
A Mixed-Methods Participatory Intervention Design Process to Develop Intervention Options in Immediate Food and Built Environments to Support Healthy Eating and Active Living among Children and Adolescents in Cameroon and South Africa

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Study Aim and Objectives
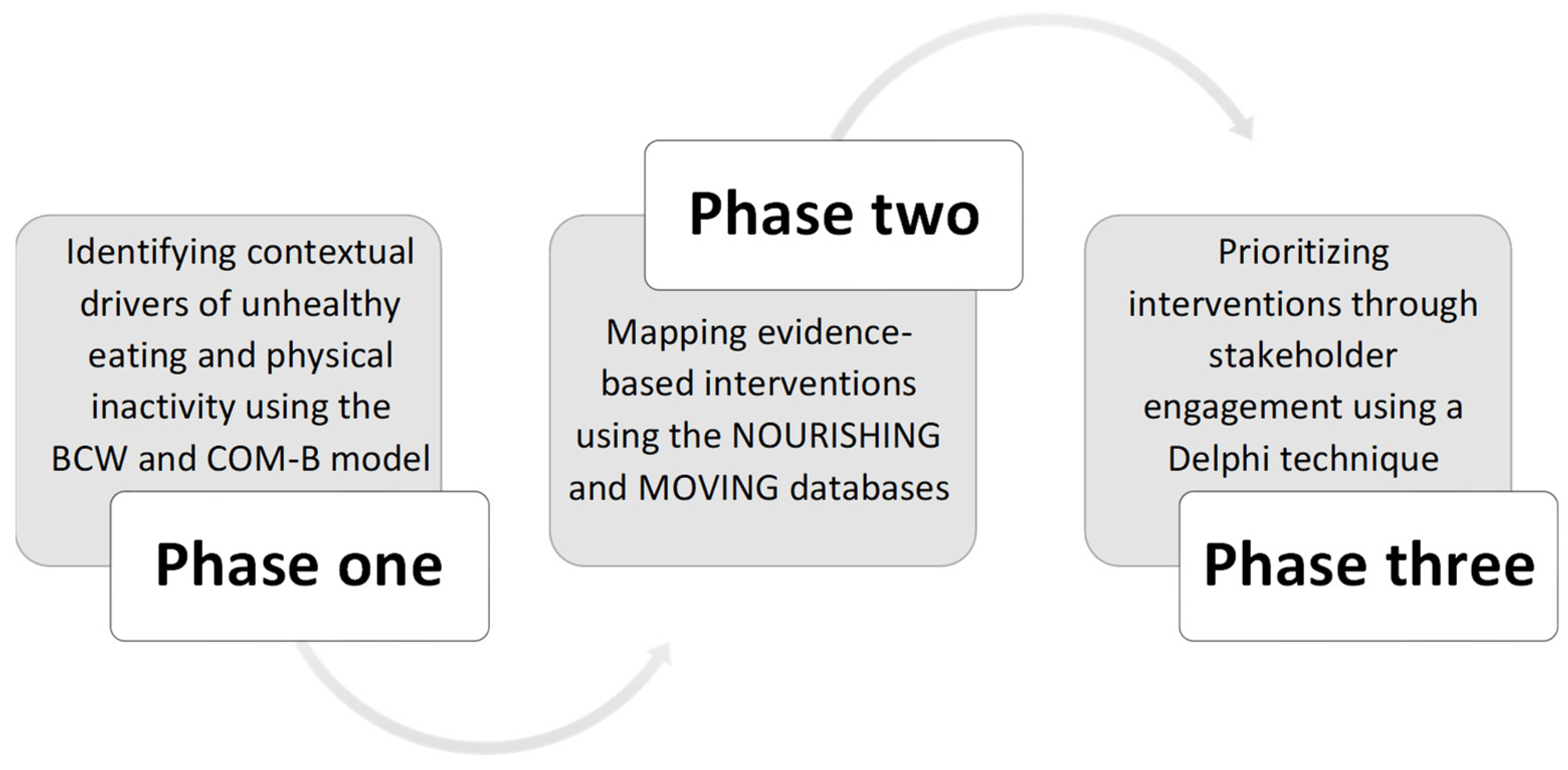
- Identify contextual drivers of unhealthy eating and physical inactivity in children and adolescents’ immediate environments;
- Map evidence-based interventions to address contextual drivers of unhealthy eating and physical inactivity in children and adolescents;
- Prioritize evidence-based interventions to address a spectrum of underlying factors influencing unhealthy eating and physical inactivity in children and adolescents through stakeholder engagement.
3. Materials and Methods
3.1. Study Settings and Design
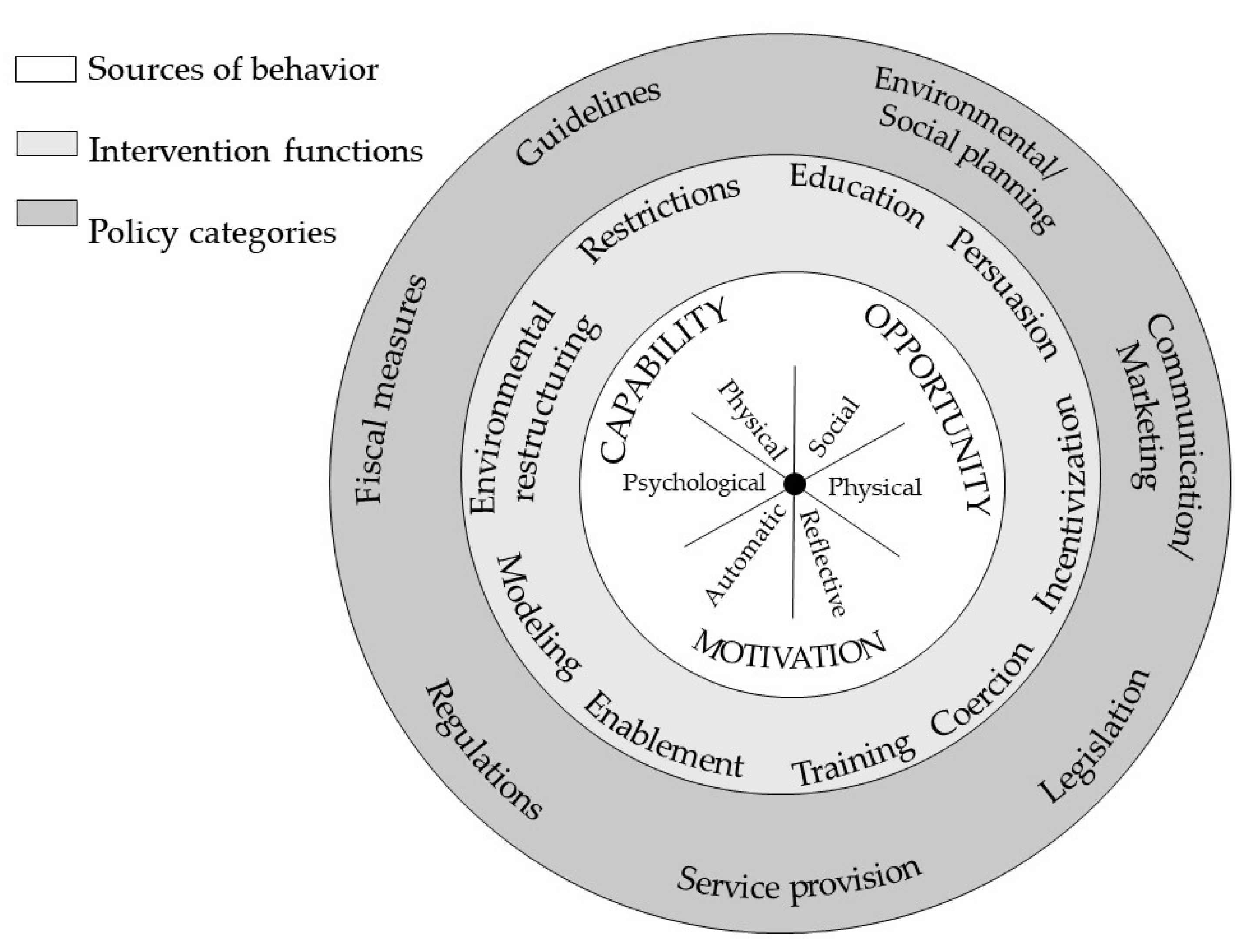
3.2. Phase One—Identify Drivers in Behavioral Terms
3.3. Phase Two—Intervention Mapping
3.4. Phase Three—Prioritizing Interventions
4. Reflections on the Study Design and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood Obesity: Causes, Consequences, and Management. Pediatr. Clin. N. Am. 2015, 62, 821–840. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.; Aggarwal, A.; Walls, H.; Herforth, A.; Drewnowski, A.; Coates, J.; Kalamatianou, S.; Kadiyala, S. Concepts and critical perspectives for food environment research: A global framework with implications for action in low- and middle-income countries. Glob. Food Secur. 2018, 18, 93–101. [Google Scholar] [CrossRef]
- Huang, T.T.; Drewnosksi, A.; Kumanyika, S.; Glass, T.A. A systems-oriented multilevel framework for addressing obesity in the 21st century. Prev. Chronic Dis. 2009, 6, A82. [Google Scholar] [PubMed]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 8 March 2022).
- Ford, N.D.; Patel, S.A.; Narayan, K.M.V. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef]
- Pacific, R.; Martin, H.D.; Kulwa, K.; Petrucka, P. Contribution of Home and School Environment in Children’s Food Choice and Overweight/Obesity Prevalence in African Context: Evidence for Creating Enabling Healthful Food Environment. Pediatric Health Med. Ther. 2020, 11, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Leandro, C.G.; Fonseca EV da S da de Lim, C.R.; Tchamo, M.E.; Ferreira-e-Silva, W.T. Barriers and Enablers That Influence Overweight/Obesity/Obesogenic Behavior in Adolescents from Lower-Middle Income Countries: A Systematic Review. Food Nutr. Bull. 2019, 40, 562–571. [Google Scholar] [CrossRef]
- Trübswasser, U.; Verstraeten, R.; Salm, L.; Holdsworth, M.; Baye, K.; Booth, A.; Feskens, J.M.E.; Gillespie, S.; Talsma, F.E. Factors influencing obesogenic behaviours of adolescent girls and women in low- and middle-income countries: A qualitative evidence synthesis. Obes. Rev. 2021, 22, e13163. [Google Scholar] [CrossRef]
- Carducci, B.; Oh, C.; Roth, D.E.; Neufeld, L.M.; Frongillo, E.A.; L’Abbe, M.R.; Fanzo, J.; Herforth, A.; Sellen, D.W.; Bhutta, Z.A. Gaps and priorities in assessment of food environments for children and adolescents in low- and middle-income countries. Nat. Food 2021, 2, 396–403. [Google Scholar] [CrossRef]
- Turner, C.; Kalamatianou, S.; Drewnowski, A.; Kulkarni, B.; Kinra, S.; Kadiyala, S. Food Environment Research in Low- and Middle-Income Countries: A Systematic Scoping Review. Adv. Nutr. 2020, 11, 387–397. [Google Scholar] [CrossRef]
- Singhal, J.; Herd, C.; Adab, P.; Pallan, M. Effectiveness of school-based interventions to prevent obesity among children aged 4 to 12 years old in middle-income countries: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e13105. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020. 2013. Available online: https://apps.who.int/iris/handle/10665/94384 (accessed on 12 November 2021).
- Hawkes, C.; Jewell, J.; Allen, K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: The NOURISHING framework. Obes. Rev. 2013, 14, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Gill, T.; Kumanyika, S. Obesity prevention: A proposed framework for translating evidence into action. Obes. Rev. 2005, 6, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Carducci, B.; Oh, C.; Keats, E.C.; Roth, D.E.; Bhutta, Z.A. Effect of Food Environment Interventions on Anthropometric Outcomes in School-Aged Children and Adolescents in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Curr. Dev. Nutr. 2020, 4, nzaa098. [Google Scholar] [CrossRef] [PubMed]
- Verstraeten, R.; Roberfroid, D.; Lachat, C.; Leroy, J.L.; Holdsworth, M.; Maes, L.; Kolsteren, P.W. Effectiveness of preventive school-based obesity interventions in low- and middle-income countries: A systematic review. Am. J. Clin. Nutr. 2012, 96, 415–438. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Deverka, P.A.; Lavallee, D.C.; Desai, P.J.; Esmail, L.C.; Ramsey, S.D.; Veenstra, D.L.; Tunis, S.R. Stakeholder participation in comparative effectiveness research: Defining a framework for effective engagement. J. Comp. Eff. Res. 2012, 1, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Ogden, J. Celebrating variability and a call to limit systematisation: The example of the Behaviour Change Technique Taxonomy and the Behaviour Change Wheel. Health Psychol. Rev. 2016, 10, 245–250. [Google Scholar] [CrossRef]
- Byrne, M. Gaps and priorities in advancing methods for health behaviour change research. Health Psychol. Rev. 2020, 14, 165–175. [Google Scholar] [CrossRef]
- O’Cathain, A.; Croot, L.; Sworn, K.; Duncan, E.; Rousseau, N.; Turner, K.; Yardley, L.; Hoddinott, P. Taxonomy of approaches to developing interventions to improve health: A systematic methods overview. Pilot Feasibility Stud. 2019, 5, 41. [Google Scholar] [CrossRef]
- Oni, T.; Assah, F.; Erzse, A.; Foley, L.; Govia, I.; Hofman, K.J.; Lambert, E.V.; Micklesfield, L.K.; Shung-King, M.; Smith, J.; et al. The global diet and activity research (GDAR) network: A global public health partnership to address upstream NCD risk factors in urban low and middle-income contexts. Glob. Health 2020, 16, 100. [Google Scholar] [CrossRef] [PubMed]
- Odunitan-Wayas, F.A.; Wadende, P.; Mogo, E.R.I.; Brugulat-Panés, A.; Micklesfield, L.K.; Govia, I.; Mapa-Tassou, C.; Mukoma, G.; Smith, J.A.; Motlhalhedi, M.; et al. Adolescent Levers for a Diet and Physical Activity Intervention Across Socioecological Levels in Kenya, South Africa, Cameroon, and Jamaica: Mixed Methods Study Protocol. JMIR Res. Protoc. 2021, 10, e26739. [Google Scholar] [CrossRef] [PubMed]
- Erzse, A.; Christofides, N.; Stacey, N.; Lebard, K.; Foley, L.; Hofman, K. Availability and advertising of sugar sweetened beverages in South African public primary schools following a voluntary pledge by a major beverage company: A mixed methods study. Glob. Health Action 2021, 14, 1898130. [Google Scholar] [CrossRef] [PubMed]
- NOURISHING Framework. World Cancer Research Fund International. Available online: https://www.wcrf.org/policy/policy-databases/nourishing-framework/ (accessed on 2 February 2022).
- MOVING. Framework. World Cancer Research Fund International. Available online: https://www.wcrf.org/policy/policy-databases/moving-framework/ (accessed on 2 February 2022).
- Dalkey, N.C. The Delphi Method: An Experimental Study of Group Opinion. RAND Corporation. January 1969. Available online: https://www.rand.org/pubs/research_memoranda/RM5888.html (accessed on 23 February 2022).
- Heaton, J. Secondary Analysis of Qualitative Data: An Overview. Hist. Soc. Res./Hist. Soz. 2008, 33, 33–45. [Google Scholar]
- MAXQDA 2020; VERBI Software GmbH: Berlin, Germany, 2019; Available online: https://www.maxqda.com/ (accessed on 23 February 2022).
- NVivo. QSR International Pty Ltd.: Doncaster, Australia, 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 16 August 2022).
- Linstone, H.A.; Turoff, M. The Delphi Method: Techniques and Applications; Addison-Wesley: London, UK, 1975. [Google Scholar]
- Latif, R.B.; Dahlan, A.; Mulud, Z.A.; Nor, M. The Delphi Technique as a Method to Obtain Consensus in Health Care Education. Res. Educ. Med. J. 2017, 9, 89–102. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef]
- Van Newenhizen, J. The Borda method is most likely to respect the Condorcet principle. Econ. Theory 1992, 2, 69–83. [Google Scholar] [CrossRef]
- Warren, A.M.; Constantinides, S.V.; Blake, C.E.; Frongillo, E.A. Advancing knowledge about stakeholder engagement in multisectoral nutrition research. Global Food Secur. 2021, 29, 100521. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study Site | Stakeholders | Data Collection Tool | Description of Data |
|---|---|---|---|
| Johannesburg, South Africa | Public primary school principals, school tuck shop * owners and managers, heads of school governing bodies | Face-to-face qualitative interviews using a semi-structured interview guide | Issues covered: policies and guidelines related to the food environment, perceptions of the food and beverage environment, nutrition-related support/activities available at school, facilitators and barriers to change the food and beverage environment. |
| Cape Town, South Africa and Yaoundé, Cameroon | High-school-going adolescents from low and middle/high income communities and their parents | Qualitative telephonic in-depth interviews | Issues covered: food procurement, storage and preparation, food choices and challenges, leisure time activities, and the meaning and significance of food and physical activity within families and of adolescents. |
| High-school-going adolescents | Mobile application | Photos, texts, and audio narratives of adolescents’ neighborhood, school, home environments and journey from home to school with a focus on food outlets, food and sugar-sweetened beverage adverts, physical activity opportunities that are perceived to have an impact on adolescents’ diet and physical activity. |
| Driver | COM-B Domain | NOURISHING-MOVING | BCW Policy Category | BCW Intervention Function | Context Specific Intervention | |
|---|---|---|---|---|---|---|
| Policy Area | Intervention | |||||
| Rewarding children with unhealthy foods | Opportunity (Social) Motivation (Automatic) | Offer healthy food and set standards in public institutions and other specific settings | Mandatory standards for food available in schools including restrictions on unhealthy food | Regulation | Restriction | Stop the use of food as a reward in schools |
| Cheap and unhealthy foods and beverages at school tuck shop; influence of product characteristics, i.e., shelf life and pricing | Opportunity (Physical) Motivation (Reflective) | Use economic tools to address food affordability and purchase incentives | Targeted subsidies for healthy food | Fiscal measures | Incentivization | Incentivize school tuck shops to sell healthy food and drinks by giving subsidies or decreasing tax |
| Brand recognition of unhealthy foods | Opportunity (Social) Motivation (Reflective) | Restrict food advertising and other forms of commercial promotion | Mandatory regulation of food marketing in schools and more broadly | Legislation | Persuasion; Environmental restructuring | Stop advertising of unhealthy food products to children, including promotional materials, billboards, or signs in the school and surrounding areas |
| Polluted neighborhoods, unclean and vandalized public equipment, and PA facilities | Opportunity (Physical) | Visualize and enact structures and surroundings which promote physical activity | Policies that support access to quality public open space and green spaces | Environmental/social planning | Environmental restructuring, Enablement | Encourage strong community participation and engagement with local government to prevent vandalism, reduce litter, and promote upkeep of public spaces |
| Limited sports equipment in the schools and few sports options available to participate | Opportunity (Physical) Motivation (Reflective) | Make opportunities and initiatives that promote physical activity in schools, the community, and sport and recreation | Financial and non-financial incentives to promote physical activity | Service provision | Enablement | Collaboration between schools and sports clubs for student access free of charge and donations of sports equipment |
| Physical education and activities not taken seriously by teachers and learners | Motivation (Reflective) | Normalize and increase physical activity through public communication that motivates and builds behavior change skills | Develop and communicate physical activity guidelines | Guidelines | Education, Incentivization | Co-creation of creative ways of PE varieties by both the teachers and the learners based on the PE curriculum to motivate learners to be more physical active |
| Lack of motivation and laziness to exercise at home or in the neighborhood | Opportunity (Social) Motivation (Automatic) | Normalize and increase physical activity through public communication that motivates and builds behavior change skills | Mass communication campaigns including social marketing to increase awareness and knowledge about benefits of physical activity through the life course | Communication/marketing | Modelling, Persuasion | Social media campaigns and mass media messaging to raise awareness of the health benefits of playing sports or regular physical activity through celebrity endorsement; role models in various fields, such as athletes, singers, and actors. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erzse, A.; Rwafa-Ponela, T.; Kruger, P.; Wayas, F.A.; Lambert, E.V.; Mapa-Tassou, C.; Ngwa, E.; Goldstein, S.; Foley, L.; Hofman, K.J.; et al. A Mixed-Methods Participatory Intervention Design Process to Develop Intervention Options in Immediate Food and Built Environments to Support Healthy Eating and Active Living among Children and Adolescents in Cameroon and South Africa. Int. J. Environ. Res. Public Health 2022, 19, 10263. https://doi.org/10.3390/ijerph191610263
Erzse A, Rwafa-Ponela T, Kruger P, Wayas FA, Lambert EV, Mapa-Tassou C, Ngwa E, Goldstein S, Foley L, Hofman KJ, et al. A Mixed-Methods Participatory Intervention Design Process to Develop Intervention Options in Immediate Food and Built Environments to Support Healthy Eating and Active Living among Children and Adolescents in Cameroon and South Africa. International Journal of Environmental Research and Public Health. 2022; 19(16):10263. https://doi.org/10.3390/ijerph191610263
Chicago/Turabian StyleErzse, Agnes, Teurai Rwafa-Ponela, Petronell Kruger, Feyisayo A. Wayas, Estelle Victoria Lambert, Clarisse Mapa-Tassou, Edwin Ngwa, Susan Goldstein, Louise Foley, Karen J. Hofman, and et al. 2022. "A Mixed-Methods Participatory Intervention Design Process to Develop Intervention Options in Immediate Food and Built Environments to Support Healthy Eating and Active Living among Children and Adolescents in Cameroon and South Africa" International Journal of Environmental Research and Public Health 19, no. 16: 10263. https://doi.org/10.3390/ijerph191610263
APA StyleErzse, A., Rwafa-Ponela, T., Kruger, P., Wayas, F. A., Lambert, E. V., Mapa-Tassou, C., Ngwa, E., Goldstein, S., Foley, L., Hofman, K. J., Teguia, S., Oni, T., Assah, F., Shung-King, M., & Abdool Karim, S. (2022). A Mixed-Methods Participatory Intervention Design Process to Develop Intervention Options in Immediate Food and Built Environments to Support Healthy Eating and Active Living among Children and Adolescents in Cameroon and South Africa. International Journal of Environmental Research and Public Health, 19(16), 10263. https://doi.org/10.3390/ijerph191610263