

Perception of Realism and Acquisition of Clinical Skills in Simulated Pediatric Dentistry Scenarios



Abstract
1. Introduction
2. Materials and Methods
2.1. Student Sample
2.2. Teacher Sample
2.3. Statistical Methods
3. Results
3.1. Student Evaluation
3.2. Teacher Evaluation
3.3. Comparison between Students and Teachers
3.4. Connection between Students’ Perception of Competence and Realisms Perceived by Students and Teachers
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smink, D.S.; Yule, S.J.; Ashley, S.W. Realism in simulation: How much is enough? JAMA Surg. 2017, 152, 825–826. [Google Scholar] [CrossRef]
- Quilici, A.P.; Bicudo, A.M.; Gianotto-Oliveira, R.; Timerman, S.; Gutierrez, F.; Abrao, K.C. Faculty perceptions of simulation programs in healthcare education. Int. J. Med. Educ. 2015, 6, 166–171. [Google Scholar] [CrossRef]
- Carey, J.M.; Rossler, K. The how when why of high-fidelity simulation. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 8 May 2022. [Google Scholar]
- Conlon, M.M.; McIntosh, G.L. Perceptions of realism in digital scenarios: A mixed methods descriptive study. Nurse Educ. Pract. 2020, 46, 102794. [Google Scholar] [CrossRef]
- Dalwood, N.; Maloney, S.; Cox, N.; Morgan, P. Preparing physiotherapy students for clinical placement student perceptions of low-cost peer simulation. A mixed-methods study. Simul. Healthc. 2018, 13, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Tufts, L.M.; Hensley, C.A.; Frazier, M.D.; Hossino, D.; Domanico, R.S.; Harris, J.K.; Flesher, S.L. Utilizing high-fidelity simulators in improving trainee confidence and competency in code management. Pediatr. Qual. Saf. 2021, 6, e496. [Google Scholar] [CrossRef]
- Lubbers, J.; Rossman, C. Satisfaction and self-confidence with nursing clinical simulation: Novice learners, medium-fidelity, and community settings. Nurse Educ. Today 2017, 48, 140–144. [Google Scholar] [CrossRef]
- Stokes-Parish, J.; Duvivier, R.; Jolly, B. Expert opinions on the authenticity of moulage in simulation: A Delphi study. Adv. Simul. 2019, 4, 16. [Google Scholar] [CrossRef]
- Engström, H.; Hagiwara, M.A.; Backlund, P.; Lebram, M.; Lundberg, L.; Johannesson, M.; Sterner, A.; Söderholm, H.M. The impact of contextualization on immersion in healthcare simulation. Adv. Simul. 2016, 1, 8. [Google Scholar] [CrossRef]
- Hadfield, A.; Thompson, S.; Hall, J.; Diaz-Navarro, C. Perception of simulation training in emergencies for dental sedation practitioners. Clin. Teach. 2018, 15, 52–56. [Google Scholar] [CrossRef]
- Adams, T.; Newton, C.; Patel, H.; Sulistio, M.; Tomlinson, A.; Lee, W. Resident versus faculty member simulation debriefing. Clin. Teach. 2018, 15, 462–466. [Google Scholar] [CrossRef]
- Cooper, D.D.; Wilson, A.B.; Huffman, G.N.; Humbert, A.J. Medical students’ perception of residents as teachers: Comparing effectiveness of residents and faculty during simulation de-briefings. J. Grad. Med. Educ. 2012, 4, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Aljahany, M.; Malaekah, H.; Alzahrani, H.; Alhamadah, F.; Dator, W.L. Simulation-based peer-assisted learning: Perceptions of health science students. Adv. Med. Educ. Pract. 2021, 12, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Meerdink, M.; Khan, J. Comparison of the use of manikins and simulated patients in a multidisciplinary in situ medical simulation program for healthcare professionals in the United Kingdom. J. Educ. Eval. Health Prof. 2021, 18, 8. [Google Scholar] [CrossRef]
- Alsaad, A.A.; Davuluri, S.; Bhide, V.Y.; Lannen, A.M.; Maniaci, M.J. Assessing the performance and satisfaction of medical residents utilizing standardized patient versus mannequin-simulated training. Adv. Med. Educ. Pract. 2017, 8, 481–486. [Google Scholar] [CrossRef]
- Singh, D.; Kojima, T.; Gurnaney, H.; Deutsch, E.S. Do fellows and faculty share the same perception of simulation fidelity? A pilot study. Simul. Healthc. 2020, 15, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Warren, J.N.; Luctkar-Flude, M.; Godfrey, C.; Lukewich, J. A systematic review of the effectiveness of simulation-based education on satisfaction and learning outcomes in nurse practitioner programs. Nurse Educ. Today 2016, 46, 99–108. [Google Scholar] [CrossRef]
- Elshama, S.S. How to Use Moulage as a Simulation Tool in Medical Education? Iberoam. J. Med. 2020, 2, 219–222. [Google Scholar] [CrossRef]
- Stokes-Parish, J.B.; Duvivier, R.; Jolly, B. How does moulage contribute to medical students’ perceived engagement in simulation? A mixed-methods pilot study. Adv. Simul. 2020, 5, 23. [Google Scholar] [CrossRef]
- Backlund, P.; Söderholm, H.M.; Engström, H.; Hagiwara, M.A.; Lebram, M. Breaking out of the bubble putting simulation into context to increase immersion and performance. Simul. Gaming 2018, 49, 642–660. [Google Scholar] [CrossRef]
- Graham, A.C.; McAleer, S. An overview of realist evaluation for simulation-based education. Adv. Simul. 2018, 3, 13. [Google Scholar] [CrossRef]
- Hagiwara, M.A.; Backlund, P.; Hanna Söderholm, H.M.; Lundberg, L.; Lebram, M.; Engström, H. Measuring participants’ immersion in healthcare simulation: The development of an instrument. Adv. Simul. 2016, 1, 17. [Google Scholar] [CrossRef] [PubMed]
- Coro-Montante, G.; Pardo Monedero, M.J.; De la Hoz Calvo, A.; Sánchez Ituarte, J.; Oliva Fernández, O.; Inouye, S.L. ProRealSim v1.0. Tool to Calculate the Realism Index Obtained in Clinical Simulation Scenarios in Physical Environments [Internet]; Universidad Europea: Madrid, Spain, 2021; Available online: https://prorealsim.universidadeuropea.com (accessed on 20 April 2022).
- Kim, M.J.; Kang, H.S.; De Gagne, J.C. Nursing students’ perceptions and experiences of using virtual simulation during the COVID-19 pandemic. Clin. Simul. Nurs. 2021, 60, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Abu Dabrh, A.M.; Waller, T.A.; Bonacci, R.P.; Nawaz, A.J.; Keith, J.J.; Agarwal, A.; Merfeld, J.; Nordin, T.; Winscott, M.M.; Belda, T.E.; et al. Professionalism and inter-communication skills (ICS): A multi-site validity study assessing proficiency in core competencies and milestones in medical learners. BMC Med. Educ. 2020, 20, 362. [Google Scholar] [CrossRef]
- Carrero-Planells, A.; Pol-Castañeda, S.; Alamillos-Guardiola, M.A.; Prieto-Alomar, A.; Tomás-Sánchez, M.; Moreno-Mulet, C. Students and teachers’ satisfaction and perspectives on high-fidelity simulation for learning fundamental nursing procedures: A mixed-method study. Nurse Educ. Today 2021, 104, 104981. [Google Scholar] [CrossRef]
- Dafli, E.; Fountoukidis, I.; Hatzisevastou-Loukidou, C.; Bamidis, P.D. Curricular integration of virtual patients: A unifying perspective of medical teachers and students. BMC Med. Educ. 2019, 19, 416. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.; Hewett, D.G.; Jolly, B.C.; Janssen, S.; Beckmann, M.M. Is that realistic? The development of a realism assessment questionnaire and its application in appraising three simulators for a gynaecology procedure. Adv. Simul. 2018, 3, 21. [Google Scholar] [CrossRef]
- Piryani, R.M.; Piryani, S.; Shrestha, U.; Acharya, A.; Kanskar, S.; Shahi, M.; Kayastha, J.; Chaulagain, A.; Agarwal, J.P.; Bajracharya, S.R. Simulation-based education workshop: Perceptions of participants. Adv. Med. Educ. Pract. 2019, 10, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Roze, E.; Flamand-Roze, C.; Méneret, A.; Ruiz, M.; Le Liepvre, H.; Duguet, A.; Renaud, M.-C.; Alamowitch, S.; Steichen, O. ‘The Move’, an innovative simulation-based medical education program using roleplay to teach neurological semiology: Students’ and teachers’ perceptions. Rev. Neurol. 2016, 172, 289–294. [Google Scholar] [CrossRef]
- Cabañero-Martínez, M.J.; García-Sanjuán, S.; Escribano, S.; Fernández-Alcántara, M.; Martí-nez-Riera, J.R.; Juliá-Sanchís, R. Mixed-method study on the satisfaction of a high-fidelity simulation program in a sample of nursing-degree students. Nurse Educ. Today 2021, 100, 104858. [Google Scholar] [CrossRef] [PubMed]
- Hanshaw, S.L.; Dickerson, S.S. High fidelity simulation evaluation studies in nursing education: A review of the literature. Nurse Educ. Pract. 2020, 46, 102818. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Perception of Realism (Postscenario) |
|---|
| How realistic did you find the dental office? |
| How realistic did you find the girl patient manikin? |
| How realistic did the mother seem to you? |
| How realistic did everything seem to you, overall? |
| Perception of clinical competence (Posttest) |
| How capable do you feel, at this point, to perform behavioral management of a pediatric patient and their parents, and to diagnose and correctly treat a pulp therapy case in a real pediatric dentistry practice? |
| Perceived Realism of the Simulated Office | Perceived Realism of the Mannequin | Perceived Realism of the Simulated Participant | Perceived Global Realism | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Number of Scenarios | Media | Standard Deviation | p-Value | Mean | Standard Deviation | p-Value | Mean | Standard Deviation | p-Value | Mean | Standard Deviation | p-Value |
| 8 | 7.833 | 1.48 | 0.009502 (a) | 6.79 | 2.22 | 0.001456 | 8.99 | 1.28 | 0.7292 (a) | 8.15 | 1.22 | 0.009441 (a) |
| Mean | Standard Deviation | p-Value | |
|---|---|---|---|
| Perceived realism of the office | 5.81 | 0.43 | 1.54 × 10−32 (a) |
| Perceived realism of the mannequin | 4.25 | 0.45 | 1.54 × 10−32 (a) |
| Perceived realism of the participant | 7.49 | 1.13 | 1.54 × 10−32 (a) |
| Global perceived realism | 6.34 | 0.64 | 1.54 × 10−32 (a) |
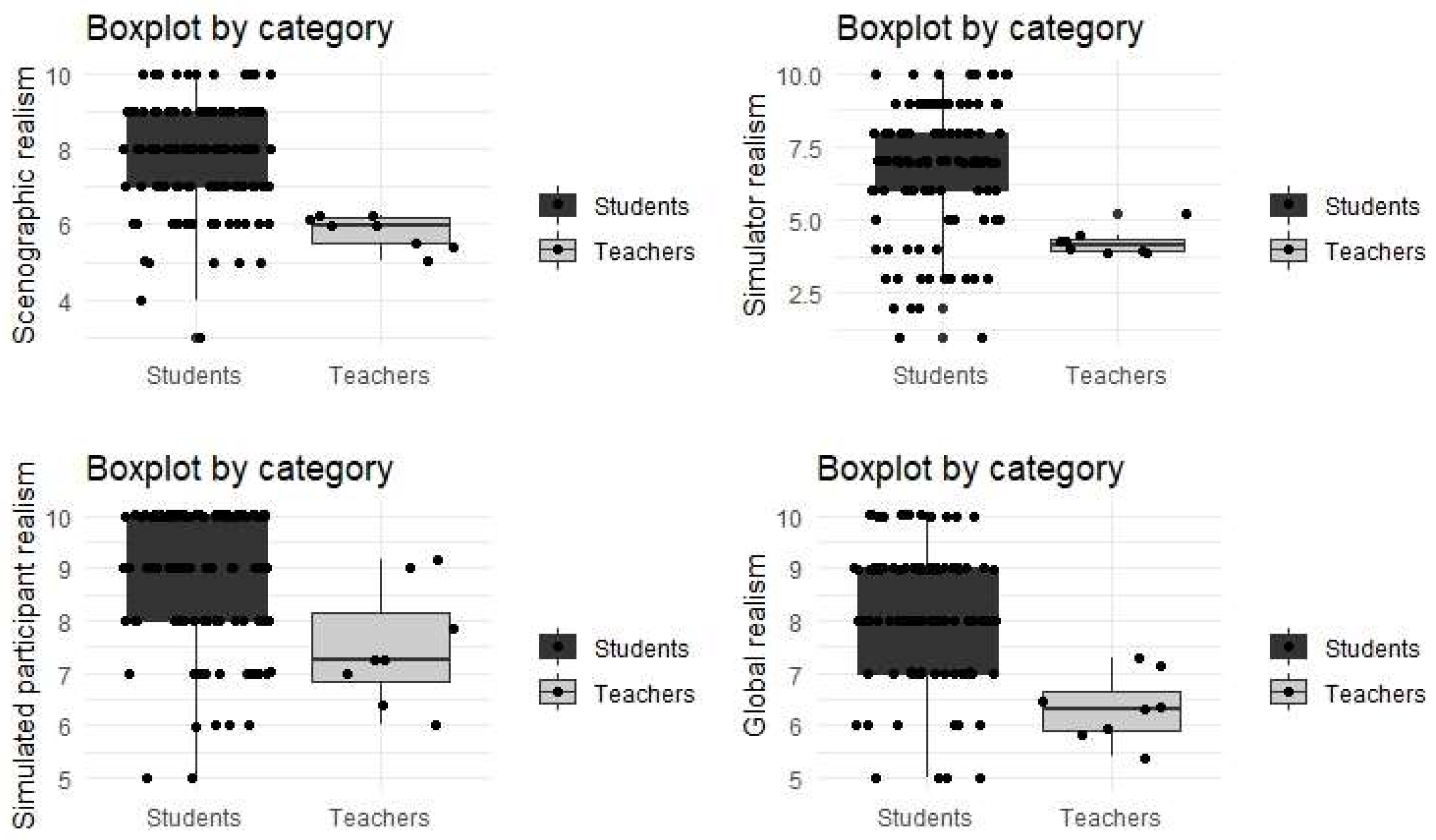
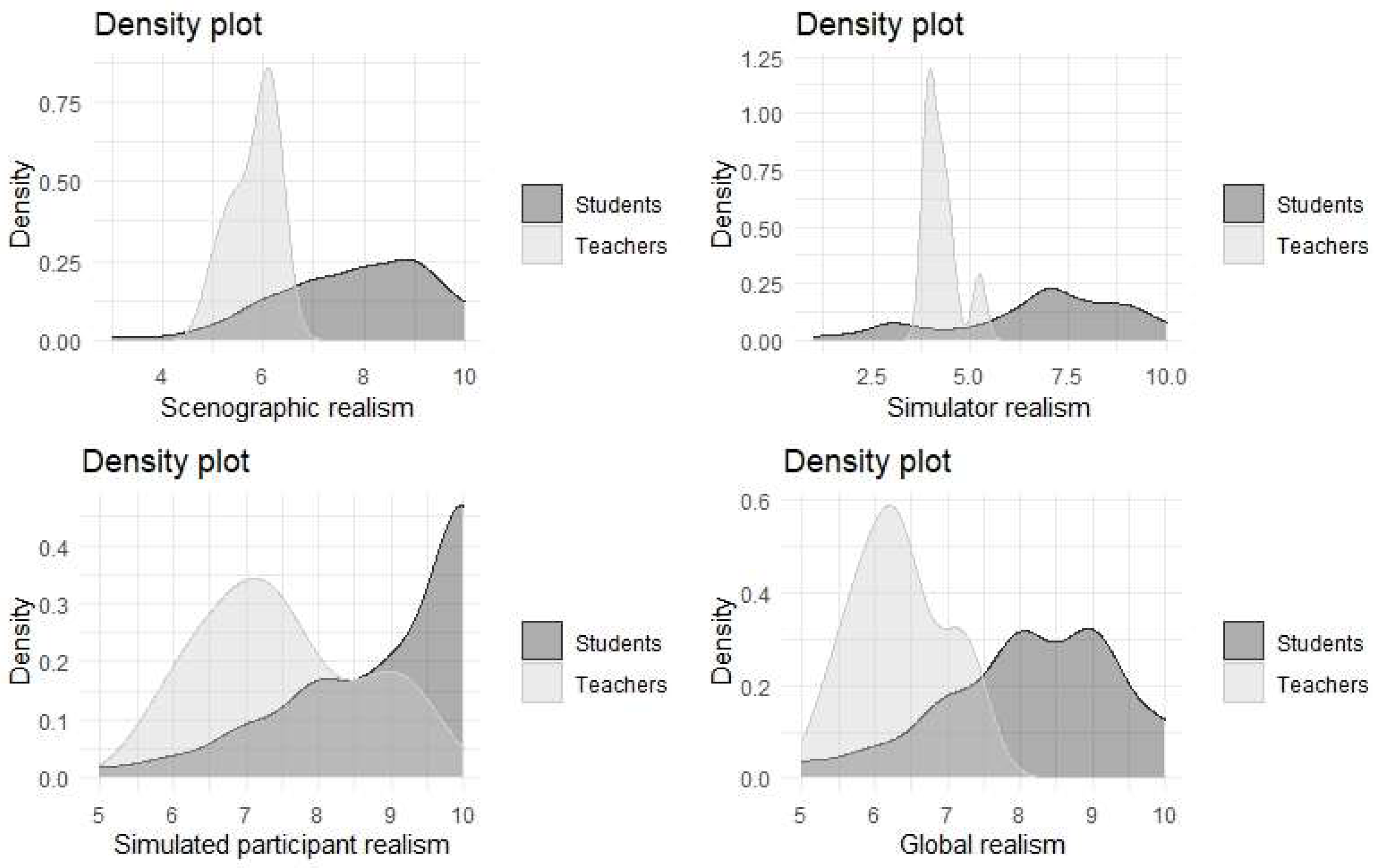
| Perceived Realism of the Office | Perceived Realism of the Mannequin | Perceived Realism of the Participant | Global Perceived Realism | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Position | Mean | Standard Deviation | p-Value | Mean | Standard Deviation | p-Value | Mean | Standard Deviation | p-Value | Mean | Standard Deviation | p-Value |
| Student | 7.83 | 1.48 | 0.0001797 (a) | 6.79 | 2.22 | 0.001181 (a) | 8.99 | 1.28 | 0.001857 (a) | 8.15 | 1.22 | 0.0001889 (a) |
| Teacher | 5.81 | 0.453 | 0.0001797 (a) | 4.25 | 0.454 | 0.001181 (a) | 7.49 | 1.13 | 0.001857 (a) | 6.34 | 0.641 | 0.0001889 (a) |
| 95% CI for Student-Faculty Variance Difference | ||||
|---|---|---|---|---|
| Perceived Realism of the Office | Perceived Realism of the Mannequin | Perceived Realism of the Participant | Global Perceived Realism | |
| Punctuation | 2.020833 | 2.535724 | 1.499978 | 1.810373 |
| 95% IC | [1.579782, 2.461884] | [2.005260, 3.066188] | [0.5415388, 2.4584174] | [1.251806, 2.368940] |
| Realism Measured by Students | Realism Measured by the Faculty | |||
|---|---|---|---|---|
| Spearman’s Correlation | p-Value | Spearman’s Correlation | p-Value | |
| Student’s perception of clinical competence | 0.26 | 0.00576 (a) | −0.1571209 | 0.09502 (a) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartolomé Villar, B.; Real Benlloch, I.; De la Hoz Calvo, A.; Coro-Montanet, G. Perception of Realism and Acquisition of Clinical Skills in Simulated Pediatric Dentistry Scenarios. Int. J. Environ. Res. Public Health 2022, 19, 11387. https://doi.org/10.3390/ijerph191811387
Bartolomé Villar B, Real Benlloch I, De la Hoz Calvo A, Coro-Montanet G. Perception of Realism and Acquisition of Clinical Skills in Simulated Pediatric Dentistry Scenarios. International Journal of Environmental Research and Public Health. 2022; 19(18):11387. https://doi.org/10.3390/ijerph191811387
Chicago/Turabian StyleBartolomé Villar, Begoña, Irene Real Benlloch, Ana De la Hoz Calvo, and Gleyvis Coro-Montanet. 2022. "Perception of Realism and Acquisition of Clinical Skills in Simulated Pediatric Dentistry Scenarios" International Journal of Environmental Research and Public Health 19, no. 18: 11387. https://doi.org/10.3390/ijerph191811387
APA StyleBartolomé Villar, B., Real Benlloch, I., De la Hoz Calvo, A., & Coro-Montanet, G. (2022). Perception of Realism and Acquisition of Clinical Skills in Simulated Pediatric Dentistry Scenarios. International Journal of Environmental Research and Public Health, 19(18), 11387. https://doi.org/10.3390/ijerph191811387