
Rare Diseases: Needs and Impact for Patients and Families: A Cross-Sectional Study in the Valencian Region, Spain

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
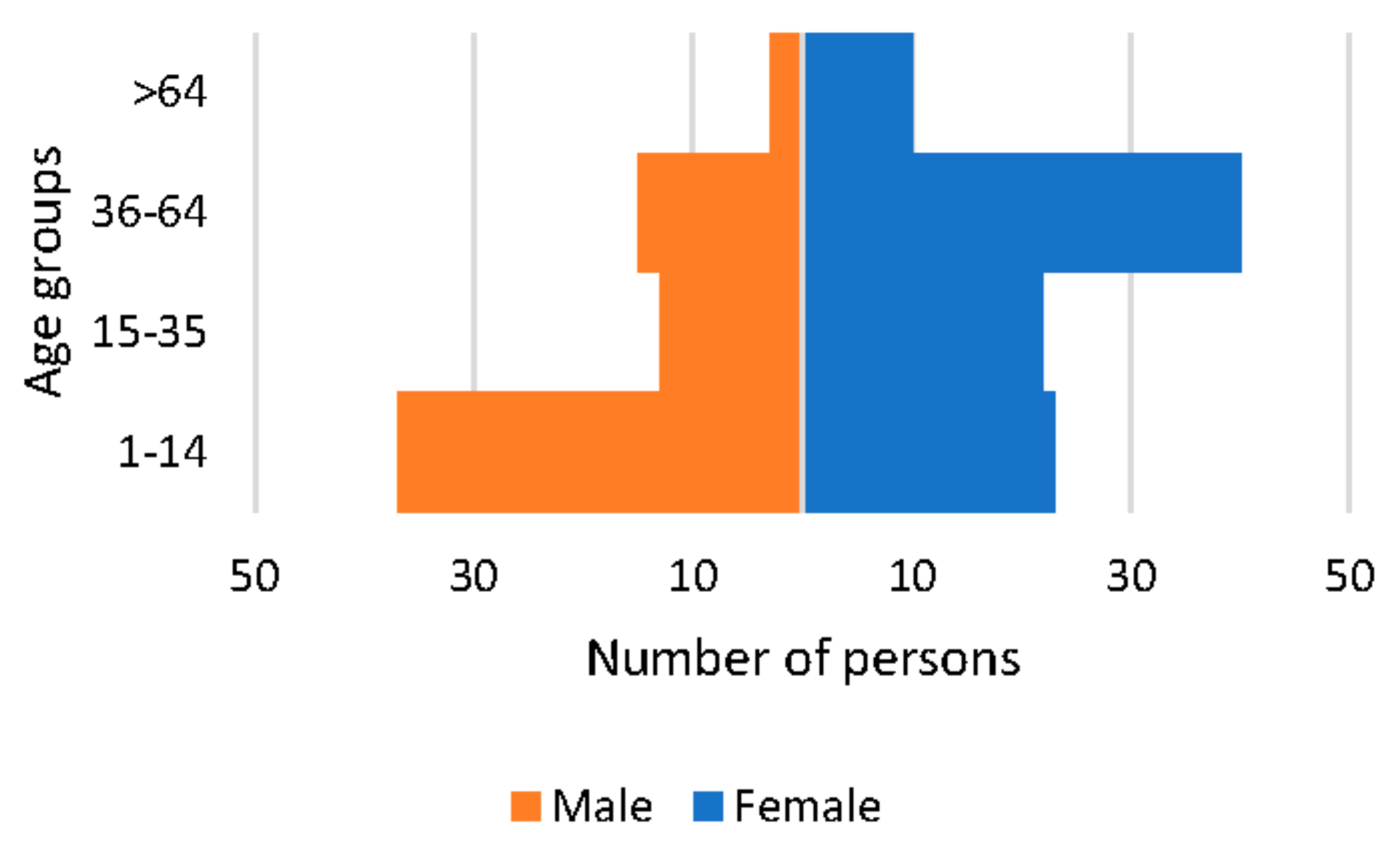
3.1. Socio-Demographic Characteristics
3.2. Socio-Economic Situation of Families with Rare Diseases
- Of the 163 households included, 157 provided information on monthly income. More than half of these families (54.1%) did not exceed €2000, a proportion that rises to 65.5% of families with paediatric patients, compared to 47.5% of families with adult patients (p < 0.05). No statistically significant differences were observed between sex, the existence of a diagnostic delay, or a history of hospitalisation or aggravation.
- There were 138 families who responded to the question about having difficulties in making ends meet, with 33.3% reporting such problems. Statistically significant differences were detected depending on the type of patient (44.2% of families with paediatric patients compared to 26.7% of families with adult patients, p < 0.05) but not according to sex, the existence of a diagnostic delay, hospitalisation, or aggravation.
- There were 148 families who answered the questions related to their ability to pay for possible expenses arising from the RD. Among them, 62.2% of the 148 families could not afford, if needed, other treatments, private psychological therapy, or a caregiver, and up to 36.5% could not afford any of these three needs. The most frequent payment they could not afford was that of a caregiver (60% of the families), with statistically significant differences by type of patient (75% of families with paediatric patients and 51.1% of families with adult patients, p < 0.05) but not by sex, the presence of a delay, or a history of hospitalisation or aggravation.
- Material deprivation could be estimated in 158 families and was detected in a total of 17 households (10.8%): 16.7% of families with a history of hospitalisation compared to 4.3% in families without such a history (p < 0.05). No statistically significant differences were found by type of patient, sex, the existence of a diagnostic delay, or aggravation.
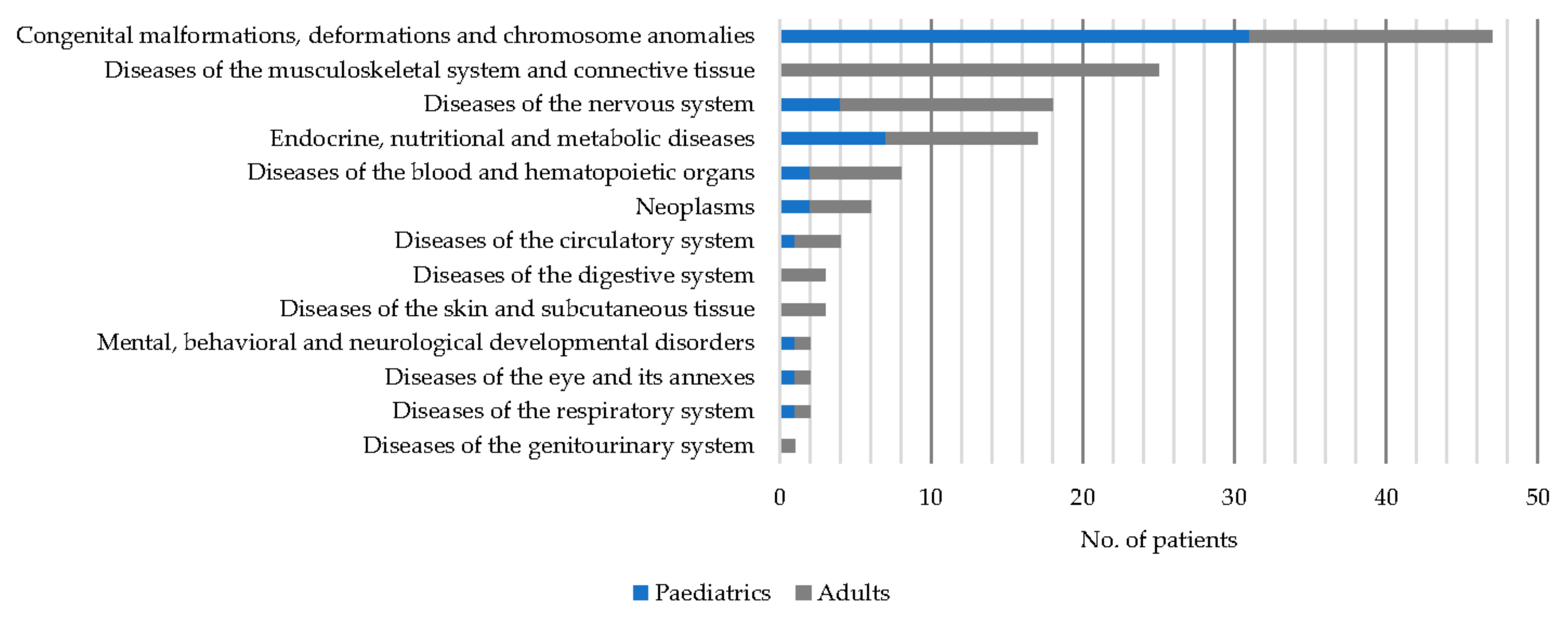
3.3. Diagnostic and Clinical Features
3.4. Treatment
- Adult patients used drugs more frequently than paediatric patients, both before and after diagnosis.
- Patients with a diagnostic delay used drugs and other treatments in the stage prior to diagnostic confirmation more frequently than those without a delay, but after diagnostic confirmation, no statistically significant differences were found in any of the treatments evaluated compared to those without a delay.
- Patients with clinical aggravation consumed more drugs and other treatments both before and after diagnostic confirmation. After diagnosis, they consumed herbal products more frequently than non-aggravated patients.
- Patients with a history of hospitalisation used alternative therapies more frequently after diagnosis than those without prior hospitalisation.
- No statistically significant differences by sex were found.
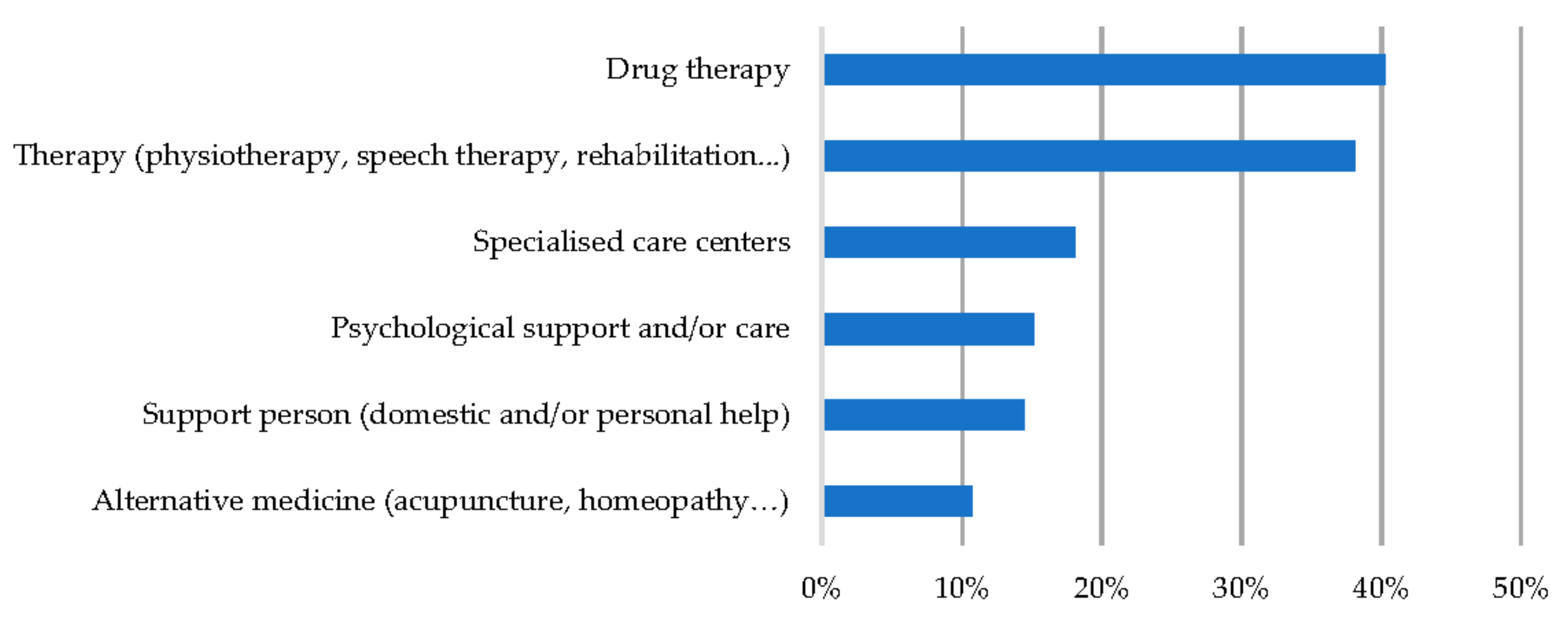
3.5. Expenditures and Unmet Needs Arising from Rare Diseases
- The most frequent expense was pharmacological (40.3% of families) (see Figure 4), with this being more frequent in women (50% compared to 26.9% of men, p < 0.05), in adult patients (40.3% compared to 27.1% of paediatric patients, p < 0.01), in patients with a history of a delayed diagnosis (53.8% compared to 33.9% of patients without a delayed diagnosis, p < 0.05), and in those families with a history of hospitalisation (51.8% vs. 28.4%, p < 0.05) and aggravation (52.2% vs. 31.1%).
- The rest of the expenses, with the exception of specialised care centres, were more frequent among families with aggravation, and expenses for psychological therapy and alternative medicine were also more common among families with a history of hospitalisation (see Table 3).

- All needs, with the exception of health care and medicines, were more frequent among patients with clinical aggravation. Physiotherapy, adaptation of housing and workplace, non-clinical adjuvant therapies, and leisure were also more frequent needs among patients with a history of hospitalisation.
- Lack of medicines or healthcare products was more common among patients with diagnostic delays, where it was also the most frequent need (27.7%).
- No differences were found by type of patient or gender in any of the needs analysed (see Table 3).
3.6. Impact on the Emotional and Social Sphere
4. Discussion
- In general, there were no major differences by sex, except for expenditure and current drug treatment, which were more frequent in women (although in the latter case, the differences were not significant), but this is often the case in the general adult population [25,36]. Mood disorders were also more frequent in women, but unlike in other studies, no greater impact on employment or higher perception of stigmatisation was found [33]. However, it is noteworthy that it was mothers who most frequently completed the survey of paediatric patients, supporting the fact that even today the role of primary caregiver is still predominantly female [37].
- In terms of age, the only significant differences found relate to the worse financial situation of families of paediatric patients (with lower monthly income and somewhat higher disease-related expenses) compared to the households of adult patients, perhaps because in the latter cases some family members, or the patient, receive a pension and a treatment allowance.
- As we had anticipated, patients with a delay in diagnosis of more than one year did not have worse outcomes, except for poorer access to drugs and higher pre-diagnosis consumption. This could be due to the fact that, in the absence of a diagnosis and specific treatment, symptoms are not controlled and thus the patient would initiate a relentless search for different treatments [1,38].
- Finally, it seems that the consequences of RDs have been more frequent in patients who have had a more torpid evolution, with previous hospitalisations and/or aggravation of the disease: all expenses and needs have been more frequent (except for the need for pharmaceutical products and health care, generally covered by the system for dependent patients or pensioners); they have had a higher consumption of medicines and even of alternative therapies after diagnosis; in short, they have experienced a greater impact. Although previous studies also seem to indicate that the use of alternative therapies may be more frequent in chronic patients with a more advanced stage of their disease, others have found no differences in the use of alternative therapies [39,40].
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heuyer, T.; Pavan, S.; Vicard, C. The health and life path of rare disease patients: Results of the 2015 French barometer. Patient Relat. Outcome Meas. 2017, 8, 97–110. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Orlando, V.; Mucherino, S.; Guarino, I.; Guerriero, F.; Trama, U.; Menditto, E. Gender Differences in Medication Use: A Drug Utilization Study Based on Real World Data. Int. J. Environ. Res. Public Health 2020, 17, 3926. [Google Scholar] [CrossRef] [PubMed]
- Wortmann, J.K.; Bremer, A.; Eich, H.; Wortmann, H.K.; Schuster, A.; Fühner, J.; Büntzel, J.; Muecke, R.; Prott, F.; Huebner, J. Use of complementary and alternative medicine by patients with cancer: A cross-sectional study at different points of cancer care. Med. Oncol. 2016, 33, 78. [Google Scholar] [CrossRef]
- Thoene, J.; Crooks, G.M. Report of the National Commission on Orphan Diseases; Public Health Service, Office of the Assistant Secretary of Health: Washington, DC, USA, 1989.
- Avellaneda, A.; Izquierdo, M.; Torrent-Farnell, J.; Ramón, J.R. Enfermedades raras: Enfermedades crónicas que requieren un nuevo enfoque sociosanitario. An. Sist. Sanit. Navar. 2007, 30, 177–190. [Google Scholar] [CrossRef]
- Ting, B.; Tsai, C.-L.; Hsu, W.-T.; Shen, M.-L.; Tseng, P.-T.; Chen, D.T.-L.; Su, K.-P.; Jingling, L. Music Intervention for Pain Control in the Pediatric Population: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 991. [Google Scholar] [CrossRef] [PubMed]
- EURORDIS. The Voice of 12,000 Patients. Experiences and Expectations of Rare Disease Patients on Diagnosis and Care in Europe; Eurordis: Paris, France, 2009; ISBN 9782953031812. [Google Scholar]
- Austin, C.P.; Cutillo, C.M.; Lau, L.P.L.; Jonker, A.H.; Rath, A.; Julkowska, D.; Thomson, D.; Terry, S.F.; De Montleau, B.; Ardigò, D.; et al. Future of Rare Diseases Research 2017–2027: An IRDiRC Perspective. Clin. Transl. Sci. 2018, 11, 21–27. [Google Scholar] [CrossRef]
- Byrne, N.; Turner, J.; Marron, R.; Lambert, D.M.; Murphy, D.N.; O’Sullivan, G.; Mason, M.; Broderick, F.; Burke, M.C.; Casey, S.; et al. The role of primary care in management of rare diseases in Ireland. Ir. J. Med. Sci. 2020, 189, 771–776. [Google Scholar] [CrossRef]
- Molster, C.; Urwin, D.; Di Pietro, L.; Fookes, M.; Petrie, D.; van der Laan, S.; Dawkins, H. Survey of healthcare experiences of Australian adults living with rare diseases. Orphanet J. Rare Dis. 2016, 11, 30. [Google Scholar] [CrossRef]
- González, L.; Estarlich, M.; Murcia, M.; Barreto-Zarza, F.; Santa-Marina, L.; Simó, S.; Larrañaga, M.I.; Ruiz-Palomino, E.; Ibarluzea, J.; Rebagliato, M. Poverty, social exclusion, and mental health: The role of the family context in children aged 7–11 years INMA mother-and-child cohort study. Eur. Child Adolesc. Psychiatry 2021. [Google Scholar] [CrossRef]
- Yan, X.; He, S.; Dong, D. Determining How Far an Adult Rare Disease Patient Needs to Travel for a Definitive Diagnosis: A Cross-Sectional Examination of the 2018 National Rare Disease Survey in China. Int. J. Environ. Res. Public Health 2020, 17, 1757. [Google Scholar] [CrossRef]
- Boettcher, J.; Boettcher, M.; Wiegand-Grefe, S.; Zapf, H. Being the Pillar for Children with Rare Diseases—A Systematic Review on Parental Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 4993. [Google Scholar] [CrossRef] [PubMed]
- Depping, M.K.; Uhlenbusch, N.; von Kodolitsch, Y.; Klose, H.F.E.; Mautner, V.-F.; Löwe, B. Supportive care needs of patients with rare chronic diseases: Multi-method, cross-sectional study. Orphanet J. Rare Dis. 2021, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Pagar o Esperar: Cómo Europa -y España- Tratan la Ansiedad y la Depresión. Available online: https://civio.es/medicamentalia/2021/03/09/acceso-a-la-salud-mental-en-europa-espana/ (accessed on 7 March 2022).
- Sestini, S.; Paneghetti, L.; Lampe, C.; Betti, G.; Bond, S.; Bellettato, C.M.; Maurizio, S. Social and medical needs of rare metabolic patients: Results from a MetabERN survey. Orphanet J. Rare Dis. 2021, 16, 336. [Google Scholar] [CrossRef] [PubMed]
- FEDER. CREER Estudio Sobre Situación de Necesidades Sociosanitarias de las Personas Con Enfermedades Raras en España; FEDER: Madrid, Spain, 2018. [Google Scholar]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Estrategia en Enfermedades Raras del Sistema Nacional de Salud; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2013.
- Kole, A.; Hedley, V. Recommendations from the Rare 2030 Foresight Study: The Future of Rare Diseases Starts Today; RARE 2030: Paris, France, 2021. [Google Scholar]
- Observatorio Sobre Enfermedades Raras. Informe: Termómetro de Necesidades de las Personas Con enfermedades Poco Frecuentes; Federación Española de Enfermedades Raras: Madrid, Spain, 2018. [Google Scholar]
- Black, N.; Martineau, F.; Manacorda, T. Diagnostic Odyssey for Rare Diseases: Exploration of Potential Indicators; Policy Innovation Research Unit (PIRU): London, UK, 2015. [Google Scholar]
- Radin, M.; Foddai, S.G.; Barinotti, A.; Cecchi, I.; Rubini, E.; Sciascia, S.; Roccatello, D. Reducing the diagnostic delay in Antiphospholipid Syndrome over time: A real world observation. Orphanet J. Rare Dis. 2021, 16, 280. [Google Scholar] [CrossRef]
- Phillips, W. Zebras on the Commons: Rare Conditions in Family Practice. J. Am. Board Fam. Pract. 2004, 17, 283–286. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Encuesta Europea de Salud en España 2020; Instituto Nacional de Estadística: Madrid, Spain, 2020. [Google Scholar]
- Gainotti, S.; Mascalzoni, D.; Bros-Facer, V.; Petrini, C.; Floridia, G.; Roos, M.; Salvatore, M.; Taruscio, D. Meeting Patients’ Right to the Correct Diagnosis: Ongoing International Initiatives on Undiagnosed Rare Diseases and Ethical and Social Issues. Int. J. Environ. Res. Public Health 2018, 15, 2072. [Google Scholar] [CrossRef]
- Vicente, E.; Pruneda, L.; Ardanaz, E. Paradoja de la rareza: A propósito del porcentaje de población afectada por enfermedades raras. Gac. Sanit. 2020, 34, 536–538. [Google Scholar] [CrossRef]
- Vega Alonso, A.T.; Zurriaga Llorens, O.; Galmés Truyols, A.; Lozano Alonso, J.E.; Paisán Maestro, L.; Gil Costa, M.; Herrero Llorente, A.; Ramos Aceitero, J.M. Guide to the principles and methods of health sentinel networks in Spain. Gac. Sanit. 2006, 20, 52–60. [Google Scholar] [CrossRef]
- Biasoli, C.; Baldacci, E.; Coppola, A.; De Cristofaro, R.; Di Minno, M.N.D.; Lassandro, G.; Linari, S.; Mancuso, M.E.; Napolitano, M.; Pasta, G.; et al. Promoting physical activity in people with haemophilia: The MEMO (Movement for persons with haEMOphilia) expert consensus project. Blood Transfus. 2022, 20, 66–77. [Google Scholar] [CrossRef]
- European Union Committee of Experts on Rare Diseases. Rare Diseases: Addressing the Need for Specialised Social Services and Integration into Social Policies; European Union Committee of Experts on Rare Diseases: London, UK, 2012. [Google Scholar]
- Bryson, B.; Bogart, K.; Atwood, M.; Fraser, K.; Locke, T.; Pugh, K.; Zerrouk, M. Navigating the unknown: A content analysis of the unique challenges faced by adults with rare diseases. J. Health Psychol. 2021, 26, 623–635. [Google Scholar] [CrossRef]
- Eurostat Glossary: Material Deprivation. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Material_deprivation (accessed on 11 March 2022).
- Paul, M.; Davey, B.; Senf, B.; Stoll, C.; Münstedt, K.; Mücke, R.; Micke, O.; Prott, F.J.; Buentzel, J.; Hübner, J. Patients with advanced cancer and their usage of complementary and alternative medicine. J. Cancer Res. Clin. Oncol. 2013, 139, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Moretti, A.; Cianci, P.; De Paoli, A.; Meroni, F.; Tajè, S.; Mariani, M.; Selicorni, A. Burden of care in families of patients with rare genetic diseases: Analysis of a large Italian cohort. Eur. J. Med. Genet. 2021, 64, 104230. [Google Scholar] [CrossRef] [PubMed]
- Avellaneda Fernández, A.; Pérez Martín, A.; Pombo Allés, G.; Gutiérrez Delgado, E.; Izquierdo Martínez, M. Percepción de las enfermedades raras por el médico de atención primaria. SEMERGEN-Med. Fam. 2011, 38, 421–431. [Google Scholar] [CrossRef] [PubMed]
- EURORDIS. Juggling Care and Daily Life. The Balancing Act of the Rare Disease Community. A Rare Barometer Survey; EURORDIS: Paris, France, 2017. [Google Scholar]
- Llubes-Arrià, L.; Sanromà-Ortíz, M.; Torné-Ruiz, A.; Carillo-Álvarez, E.; García-Expósito, J.; Roca, J. Emotional experience of the diagnostic process of a rare disease and the perception of support systems: A scoping review. J. Clin. Nurs. 2022, 31, 20–31. [Google Scholar] [CrossRef]
- Gaite, L.; García Fuentes, M.; González Lamuño, D.; Alvarez, J. Needs in rare diseases during paediatric age. An. Sist. Sanit. Navar. 2008, 31, 165–175. [Google Scholar]
- Instituto Nacional de Estadística. Nivel y Condiciones de Vida. Encuesta de Presupuestos Familiares 2020; Instituto Nacional de Estadística: Madrid, Spain, 2020. [Google Scholar]
- McMullan, J.; Crowe, A.L.; Bailie, C.; Moore, K.; McMullan, L.S.; Shamandi, N.; McAneney, H.; McKnight, A.J. Improvements needed to support people living and working with a rare disease in Northern Ireland: Current rare disease support perceived as inadequate. Orphanet J. Rare Dis. 2020, 15, 315. [Google Scholar] [CrossRef]
- Evans, W.R.; Rafi, I. Rare diseases in general practice: Recognising the zebras among the horses. Br. J. Gen. Pract. 2016, 66, 550–551. [Google Scholar] [CrossRef]
- Principales Resultados—Portal Estadístico de la Generalitat Valenciana—Generalitat Valenciana. Available online: https://pegv.gva.es/ca/ (accessed on 4 April 2022).
- Gaite, L.; Cantero, P.; González Lamuño, D.; García Fuentes, M. Necesidades de los Pacientes Pediátricos Con Enfermedades Raras y de Sus Familias en Cantabria; Real Patronato sobre Discapacidad: Madrid, Spain, 2005.
- Oviedo, G.R.; Javierre, C.; Font-Farré, M.; Tamulevicius, N.; Carbó-Carreté, M.; Figueroa, A.; Pérez-Testor, S.; Cabedo-Sanromá, J.; Moss, S.J.; Massó-Ortigosa, N.; et al. Intellectual disability, exercise and aging: The IDEA study: Study protocol for a randomized controlled trial. BMC Public Health 2020, 20, 1266. [Google Scholar] [CrossRef]
- Berrocal-Acedo, M.; Benito-Lozano, J.; Alonso-Ferreira, V.; Vilches-Arenas, Á. Diagnostic delay in rare diseases: Systematic review. Rev. Esp. Salud Publica 2022, 96, e202201001. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paediatrics | Adults | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Both Sexes | Male | Female | Both Sexes | Male | Female | Both Sexes | Male | Female | |
| n (%) | 60 (36.8%) ** | 37 (61.7%) | 23 (38.3%) | 103 (6.2%) ** | 31 (30.1%) | 72 (69.9%) | 163 (100%) | 68 (41.7%) | 95 (58.3%) |
| Mean age in years ± sd | 8.28 ± 3.22 | 8.24 ± 3.38 | 8.35 ± 3.02 | 45.08 ± 18.58 | 40.42 ± 20.37 | 47.08 ± 17.53 | 31.53 ± 23.196 | 22.91 ± 21.27 | 37.71 ± 22.64 |
| Confirmed diagnosis (%) | 50 (83.3%) | 32 (86.5%) | 18 (78.3%) | 88 (85.4%) | 26 (83.9%) | 62 (86.1%) | 138 (84.7%) | 58 (85.3%) | 80 (84.2%) |
| Average age (years) at symptom onset ± sd * | 1.46 ± 2.79 | 1.72 ± 2.99 | 1 ± 2.42 | 26.29 ± 20.69 | 21.30 ± 21.02 | 28.38 ± 20.38 | 18.02 ± 20.61 | 11.1 ± 17.58 | 22.83 ± 21.31 |
| Mean age (years) at diagnosis ± sd * | 2.4 ± 3.41 ** | 3.07 ± 3.62 | 1.24 ± 2.73 | 31.83 ± 21.17 | 28.73 ± 23.38 | 33.27 ± 20.12 | 21.11 ± 22.13 ** | 14.98 ± 20.55 | 25.81 ± 22.23 |
| Median time (months) to diagnosis (IQR) * | 5 (0–18) | 7 (0–38.25) | 0 (0–10.5) | 23.5 (5.75–95) | 20 (3–148.25) | 23.5 (9.75–74.75) | 14 (2–65) | 11 (0.5–68.25) | 14 (IQR 4–61.5) |
| Diagnostic delay (%) * | 14 (29.8%) | 12 (40%) | 2(11.8%) | 51 (62.2%) | 14 (53.8%) | 37 (66.1%) | 65 (50.4%) | 26 (46.4%) | 39 (53.4%) |
| Sex (M/F) | Type of Patient (Adult/Paediatric) | Diagnostic Delay (y/n) | Hospitalisation (y/n) | Aggravation (y/n) | ||
|---|---|---|---|---|---|---|
| Before diagnosis | Drug therapy | 25.9%/37.2% | 39.1%/20.4% * | 44.6%/20.6% * | 34.7%/29.0% | 42.6%/23.3% * |
| Other treatments | 24.1%/40.0% | 35.7%/28.6% | 44.4%/21.3% ** | 37.1%/29.0% | 47.5%/21.9% ** | |
| Alternative therapies | 13.8%/15.8% | 17.6%/10.2% | 15.6%/13.1% | 16.9%/12.9% | 20.0%/11.0% | |
| Medicinal plants and/or herbal products | 3.5%/9.2% | 8.2%/4.2% | 7.8%/6.7% | 8.5%/4.9% | 11.7%/2.8% | |
| After diagnosis | Drug therapy | 56.4%/71.1% | 74.7%/47.9% ** | 23.4%/12.9% | 75.7%/53.3% * | 77.6%/55.6% * |
| Other treatments | 50.0%/51.9% | 53.5%/46.9% | 59.4%/43.5% | 54.2%/47.5% | 66.7%/38.4% ** | |
| Alternative therapies | 12.1%/22.1% | 22.1%/10.2% | 23.4%/12.9% | 26.8%/8.1% ** | 25.0%/12.3% | |
| Medicinal plants and/or herbal products | 12.1%/13.2% | 12.9%/12.2% | 12.7%/14.5% | 17.1%/8.1% | 22.0%/5.5% ** |
| Sex (M/F) | Type of Patient (Adult/Paediatric) | Diagnostic Delay (y/n) | Hospitalisation (y/n) | Aggravation (y/n) | ||
|---|---|---|---|---|---|---|
| Expenditures n = 161 | Drug therapy (medicines) | 26.9%/50% * | 48%/27.1% ** | 53.8%/33.9% * | 51.8%/28.4% * | 52.2%/31.1% * |
| Therapy (physiotherapy, speech therapy, rehabilitation) | 44.1%/33.7% | 34%/45% | 37.5%/40.6% | 44.6%/29.7% | 47.8%/28.9% * | |
| Psychological support | 11.8%/17.6% | 15%/15.3% | 18.8%/11.1% | 22.9%/6.8% ** | 25.4%/6.7% ** | |
| Alternative medicine | 7.4%/13.2% | 10%/11.9% | 12.5%/11.1% | 16.9%/4.1% * | 16.4%/5.6% * | |
| Support person | 11.8%/16.5% | 18%/8.5% | 20.3%/11.1% | 19.3%/9.5% | 22.4%/8.9% * | |
| Specialised centre | 14.7%/20.7% | 15.8%/22% | 20%/22.2% | 22.6%/12.2% | 22.1%/13.3% | |
| Unmet needs n = 159 | Medical treatment/health care | 11.9%/19.6% | 20%/10.2% | 26.2%/12.9% | 19.3%/13.5% | 19.4%/13.3% |
| Psychological support | 20.9%/23.9% | 20%/27.1% | 24.6%/16.1% | 27.7%/17.6% | 31.3%/15.6% * | |
| Physiotherapy | 23.9%/22.8% | 25%/20.3% | 24.6%/21% | 30.1%/16.2% * | 35.8%/13.3% ** | |
| Medicines and other healthcare products | 14.9%/19.6% | 19%/15.3% | 27.7%/12.9% * | 19.3%/16.2% | 22.4%/13.3% | |
| Orthopaedics | 16.4%/13% | 12%/18.6% | 7.9%/8.7% | 19.3%/9.5% | 22.4%/7.8% ** | |
| Personal support | 10.4%/13% | 14%/8.5% | 10.8%/11.3% | 15.7%/8.1% | 17.9%/6.7% * | |
| Adaptation of housing | 13.4%/12% | 14%/10.2% | 12.3%/12.9% | 18.1%/6.8% * | 22.4%/4.4% ** | |
| Adaptation of workplace | 9%/16.3% | 15%/10.2% | 16.9%/8.1% | 19.3%/6.8% * | 26.9%/2.2% ** | |
| Non-clinical adjuvant therapies | 25.4%/27.2% | 24%/30.5% | 26.2%/25.8% | 36.1%/16.2% ** | 44.8%/12.2% ** | |
| Leisure and free time | 19.4%/20.7% | 20%/20.3% | 20%/21% | 27.7%/12.2% * | 32.8%/10% ** | |
| Other | 7.5%/8.8% | 7%/10.3% | 4.6%/9.8% | 9.8%/6.8% | 11.9%/5.6% | |
| Impacts n = 155 | Travel to other health centres | 55.9%/55.2% | 58%/55.9% | 64.1%/60.3% | 71.4%/41.1% ** | 73.5%/43.8% ** |
| Employment repercussions | 32.4%/45.7% | 44.6%/32.2% | 43.1%/41.3% | 57.1%/21.6% ** | 58.8%/25.6% ** | |
| Disruption of personal relationships | 41.2%/56.5% | 55.4%/40.7% | 55.4%/50.8% | 69%/28.4% ** | 76.5%/28.9% ** | |
| Disruption of relationship with partner | 16.4%/13.2% | 17%/10.3% | 24.6%/11.5% | 23.2%/5.4% ** | 20.9%/10% | |
| Mood disruption | 48.5%/65.2% * | 65.3%/45.8% * | 56.9%/63.5% | 72.6%/40.5% ** | 79.4%/41.1% ** | |
| Disruption of daily routine | 58.8%/59.8% | 62.4%/54.2% | 61.5%/65.1% | 76.2%/40.5% ** | 80.9%/43.3% ** | |
| Reduced social network | 25%/37% | 36.6%/23.7% | 36.9%/30.2% | 44%/18.9% ** | 50%/17.8% ** | |
| Discrimination | 22.1%/25% | 25.7%/20.3% | 27.7%/25.4% | 32.1%/14.9% * | 33.8%/16.7% * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gimenez-Lozano, C.; Páramo-Rodríguez, L.; Cavero-Carbonell, C.; Corpas-Burgos, F.; López-Maside, A.; Guardiola-Vilarroig, S.; Zurriaga, O. Rare Diseases: Needs and Impact for Patients and Families: A Cross-Sectional Study in the Valencian Region, Spain. Int. J. Environ. Res. Public Health 2022, 19, 10366. https://doi.org/10.3390/ijerph191610366
Gimenez-Lozano C, Páramo-Rodríguez L, Cavero-Carbonell C, Corpas-Burgos F, López-Maside A, Guardiola-Vilarroig S, Zurriaga O. Rare Diseases: Needs and Impact for Patients and Families: A Cross-Sectional Study in the Valencian Region, Spain. International Journal of Environmental Research and Public Health. 2022; 19(16):10366. https://doi.org/10.3390/ijerph191610366
Chicago/Turabian StyleGimenez-Lozano, Cristina, Lucía Páramo-Rodríguez, Clara Cavero-Carbonell, Francisca Corpas-Burgos, Aurora López-Maside, Sandra Guardiola-Vilarroig, and Oscar Zurriaga. 2022. "Rare Diseases: Needs and Impact for Patients and Families: A Cross-Sectional Study in the Valencian Region, Spain" International Journal of Environmental Research and Public Health 19, no. 16: 10366. https://doi.org/10.3390/ijerph191610366
APA StyleGimenez-Lozano, C., Páramo-Rodríguez, L., Cavero-Carbonell, C., Corpas-Burgos, F., López-Maside, A., Guardiola-Vilarroig, S., & Zurriaga, O. (2022). Rare Diseases: Needs and Impact for Patients and Families: A Cross-Sectional Study in the Valencian Region, Spain. International Journal of Environmental Research and Public Health, 19(16), 10366. https://doi.org/10.3390/ijerph191610366