
Mental Health of Japanese Workers: Amotivation Mediates Self-Compassion on Mental Health Problems



Abstract
:1. Introduction
1.1. Poor Mental Health in Japanese Workforce
1.2. Self-Compassion
1.3. Work Motivation
1.4. Work Motivation on Pathway from Self-Compassion to Mental Health
1.5. Study Aims
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Instruments
3. Results
3.1. Relationships between Mental Health Problems, Self-Compassion and Work Motivation (Aim 1)
3.2. Mediation of Motivation for Self-Compassion in Mental Health Problems (Aim 2)
3.2.1. Intrinsic Motivation
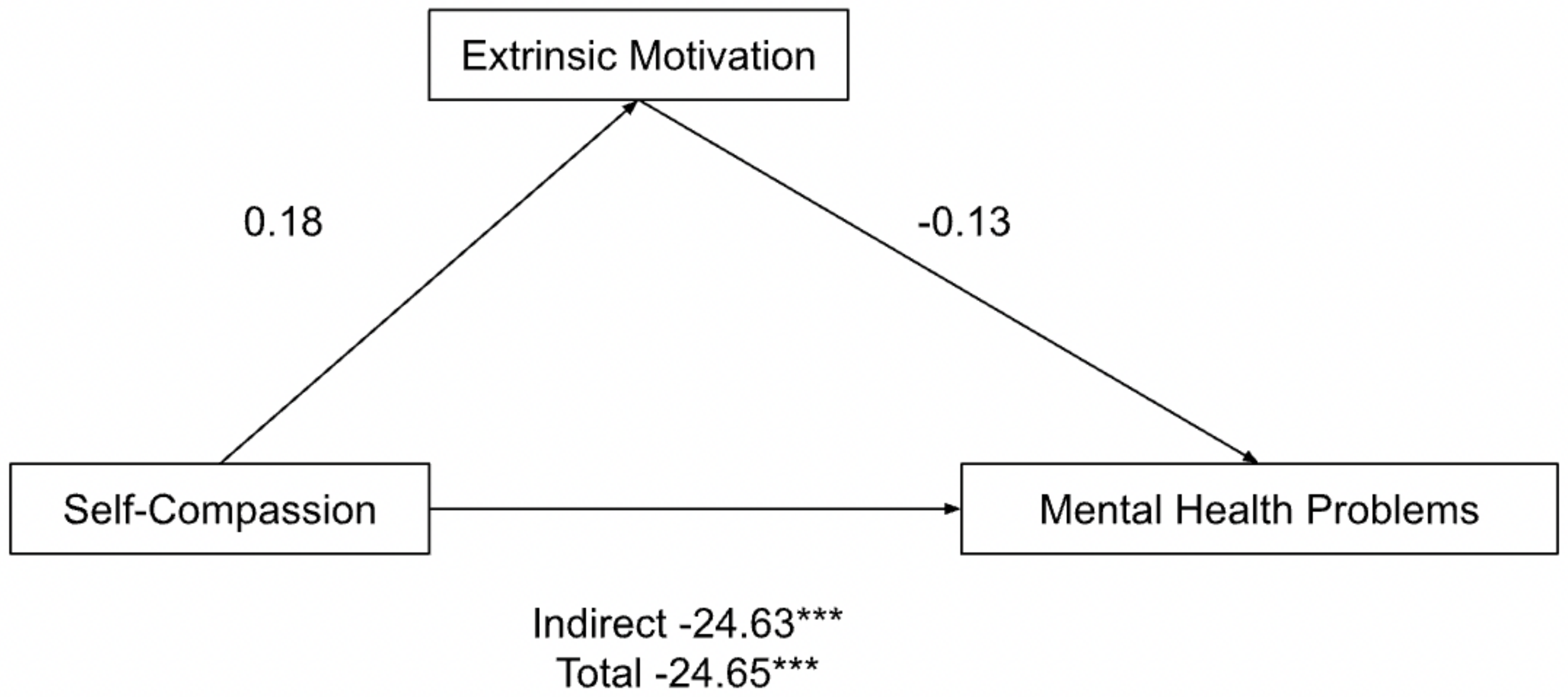
3.2.2. Extrinsic Motivation
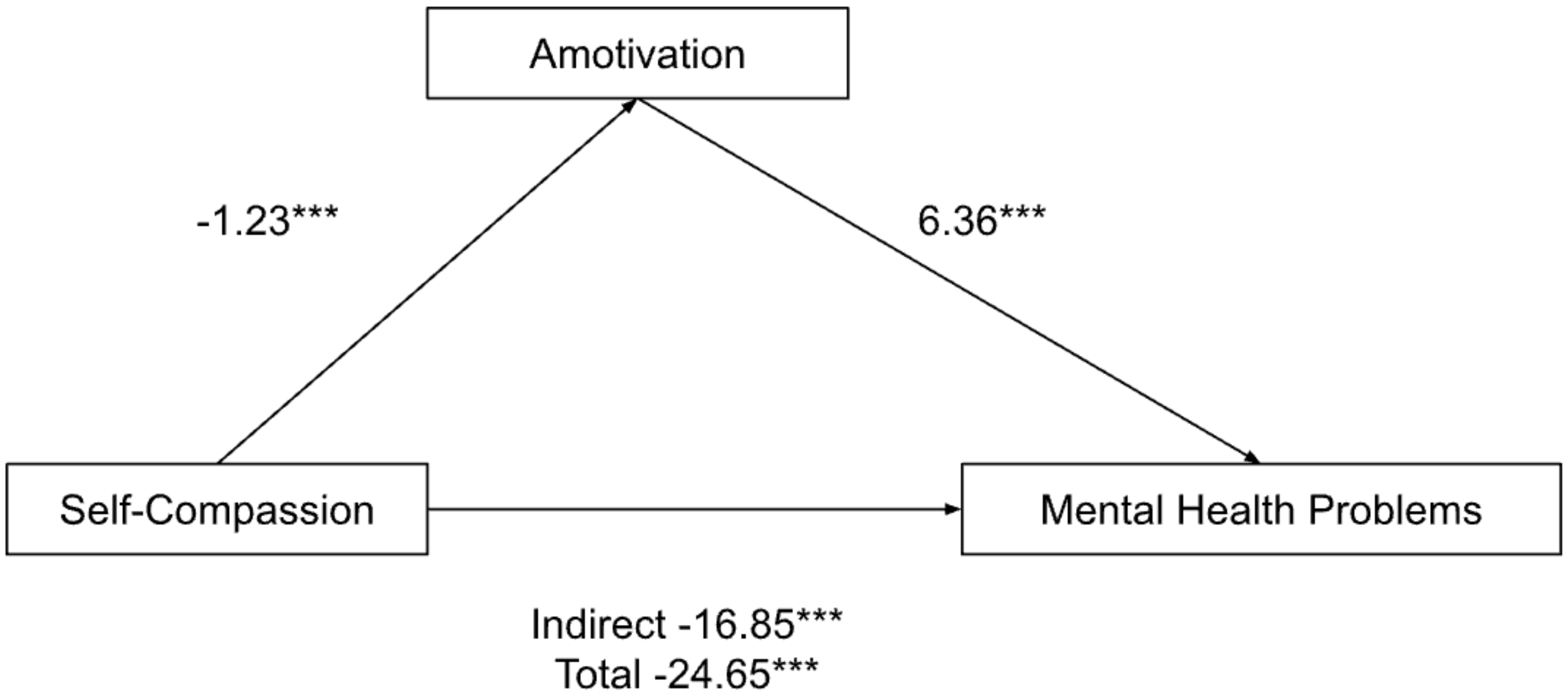
3.2.3. Amotivation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauz, E.; Eicher, S.; Peitz, D.; Junker, S.; Hölling, H.; Thom, J. Psychische Gesundheit der erwachsenen Bevölkerung in Deutschland während der COVID-19-Pandemie. Ein Rapid-Review. J. Health Monit. 2021, 6, 1–65. (In German) [Google Scholar] [CrossRef]
- Health and Safety Executive. Work-Related Stress, Anxiety or Depression Statistics in Great Britain, 2021; Health and Safety Executive: London, UK, 2021. [Google Scholar]
- Abdin, E.; Chong, S.A.; Vaingankar, J.A.; Shafie, S.; Verma, S.; Luo, N.; Tan, K.B.; James, L.; Heng, D.; Subramaniam, M. Impact of mental disorders and chronic physical conditions on quality-adjusted life years in Singapore. Sci. Rep. 2020, 10, 2695. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Surányi, R. Gaining trust and remaining mentally sane while working from home: The importance of employee wellbeing. Intersections 2021, 7, 223–240. [Google Scholar] [CrossRef]
- Kotera, Y.; Vione, K.C. Psychological Impacts of the New Ways of Working (NWW): A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5080. [Google Scholar] [CrossRef]
- Oakman, J.; Kinsman, N.; Stuckey, R.; Graham, M.; Weale, V. A rapid review of mental and physical health effects of working at home: How do we optimise health? BMC Public Health 2020, 20, 1825. [Google Scholar] [CrossRef]
- Koch-Institut, R. Depressive symptoms in a European comparison—Results from the European Health Interview Survey (EHIS) 2. J. Health Monit. 2019, 4, 57. [Google Scholar] [CrossRef]
- United Nations. Sustainable Development Goals; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a new definition of mental health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef] [Green Version]
- YKotera, Y.; Tsuda-McCaie, F.; Maughan, G.; Green, P. Cross-cultural comparison of mental health in social work students between UK and Ireland: Mental health shame and self-compassion. Br. J. Soc. Work 2021, bcab240. [Google Scholar] [CrossRef]
- Henrich, J. The Weirdest People in the World: How the West Became Psychologically Peculiar and Particularly Prosperous; Penguin Random House: Dublin, Ireland, 2020; 680p. [Google Scholar]
- Moleiro, C. Culture and Psychopathology: New Perspectives on Research, Practice, and Clinical Training in a Globalized World. Front. Psychiatry 2018, 9, 366. [Google Scholar] [CrossRef]
- Cuellar, N.G. Marginalization of Cultural Groups. J. Transcult. Nurs. 2016, 27, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyashanu, M.; Ganga, G.; Chenneville, T. Exploring the Impact of Religion, Superstition, and Professional Cultural Competence on Access to HIV and Mental Health Treatment among Black Sub-Sahara African Communities in the English City of Birmingham. J. Relig. Health 2022, 61, 252–268. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Ting, S.-H.; Neary, S. Mental health of Malaysian university students: UK comparison, and relationship between negative mental health attitudes, self-compassion, and resilience. High. Educ. 2020, 81, 403–419. [Google Scholar] [CrossRef]
- Kotera, Y.; Lieu, J.; Kirkman, A.; Barnes, K.; Liu, G.H.T.; Jackson, J.; Wilkes, J.; Riswani, R. Mental Wellbeing of Indonesian Students: Mean Comparison with UK Students and Relationships with Self-Compassion and Academic Engagement. Healthcare 2022, 10, 1439. [Google Scholar] [CrossRef]
- Kotera, Y.; Sheffield, D.; Green, P.; Asano, K. Cross-Cultural Comparison of Mental Health Shame: Negative Attitudes and External, Internal, and Reflected Shame About Mental Health in Japanese and UK Workers. In Shame 4.0; Springer: Cham, Switzerland, 2021; pp. 55–71. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. White Paper about Suicide Prevention in Japan [Jisatsu Taisaku Hakusho]; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2021. [Google Scholar]
- Hidaka, Y.; Imamura, K.; Watanabe, K.; Tsutsumi, A.; Shimazu, A.; Inoue, A.; Hiro, H.; Odagiri, Y.; Asai, Y.; Yoshikawa, T.; et al. Associations between work-related stressors and QALY in a general working population in Japan: A cross-sectional study. Int. Arch. Occup. Environ. Health 2021, 94, 1375–1383. [Google Scholar] [CrossRef]
- Kotera, Y.; Ozaki, A.; Miyatake, H.; Tsunetoshi, C.; Nishikawa, Y.; Tanimoto, T. Mental health of medical workers in Japan during COVID-19: Relationships with loneliness, hope and self-compassion. Curr. Psychol. 2021, 40, 6271–6274. [Google Scholar] [CrossRef]
- Amagasa, T.; Nakayama, T.; Takahashi, Y. Karojisatsu in Japan: Characteristics of 22 Cases of Work-Related Suicide. J. Occup. Health 2005, 47, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Imamura, K.; Kawakami, N. Working hours and the onset of depressive disorder: A systematic review and meta-analysis. Occup. Environ. Med. 2016, 73, 877–884. [Google Scholar] [CrossRef]
- Inoue, Y.; Yamamoto, S.; Fukunaga, A.; Van Hoang, D.; Miki, T.; Islam, Z.; Miyo, K.; Ishii, M.; Ishiwari, H.; Konishi, M.; et al. Association between engagement in COVID-19-related work and depressive symptoms among hospital workers in a designated COVID-19 hospital in Japan: A cross-sectional study. BMJ Open 2021, 11, e049996. [Google Scholar] [CrossRef]
- Ogawa, R.; Seo, E.; Maeno, T.; Ito, M.; Sanuki, M.; Maeno, T. The relationship between long working hours and depression among first-year residents in Japan. BMC Med Educ. 2018, 18, 50. [Google Scholar] [CrossRef] [Green Version]
- D’Ambrogio, E. Japan’s Ageing Society. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2020/659419/EPRS_BRI(2020)659419_EN.pdf.
- Muris, P.; Meesters, C.; Pierik, A.; De Kock, B. Good for the Self: Self-Compassion and Other Self-Related Constructs in Relation to Symptoms of Anxiety and Depression in Non-clinical Youths. J. Child Fam. Stud. 2016, 25, 607–617. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Conway, E.; Van Gordon, W. Ethical Judgement in UK Business Students: Relationship with Motivation, Self-Compassion and Mental Health. Int. J. Ment. Health Addict. 2019, 17, 1132–1146. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Van Gordon, W. Effects of Self-Compassion Training on Work-Related Well-Being: A Systematic Review. Front. Psychol. 2021, 12, 630798. [Google Scholar] [CrossRef] [PubMed]
- Zessin, U.; Dickhäuser, O.; Garbade, S. The Relationship between Self-Compassion and Well-Being: A Meta-Analysis. Appl. Psychol. Health Well-Being 2015, 7, 340–364. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Green, P.; Sheffield, D. Mental health of therapeutic students: Relationships with attitudes, self-criticism, self-compassion, and caregiver identity. Br. J. Guid. Couns. 2019, 49, 701–712. [Google Scholar] [CrossRef]
- Kotera, Y.; Cockerill, V.; Chircop, J.; Kaluzeviciute, G.; Dyson, S. Predicting self-compassion in UK nursing students: Relationships with resilience, engagement, motivation, and mental wellbeing. Nurse Educ. Pract. 2021, 51, 102989. [Google Scholar] [CrossRef]
- Forkus, S.R.; Breines, J.G.; Weiss, N.H. Morally injurious experiences and mental health: The moderating role of self-compassion. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 630–638. [Google Scholar] [CrossRef]
- Kurebayashi, Y. Self-compassion and nursing competency among Japanese psychiatric nurses. Perspect. Psychiatr. Care 2020, 57, 1009–1018. [Google Scholar] [CrossRef]
- Montero-Marin, J.; Kuyken, W.; Crane, C.; Gu, J.; Baer, R.; Al-Awamleh, A.A.; Akutsu, S.; Araya-Véliz, C.; Ghorbani, N.; Chen, Z.J.; et al. Self-Compassion and Cultural Values: A Cross-Cultural Study of Self-Compassion Using a Multitrait-Multimethod (MTMM) Analytical Procedure. Front. Psychol. 2018, 9, 2638. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Sugiyama, F.; Kikai, T.; Kawashima, I.; Guan, S.; Oguchi, M.; Uchida, T.; Kumano, H. Changes in depression and anxiety through mindfulness group therapy in Japan: The role of mindfulness and self-compassion as possible mediators. BioPsychoSoc. Med. 2019, 13, 4. [Google Scholar] [CrossRef] [Green Version]
- Wilson, A.C.; Mackintosh, K.; Power, K.; Chan, S.W.Y. Effectiveness of Self-Compassion Related Therapies: A Systematic Review and Meta-analysis. Mindfulness 2018, 10, 979–995. [Google Scholar] [CrossRef] [Green Version]
- Kurebayashi, Y. The effect of revised process recording on self-focus and self-compassion: A randomized controlled pilot study. Perspect. Psychiatr. Care 2021, 57, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.-F.; Yang, L.; Ma, J.-P.; Qin, Z.-J. Path analysis of the association between self-compassion and depressive symptoms among nursing and medical students: A cross-sectional survey. BMC Nurs. 2022, 21, 67. [Google Scholar] [CrossRef]
- Voon, S.P.; Lau, P.L.; Leong, K.E.; Jaafar, J.L.S. Self-Compassion and Psychological Well-Being among Malaysian Counselors: The Mediating Role of Resilience. Asia-Pac. Educ. Res. 2021, 31, 475–488. [Google Scholar] [CrossRef]
- Prentice, K.; Rees, C.; Finlay-Jones, A. Self-Compassion, Wellbeing, and Distress in Adolescents and Young Adults with Chronic Medical Conditions: The Mediating Role of Emotion Regulation Difficulties. Mindfulness 2021, 12, 2241–2252. [Google Scholar] [CrossRef] [PubMed]
- Raes, F. Rumination and worry as mediators of the relationship between self-compassion and depression and anxiety. Personal. Individ. Differ. 2010, 48, 757–761. [Google Scholar] [CrossRef]
- Kotera, Y.; Gilbert, P.; Asano, K.; Ishimura, I.; Sheffield, D. Self-criticism and self-reassurance as mediators between mental health attitudes and symptoms: Attitudes toward mental health problems in Japanese workers. Asian J. Soc. Psychol. 2018, 22, 183–192. [Google Scholar] [CrossRef]
- Kotera, Y.; Adhikari, P.; Van Gordon, W. Motivation Types and Mental Health of UK Hospitality Workers. Int. J. Ment. Health Addict. 2018, 16, 751–763. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Kikuchi, H.; Odagiri, Y.; Ohya, Y.; Nakanishi, Y.; Shimomitsu, T.; Theorell, T.; Inoue, S. Association of overtime work hours with various stress responses in 59,021 Japanese workers: Retrospective cross-sectional study. PLoS ONE 2020, 15, e0229506. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Taylor, E.; Fido, D.; Williams, D.; Tsuda-McCaie, F. Motivation of UK graduate students in education: Self-compassion moderates pathway from extrinsic motivation to intrinsic motivation. Curr. Psychol. 2021. [Google Scholar] [CrossRef]
- Kotera, Y.; Green, P.; Sheffield, D. Mental Health Attitudes, Self-Criticism, Compassion and Role Identity among UK Social Work Students. Br. J. Soc. Work 2019, 49, 351–370. [Google Scholar] [CrossRef]
- Kotera, Y.; Ting, S.-H. Positive Psychology of Malaysian University Students: Impacts of Engagement, Motivation, Self-Compassion, and Well-being on Mental Health. Int. J. Ment. Health Addict. 2021, 19, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Green, P.; Sheffield, D. Mental Health Shame of UK Construction Workers: Relationship with Masculinity, Work Motivation, and Self-Compassion. Rev. Psicol. Trab. Organ. 2019, 35, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Green, P.; Sheffield, D. Positive Psychology for Mental Wellbeing of UK Therapeutic Students: Relationships with Engagement, Motivation, Resilience and Self-Compassion. Int. J. Ment. Health Addict. 2021, 20, 1611–1626. [Google Scholar] [CrossRef]
- Neff, K.D.; Hsieh, Y.-P.; Dejitterat, K. Self-compassion, Achievement Goals, and Coping with Academic Failure. Self Identity 2005, 4, 263–287. [Google Scholar] [CrossRef]
- Dundas, I.; Binder, P.-E.; Hansen, T.G.B.; Stige, S.H. Does a short self-compassion intervention for students increase healthy self-regulation? A randomized control trial. Scand. J. Psychol. 2017, 58, 443–450. [Google Scholar] [CrossRef]
- Neff, K.D.; Kirkpatrick, K.L.; Rude, S.S. Self-compassion and adaptive psychological functioning. J. Res. Personal. 2007, 41, 139–154. [Google Scholar] [CrossRef]
- Shapiro, S.L.; Astin, J.A.; Bishop, S.R.; Cordova, M. Mindfulness-Based Stress Reduction for Health Care Professionals: Results From a Randomized Trial. Int. J. Stress Manag. 2005, 12, 164–176. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Tsuda-McCaie, F.; Edwards, A.-M.; Bhandari, D.; Maughan, G. Self-Compassion in Irish Social Work Students: Relationships between Resilience, Engagement and Motivation. Int. J. Environ. Res. Public Health 2021, 18, 8187. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Van Laethem, M.; Ohshima, R. Cross-cultural comparison of mental health between Japanese and Dutch workers: Relationships with mental health shame, self-compassion, work engagement and motivation. Cross Cult. Strat. Manag. 2020, 27, 511–530. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2013; p. 507. [Google Scholar]
- Lovibond, S.; Lovibond, P. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Neff, K.D. The Development and Validation of a Scale to Measure Self-Compassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Tremblay, M.A.; Blanchard, C.M.; Taylor, S.; Pelletier, L.G.; Villeneuve, M. Work Extrinsic and Intrinsic Motivation Scale: Its value for organizational psychology research. Can. J. Behav. Sci./Rev. Can. Sci. Comport. 2009, 41, 213–226. [Google Scholar] [CrossRef]
- Kotera, Y.; Mayer, C.-H.; Vanderheiden, E. Cross-Cultural Comparison of Mental Health Between German and South African Employees: Shame, Self-Compassion, Work Engagement, and Work Motivation. Front. Psychol. 2021, 12, 627851. [Google Scholar] [CrossRef]
- Kotera, Y.; Maxwell-Jones, R.; Edwards, A.-M.; Knutton, N. Burnout in Professional Psychotherapists: Relationships with Self-Compassion, Work–Life Balance, and Telepressure. Int. J. Environ. Res. Public Health 2021, 18, 5308. [Google Scholar] [CrossRef]
- Kotera, Y.; Rhodes, C. Pathways to Sex Addiction: Relationships with Adverse Childhood Experience, Attachment, Narcissism, Self-Compassion and Motivation in a Gender-Balanced Sample. Sex. Addict. Compulsivity 2019, 26, 54–76. [Google Scholar] [CrossRef]
- Kotera, Y.; Conway, E.; Van Gordon, W. Mental health of UK university business students: Relationship with shame, motivation and self-compassion. J. Educ. Bus. 2018, 94, 11–20. [Google Scholar] [CrossRef]
- Houkes, I.; Janssen, P.P.; de Jonge, J.; Bakker, A.B. Specific determinants of intrinsic work motivation, emotional exhaustion and turnover intention: A multisample longitudinal study. J. Occup. Organ. Psychol. 2003, 76, 427–450. [Google Scholar] [CrossRef] [Green Version]
- Gagné, M.; Forest, J.; Vansteenkiste, M.; Crevier-Braud, L.; Broeck, A.V.D.; Aspeli, A.K.; Bellerose, J.; Benabou, C.; Chemolli, E.; Güntert, S.T.; et al. The Multidimensional Work Motivation Scale: Validation evidence in seven languages and nine countries. Eur. J. Work Organ. Psychol. 2014, 24, 178–196. [Google Scholar] [CrossRef]
- Kotera, Y. A qualitative investigation into the experience of neuro-linguistic programming certification training among Japanese career consultants. Br. J. Guid. Couns. 2017, 46, 39–50. [Google Scholar] [CrossRef]
- Kotera, Y.; Ozaki, A.; Miyatake, H.; Tsunetoshi, C.; Nishikawa, Y.; Kosaka, M.; Tanimoto, T. Qualitative Investigation into the Mental Health of Healthcare Workers in Japan during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 568. [Google Scholar] [CrossRef]
- Gerhart, B.; Fang, M. Pay, Intrinsic Motivation, Extrinsic Motivation, Performance, and Creativity in the Workplace: Revisiting Long-Held Beliefs. Annu. Rev. Organ. Psychol. Organ. Behav. 2015, 2, 489–521. [Google Scholar] [CrossRef] [Green Version]
- Taguchi, Y. Factors Forming Work Motivation in Japan. Procedia Manuf. 2015, 3, 717–722. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Sheffield, D. Revisiting the Self-compassion Scale-Short Form: Stronger Associations with Self-inadequacy and Resilience. SN Compr. Clin. Med. 2020, 2, 761–769. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Japanese Workers (n = 165) | |||
|---|---|---|---|
| M | SD | α | |
| Mental Health Problems | 22.29 | 22.93 | 0.96 |
| Self-Compassion | 3.02 | 0.49 | 0.77 |
| Intrinsic Motivation | 3.75 | 1.32 | 0.84 |
| Extrinsic Motivation | 4.10 | 0.82 | 0.80 |
| Amotivation | 2.85 | 1.30 | 0.82 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
|---|---|---|---|---|---|---|---|---|
| 1 | Age | - | ||||||
| 2 | Gender (0 = F, 1 = M) | 0.34 ** | - | |||||
| 3 | Mental Health Problems | −0.18 * | −0.03 | - | ||||
| 4 | Self-Compassion | 0.09 | 0.01 | −0.53 ** | - | |||
| 5 | Intrinsic Motivation | −0.02 | −0.01 | −0.14 | 0.28 ** | - | ||
| 6 | Extrinsic Motivation | −0.04 | −0.10 | −0.06 | 0.11 | 0.67 ** | - | |
| 7 | Amotivation | 0.01 | 0.15 | 0.53 ** | −0.47 ** | −0.33 ** | −0.18 * | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotera, Y.; Asano, K.; Kotera, H.; Ohshima, R.; Rushforth, A. Mental Health of Japanese Workers: Amotivation Mediates Self-Compassion on Mental Health Problems. Int. J. Environ. Res. Public Health 2022, 19, 10497. https://doi.org/10.3390/ijerph191710497
Kotera Y, Asano K, Kotera H, Ohshima R, Rushforth A. Mental Health of Japanese Workers: Amotivation Mediates Self-Compassion on Mental Health Problems. International Journal of Environmental Research and Public Health. 2022; 19(17):10497. https://doi.org/10.3390/ijerph191710497
Chicago/Turabian StyleKotera, Yasuhiro, Kenichi Asano, Hiromasa Kotera, Remi Ohshima, and Annabel Rushforth. 2022. "Mental Health of Japanese Workers: Amotivation Mediates Self-Compassion on Mental Health Problems" International Journal of Environmental Research and Public Health 19, no. 17: 10497. https://doi.org/10.3390/ijerph191710497
APA StyleKotera, Y., Asano, K., Kotera, H., Ohshima, R., & Rushforth, A. (2022). Mental Health of Japanese Workers: Amotivation Mediates Self-Compassion on Mental Health Problems. International Journal of Environmental Research and Public Health, 19(17), 10497. https://doi.org/10.3390/ijerph191710497