
Moral Distress among Frontline Physicians and Nurses in the Early Phase of COVID-19 Pandemic in Italy

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measurements
2.3. Back-Forward Translation of the Stress of Conscience Questionnaire
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Sample
3.2. Factor Analysis of the Stress of Conscience Questionnaire
3.3. Correlation Analyses
3.4. Independent t-Test Analyses and Analyses of Variance
3.5. Hypotheses Testing
3.5.1. Mediation Analysis
3.5.2. The Moderated Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ando, M.; Kawano, M. Relationships among moral distress, sense of coherence, and job satisfaction. Nurs. Ethics 2018, 25, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Maffoni, M.; Argentero, P.; Giorgi, I.; Hynes, J.; Giardini, A. Healthcare professionals’ moral distress in adult palliative care: A systematic review. BMJ Support. Palliat. Care 2019, 9, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Glasberg, A.L.; Eriksson, S.; Dahlqvist, V.; Lindahl, E.; Strandberg, G.; Söderberg, A.; Sørlie, V.; Norberg, A. Development and initial validation of the Stress of Conscience Questionnaire. Nurs. Ethics 2006, 13, 633–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuzelo, P.R. Exploring the moral distress of registered nurses. Nurs. Ethics 2007, 14, 344–359. [Google Scholar] [CrossRef]
- Maffoni, M.; Argentero, P.; Giorgi, I.; Giardini, A. Healthcare professionals’ perceptions about the Italian law on advance directives. Nurs. Ethics 2020, 27, 796–808. [Google Scholar] [CrossRef]
- Maffoni, M.; Argentero, P.; Giorgi, I.; Giardini, A. Underneath the White Coat: Risk and Protective Factors for Palliative Care Providers in Their Daily Work. J. Hosp. Palliat. Nurs. 2020, 22, 108–114. [Google Scholar] [CrossRef]
- Norman, S.B.; Feingold, J.H.; Kaye-Kauderer, H.; Kaplan, C.A.; Hurtado, A.; Kachadourian, L.; Feder, A.; Murrough, J.W.; Charney, D.; Southwick, S.M.; et al. Moral distress in frontline healthcare workers in the initial epicenter of the COVID-19 pandemic in the United States: Relationship to PTSD symptoms, burnout, and psychosocial functioning. Depress. Anxiety 2021, 38, 1007–1017. [Google Scholar] [CrossRef]
- Maffoni, M.; Sommovigo, V.; Giardini, A.; Paolucci, S.; Setti, I. Dealing with ethical issues in rehabilitation medicine: The relationship between managerial support and emotional exhaustion is mediated by moral distress and enhanced by positive affectivity and resilience. J. Nurs. Manag. 2020, 28, 1114–1125. [Google Scholar] [CrossRef]
- Iserson, K.V. SARS-CoV-2 (COVID-19) vaccine development and production: An ethical way forward. Camb. Q. Heal. Ethics 2021, 30, 59–68. [Google Scholar] [CrossRef]
- Miljeteig, I.; Forthun, I.; Hufthammer, K.O.; Engelund, I.E.; Schanche, E.; Schaufel, M.; Onarheim, K.H. Priority-setting dilemmas, moral distress and support experienced by nurses and physicians in the early phase of the COVID-19 pandemic in Norway. Nurs. Ethics 2021, 28, 66–81. [Google Scholar] [CrossRef]
- Maffoni, M.; Torlaschi, V.; Pierobon, A. It’s all a matter of time. Ann. Di Ig. 2020, 32, 689–690. [Google Scholar] [CrossRef]
- Maffoni, M.; Torlaschi, V.; Pierobon, A.; Zanatta, F.; Grasso, R.; Bagliani, S.; Govoni, L.; Biglieri, M.; Cerri, L.; Gerace, L.; et al. Video calls during the COVID-19 pandemic: A bridge for patients, families, and respiratory therapists. Fam. Syst. Health 2021, 31, 650–658. [Google Scholar] [CrossRef]
- Camporesi, S.; Mori, M. Ethicists, doctors and triage decisions: Who should decide? And on what basis? J. Med. Ethics 2021, 47, e18. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-Related Mental Health Effects in the Workplace: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. J. Am. Med. Assoc. 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Deressa, W.; Worku, A.; Abebe, W.; Gizaw, M.; Amogne, W. Risk perceptions and preventive practices of COVID-19 among healthcare professionals in public hospitals in Addis Ababa, Ethiopia. PLoS ONE 2021, 16, e0242471. [Google Scholar] [CrossRef]
- Arnetz, J.E.; Goetz, C.M.; Arnetz, B.B.; Arble, E. Nurse Reports of Stressful Situations during the COVID-19 Pandemic: Qualitative Analysis of Survey Responses. Int. J. Environ. Res. 2020, 17, 8126. [Google Scholar] [CrossRef]
- Danial, F.; Khattak, I.U. Psychological impact of COVID-19 pandemic on nurses: A qualitative study. Ukr. J. Nephrol. Dial. 2021, 2, 48–55. [Google Scholar] [CrossRef]
- Smallwood, N.; Pascoe, A.; Karimi, L.; Willis, K. Moral distress and perceived community views are associated with mental health symptoms in frontline health workers during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 8723. [Google Scholar] [CrossRef]
- Tian, X.; Jin, Y.; Chen, H.; Jiménez-Herrera, M.F. Instruments for detecting moral distress in clinical nurses: A systematic review. Inq. J. Health Care Organ. Provis. Financ. 2021, 58, 0046958021996499. [Google Scholar] [CrossRef]
- Lake, E.T.; Narva, A.M.; Holland, S.; Smith, J.G.; Cramer, E.; Rosenbaum, K.E.F.; French, R.; Clark, R.R.S.; Rogowski, J.A. Hospital nurses’ moral distress and mental health during COVID-19. J. Adv. Nurs. 2021, 78, 799–809. [Google Scholar] [CrossRef]
- Dahlqvist, V.; Eriksson, S.; Glasberg, A.L.; Lindahl, E.; Lützén, K.; Strandberg, G.; Söderberg, A.; Sørlie, V.; Norberg, A. Development of the perceptions of conscience questionnaire. Nurs. Ethics 2007, 14, 181–193. [Google Scholar] [CrossRef]
- Lützén, K.; Kvist, B.E. Moral distress: A comparative analysis of theoretical understandings and inter-related concepts. HEC Forum 2012, 24, 13–25. [Google Scholar] [CrossRef]
- Alkrisat, M.; Alatrash, M. Stress of conscience: Concept clarification. Online J. Health Ethics 2016, 12, 2. [Google Scholar] [CrossRef] [Green Version]
- Badolamenti, S.; Fida, R.; Biagioli, V.; Caruso, R.; Zaghini, F.; Sili, A. Modified moral distress scale (MDS-11): Validation study among Italian nurses. Prof. Inferm. 2017, 70, 238–248. [Google Scholar] [CrossRef]
- Åhlin, J.; Ericson-Lidman, E.; Eriksson, S.; Norberg, A.; Strandberg, G. Longitudinal relationships between stress of conscience and concepts of importance. Nurs. Ethics 2013, 20, 927–942. [Google Scholar] [CrossRef]
- Jokwiro, Y.; Pascoe, E.; Edvardsson, K.; Muhammad, A.R.; McDonald, E.; Lood, Q.; Edvardsson, D. Stress of Conscience Questionnaire (SCQ): Exploring dimensionality and psychometric properties at a tertiary hospital in Australia. BMC Psychol. 2020, 8, 109. [Google Scholar] [CrossRef]
- Nilsson, U.; Odom-Forren, J.; Ring, M.; van Kooten, H.; Brady, J.M. Stress of conscience of COVID-19 among perianaesthesia nurses having worked in a COVID-ICU during the coronavirus pandemic: An international perspective. BMC Nurs. 2022, 21, 82. [Google Scholar] [CrossRef]
- Giannetta, N.; Villa, G.; Pennestrì, F.; Sala, R.; Mordacci, R.; Manara, D.F. Instruments to assess moral distress among healthcare workers: A systematic review of measurement properties. Int. J. Nurs. Stud. 2020, 111, 103767. [Google Scholar] [CrossRef] [PubMed]
- Fraccaroli, F.; Schadee, H.M. L’analisi fattoriale confermativa applicata al General Health Questionnaire. Una comparazione della versione inglese e italiana. G. Ital. Di Psicol. 1993, 20, 319–338. [Google Scholar]
- Setti, I.; van der Velden, P.G.; Sommovigo, V.; Ferretti, M.S.; Giorgi, G.; O’Shea, D.; Argentero, P. Well-Being and Functioning at Work Following Thefts and Robberies: A Comparative Study. Front. Psychol. 2018, 9, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shevlin, M.; Adamson, G. Alternative factor models and factorial invariance of the GHQ-12: A large sample analysis using confirmatory factor analysis. Psychol. Assess. 2005, 17, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Glasberg, A.; Eriksson, S.; Norberg, A. Burnout and “stress of conscience” among healthcare personnel. J. Adv. Nurs. 2007, 57, 392–403. [Google Scholar] [CrossRef]
- Orrung, W.A. Psychometric properties concerning four instruments measuring job satisfaction, strain, and stress of conscience in a residential care context. Arch. Gerontol. Geriatr. 2013, 57, 162–171. [Google Scholar] [CrossRef]
- Åhlin, J.; Ericson-Lidman, E.; Norberg, A.; Strandberg, G. Revalidation of the perceptions of conscience questionnaire (PCQ) and the stress of conscience questionnaire (SCQ). Nurs. Ethics 2012, 19, 220–232. [Google Scholar] [CrossRef]
- Saarnio, R.; Sarvimäki, A.; Laukkala, H.; Isola, A. Stress of conscience among staff caring for older persons in Finland. Nurs. Ethics 2012, 19, 104–115. [Google Scholar] [CrossRef]
- World Health Organization. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 30 March 2020).
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. ABC of content validation and content validity index calculation. Resource 2019, 11, 49–54. [Google Scholar] [CrossRef]
- Maffoni, M.; Sommovigo, V.; Giardini, A.; Argentero, P.; Setti, I. The Italian Version Of The Hospital Ethical Climate Survey: First Psychometric Evaluations In A Sample Of Healthcare Professionals Employed In Neurorehabilitation Medicine And Palliative Care Specialties. TPM: Test. Psychom. Methodol. Appl. Psychol. 2021, 28, 441–466. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Sommovigo, V.; Bernuzzi, C.; Setti, I. Helping others not always helps ourselves: The relationship between victim incivility and emergency workers’ burnout through work-to-family conflict. Int. J. Workplace Health Manag. 2022, 15, 467–492. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to mediation, moderation and conditional process analysis: A regression-based approach. J. Educ. Meas. 2013, 51, 335–337. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, 2nd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Armocida, D.; Palmieri, M.; Frati, A.; Santoro, A.; Pesce, A. How SARS-Cov-2 can involve the central nervous system. A systematic analysis of literature of the department of human neurosciences of Sapienza University, Italy. J. Clin. Neurosci. 2020, 79, 231–236. [Google Scholar] [CrossRef]
- Grasso, C.; Massidda, D.; Maslak, K.Z.; Favara-Scacco, C.; Grasso, F.A.; Bencivenga, C.; Confalone, V.; Lampugnani, E.; Moscatelli, A.; Somaini, M.; et al. Moral Distress in Healthcare Providers Who Take Care of Critical Pediatric Patients throughout Italy—Cultural Adaptation and Validation of the Italian Pediatric Instrument. Int. J. Environ. Res. Public Health 2022, 19, 3880. [Google Scholar] [CrossRef]
- Mazzotta, R.; De Maria, M.; Bove, D.; Badolamenti, S.; Saraiva Bordignon, S.; Silveira, L.; Vellone, E.; Alvaro, R.; Bulfone, G. Moral distress in nursing students: Cultural adaptation and validation study. Nurs. Ethics 2022, 29, 384–401. [Google Scholar] [CrossRef]
- Lamiani, G.; Setti, I.; Barlascini, L.; Vegni, E.; Argentero, P. Measuring moral distress among critical care clinicians: Validation and psychometric properties of the Italian moral distress scale-revised. Crit. Care Med. 2017, 45, 430–437. [Google Scholar] [CrossRef]
- Sommovigo, V.; Bernuzzi, C.; Setti, I. Investigating the association between patient verbal aggression and emotional exhaustion among Italian health care professionals during the COVID-19 pandemic. J. Nurs. Manag. 2022, 1–11. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The psychological impact of the COVID-19 outbreak on health professionals: A cross-sectional study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Almutairi, A.F.; Salam, M.; Adlan, A.A.; Alturki, A.S. Prevalence of severe moral distress among healthcare providers in Saudi Arabia. Psychol. Res. Behav. Manag. 2019, 12, 107. [Google Scholar] [CrossRef] [Green Version]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernanandes, C.M.B.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis. 2006, 12, 1924. [Google Scholar] [CrossRef]
- Braquehais, M.D.; Vargas-Cáceres, S.; Gómez-Durán, E.; Nieva, G.; Valero, S.; Casas, M.; Bruguera, E. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. QJM: Int. J. Med. 2020, 113, 613–617. [Google Scholar] [CrossRef]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. EClinicalMedicine 2020, 24, 100424. [Google Scholar] [CrossRef]
- Apisarnthanarak, A.; Apisarnthanarak, P.; Siripraparat, C.; Saengaram, P.; Leeprechanon, N.; Weber, D. Impact of anxiety and fear for COVID-19 toward infection control practices among Thai healthcare workers. Infect. Control. Hosp. Epidemiol. 2020, 41, 1093–1094. [Google Scholar] [CrossRef]
- Messias, E.; Gathright, M.M.; Freeman, E.S.; Flynn, V.; Atkinson, T.; Thrush, C.R.; Clardy, J.A.; Thapa, P. Differences in burnout prevalence between clinical professionals and biomedical scientists in an academic medical centre: A cross-sectional survey. BMJ Open 2019, 9, e023506. [Google Scholar] [CrossRef] [Green Version]
- Maffoni, M.; Sommovigo, V.; Giardini, A.; Velutti, L.; Setti, I. Well-being and professional efficacy among health care professionals: The role of resilience through the mediation of ethical vision of patient care and the moderation of managerial support. Eval. Health Prof. 2021, 01632787211042660. [Google Scholar] [CrossRef]
- Lau, J.; Tan, D.H.Y.; Wong, G.J.; Lew, Y.J.; Chua, Y.X.; Low, L.L.; Ho, H.K.; Kwek, T.S.; Sue-Anne, E.S.; Tan, K.K. Prepared and highly committed despite the risk of COVID-19 infection: A cross-sectional survey of primary care physicians’ concerns and coping strategies in Singapore. BMC Fam. Pract. 2021, 22, 22. [Google Scholar] [CrossRef] [PubMed]
- Marcolongo, F.; Ottaviani, M.; Romano, P.; Bonassi, S.; Garramone, A.; Infarinato, F.; Russo, P.; Tamburrano, A.; Tomino, C.; Prinzi, G. The role of resilience and coping among Italian healthcare workers during the COVID-19 pandemic. La Med. Del Lav. 2021, 112, 496. [Google Scholar] [CrossRef]
- Yamane, D.; Zarabian, K.; Devine, K.; Benjenk, I.; Farrar, K.; Park, O.L.; Kim, J.; Davidson, D.; Heinz, E. Hospital-Based Healthcare Worker Perceptions of Personal Risk Related to COVID-19: One Year Follow-Up. J. Am. Board Fam. Med. 2022, 35, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Almagro, J.; Hernández-Martínez, A.; Romero-Blanco, C.; Martínez-Arce, A.; Prado-Laguna, M.D.C.; García-Sanchez, F.J. Experiences and perceptions of nursing students during the COVID-19 crisis in Spain. Int. J. Environ. Res. Public Health 2021, 18, 10459. [Google Scholar] [CrossRef] [PubMed]
- Zhu, P.; Liu, X.; Wu, Q.; Loke, J.; Lim, D.; Xu, H. China’s Successful Recruitment of Healthcare Professionals to the Worst-Hit City: A Lesson Learned. Int. J. Environ. Res. Public Health 2021, 18, 8737. [Google Scholar] [CrossRef]
- Lam, S.K.; Kwong, E.W.; Hung, M.S.; Pang, S.M.; Chiang, V.C. Nurses’ preparedness for infectious disease outbreaks: A literature review and narrative synthesis of qualitative evidence. J. Clin. Nurs. 2018, 27, e1244–e1255. [Google Scholar] [CrossRef]
- Papandrea, D. In the Face of a Pandemic: Ensuring Safety and Health at Work. Available online: https://www.ilo.org/global/topics/safety-and-health-at-work/events-training/events-meetings/world-day-safety-health-at-work/WCMS_742463/lang--en/index.htm (accessed on 31 May 2020).
- Rego, F.; Sommovigo, V.; Setti, I.; Giardini, A.; Alves, E.; Morgado, J.; Maffoni, M. How Supportive Ethical Relationships Are Negatively Related to Palliative Care Professionals’ Negative Affectivity and Moral Distress: A Portuguese Sample. Int. J. Environ. Res. Public Health 2022, 19, 3863. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| % (n) | |
|---|---|
| Gender | |
| Women | 73.20 (199) |
| Profession | |
| Nursing profession | 50.00 (133) |
| Medical profession | 50.00 (133) |
| Ward | |
| Medical wards | 21.60 (55) |
| Emergency rooms | 18.00 (46) |
| Infectious disease wards | 9.00 (23) |
| Service of anesthesiology and intensive care | 8.60 (22) |
| Surgical departments | 9.80 (25) |
| COVID-19 units | 4.70 (12) |
| Intensive care units | 3.10 (8) |
| Other wards | 25.20 |
| Geographic location | |
| Lombardy Region | 92.6 (140) |
| Other regions in Northern Italy (Aosta Valley, Liguria, Emilia-Romagna, Piedmont, Veneto) | 6.60 (18) |
| Regions in Central (Lazio, Tuscany, Umbria) and Southern Italy (Campania) | 3.00 (8) |
| Since the pandemic started, have you performed duties other than your usual ones? | |
| Yes | 50.00 (136) |
| If yes, how has this change in duties been? | |
| On an ongoing basis | 54.90 (78) |
| On an occasional basis | 45.10 (64) |
| Have you received additional training for this change in duties? | |
| Yes | 45.40 (64) |
| If yes, the training provided was: | |
| poorly suited to your needs of performing a different role | 25.30 (20) |
| useful for acquiring barely sufficient basic skills to function in emergencies | 49.40 (39) |
| useful for acquiring necessary skills to function effectively in your different role | 25.30 (20) |
| Have any of your colleagues been diagnosed with COVID-19? | |
| Yes, without hospitalization | 47.60 (123) |
| Yes, with hospitalization | 52.40 (142) |
| Have any of your known persons (i.e., acquaintance, colleagues, families) been among fatalities? | |
| Yes | 53.00 (144) |
| The most critical period in your work during the assistance of patients with COVID has been: | |
| During the lockdown (February 2020–May 2020) | 73.80 (200) |
| During a later stage of pandemic management (September 2020–February 2021) | 19.60 (53) |
| The present period | 6.60 (18) |
| Item | Q1: to What Extent Do You Agree That the Item Is Representative of the Definition of Moral Distress? | Q2: to What Extent This Item Is Essential to the Measure of the Construct of Moral Distress? | Expert in Agreement on the Understandability of the Item | Expert in Agreement on Keeping the Item | I-CVI |
|---|---|---|---|---|---|
| Item 1 | 5.00 | 3.00 | 3 | 3 | 1 |
| Item 2 | 5.00 | 3.00 | 3 | 3 | 1 |
| Item 3 | 5.00 | 3.00 | 3 | 3 | 1 |
| Item 4 | 5.00 | 3.00 | 3 | 3 | 1 |
| Item 5 | 4.33 | 2.67 | 3 | 3 | 1 |
| Item 6 | 3.33 | 2.33 | 3 | 3 | 1 |
| Item 7 | 4.00 | 2.67 | 3 | 3 | 1 |
| Item 8 | 4.00 | 2.67 | 3 | 3 | 1 |
| Item 9 | 3.33 | 2.67 | 3 | 3 | 1 |
| Scale of response | 1 (Totally disagree)– 5 (Totally agree) | 1 (Useless)–3 (Essential) | S-CVI/Ave | 1 | |
| S-CVI/UA |
| Descriptive Statistics | Factor Loading | ||||
|---|---|---|---|---|---|
| Scale Item | M | SD | Skewness | Kurtosis | 1 |
| Item 1 | 12.29 | 8.34 | 0.05 | −1.19 | 0.77 |
| Item 2 | 6.24 | 7.53 | 1.13 | 0.10 | 0.75 |
| Item 3 | 9.07 | 8.25 | 0.53 | −0.90 | 0.77 |
| Item 7 | 13.87 | 9.18 | −0.16 | −1.37 | 0.74 |
| Item 8 | 8.56 | 8.69 | 0.65 | −0.96 | 0.75 |
| Item 9 | 5.32 | 7.41 | 1.41 | 1.02 | 0.53 |
| Explained variance (%) | 52.08% | ||||
| Cronbach’s alpha | 0.81 | ||||
| McDonald’s omega | 0.82 | ||||
| M | SD | Skew. | Kurt. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender | - | - | - | - | - | |||||||||||
| 2. Age | 45.26 | 11.57 | - | - | −0.05 a | - | ||||||||||
| 3. Job tenure | 17.81 | 11.46 | - | - | −0.03 a | 0.89 **,a | - | |||||||||
| 4. Profession | - | - | - | - | 0.14 *,b | −0.28 ***,a | −0.08 a | - | ||||||||
| 5. Having hospitalized colleagues | - | - | - | - | −0.05 b | 0.06 a | 0.08 a | 0.02 c | - | |||||||
| 6. Loss of someone due to COVID | - | - | - | - | 0.13 *,b | 0.05 a | 0.07 a | 0.06 c | 0.17 **,c | - | ||||||
| 7. Most critical time experienced | - | - | - | - | 0.02 b | 0.18 **,a | 0.15 *,a | −0.06 c | 0.11 c | 0.11 c | - | |||||
| 8. Change of duties | −0.06 b | 0.09 a | 0.05 a | −0.26 ***,c | 0.19 **,c | 0.03 c | 0.07 c | - | ||||||||
| 9. Moral distress | 55.36 | 35.62 | 0.37 | −0.50 | 0.07 a | −0.13 **,c | −0.09 *,c | 0.01 a | 0.01 a | 0.08 a | 0.02 a | 0.14 **,a | 0.81 | |||
| 10. Psycho-physical malaise | 18.62 | 6.91 | 0.15 | −0.37 | 0.15 *,a | −0.11*,c | −0.02 c | 0.14 *,a | 0.03 a | 0.07 a | −0.06 a | −0.03 a | 0.60 **,d | 0.82 | ||
| MED | IQR | Q1 | Q3 | Skew. | Kurt. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| 11. Concern about the infection | 3.00 | 1.00 | 2.00 | 3.00 | −0.35 | −0.31 | 0.02 a | −0.06 a | −0.01 a | 0.20 **,a | 0.06 a | 0.15 *,a | −0.08 a | 0.28 c | 0.17 **,a | 0.12 *,a |
| 12. Having felt discriminated | 1.68 | 1.00 | 1.00 | 2.00 | 0.70 | −0.89 | 0.19 **,a | −0.19 **,a | −0.09 a | 0.18 **,a | −0.07 a | 0.09 a | −0.14 *,a | −0.09 c | 0.26 **,a | 0.27 **,a |
| Men (n = 73) | Women (n = 199) | t | p | 95% CI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | LL | |||||||||
| Moral distress | 51.03 | 31.67 | 46.90 | 36.90 | −1.22 | 0.225 | −15.51 | ||||||
| Malaise | 16.97 | 6.37 | 19.23 | 7.02 | −2.41 | 0.017 | −4.10 | ||||||
| MED | IQR | Q1 | Q2 | MR | MED | IQR | Q1 | Q2 | MR | z | p | ||
| Concern | 3.00 | 1.00 | 2.00 | 3.00 | 129.49 | 3.00 | 1.00 | 2.00 | 3.00 | 132.89 | −0.34 | 0.731 | |
| Nurses (n = 133) | Doctors (n = 133) | t | p | 95% CI | |||||||||
| M | SD | M | SD | LL | |||||||||
| Moral distress | 54.85 | 32.84 | 56.07 | 37.50 | −0.28 | 0.777 | −9.73 | ||||||
| Malaise | 17.62 | 7.03 | 19.62 | 6.37 | −2.44 | 0.015 | −3.63 | ||||||
| MED | IQR | Q1 | Q2 | MR | MED | IQR | Q1 | Q2 | MR | z | p | ||
| Concern | 3.00 | 1.00 | 2.00 | 3.00 | 142.96 | 3.00 | 0.00 | 3.00 | 3.00 | 115.62 | −3.17 | 0.002 | |
| Change of duties on an ongoing basis (n = 64) | Change of duties on an occasional basis (n = 78) | t | p | 95% CI | |||||||||
| M | SD | M | SD | LL | |||||||||
| Moral distress | 59.23 | 33.96 | 66.78 | 36.44 | −1.27 | 0.208 | −19.33 | ||||||
| Malaise | 19.19 | 7.41 | 18.88 | 5.95 | 0.27 | 0.787 | −1.91 | ||||||
| MED | IQR | Q1 | Q2 | MR | MED | IQR | Q1 | Q2 | MR | z | p | ||
| Concern | 3.00 | 1.75 | 2.25 | 4.00 | 56.98 | 3.00 | 1.00 | 2.00 | 3.00 | 77.60 | −3.22 | 0.001 | |
| No additional training (n = 77) | Additional training (n = 64) | t | p | 95% CI | |||||||||
| M | SD | M | SD | LL | |||||||||
| Moral distress | 60.70 | 38.05 | 65.25 | 32.95 | −0.75 | 0.454 | −16.53 | ||||||
| Malaise | 19.06 | 6.87 | 18.73 | 6.42 | 0.29 | 0.770 | −1.91 | ||||||
| MED | IQR | Q1 | Q2 | MR | MED | IQR | Q1 | Q2 | MR | z | p | ||
| Concern | 3.00 | 1.00 | 2.00 | 3.00 | 60.85 | 3.00 | 2.00 | 2.00 | 4.00 | 77.21 | −2.56 | 0.010 | |
| Non-hospitalized colleagues (n = 129) | Hospitalized colleagues (n = 142) | t | p | 95% CI | |||||||||
| M | SD | M | SD | LL | |||||||||
| Moral distress | 55.07 | 35.13 | 56.01 | 35.99 | −0.22 | 0.827 | −9.46 | ||||||
| Malaise | 18.32 | 7.20 | 18.99 | 6.58 | −0.79 | 0.426 | −2.31 | ||||||
| MED | IQR | Q1 | Q2 | MR | MED | IQR | Q1 | Q2 | MR | z | p | ||
| Concern | 3.00 | 1.00 | 2.00 | 3.00 | 127.02 | 3.00 | 1.00 | 2.00 | 3.00 | 135.40 | −0.96 | 0.335 | |
| No loss (n = 197) | Suffered loss (n = 113) | t | p | 95% CI | |||||||||
| M | SD | M | SD | LL | |||||||||
| Moral distress | 52.53 | 36.25 | 57.87 | 34.98 | −1.24 | 0.217 | −13.85 | ||||||
| Malaise | 18.11 | 7.56 | 19.08 | 6.27 | −1.16 | 0.247 | −2.63 | ||||||
| MED | IQR | Q1 | Q2 | MR | MED | IQR | Q1 | Q2 | MR | z | p | ||
| Concern | 3.00 | 1.00 | 2.00 | 3.00 | 120.79 | 3.00 | 2.00 | 2.00 | 4.00 | 142.16 | −2.46 | 0.014 | |
| Dimension | Job Tenure | Mean | SD | F | |||
|---|---|---|---|---|---|---|---|
| Moral distress | ≤10 years | 59.49 | 37.91 | 1.33 | |||
| 11–20 years | 56.25 | 29.90 | |||||
| >20 years | 51.22 | 37.42 | |||||
| Psycho-physical malaise | ≤10 years | 18.53 | 6.58 | 0.50 | |||
| 11–20 years | 18.09 | 6.95 | |||||
| >20 years | 19.10 | 7.19 | |||||
| MED | IQR | Q1 | Q2 | MR | X2 | ||
| Concern about the infection | ≤10 years | 3.00 | 1.00 | 2.00 | 3.00 | 136.28 | 0.59 |
| 11–20 years | 3.00 | 1.00 | 2.00 | 3.00 | 131.98 | ||
| >20 years | 3.00 | 1.00 | 2.00 | 3.00 | 128.37 | ||
| Dimension | Age | Mean | SD | F | |||
| Moral distress | ≤35 years | 58.23 | 38.27 | 5.28 ** | |||
| 36–45 years | 63.62 | 31.51 | |||||
| 46–55 years | 57.57 | 33.65 | |||||
| >55 years | 38.73 | 35.38 | |||||
| Psycho-physical malaise | ≤35 years | 19.20 | 6.46 | 2.09 | |||
| 36–45 years | 19.44 | 6.81 | |||||
| 46–55 years | 18.88 | 7.01 | |||||
| >55 years | 16.52 | 7.21 | |||||
| MED | IQR | Q1 | Q2 | MR | X2 | ||
| Concern about the infection | ≤35 years | 3.00 | 1.00 | 3.00 | 4.00 | 152.38 | 19.92 *** |
| 36–45 years | 2.00 | 1.00 | 2.00 | 3.00 | 96.66 | ||
| 46–55 years | 3.00 | 1.00 | 2.00 | 3.00 | 136.20 | ||
| >55 years | 3.00 | 1.00 | 2.00 | 3.00 | 135.91 | ||
| Dimension | Most critical period experienced | Mean | SD | F | |||
| Moral distress | Lockdown | 56.10 | 35.62 | 0.16 | |||
| Later stage | 54.45 | 37.01 | |||||
| Present period | 51.55 | 33.12 | |||||
| Psycho-physical malaise | Lockdown | 18.45 | 6.67 | 2.79 | |||
| Later stage | 20.24 | 6.87 | |||||
| Present period | 16.05 | 8.87 | |||||
| MED | IQR | Q1 | Q2 | MR | X2 | ||
| Concern about the infection | Lockdown | 3.00 | 1.00 | 2.00 | 3.00 | 128.20 | 6.06 |
| Later stage | 3.00 | 1.00 | 2.00 | 3.00 | 129.53 | ||
| Present period | 3.00 | 1.00 | 2.00 | 3.00 | 111.27 | ||
| Dimension | Quality of training received | Mean | SD | F | |||
| Moral distress | Inadequate | 80.75 | 29.22 | 6.87 ** | |||
| Basic | 63.87 | 33.79 | |||||
| Adequate | 42.35 | 34.44 | |||||
| Psycho-physical malaise | Inadequate | 18.10 | 4.30 | 1.22 | |||
| Basic | 19.10 | 6.21 | |||||
| Adequate | 16.40 | 7.93 | |||||
| MED | IQR | Q1 | Q2 | MR | X2 | ||
| Concern about the infection | Inadequate | 4.00 | 0.25 | 3.75 | 4.00 | 51.39 | 12.56 ** |
| Basic | 3.00 | 1.75 | 2.00 | 3.75 | 33.35 | ||
| Adequate | 3.00 | 1.00 | 2.00 | 3.00 | 30.47 | ||
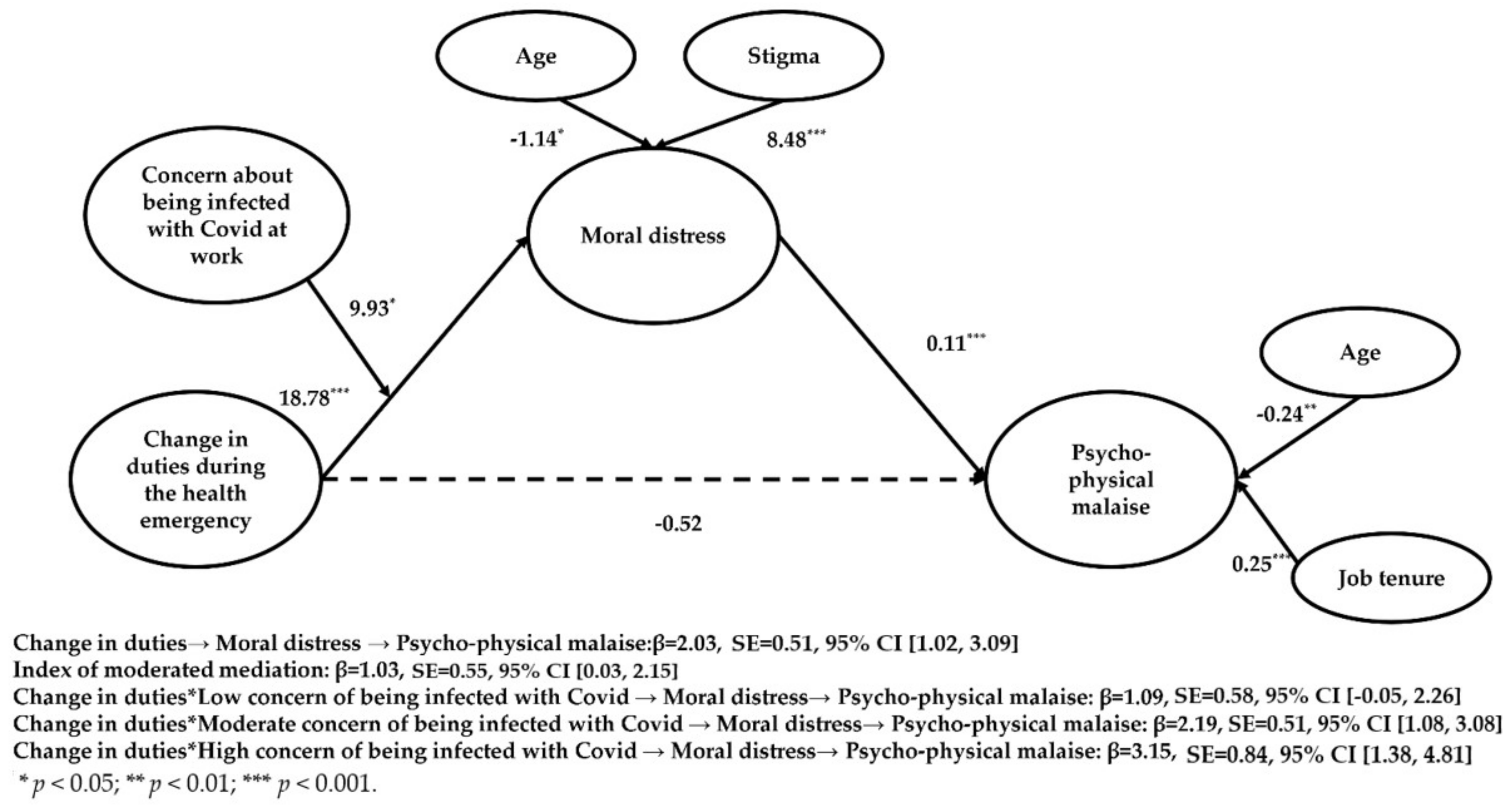
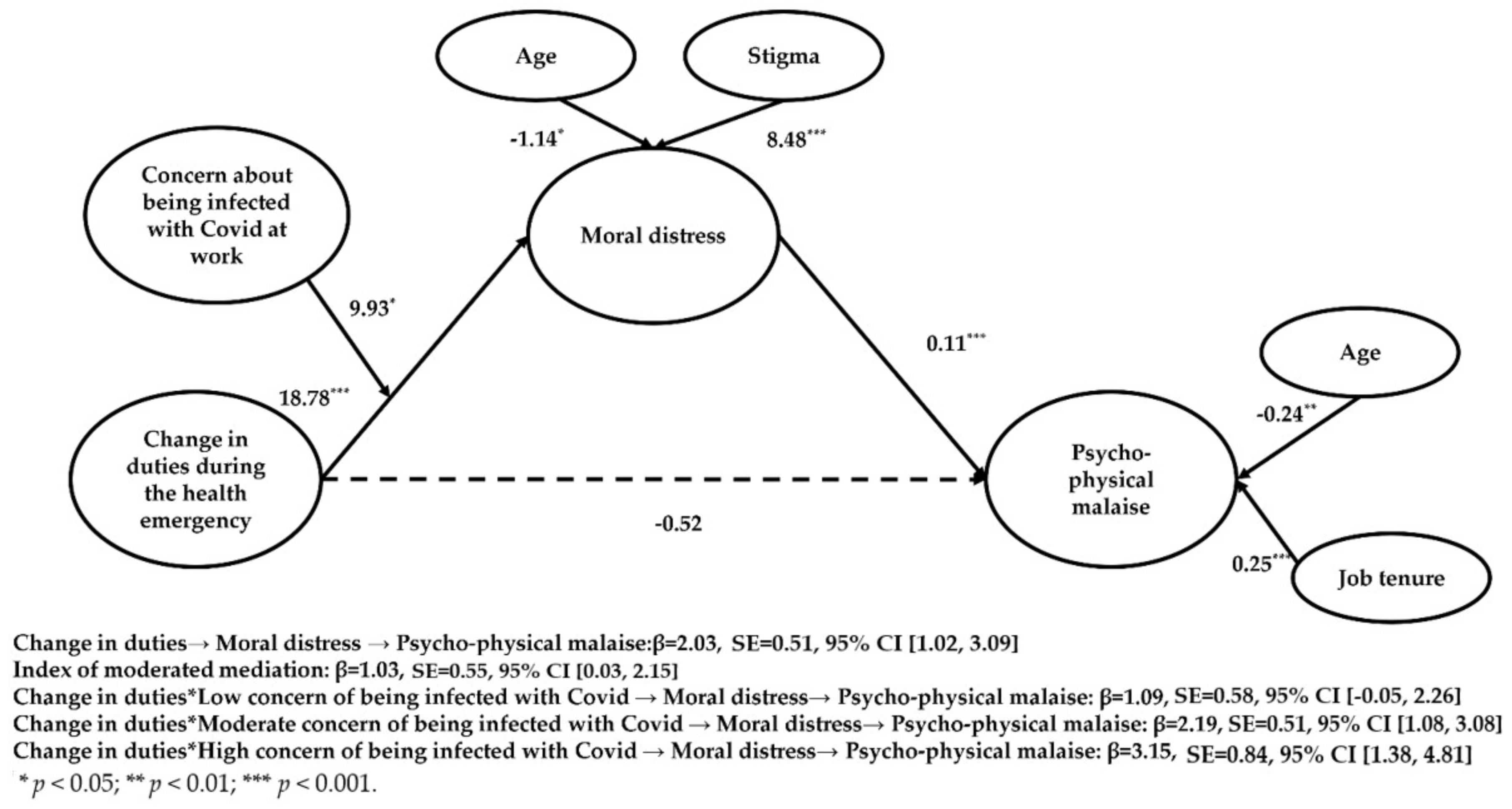
| Model (Outcome) | R | R2 | p | MSE | F | df1 |
|---|---|---|---|---|---|---|
| Model 3a (Moral distress) | 0.47 | 0.33 | 0.00 | 998.25 | 6.20 | 11 |
| Model 3b (Psycho-physical malaise) | 0.63 | 0.40 | 0.00 | 26.87 | 16.29 | 10 |
| Standardized direct and conditional effects | ||||||
| Effects—Model 3a | B | SE | t | p | ||
| Change in duties → Moral distress | 18.78 *** | 4.21 | 4.53 | 0.00 | ||
| Concern → Moral distress | 5.84 * | 2.58 | 2.26 | 0.02 | ||
| Change in duties * Concern → Moral distress | 9.93 * | 5.01 | 1.98 | 0.04 | ||
| Gender → Moral distress | 1.62 | 4.67 | 0.35 | 0.73 | ||
| Age → Moral distress | −1.14 * | 0.47 | −2.43 | 0.01 | ||
| Job tenure → Moral distress | 0.56 | 0.45 | 1.25 | 0.21 | ||
| Occupation → Moral distress | −4.84 | 4.94 | −0.98 | 0.33 | ||
| Stigma → Moral distress | 8.48 *** | 2.47 | 3.43 | 0.00 | ||
| Hospitalized colleagues → Moral distress | −0.96 | 4.15 | −0.23 | 0.82 | ||
| Most critical period experienced → Moral distress | 4.55 | 4.49 | 1.01 | 0.31 | ||
| Suffered lost → Moral distress | 3.78 | 4.20 | 0.90 | 0.37 | ||
| Effects—Model 3b | B | SE | t | p | ||
| Change in duties → Malaise | −0.52 | 0.72 | −0.73 | 0.47 | ||
| Stress → Malaise | 0.11 *** | 0.01 | 10.07 | 0.00 | ||
| Gender → Malaise | 1.01 | 0.76 | 1.32 | 0.19 | ||
| Age → Malaise | −0.24 ** | 0.08 | −3.13 | 0.00 | ||
| Job tenure → Malaise | 0.25 *** | 0.07 | 3.42 | 0.00 | ||
| Occupation → Malaise | 0.09 | 0.80 | 0.11 | 0.91 | ||
| Having felt discriminated → Malaise | 0.35 | 0.41 | 0.85 | 0.39 | ||
| Having hospitalized colleagues → Malaise | 0.45 | 0.68 | 0.67 | 0.50 | ||
| Most critical period experienced → Malaise | −0.67 | 0.73 | −0.91 | 0.36 | ||
| Suffered lost → Malaise | 0.04 | 0.68 | 0.06 | 0.95 | ||
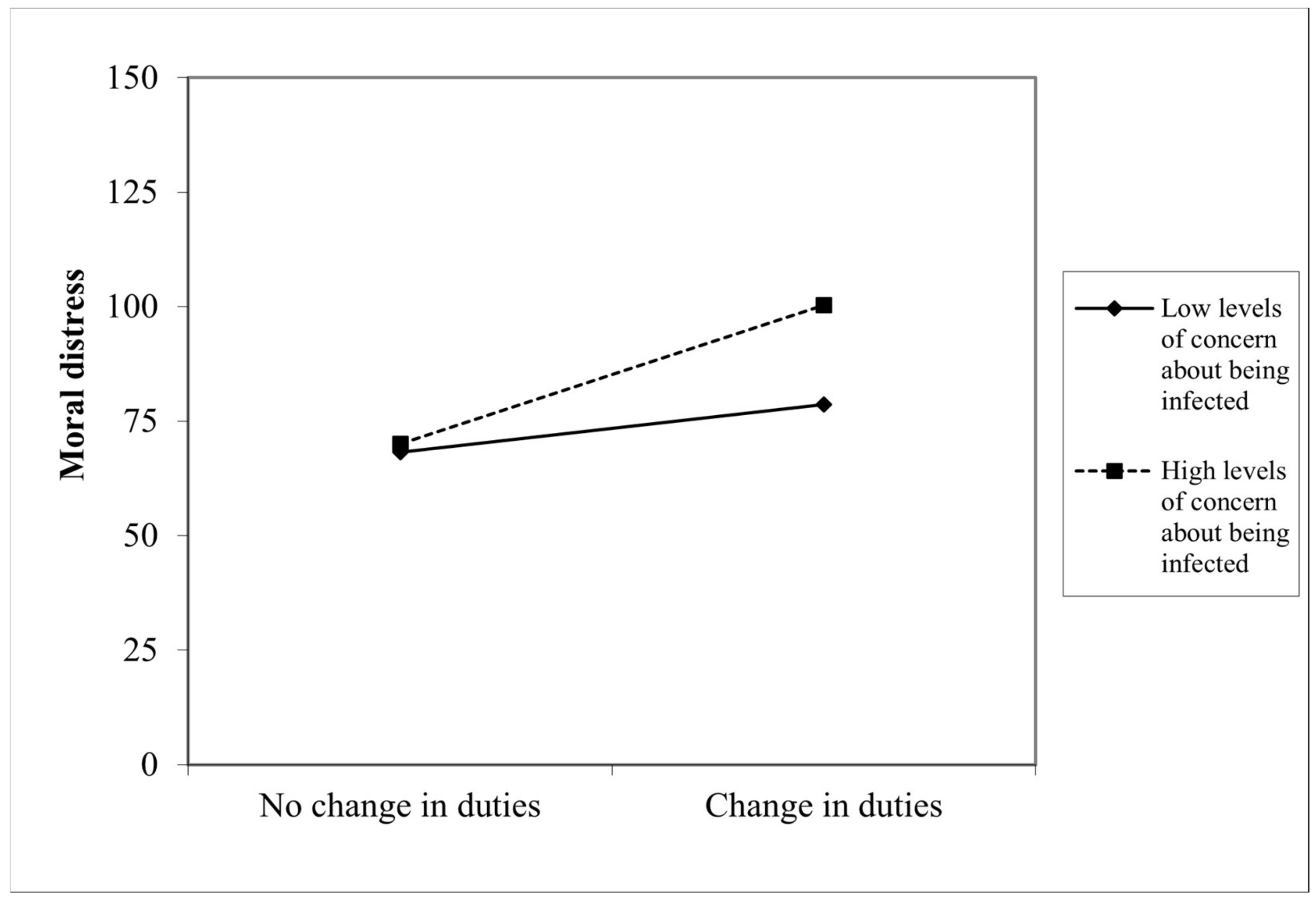
| Conditional effects | B | SE | ||||
| Change in duties * Low Concern → Distress →Malaise | 1.09 | 0.58 | ||||
| Change in duties * Moderate Concern→ Distress →Malaise | 2.19 | 0.51 | ||||
| Change in duties * High Concern→ Distress →Malaise | 3.15 | 0.84 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maffoni, M.; Fiabane, E.; Setti, I.; Martelli, S.; Pistarini, C.; Sommovigo, V. Moral Distress among Frontline Physicians and Nurses in the Early Phase of COVID-19 Pandemic in Italy. Int. J. Environ. Res. Public Health 2022, 19, 9682. https://doi.org/10.3390/ijerph19159682
Maffoni M, Fiabane E, Setti I, Martelli S, Pistarini C, Sommovigo V. Moral Distress among Frontline Physicians and Nurses in the Early Phase of COVID-19 Pandemic in Italy. International Journal of Environmental Research and Public Health. 2022; 19(15):9682. https://doi.org/10.3390/ijerph19159682
Chicago/Turabian StyleMaffoni, Marina, Elena Fiabane, Ilaria Setti, Sara Martelli, Caterina Pistarini, and Valentina Sommovigo. 2022. "Moral Distress among Frontline Physicians and Nurses in the Early Phase of COVID-19 Pandemic in Italy" International Journal of Environmental Research and Public Health 19, no. 15: 9682. https://doi.org/10.3390/ijerph19159682
APA StyleMaffoni, M., Fiabane, E., Setti, I., Martelli, S., Pistarini, C., & Sommovigo, V. (2022). Moral Distress among Frontline Physicians and Nurses in the Early Phase of COVID-19 Pandemic in Italy. International Journal of Environmental Research and Public Health, 19(15), 9682. https://doi.org/10.3390/ijerph19159682