
Health-Related Quality of Life and Perceived Burden of Informal Caregivers of Patients with Rare Diseases in Selected European Countries

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Measures
2.2.1. Caregiver Burden and Informal Care
2.2.2. Health-Related Quality of Life
2.2.3. Other Information
2.3. Statistical Analysis
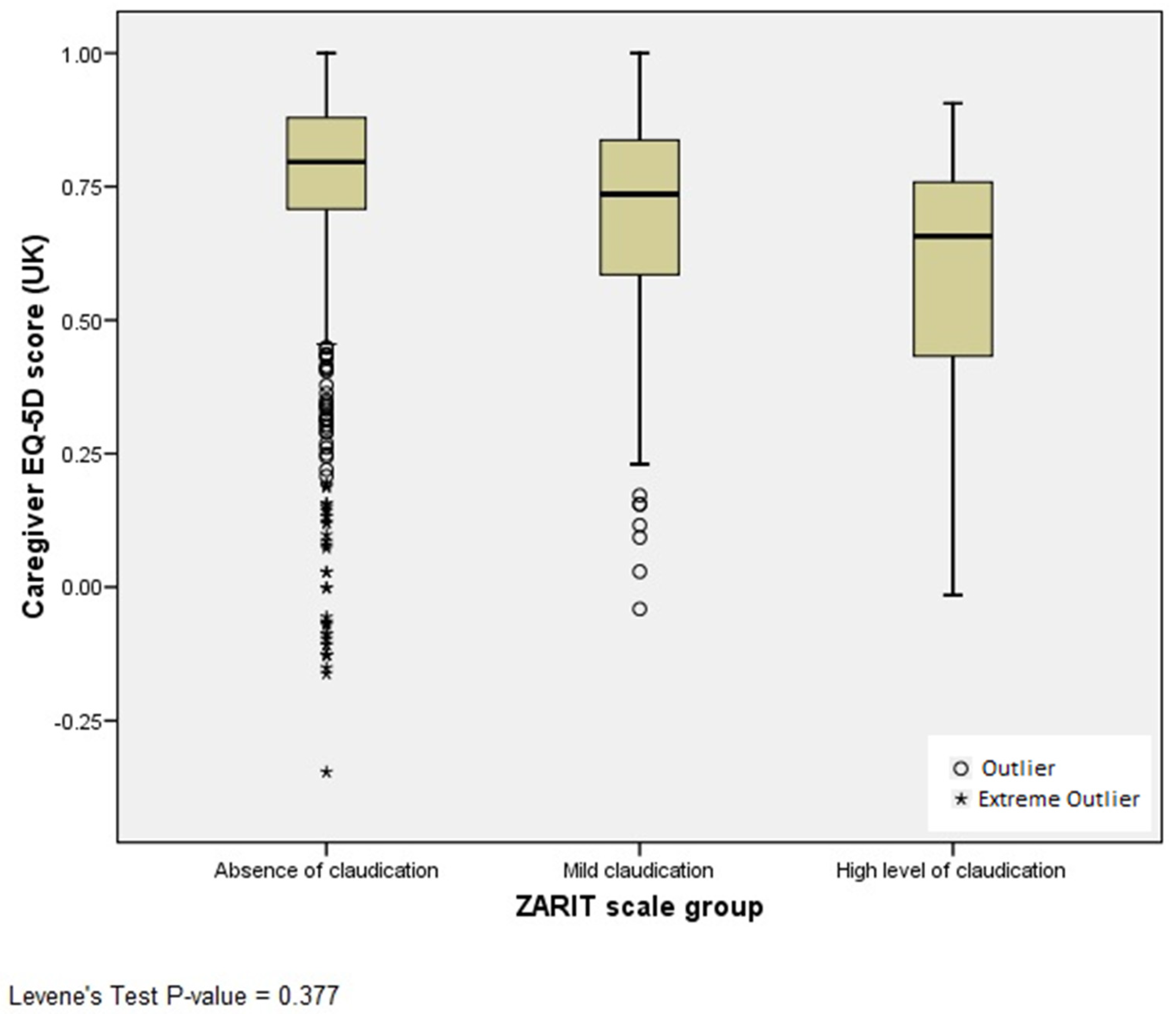
2.3.1. The EQ-5D Capacity to Discriminate HRQOL between Caregivers’ Burden Groups
2.3.2. Factors Related to Caregivers’ HRQOL
3. Results
3.1. The EQ-5D Capacity to Discriminate HRQOL between Caregivers’ Burden Groups
3.2. Factors Related to Caregivers’ HRQOL
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions on Rare Diseases: Europe’s Challenges, (2009/C151/02). Available online: http://ec.europa.eu/health/ph_threats/non_com/docs/rare_com_en.pdf (accessed on 15 January 2018).
- Faurisson, F. Survey of the Delay in Diagnosis for 8 Rare Diseases in Europe, 2004: EurordisCare2. European Organisation for Rare Diseases Web Site. Available online: http://www.eurordis.org/sites/default/files/publications/Fact_Sheet_Eurordiscare2.pdf (accessed on 15 January 2018).
- Alonso, V.; Villaverde-Hueso, A.; Hens, M.; Morales-Piga, A.; Abaitua, I.; Posada de la Paz, M. Public health research on rare diseases. Georgian Med. News 2011, 193, 11–16. [Google Scholar]
- Kanters, T.A.; van der Ploeg, A.T.; Brouwer, W.B.; Hakkaart, L. The impact of informal care for patients with Pompe disease: An application of the CarerQol instrument. Mol. Genet. Metab. 2013, 110, 281–286. [Google Scholar] [CrossRef]
- Buhse, M. Assessment of caregiver burden in families of persons with multiple sclerosis. J. Neurosci. Nurs. 2008, 40, 25–31. [Google Scholar] [CrossRef]
- Michalik, J. Rare diseases and the quality of life of caregivers. Soc. Welf. Interdiscip. Approach 2012, 2, 8–17. [Google Scholar]
- Landfeldt, E.; Lindgren, P.; Bell, C.F.; Guglieri, M.; Straub, V.; Lochmüller, H.; Bushby, K. Quantifying the burden of caregiving in Duchenne muscular dystrophy. J. Neurol. 2016, 263, 906–915. [Google Scholar] [CrossRef] [Green Version]
- Litzelman, K.; Skinner, H.G.; Gangnon, R.E.; Nieto, F.J.; Malecki, K.; Witt, W.P. The relationship among caregiving characteristics, caregiver strain, and health-related quality of life: Evidence from the Survey of the Health of Wisconsin. Qual. Life Res. 2015, 24, 1397–1406. [Google Scholar] [CrossRef] [Green Version]
- Carod-Artal, F.J.; Mesquita, H.M.; Ziomkowski, S.; Martinez-Martin, P. Burden and health-related quality of life among caregivers of Brazilian Parkinson’s disease patients. Parkinsonism Relat. Disord. 2013, 19, 943–948. [Google Scholar] [CrossRef]
- Klassen, A.F.; Raina, P.; McIntosh, C.; Sung, L.; Klaassen, R.J.; O’Donnell, M.; Yanofsky, R.; Dix, D. Parents of children with cancer: Which factors explain differences in health-related quality of life. Int. J. Cancer 2011, 129, 1190–1198. [Google Scholar] [CrossRef]
- Li, T.C.; Lee, Y.D.; Lin, C.C.; Amidon, R.L. Quality of life of primary caregivers of elderly with cerebrovascular disease or diabetes hospitalized for acute care: Assessment of well-being and functioning using the SF-36 health questionnaire. Qual. Life Res. 2004, 13, 1081–1088. [Google Scholar] [CrossRef]
- Serrano-Aguilar, P.G.; Lopez-Bastida, J.; Yanes-Lopez, V. Impact on health-related quality of life and perceived burden of informal caregivers of individuals with Alzheimer’s disease. Neuroepidemiology 2006, 27, 136–142. [Google Scholar] [CrossRef]
- Rivera-Navarro, J.; Benito-León, J.; Oreja-Guevara, C.; Pardo, J.; Dib, W.B.; Orts, E.; Belló, M.; Caregiver Quality of Life in Multiple Sclerosis (CAREQOL-MS) Study Group. Burden and health-related quality of life of Spanish caregivers of persons with multiple sclerosis. Mult. Scler. J. 2009, 15, 1347–1355. [Google Scholar] [CrossRef]
- Bleijlevens, M.H.; Stolt, M.; Stephan, A.; Zabalegui, A.; Saks, K.; Sutcliffe, C.; Lethin, C.; Soto, M.E.; Zwakhalen, S.M.; RightTimePlaceCare Consortium. Changes in caregiver burden and health-related quality of life of informal caregivers of older people with Dementia: Evidence from the European RightTimePlaceCare prospective cohort study. J. Adv. Nurs. 2014, 71, 1378–1391. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Guide to the Methods of Technology Appraisal; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- Reed, C.; Barret, A.; Lebrec, J.; Dodel, R.; Jones, R.W.; Vellas, B.; Wimo, A.; Argimon, J.M.; Bruno, G.; Haro, J.M. How useful is the EQ-5D in assessing the impact of caring for people with Alzheimer’s disease? Health Qual. Life Outcomes 2017, 15, 16. [Google Scholar] [CrossRef] [Green Version]
- Linertová, R.; Serrano-Aguilar, P.; Posada-de-la-Paz, M.; Hens-Pérez, M.; Kanavos, P.; Taruscio, D.; Schieppati, A.; Stefanov, R.; Péntek, M.; Delgado, C.; et al. Delphi approach to select rare diseases for a European representative survey. The BURQOL-RD study. Health Policy 2012, 108, 19–26. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Hérbert, R.; Bravo, G.; Préville, M. Reliability, validity, and reference values of the Zarit Burden Interview for assessing informal caregivers of community-dwelling older persons with dementia. Can. J. Aging 2000, 19, 494–507. [Google Scholar]
- Mar, J.; Arrospide, A.; Begiristain, J.M.; Larrañaga, I.; Sanz-Guinea, A.; Quemada, I. Quality of life and burden of carers of patients with acquired brain injury. Rev. Esp. Geriatr. Gerontol. 2011, 46, 200–205. [Google Scholar] [CrossRef]
- The EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Wille, N.; Badia, X.; Bonsel, G.; Burström, K.; Cavrini, G.; Devlin, N.; Egmar, A.C.; Greiner, W.; Gusi, N.; Herdman, M.; et al. Development of the EQ-5D-Y: A child-friendly version of the EQ-5D. Qual. Life Res 2010, 19, 875–886. [Google Scholar] [CrossRef] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Van Hout, B.; Janssen, M.F.; Feng, Y.S.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Craig, B.M.; Greiner, W.; Brown, D.S.; Reeve, B.B. Valuation of child health-related quality of life in the United States. Health Econ. 2016, 25, 768–777. [Google Scholar] [CrossRef]
- Greene, W.H. Econometric Analysis; Prentice Hall: London, UK, 1997. [Google Scholar]
- Long, J.S. Regression Models for Categorical and Limited Dependent Variables; SAGE: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- StataCorp. Stata Statistical Software; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Morimoto, T.; Schreiner, A.S.; Asano, H. Caregiver burden and health-related quality of life among Japanese stroke caregivers. Age Ageing 2003, 32, 218–223. [Google Scholar] [CrossRef] [Green Version]
- Crossnohere, N.L.; Fischer, R.; Lloyd, A.; Prosser, L.A.; Bridges, J. Assessing the Appropriateness of the EQ-5D for Duchenne Muscular Dystrophy: A Patient-Centered Study. Med. Decis. Mak. 2021, 41, 209–221. [Google Scholar] [CrossRef]
- Antoniadi, A.; Galvin, M.; Heverin, M.; Hardiman, O.; Mooney, C. Prediction of caregiver quality of life in amyotrophic lateral sclerosis using explainable machine learning. Sci. Rep. 2021, 10, 12237. [Google Scholar] [CrossRef]
- Kim, K.R.; Lee, E.; Namkoong, K.; Lee, Y.M.; Lee, J.S.; Kim, H.D. Caregiver’s burden and quality of life in mitochondrial disease. Pediatr. Neurol. 2010, 42, 271–276. [Google Scholar] [CrossRef]

{kind=link}
| France (N = 147) | Germany (N = 124) | Italy (N = 229) | Spain (N = 221) | Sweden (N = 28) | UK (N = 76) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Caregivers | Patients | Caregivers | Patients | Caregivers | Patients | Caregivers | Patients | Caregivers | Patients | Caregivers | Patients | |
| Female, N (%) | 121 (82.3%) | 53 (36.1%) | 110 (88.7%) | 59 (47.6%) | 162 (70.7%) | 73 (31.9%) | 182 (82.4%) | 79 (35.7%) | 18 (64.3%) | 14 (50%) | 69 (90.8%) | 30 (39.5%) |
| Age, mean ± sd | NA | 22.83 ± 15.59 | NA | 30.48 ± 13.18 | NA | 35.54 ± 16.70 | NA | 31.08 ± 14.06 | NA | 34.14 ± 12.43 | NA | 31.30 ± 11.45 |
| EQ-5D index (UK), mean ± sd | 0.715 ± 0.256 | 0.499 ± 0.284 | 0.619 ± 0.344 | 0.235 ± 0.271 | 0.736 ± 0.255 | 0.225 ± 0.325 | 0.702 ± 0.257 | 0.335 ± 0.306 | 0.625 ± 0.314 | 0.451 ± 0.245 | 0.787 ± 0.240 | 0.239 ± 0.297 |
| EQ-VAS, mean ± sd | 74.35 ± 20.18 | 64.55 ± 20.62 | 74.71 ± 15.86 | 64.35 ± 21.71 | 76.67 ± 17.12 | 61.43 ± 21.16 | 71.89 ± 18.00 | 63.94 ± 21.00 | 72.30 ± 17.90 | 65.61 ± 15.67 | 77.37 ± 18.56 | 63.13 ± 19.01 |
| ZBI, N (%) | ||||||||||||
| Absence of claudication | 103 (70.1%) | -- | 115 (92.7%) | -- | 209 (91.3%) | -- | 179 (81%) | -- | 23 (82.1%) | -- | 64 (84.2%) | -- |
| Mild claudication | 29 (19.7%) | -- | 9 (7.3%) | -- | 16 (7.0%) | -- | 23 (10.4%) | -- | 4 (14.3%) | -- | 8 (10.5%) | -- |
| High level of claudication | 15 (10.2%) | -- | 0 (0%) | -- | 4 (1.7%) | -- | 19 (8.6%) | -- | 1 (3.6%) | -- | 4 (5.3%) | -- |
| Caregivers | Patients | |
|---|---|---|
| Female, N (%) | 662 (80.2%) | 516 (62.5%) |
| Age, mean ± sd | NA | 14.93 ± 14.18 |
| EQ-5D index (UK), mean ± sd | 0.737 ± 0.244 | 0.324 ± 0.313 |
| EQ-5D index (Spain), mean ± sd | 0.773 ± 0.268 | 0.290 ± 0.378 |
| EQ-5D index (France), mean ± sd | 0.735 ± 0.282 | 0.221 ± 0.312 |
| EQ-VAS, mean ± sd | 75.52 ± 17.79 | 63.00 ± 20.47 |
| Years of caring, mean ± sd | 9.01 ± 9.46 | -- |
| NHS Satisfaction, mean ± sd | -- | 6.54 ± 2.32 |
| Relationship to patient, N (%) | ||
| Spouse | 166 (20.1%) | -- |
| Son/Daughter | 224 (27.2%) | -- |
| Mother/Father | 405 (49.1%) | -- |
| Other | 30 (3.6%) | -- |
| Working situation, N (%) | ||
| Employed | 455 (55.1%) | -- |
| Retired or pensioner | 69 (8.4%) | -- |
| House wife/House husband | 241 (29.2%) | -- |
| No reply | 60 (7.3%) | -- |
| ZBI, N (%) | ||
| Absence of claudication | 693 (84%) | -- |
| Mild claudication | 89 (10.8%) | -- |
| High level of claudication | 43 (5.2%) | -- |
| Care hours per week (main carer), mean ± sd | 54.65 ± 35.93 | -- |
| Care hours per week (other carers), mean ± sd | 20.16 ± 0.28 | -- |
| Problem | Mobility | Self-Care | Usual Activities | Pain/Discomfort | Anxiety/Depression |
|---|---|---|---|---|---|
| No problems | 643 (77.9%) | 669 (81.1%) | 518 (62.8%) | 366 (44.4%) | 324 (39.3%) |
| Slight problems | 94 (11.4%) | 62 (7.5%) | 156 (18.9%) | 276 (33.5%) | 301 (36.5%) |
| Moderate problems | 46 (5.6%) | 44 (5.3%) | 101 (12.2%) | 144 (17.5%) | 145 (17.6%) |
| Severe problems | 21 (2.5%) | 15 (1.8%) | 35 (4.2%) | 34 (4.1%) | 40 (4.8%) |
| Extreme problems | 21 (2.5%) | 35 (4.2%) | 15 (1.8%) | 5 (0.6%) | 15 (1.8%) |
| Mobility | Self-Care | Usual Activities | Pain/Discomfort | Anxiety/Depression | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Slight Problems | Moderate Problems | Severe Problems + Unable/Extreme Problems | Slight Problems | Moderate Problems | Severe Problems + Unable/Extreme Problems | Slight Problems | Moderate Problems | Severe Problems + Unable/Extreme Problems | Slight Problems | Moderate Problems | Severe Problems + Extreme Problems | Slight Problems | Moderate Problems | Severe Problems + Extreme Problems | |
| Patient age | 1.008 (0.010) | 1.021 (0.132) | 1.047 ** (0.150) | 0.978 (0.015) | 1.009 (0.130) | 1.020 (0.160) | 0.976 * (0.010) | 1.009 (0.010) | 1.007 (0.144) | 0.999 (0.008) | 1.023 * (0.010) | 1.061 ** (0.015) | 0.990 (0.008) | 1.016 (0.010) | 1.026 (0.137) |
| Satisfaction with NHS | 0.993 (0.057) | 1.046 (0.087) | 1.108 (0.104) | 1.029 (0.768) | 1.014 (0.077) | 1.031 (0.101) | 0.989 (0.051) | 1.010 (0.060) | 1.061 (0.089) | 0.959 (0.043) | 0.969 (0.054) | 1.066 (0.097) | 0.995 (0.046) | 0.915 (0.053) | 0.848 * (0.065) |
| Hours/week other caregiver | 1.007 (0.005) | 0.999 (0.007) | 1.016 * (0.006) | 1.011 (0.006) | 1.006 (0.006) | 1.009 (0.007) | 1.000 (0.004) | 1.005 (0.005) | 1.011 (0.005) | 1.006 (0.004) | 1.004 (0.005) | 1.006 (0.008) | 0.999 (0.004) | 0.995 (0.005) | 0.993 (0.007) |
| Years of caring | |||||||||||||||
| 0 to 5 years | 1.221 (0.420) | 1.800 (0.845) | 2.044 (1.041) | 2.701 * (1.285) | 0.695 (0.327) | 2.276 (1.284) | 0.754 (0.231) | 0.748 (0.270) | 1.464 (0.680) | 0.630 (0.166) | 0.943 (0.298) | 1.189 (0.632) | 1.016 (0.268) | 1.228 (0.397) | 1.108 (0.516) |
| 5 to 10 years | 1.385 (0.469) | 1.746 (0.875) | 2.589 (1.289) | 3.870 ** (1.740) | 1.385 (0.588) | 3.356 * (1.844) | 1.303 (0.386) | 1.637 (0.543) | 1.434 (0.707) | 0.683 (0.181) | 0.957 (0.311) | 1.389 (0.753) | 0.961 (0.247) | 0.661 (0.238) | 0.682 (0.352) |
| Caregiver working situation | |||||||||||||||
| Employed | 0.845 (0.244) | 0.643 (0.262) | 0.750 (0.330) | 1.427 (0.520) | 0.849 (0.322) | 1.039 (0.488) | 1.080 (0.270) | 1.565 (0.463) | 0.696 (0.284) | 0.615 * (0.135) | 1.170 (0.314) | 0.456 (0.214) | 1.261 (0.279) | 1.050 (0.297) | 0.873 (0.345) |
| ZBI | |||||||||||||||
| Absence of claudication | 0.469 (0.218) | 1.443 (1.533) | 0.986 (0.881) | 0.283 * (0.145) | 0.899 (0.713) | 0.627 (0.539) | 0.376 * (0.162) | 0.476 (0.267) | 0.246 * (0.148) | 1.268 (0.553) | 0.602 (0.285) | 0.307 (0.232) | 0.259 * (0.170) | 0.085 ** (0.059) | 0.031 ** (0.022) |
| Caregiver sex | |||||||||||||||
| Female | 0.868 (0.302) | 1.019 (0.450) | 0.723 (0.340) | 0.818 (0.348) | 0.446 * (0.184) | 0.515 (0.251) | 1.296 (0.425) | 0.884 (0.296) | 0.629 (0.280) | 1.376 (0.361) | 1.729 (0.567) | 1.446 (0.772) | 2.107 ** (0.560) | 1.310 (0.423) | 1.688 (0.814) |
| Patient sex | |||||||||||||||
| Female | 0.303 ** (0.085) | 0.955 (0.391) | 1.531 (0.727) | 0.492 * (0.173) | 0.899 (0.342) | 1.761 (0.920) | 0.621 (0.151) | 0.723 (0.211) | 1.256 (0.539) | 0.668 (0.147) | 0.752 (0.204) | 0.558 (0.249) | 0.800 (0.174) | 1.318 (0.387) | 0.999 (0.397) |
| Patient utility index | 0.818 (0.093) | 0.854 (0.138) | 0.579 ** (0.079) | 1.062 (0.173) | 0.857 (0.113) | 0.713 * (0.101) | 0.914 (0.092) | 0.771 * (0.083) | 0.774 (0.104) | 0.784 * (0.087) | 0.570 ** (0.067) | 0.501 ** (0.088) | 0.991 (0.091) | 0.900 (0.099) | 0.887 (0.143) |
| AIC | 876.67 | 773.70 | 1151.69 | 1300.89 | 1319.27 | ||||||||||
| BIC | 1057.46 | 954.48 | 1332.47 | 1481.68 | 1500.05 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valcárcel-Nazco, C.; Ramallo-Fariña, Y.; Linertová, R.; Ramos-Goñi, J.M.; García-Pérez, L.; Serrano-Aguilar, P. Health-Related Quality of Life and Perceived Burden of Informal Caregivers of Patients with Rare Diseases in Selected European Countries. Int. J. Environ. Res. Public Health 2022, 19, 8208. https://doi.org/10.3390/ijerph19138208
Valcárcel-Nazco C, Ramallo-Fariña Y, Linertová R, Ramos-Goñi JM, García-Pérez L, Serrano-Aguilar P. Health-Related Quality of Life and Perceived Burden of Informal Caregivers of Patients with Rare Diseases in Selected European Countries. International Journal of Environmental Research and Public Health. 2022; 19(13):8208. https://doi.org/10.3390/ijerph19138208
Chicago/Turabian StyleValcárcel-Nazco, Cristina, Yolanda Ramallo-Fariña, Renata Linertová, Juan Manuel Ramos-Goñi, Lidia García-Pérez, and Pedro Serrano-Aguilar. 2022. "Health-Related Quality of Life and Perceived Burden of Informal Caregivers of Patients with Rare Diseases in Selected European Countries" International Journal of Environmental Research and Public Health 19, no. 13: 8208. https://doi.org/10.3390/ijerph19138208
APA StyleValcárcel-Nazco, C., Ramallo-Fariña, Y., Linertová, R., Ramos-Goñi, J. M., García-Pérez, L., & Serrano-Aguilar, P. (2022). Health-Related Quality of Life and Perceived Burden of Informal Caregivers of Patients with Rare Diseases in Selected European Countries. International Journal of Environmental Research and Public Health, 19(13), 8208. https://doi.org/10.3390/ijerph19138208