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Soc. Cogn. Affect. Neurosci. 2012, 8, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Price, C.J.; Hooven, C. Interoceptive Awareness Skills for Emotion Regulation: Theory and Approach of Mindful Awareness in Body-Oriented Therapy (MABT). Front. Psychol. 2018, 9, 798. [Google Scholar] [CrossRef] [PubMed]
- Sze, J.A.; Gyurak, A.; Yuan, J.W.; Levenson, R.W. Coherence between emotional experience and physiology: Does body awareness training have an impact? Emotion 2010, 10, 803–814. [Google Scholar] [CrossRef]
- Ochsner, K.N.; Gross, J.J. The cognitive control of emotion. Trends Cogn. Sci. 2005, 9, 242–249. [Google Scholar] [CrossRef]
- Chambers, R.; Gullone, E.; Allen, N.B. Mindful emotion regulation: An integrative review. Clin. Psychol. Rev. 2009, 29, 560–572. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A.; Jakobsen, J.C. Mindfulness: Top–down or bottom–up emotion regulation strategy? Clin. Psychol. Rev. 2013, 33, 82–96. [Google Scholar] [CrossRef]
- Park, C.L.; Riley, K.E.; Braun, T.D.; Jung, J.Y.; Suh, H.G.; Pescatello, L.S.; Antoni, M.H. Yoga and Cognitive-behavioral Interventions to Reduce Stress in Incoming College Students: A Pilot Study. J. Appl. Biobehav. Res. 2017, 22, e12068. [Google Scholar] [CrossRef]
- Sauer-Zavala, S.E.; Walsh, E.C.; Eisenlohr-Moul, T.A.; Lykins, E.L.B. Comparing Mindfulness-Based Intervention Strategies: Differential Effects of Sitting Meditation, Body Scan, and Mindful Yoga. Mindfulness 2012, 4, 383–388. [Google Scholar] [CrossRef]
- Kok, B.E.; Singer, T. Phenomenological fingerprints of four meditations: Differential state changes in affect, mind-wandering, meta-cognition, and interoception before and after daily practice across 9 months of training. Mindfulness 2017, 8, 218–231. [Google Scholar] [CrossRef]
- Daubenmier, J.; Mehling, W.; Price, C.; Bartmess-Levasseur, E.; Acree, M.; Stewart, A. OA14.02. Exploration of body awareness and pain and emotion regulation among yoga and meditation practitioners: Does type of mind-body practice matter? BMC Com-Plement Altern. Med. 2012, 12, O54. [Google Scholar] [CrossRef]
- Gard, T.; Brach, N.; Hölzel, B.K.; Noggle, J.J.; Conboy, L.A.; Lazar, S. Effects of a yoga-based intervention for young adults on quality of life and perceived stress: The potential mediating roles of mindfulness and self-compassion. J. Posit. Psychol. 2012, 7, 165–175. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G. Yoga for depression: A systematic review and me-ta-analysis. Depress. Anxiety 2013, 30, 1068–1083. [Google Scholar] [CrossRef] [PubMed]
- Kinser, P.A.; Robins, J.L. Control group design: Enhancing rigor in research of mind-body thera-pies for depression. Evid. Based Complement. Alternat. Med. 2013, 2013, e140467. [Google Scholar] [CrossRef]
- Lindsay, E.K.; Chin, B.; Greco, C.M.; Young, S.; Brown, K.W.; Wright, A.G.C.; Smyth, J.M.; Burkett, D.; Creswell, J.D. How mindfulness training promotes positive emotions: Dismantling acceptance skills training in two randomized controlled trials. J. Pers. Soc. Psychol. 2018, 115, 944–973. [Google Scholar] [CrossRef] [PubMed]
- May, C.J.; Weyker, J.R.; Spengel, S.K.; Finkler, L.J.; Hendrix, S.E. Tracking longitudinal changes in affect and mindfulness caused by concentration and loving-kindness meditation with hierarchical linear modeling. Mindfulness 2014, 5, 249–258. [Google Scholar] [CrossRef]
- Bringmann, H.C.; Bringmann, N.; Jeitler, M.; Brunnhuber, S.; Michalsen, A.; Sedlmeier, P. Meditation-Based Lifestyle Modification: Development of an Integrative Mind-Body Program for Mental Health and Human Flourishing. Complement. Med. Res. 2020, 28, 252–262. [Google Scholar] [CrossRef]
- Barlow, D.H.; Nock, M.; Hersen, M. Single Case Experimental Designs: Strategies for Studying Behavior for Change, 3rd ed.; Pearson: Boston, MA, USA, 2009. [Google Scholar]
- Menezes, C.B.; Dalpiaz, N.R.; Kiesow, L.G.; Sperb, W.; Hertzberg, J.; Oliveira, A.A. Yoga and emotion regulation: A review of primary psychological outcomes and their physiological correlates. Psychol. Neurosci. 2015, 8, 82–101. [Google Scholar] [CrossRef]
- Matko, K.; Sedlmeier, P.; Bringmann, H.C. Differential effects of ethical education, physical Hatha yoga, and mantra meditation on well-being and stress in healthy participants—An experimental single-case study. Front Psychol. 2021, 12, 672301. [Google Scholar] [CrossRef]
- Matko, K.; Berghöfer, A.; Jeitler, M.; Sedlmeier, P.; Bringmann, H.C. Who Benefits Most? Interactions between Personality Traits and Outcomes of Four Incremental Meditation and Yoga Treatments. J. Clin. Med. 2022, 11, 4553. [Google Scholar] [CrossRef]
- Leiner, D.J. SoSci Survey. 2019. Available online: https://www.soscisurvey.de (accessed on 31 May 2021).
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef]
- Miller, L.C.; Murphy, R.; Buss, A.H. Consciousness of body: Private and public. J. Pers. Soc. Psychol. 1981, 41, 397–406. [Google Scholar] [CrossRef]
- Shields, S.A.; Mallory, M.E.; Simon, A. The Body Awareness Questionnaire: Reliability and Validity. J. Pers. Assess. 1989, 53, 802–815. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2003, 26, 41–54. [Google Scholar] [CrossRef]
- Russell, J.A.; Weiss, A.; Mendelsohn, G.A. Affect grid: A Singleitem Scale of Pleasure and Arousal. J. Pers. Soc. Psychol. 1989, 57, 493–502. [Google Scholar] [CrossRef]
- Killgore, W.D.S. The Affect Grid: A Moderately Valid, Nonspecific Measure of Pleasure and Arousal. Psychol. Rep. 1998, 83, 639–642. [Google Scholar] [CrossRef]
- Simons, J.S.; Gaher, R.M. The Distress Tolerance Scale: Development and Validation of a Self-Report Measure. Motiv. Emot. 2005, 29, 83–102. [Google Scholar] [CrossRef]
- Hupfeld, J.; Ruffieux, N. Validierung einer deutschen Version der Self-Compassion Scale (SCS-D). Z Für Klin. Psychol. Psychother. 2011, 40, 115–123. [Google Scholar] [CrossRef]
- Machalicek, W.; Horner, R.H. Special Issue on Advances in Single-Case Research Design and Analysis. Dev. Neurorehabilit. 2018, 21, 209–211. [Google Scholar] [CrossRef]
- Shadish, W.R. Analysis and meta-analysis of single-case designs: An introduction. J. Sch. Psychol. 2014, 52, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.D.; Gast, D.L. Visual analysis in single case experimental design studies: Brief review and guidelines. Neuropsychol. Rehabilitat. 2013, 24, 445–463. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.I.; Vannest, K.J.; Davis, J.L.; Sauber, S.B. Combining Nonoverlap and Trend for Single-Case Research: Tau-U. Behav. Ther. 2011, 42, 284–299. [Google Scholar] [CrossRef]
- Solomon, B.G.; Howard, T.K.; Stein, B.L. Critical Assumptions and Distribution Features Pertaining to Contemporary Single-Case Effect Sizes. J. Behav. Educ. 2015, 24, 438–458. [Google Scholar] [CrossRef]
- Dedrick, R.F.; Ferron, J.M.; Hess, M.R.; Hogarty, K.Y.; Kromrey, J.D.; Lang, T.R.; Niles, J.D.; Lee, R.S. Multilevel Modeling: A Review of Methodological Issues and Applications. Rev. Educ. Res. 2009, 79, 69–102. [Google Scholar] [CrossRef]
- Hox, J.J. Multilevel Analysis: Techniques and Applications, 2nd ed.; Quantitative methodology series; Routledge: New York, NY, USA, 2010; 382p. [Google Scholar]
- Nakagawa, S.; Schielzeth, H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Methods. Ecol Evol. 2013, 4, 133–142. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: https://www.R-project.org/ (accessed on 19 April 2022).
- Sarkar, D. Lattice: Multivariate Data Visualization with R.; Springer: New York, NY, USA, 2008; Available online: http://lmdvr.r-forge.r-project.org (accessed on 17 June 2021).
- Kassambara, A. ggpubr: ‘ggplot2’ Based Publication Ready Plots. R Package Version 0.2.5. 2019. Available online: https://CRAN.R-project.org/package=ggpubr (accessed on 3 December 2020).
- Wilbert, J.; Lueke, T. Scan: Single-Case Data Analyses for Single and Multiple Baseline Designs. 2021. Available online: https://CRAN.R-project.org/package=scan (accessed on 30 May 2022).
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D.; Team, R.C. nlme: Linear and Nonlinear Mixed Effects Models. R Package Version 3.1-120. 2015. Available online: https://CRAN.R-project.org/package=nlme (accessed on 11 February 2021).
- Titz, J. mimosa: A modern graphical user interface for 2-level mixed models. J. Open Source Softw. 2020, 5, 2116. [Google Scholar] [CrossRef]
- Stein, E.; Witkiewitz, K. Dismantling mindfulness-based programs: A systematic review to identify active components of treat-ment. Mindfulness 2020, 11, 2470–2485. [Google Scholar] [CrossRef]
- Lynch, J.; Prihodova, L.; Dunne, P.J.; Carroll, A.; Walsh, C.; McMahon, G.; White, B. Mantra meditation for mental health in the general population: A systematic review. Eur. J. Integr. Med. 2018, 23, 101–108. [Google Scholar] [CrossRef]
- Sedlmeier, P.; Eberth, J.; Schwarz, M.; Zimmermann, D.; Haarig, F.; Jaeger, S.; Kunze, S. The psychological effects of meditation: A meta-analysis. Psychol. Bull. 2012, 138, 1139–1171. [Google Scholar] [CrossRef]
- Bryant, E.F. The Yoga Sutras of Patañjali: A New Edition, Translation and Commentary; Farrar, Straus and Giroux: New York, NY, USA, 2015; 780p. [Google Scholar]
- Farb, N.; Daubenmier, J.; Price, C.J.; Gard, T.; Kerr, C.; Dunn, B.D.; Klein, A.C.; Paulus, M.P.; Mehling, W.E. Interoception, contemplative practice, and health. Front Psychol. 2015, 6, 763. [Google Scholar] [CrossRef] [PubMed]
- Gibson, J. Mindfulness, Interoception, and the Body: A Contemporary Perspective. Front. Psychol. 2019, 10, 2012. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.C.; Dixon, M.L.; Nijeboer, S.; Girn, M.; Floman, J.L.; Lifshitz, M.; Ellamil, M.; Sedlmeier, P.; Christoff, K. Functional neuroanatomy of meditation: A review and meta-analysis of 78 functional neuroimaging investigations. Neurosci. Biobehav. Rev. 2016, 65, 208–228. [Google Scholar] [CrossRef]
- Weinstabl, J. Der Einfluss unterschiedlicher Meditationsarten auf Körperwahrnehmung und Emotionsregulation. Master’s Thesis, Chemnitz University of Technology, Chemnitz, Germany, 2020. [Google Scholar]
- Matko, K.; Sedlmeier, P. What Is Meditation? Proposing an Empirically Derived Classification System. Front. Psychol. 2019, 10, 2276. [Google Scholar] [CrossRef]
- Lindahl, J.R.; Kaplan, C.T.; Winget, E.M.; Britton, W.B. A Phenomenology of Meditation-Induced Light Experiences: Traditional Buddhist and Neurobiological Perspectives. Front Psychol. 2014, 4, 973. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, D.M.; Lewis, E.; Payne, J.; Wilson, L. A qualitative analysis of sensory phenomena induced by perceptual deprivation. Phenomenol. Cogn. Sci. 2011, 11, 95–112. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action from a Conceptual and Neural Perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef] [PubMed]
- Bayot, M.; Vermeulen, N.; Kever, A.; Mikolajczak, M. Mindfulness and Empathy: Differential Effects of Explicit and Implicit Buddhist Teachings. Mindfulness 2018, 11, 5–17. [Google Scholar] [CrossRef]
- Smith, J.A.; Greer, T.; Sheets, T.; Watson, S. Is there more to yoga than exercise? Altern. Ther. Health Med. 2011, 17, 22–29. [Google Scholar]
- Cramer, H.; Sellin, C.; Schumann, D.; Dobos, G. Yoga in Arterial Hypertension. Dtsch. Arztebl. Int. 2018, 115, 833–839. [Google Scholar] [CrossRef]
- Stulz, N.; Lutz, W.; Leach, C.; Lucock, M.; Barkham, M. Shapes of early change in psychotherapy under routine outpatient conditions. J. Consult. Clin. Psychol. 2007, 75, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Belzer, F.; Schmidt, S.; Lucius-Hoene, G.; Schneider, J.F.; Orellana-Rios, C.L.; Sauer, S. Challenging the Construct Validity of Mindfulness Assessment—a Cognitive Interview Study of the Freiburg Mindfulness Inventory. Mindfulness 2012, 4, 33–44. [Google Scholar] [CrossRef]
- Krägeloh, C.U.; Bergomi, C.; Siegert, R.J.; Medvedev, O.N. Response Shift After a Mindfulness-Based Intervention: Measurement Invariance Testing of the Comprehensive Inventory of Mindfulness Experiences. Mindfulness 2017, 9, 212–220. [Google Scholar] [CrossRef]
- Kaufman, E.; Xia, M.; Fosco, G.; Yaptangco, M.; Skidmore, C.R.; Crowell, S.E. The Difficulties in Emotion Regulation Scale Short Form (DERS-SF): Validation and Replication in Adolescent and Adult Samples. J. Psychopathol. Behav. Assess. 2015, 38, 443–455. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2010, 18, 250–255. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Ann. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Hunt, M.; Al-Braiki, F.; Dailey, S.; Russell, R.; Simon, K. Mindfulness Training, Yoga, or Both? Dismantling the Active Components of a Mindfulness-Based Stress Reduction Intervention. Mindfulness 2017, 9, 512–520. [Google Scholar] [CrossRef]
- Tang, R.; Braver, T.S. Towards an individual differences perspective in mindfulness training re-search: Theoretical and empirical considerations. Front Psychol. 2020, 11, 818. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meditation | Physical Yoga | Ethical Practice | |||
|---|---|---|---|---|---|
| n | Mdn (IQR) | Mdn (IQR) | Mdn (IQR) | ||
| Last month of treatment | 41 | 248 (231) | 230 (159) | 280 (160) | |
| 2-month follow-up | 40 | 80 (160) | 100 (343) | 40 (80) | |
| 12-month follow-up | 33 | 30 (40) | 80 (180) | 10 (60) | |
| MA | 9 | 30 (40) | 80 (150) | 0 (40) | |
| MY | 7 | 40 (35) | 70 (188) | 0 (10) | |
| ME | 8 | 30 (150) | 60 (225) | 130 (275) | |
| MYE | 9 | 20 (40) | 180 (150) | 20 (60) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matko, K.; Sedlmeier, P.; Bringmann, H.C. Embodied Cognition in Meditation, Yoga, and Ethics—An Experimental Single-Case Study on the Differential Effects of Four Mind–Body Treatments. Int. J. Environ. Res. Public Health 2022, 19, 11734. https://doi.org/10.3390/ijerph191811734
Matko K, Sedlmeier P, Bringmann HC. Embodied Cognition in Meditation, Yoga, and Ethics—An Experimental Single-Case Study on the Differential Effects of Four Mind–Body Treatments. International Journal of Environmental Research and Public Health. 2022; 19(18):11734. https://doi.org/10.3390/ijerph191811734
Chicago/Turabian StyleMatko, Karin, Peter Sedlmeier, and Holger C. Bringmann. 2022. "Embodied Cognition in Meditation, Yoga, and Ethics—An Experimental Single-Case Study on the Differential Effects of Four Mind–Body Treatments" International Journal of Environmental Research and Public Health 19, no. 18: 11734. https://doi.org/10.3390/ijerph191811734
APA StyleMatko, K., Sedlmeier, P., & Bringmann, H. C. (2022). Embodied Cognition in Meditation, Yoga, and Ethics—An Experimental Single-Case Study on the Differential Effects of Four Mind–Body Treatments. International Journal of Environmental Research and Public Health, 19(18), 11734. https://doi.org/10.3390/ijerph191811734