1. Introduction
The World Health Organization (WHO) recognizes sexual health as an essential aspect of the life of human beings and strives to promote recognition and attention to sexual rights through policies, education, and integration in health systems [
1]. Despite this, the training of professionals around sexual health is scarce, and sexuality continues to be ignored in clinical practice [
2,
3]. Sexually transmitted infections affect about 365 million people per year, and it is a mandatory point to address in primary health care [
4].
Family physicians have an essential role in this regard, being the first to be consulted on these issues and being able to detect problems in the sexual sphere of their patients [
2,
5,
6]. Elements such as longitudinally in time allow an approach based on greater confidence [
2,
7,
8]. In addition, they have patients in consultation who associate various types of pathologies, from diabetes to cardiovascular diseases, which affect the sexual sphere to a different extent, making difficulties in this matter more prevalent [
9,
10,
11]. They generally have a good predisposition to attend to the sexuality of their patients, but there are several clear barriers to overcome [
5]. Physicians’ attitudes are influenced by various factors, such as patients’ age, health status, or socioeconomic status, as well as their usual focus on family planning and sexually transmitted infections [
5,
6,
11].
The level of training in sexual health among professionals is usually related to a more excellent approach to patients’ sexuality in their clinical practice, and understanding the development of this training is a priority to improve the skills of professionals [
6,
12]. The lack of training, consequently, conditions low confidence to address these issues, a poor perception of available therapeutic options and an underestimation of the prevalence of these difficulties, so they can be infra-diagnosed [
12]. There is often an assumption that the sexual sphere passes into the background or that its deterioration is expected when other diseases appear [
10]. The main barriers are that the patient and the doctor feel discomfort when dealing with these issues and time pressure. The latter is the most described by professionals [
13,
14,
15,
16].
Family doctors tend not to ask about sexuality and focus on the biological rather than psychological aspects of their patients’ sexuality [
10,
11,
17]. However, despite the modesty of doctors, most patients do not feel invaded when asked about sexual aspects, even when the reason for consultation is another [
11]. These barriers could be overcome by improving the training of professionals, something the professionals have demanded [
12,
14,
16,
18]. Regarding recording the sexual clinical history, again, the studies find that elements such as intimacy or lack of time play against [
3,
6,
13,
14,
15]. In recent years, patients’ sexuality has become an enlightened area to address in their health, although they remain reluctant to consult about it. Evidence suggests that patients feel comfortable with physicians asking about their sexuality when it is appropriately approached, building stronger relationships with them. However, asking about sexuality exposes underlying concerns that patients would not consult otherwise [
11].
There have been studies that present a nonstandardized method in their analyses [
5], with a qualitative approach [
10,
11] or focused on patients [
19]. However, no standardized questionnaires have been found to assess family physicians’ work regarding sexuality quantitatively. In addition, previous studies have focused on patients’ sexual orientation and physicians’ behavior towards it [
20,
21,
22], but our research did not find studies in which doctors’ sexual orientation was considered.
Therefore, the main objective of this study was to assess the family physicians’ competence and attitude regarding sexuality quantitatively. To perform this, we assessed three spheres of family physicians’ practice regarding patients’ sexuality: their attitudes or mindset, their aptitudes or capacity to approach this issue, and their procedures or actual labor in this area. A questionnaire was developed to perform this task. We also sought to assess the validity of the questionnaire.
2. Materials and Methods
2.1. Design of the Study
A cross-sectional observational study was performed to evaluate physicians’ performance toward patients’ sexuality according to their attitudes, aptitudes, and procedures in clinical practice. The study was carried out among family and community medicine physicians in primary care of the Andalusian Health Service in Almería, located in southeastern Spain. This location was selected for reasons of plausibility and methodological soundness. According to the Spanish National Statistics Institute, these professionals attended to a population of 731,792 inhabitants as of 1 January 2022 [
23]. The questionnaire was developed from scratch based on data obtained from a literature review and the author’s experience. The questionnaire collected five demographic aspects (sex, age, sexual orientation, if the participants had a partner, and sexology training); and fifty qualitative items that assessed the participants’ competence, attitude, and procedures. The questionnaire obeyed a Likert scale format, where participants responded one to four, where one meant «never» or «totally disagree» and four, «always» or «totally agree».
2.2. Sample Size Estimation
The sample size was calculated utilizing the Epi Info™ app, from Atlanta CDC, with the following parameters: population size of 731,792 [
23], 80% confidence interval, and a level of precision of 5%. These parameters indicated a required sample size of 164 participants. The authors decided to collect at least 250 responses to lower potential auto selection bias and to comply with the classic rule established by Kline et al. [
24] of using two to twenty subjects for each questionnaire item for the factorial analysis.
2.3. Eligible Population and Recruitment
The eligible populations were family and community medicine physicians in the Andalusian Health Service primary care in Almería. Population peculiarities were not contemplated, as the subject of the study were physicians and not their patients. The questionnaire was sent by email from the Almeria Primary Care Management of the Andalusian Health Service to the professionals potentially eligible to participate in the study. The inclusion criteria were: being family and community medicine physicians, working in the Andalusian Health Service in Almería, working in primary care, and being able to speak and read Spanish fluently. The exclusion criteria were: not meeting any of the referred inclusion criteria and not wishing to participate in the study, despite meeting the criteria.
2.4. Questionnaire Validation
Content validation was performed by an expert panel made up of nine family physicians and sexologists. The tool’s reliability was measured using Cronbach’s alpha [
25]. The split-half method was used to assess the stability as the questionnaire could not be retested with the same users [
26]. The adequacy of the exploratory factor analysis (EFA) was determined through the analysis of Bartlett’s test and the Kaiser–Meyer–Olkin (KMO) measure. For construct validity, the qualitative items of the questionnaire were evaluated through exploratory factor analysis. Confirmatory factor analysis (CFA) was conducted using AMOS software’s maximum likelihood estimation technique. This method read the structures determined in the exploratory factor analysis. The goodness of fit was assessed using the most typical fit indices employed in the literature [
27]: the root mean square error of approximation (RMSEA), the normed fit index (NFI), the non-normed fit index (NNFI), or Tucker–Lewis index (TLI), and the comparative fit index (CFI).
2.5. Statistical Analyses and Review Board Approval
Statistical analyses and the exploratory factorial analysis were performed using SPSS version 28 (IBM Inc., Armonk, NY, USA). Univariant and bivariant analyses were conducted. The statistical software AMOS version 26.0.0 (IBM Inc., Armonk, NY, USA) was used for confirmatory factor analysis. The study was conducted in accordance with the Declaration of Helsinki. Informed consent was shown at the beginning of the questionnaire. Personal data were not collected. The confidentiality of the participants was absolute as no personal data were collected or stored, and the researchers only could access completely anonymous questionnaires. Although the responses were anonymous and, therefore, participants could not be identified, the questionnaires were stored in encrypted servers of the Andalusian Health Service. This study was approved by the Research and Ethics Committee of Nursing, Physiotherapy, and Medicine Department of the University of Almeria (Spain), with approval number EFM 205/2022.
4. Discussion
The main objective of this study was to assess the family physicians’ work regarding sexuality quantitatively through a questionnaire that evaluated their attitudes (that is, their disposition in this regard), their aptitudes (what they could do) and the procedures (what they currently did) of professionals of primary care regarding the sexuality of their patients. We also sought to assess the validity of the questionnaire to perform this specific task.
4.1. Sociodemographic Features
Most of the physicians that participated in this research were women, which can be representative of the current composition of primary care physicians, as stated by other authors [
28]. This finding also agrees with the available data from the Andalusian Health Service [
29]. The mean age of the doctors in our sample is similar to other similar research based on surveys performed on physicians [
30]. An important aspect to consider is that there are studies assessing potential homophobia among doctors [
31,
32], but we have not found research that describes the percentage of heterosexual, homosexual, or bisexual doctors. Therefore, this research could be a pioneer in not only describing this aspect but also correlating it to the competencies, attitudes, and knowledge of procedures regarding sexology. Few studies have neither assessed having a partner regarding these aspects. Although some studies analyze the training in sexology regarding professional attitudes towards sexuality [
33], they are scarce.
4.2. Validation of the Questionnaire
The exploratory factor analysis excluded 38 items from the initial 50-item questionnaire. This process allowed us to define a much shorter validated questionnaire, also easier to fulfill, based on the 12 items that contributed most to the construct of the questionnaire. This figure may appear significant but aligns with other studies in other ambits [
34,
35]. Moreover, the exclusion of those items permitted us to define better the four domains using fewer items. These domains were assessed based on the items which defined them, as stated by other authors [
27]. Cronbach’s alpha coefficient is the most used method to evaluate the internal consistency of a questionnaire [
27], and the value obtained can be regarded as excellent, according to other authors [
27,
34]. The split-half method, used in the same period or when other techniques such as test-retest cannot be used [
36], verified the stability of the questionnaire.
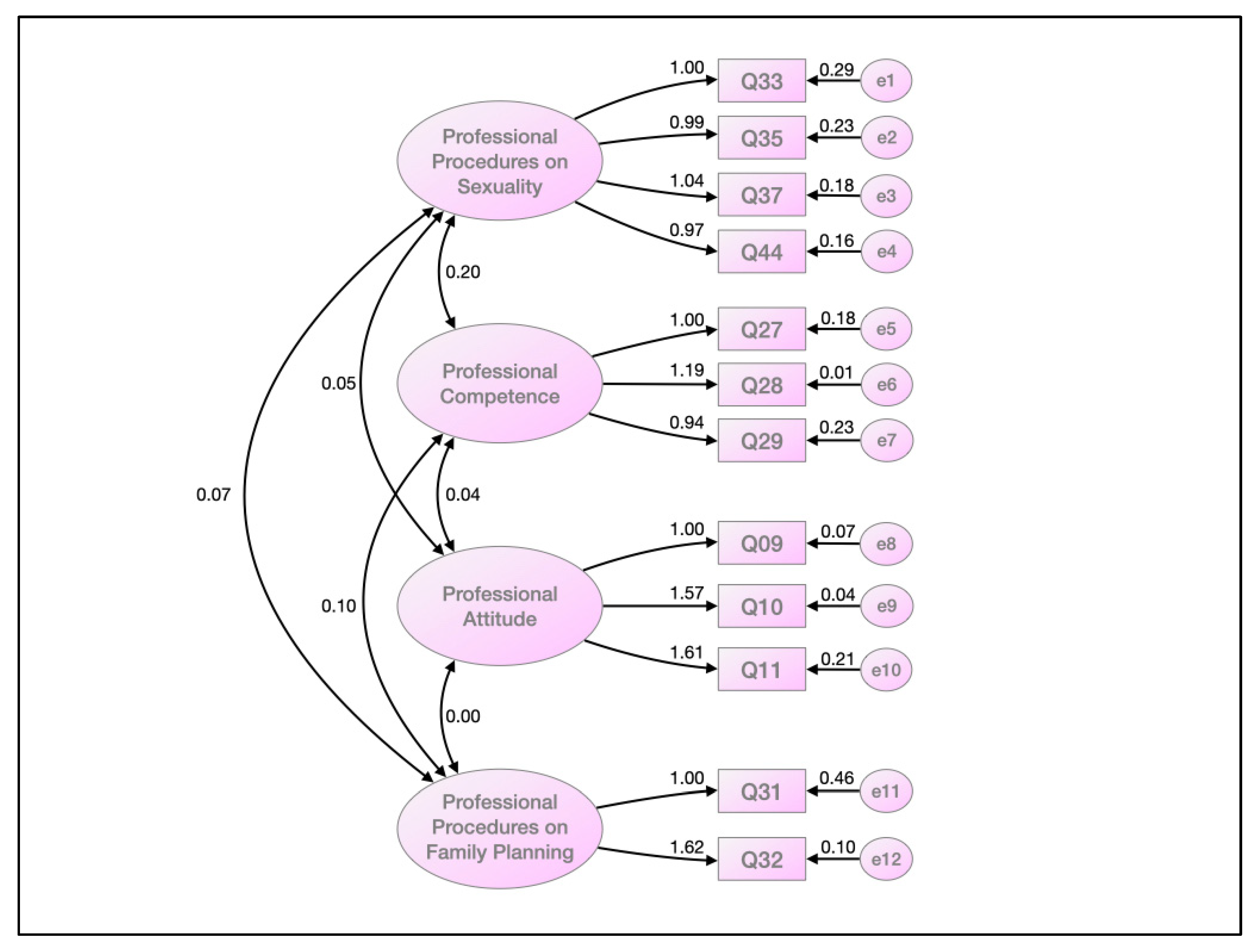
The confirmatory factorial analysis was utilized to establish the questionnaire’s underlying conceptual structure [
37]. Albeit the evaluation of RMSEA can be subjective, weights under 0.08 are considered indicative of a good fit, and in our case, it was much lower. The rest of the parameters used to evaluate the model’s goodness of fit were the most used in the literature [
27], and all of them were close to one, indicating a near-to-perfect fit.
4.3. Univariant Analysis
Contrary to some authors who state that physicians’ attitudes toward sexology could be improved [
38,
39], the domain that defined their attitude toward sexology achieved the highest score among our physicians. However, as the overall score of the questionnaire was lower, and the score of the professional procedures on the sexuality domain achieved the lowest score, we agree with the affirmations of these same authors, who propose improving role modeling and education or multicomponent implementation programs to improve health professionals’ knowledge and competence when addressing sexuality issues with their patients [
38,
39].
4.4. Bivariant Analysis
The analysis of the different domains of the questionnaire regarding different aspects of the family physicians, such as sex, sexual orientation, training in sexuality, or if they had a partner, showed some interesting findings. Similar to other research [
20,
21], women scored higher in the domain that defined professional attitude. However, men scored higher in the domain that defined professional competence and the global score of the questionnaire, while other authors state that healthcare professionals have limited knowledge and confidence when addressing sexuality [
21,
39]. A plausible interpretation of this finding is that perhaps men may be more confident than women in their sexology skills and attitudes, even subjectively. Another important finding is that no differences were found in the scores of the domains or the global score regarding if the family physicians had a partner. This finding may be innovative, and it can help compare future research.
Some authors have described that heterosexual healthcare providers have a more positive attitude toward sexuality when they address heterosexual people [
22]. However, in our research, we found two interesting findings: albeit heterosexual participants scored lower in the attitude domain, and pairwise comparison showed that the heterosexual participants scored lower than the bisexual ones, the
p-value was slightly under the significance value. Even more, in the rest of the domains or the global score, no significant differences were found regarding the sexual orientation of the Family physicians. Therefore, we can conclude that the attitude toward sexuality was independent of the sexual orientation of the healthcare providers, excepting a possible worse attitude from heterosexual professionals. However, given the slight differences, this specific finding should be studied in more detail in future research.
It seems logical that the professionals with higher training in sexuality scored higher in the global score and the domains that defined the professional procedures on sexuality, family planning, and professional competence. However, contrary to several authors’ findings [
6,
12,
40,
41,
42], we found no differences in the attitude of the professionals regarding their training in sexuality. We believe this is an exciting finding, as our interpretation is that if family physicians’ attitudes toward sexuality is the same, independently of their training in sexuality, it is because finally, professionals, whether trained in sexology or not, are at least beginning to be aware of the importance of adopting a proactive attitude to this issue.
The last aspect analyzed, the age of the family physicians, shows some striking results not reflected in the literature. It seems logical that younger physicians score higher in the domain that defines the attitude toward sexuality, while older participants score higher in the domains that define the knowledge of professional procedures on sexuality and family training. However, there was a positive correlation between the age of the physicians and the global score of the questionnaire. A possible conclusion of these findings is that, independently of their age, family physicians seem to become more involved with their patients’ sexuality as they gain professional experience. We believe that this is another critical finding that seems logical and promising.
A significant interpretation of our results is the potential applicability for clinical practice and professional training programs’ development. The validation of this questionnaire was intended to allow further application abroad, nationally or internationally, to comprehend family medicine physicians’ situation towards sexuality. This potential future research may allow the development of strategies to improve the situation when required. The data obtained from its appliance could also raise awareness among professionals about the relevance of education in these matters. Future research could dig into themes such as practitioners’ flaws and the resources they consider more helpful to acquiring sexuality concerns in their day-to-day work.
4.5. Limitations and Strengths
This research has some limitations. The most important is the selection bias due to various factors. Our sample was obtained from the family physicians of a province of 731,792 inhabitants, but it could not be representative of other regions or countries. In addition, participation was voluntary, which contributes to the potential selection bias. We must also consider that the questionnaire and the study were in Spanish. Larger sample sizes could also help increase the confidence interval. These aspects must be considered when assessing the external validity of our conclusions, which should be interpreted with caution.
This research also has some strengths. The most important one is that the questionnaire obtained excellent results in the exploratory and confirmatory factor analyses and the reliability studies. These aspects give almost complete validity to the final questionnaire and support the possibility of using it in future studies. Another important strength is that the study has been performed with current real healthcare professionals from primary care, and some of the aspects assessed are innovative. Thus, our findings can be helpful for current clinical practice and future research.
5. Conclusions
This study could be the first to describe the percentage of heterosexual, homosexual, and bisexual family physicians or the percentage with a partner and correlate these aspects to their competencies, attitudes, and knowledge of procedures regarding sexology and family planning in their patients. While female family physicians may show a more positive attitude toward sexuality, males feel more confident globally. Competences, attitudes, and knowledge of procedures are the same, independent of whether the professional has a partner, and there may be slight differences regarding attitude when considering the sexual orientation of the physicians. One of the most important findings is that the attitude toward sexuality does not depend on their previous training in this topic. Even more, albeit younger family physicians have a more positive attitude toward sexuality, all providers seem to become more involved with their patients’ sexuality as they gain professional experience. These are critical findings that can break some clichés. Finally, the developed questionnaire is a valid tool to assess these aspects and could be translated and culturally adapted to other languages or countries for future research.


 ,
, 


{kind=link}
{kind=link}