
Understanding Moral Distress among Eldercare Workers: A Scoping Review

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Aim of the Study
- (1)
- What factors cause moral distress in eldercare?
- (2)
- What are the consequences of moral distress for employees’ wellbeing?
- (3)
- What kind of interventions to mitigate moral distress have been implemented in eldercare?
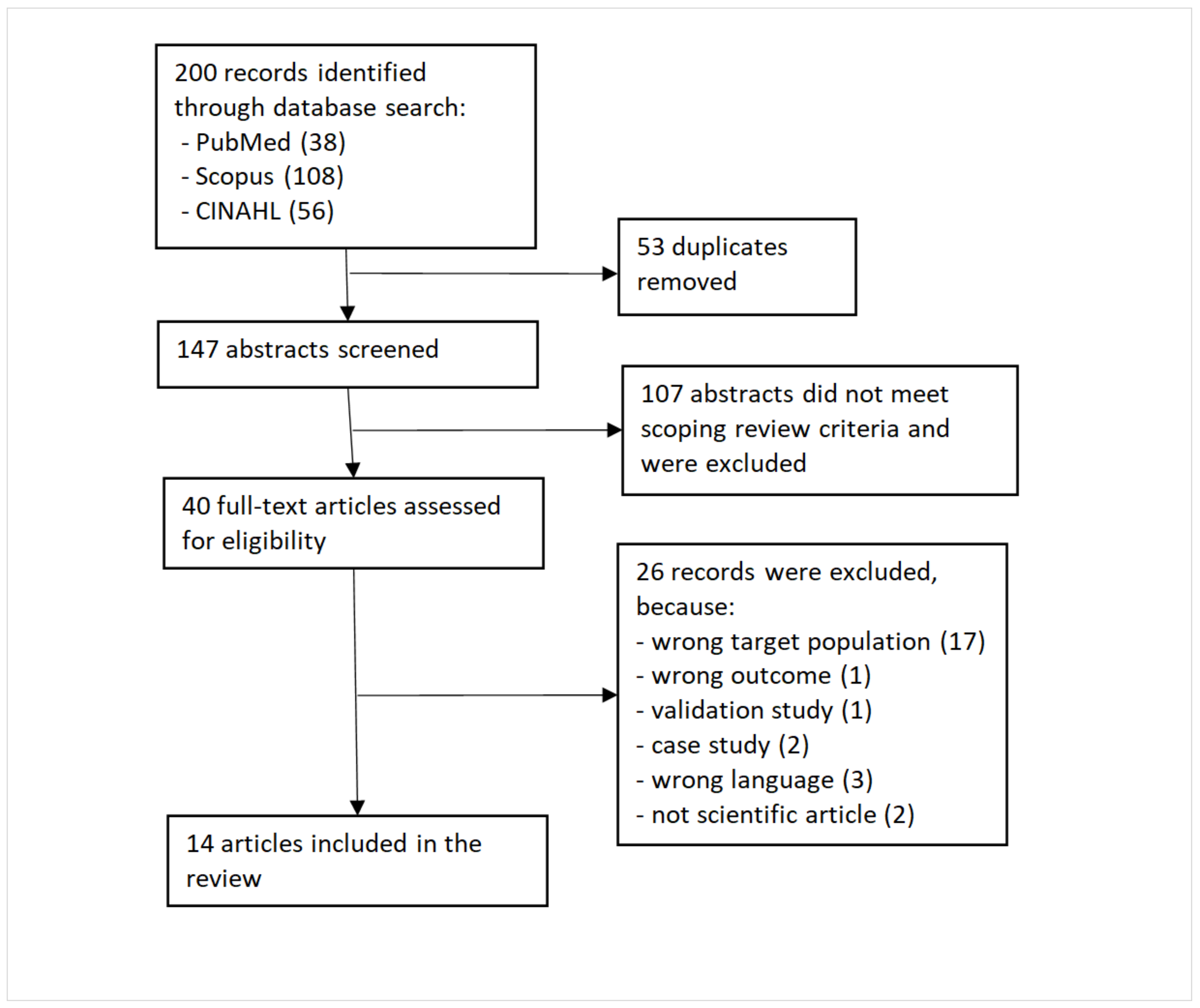
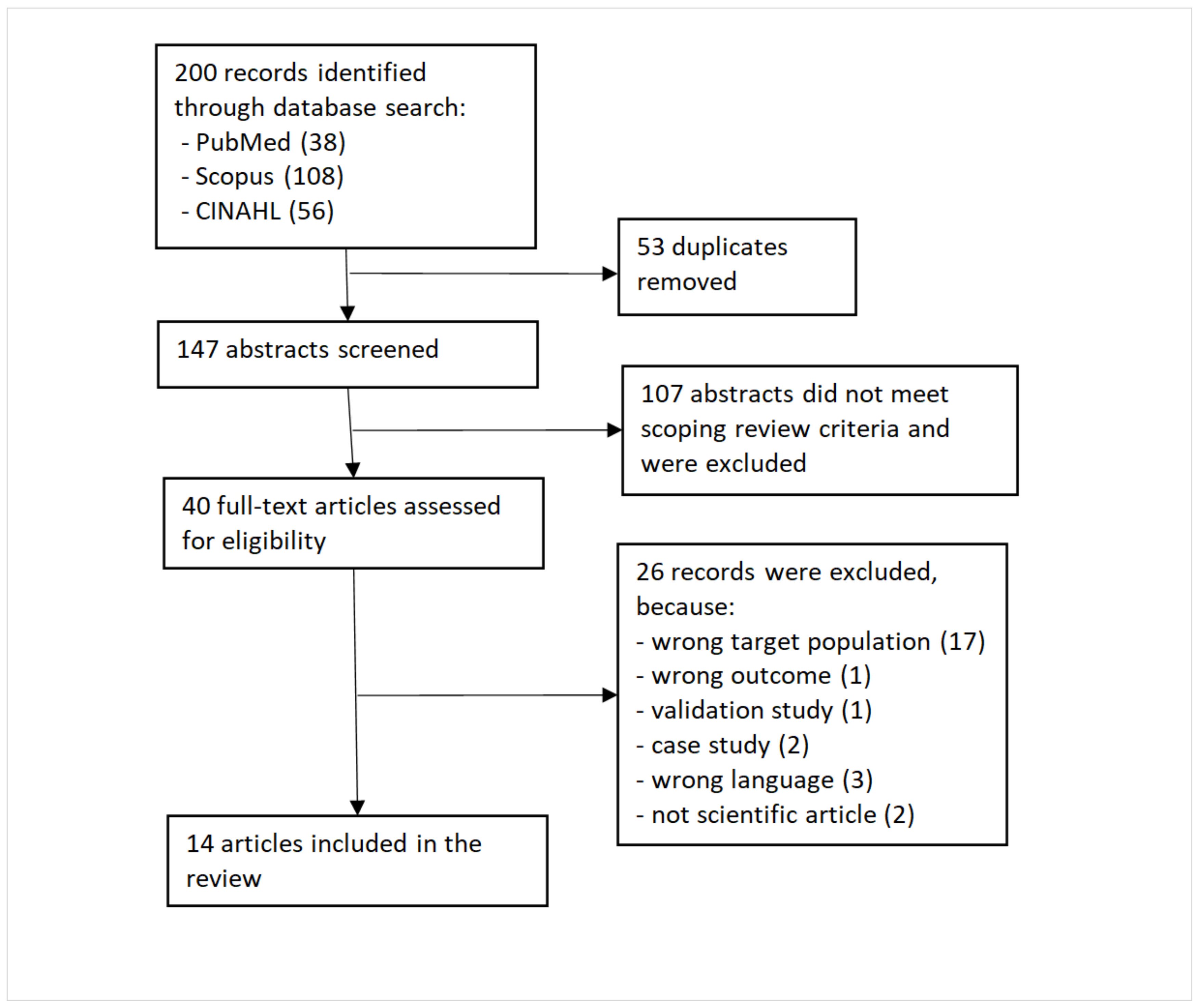
3. Methods
- We included studies where the target population comprised employees working in eldercare services and in close contact with elderlies. We excluded studies of services with multiple patient groups, such as palliative care, where elderlies are one among multiple patient groups. We also excluded studies of eldercare managers who had little contact with elderlies.
- We included studies which focused on eldercare workers’ moral distress. We excluded studies which examined moral distress in caregiving in general or examined it from the clients’ perspective.
- We included studies published in 1997–2022, written in English and published in peer-reviewed journals.
- We included both qualitative and quantitative studies, excluding validation studies and case studies.
4. Results
4.1. Target Populations in Studies
4.2. Definitions of Moral Distress
4.3. How Moral Distress Was Measured
4.4. What Causes or Affects Moral Distress

{kind=link}
| Causes of Moral Distress: Main Category | Causes of Moral Distress: Sub-Category | Causes of Moral Distress | Number of Causes |
|---|---|---|---|
| Organizational restraints | Organizational policies and leadership (in 9 studies) | Administration quantifies the performance of the nurses (1), neglecting non-registered clients (1), no time with patients in the rotating system for visiting care (1), organizational interest in becoming digital vs. duty of care for the patients (3), lack of trust in the healthcare organization (4), conflict between what workers felt right and what was the duty of care (5), acceptance of work pressure (8), inconsistent care expectations (9), leadership failures (10), inadequate care models and resources (10), a culture of tasks over touch (10), policies not in the best interest of the patients (11), fearing consequences if advocating for residents (14), | 13 |
| Inadequate resources and resource allocation (in 7 studies) | allocation of resources (2), structure and quality of services and resource allocation within the nursing home (5), lack of staff (7), having to rush the care and making patients wait (7), being forced to provide low-quality care to reduce costs (8), lack of resources (9), lack of time, balancing residents’ needs (11, 12) | 8 | |
| Relational and power-related issues | Hierarchy/power to influence care (in 3 studies) | Lack of control over the development of digital solutions (3), relations between physicians and nurses (8), undervaluing expertise (11) | 3 |
| Relations/conflicts with colleagues (in 3 studies) | Working with incompetent/unaccountable colleagues (6, 9, 10) not involved in end-of-life decisions (6), lack of ethical debate (6), | 5 | |
| Relationship between patients/families and professionals (in 8 studies) | Differences in the understanding of moral and legal responsibility of care (4), conflicts within the relationships of staff, families, and residents (5, 9, 14), families do not provide necessities such as clothing (7), conflicting expectations with families around care (10), difficult communication (12, 14) | 8 | |
| Caring for patients | Inadequate/futile care (in 2 studies) | Unjustifiable life support (6), unnecessary tests and treatments (6), decision about life-sustaining treatment (13), discordance when preferring a more comfort-focused plan than the patient is receiving (13) | 4 |
| Patients suffering (in 3 studies) | Working in acute (vs. chronic) geriatric care (6), seeing a low quality of life due to lack of activities (7), proximity to the bedside (7), unpredictable dying trajectories (14) | 4 | |
| Patient autonomy (in 2 studies) | Refusal of care (2), collecting and sharing personal patient data (2), balancing autonomy, care and dignity (4) | 3 | |
| Workers’ self-assessment | Lack of competence & safety issues (in 5 studies) | Acknowledgement of visiting nurses’ limitations (1), unprepared to use digital solutions (3), managing patients’ dementia behaviors (9), remaining silent to avoid consequences (10), self-perceived weakness (12) | 5 |
| Consequences of a Moral Distress: Main Category | Consequences of Moral Distress | Number of Consequences |
|---|---|---|
| 1. Avoidance and resistance (in 4 studies) | Intentional or actual job leave (6), reduced job satisfaction and wanting to quit job (8), quitting job (10), sick leave (10), negotiating the organizational constraints in various, often creative ways (11) | 5 |
| 2. Mental health problems (in 10 studies) | Distress and anxiety (1), distress (3, 5), exhaustion (4), burnout (7), psychological distress: feeling angry, powerless, and frustrated (8), feeling emotionally drained (8), emotional reactions (10), emotional distress (11, 12), helplessness and fear (12), powerlessness (14) | 12 |
| 3. Unhealthy and asocial behavior (in 3 studies) | Engaging in unhealthy behaviors (8), relationship effects (9), distraction and isolation (12) | 3 |
| 4. Physical symptoms (in 2 studies) | Physical exhaustion (8), physical reactions (9) | 2 |
4.5. Consequences of Moral Distress on Workers
4.6. Interventions to Mitigate Moral Distress
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Selander, K.; Nikunlaakso, R.; Laitinen, J. Association between work ability and work stressors: Cross-sectional survey of elderly services and health and social care service employees. Arch. Public Health 2022, 80, 83. [Google Scholar] [CrossRef] [PubMed]
- Rainer, J.; Schneider, J.K.; Lorenz, R.A. Ethical dilemmas in nursing: An integrative review. J. Clin. Nurs. 2018, 27, 3446–3461. [Google Scholar] [CrossRef] [PubMed]
- Giannetta, N.; Villa, G.; Pennestrì, F.; Sala, R.; Mordacci, R.; Manara, D.F. Ethical Problems and Moral Distress in Primary Care: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7565. [Google Scholar] [CrossRef] [PubMed]
- Kooli, C. COVID-19: Public health issues and ethical dilemmas. Eth. Med. Public Health 2021, 17, 100635. [Google Scholar] [CrossRef]
- Pakkanen, P.; Häggman-Laitila, A.; Kangasniemi, M. Ethical issues identified in nurses’ interprofessional collaboration in clinical practice: A meta-synthesis. J. Interprof. Care 2021, 23, 1–10. [Google Scholar] [CrossRef]
- Aitamaa, E.; Leino-Kilpi, H.; Iltanen, S.; Suhonen, R. Ethical problems in nursing management: The views of nurse managers. Nurs. Eth. 2016, 23, 646–658. [Google Scholar] [CrossRef]
- Laukkanen, L.; Suhonen, R.; Leino-Kilpi, H. Solving work-related ethical problems: The activities of nurse managers. Nurs. Eth. 2015, 23, 838–850. [Google Scholar] [CrossRef]
- Epstein, E.G.; Whitehead, P.B.; Prompahakul, C.; Thacker, L.R.; Hamric, A.B. Enhancing Understanding of Moral Distress: The Measure of Moral Distress for Health Care Professionals. AJOB Empir. Bioeth. 2019, 10, 113–124. [Google Scholar] [CrossRef]
- Kim, M.; Oh, Y.; Kong, B. Ethical Conflicts Experienced by Nurses in Geriatric Hospitals in South Korea: “If You Can’t Stand the Heat, Get Out of the Kitchen”. Int. J. Environ. Res. Public Health 2020, 17, 4442. [Google Scholar] [CrossRef]
- Oh, Y.; Gastmans, C. Moral distress experienced by nurses: A quantitative literature review. Nurs. Eth. 2015, 22, 15–31. [Google Scholar] [CrossRef]
- Ganahl, S.; Knaus, M.; Wiesenhuetter, I.; Klemm, V.; Jabinger, E.M.; Strametz, R. Second Victims in Intensive Care—Emotional Stress and Traumatization of Intensive Care Nurses in Western Austria after Adverse Events during the Treatment of Patients. Int. J. Environ. Res. Public Health 2022, 19, 3611. [Google Scholar] [CrossRef]
- Trifunovic-Koenig, M.; Strametz, R.; Gerber, B.; Mantri, S.; Bushuven, S. Validation of the German Version of the Moral Injury Symptom and Support Scale for Health Professionals (G-MISS-HP) and Its Correlation to the Second Victim Phenomenon. Int. J. Environ. Res. Public Health 2022, 19, 4857. [Google Scholar] [CrossRef]
- Foà, C.; Guarnieri, M.C.; Bastoni, G.; Benini, B.; Giunti, O.M.; Mazzotti, M.; Rossi, M.; Savoia, A.; Sarli, L.; Artioli, G. Job satisfaction, work engagement and stress/burnout of elderly care staff: A qualitative research. Acta Biomed. 2020, 91, e2020014. [Google Scholar] [CrossRef]
- Podgorica, N.; Flatscher-Thöni, M.; Deufert, D.; Siebert, U.; Ganner, M. A systematic review of ethical and legal issues in elder care. Nurs. Eth. 2021, 28, 895–910. [Google Scholar] [CrossRef]
- Enes, S.P.D.; De Vries, K. A survey of ethical issues experienced by nurses caring for terminally ill elderly people. Nurs. Eth. 2004, 11, 150–164. [Google Scholar] [CrossRef]
- De Casterle, B.D.; Goethals, S.; Gastmans, C. Contextual influences on nurses’ decision-making in cases of physical restraint. Nurs. Eth. 2015, 22, 642–651. [Google Scholar] [CrossRef]
- Smith, K.V. Ethical issues related to health care: The older adult’s perspective. J. Gerontol. Nurs. 2005, 31, 32–39. [Google Scholar] [CrossRef]
- Fourie, C. Moral distress and moral conflict in clinical ethics. Bioethics 2015, 29, 91–97. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Jameton, A. Nursing Practice: The Ethical Issues; Series in the philosophy of medicine; Prentice-Hall: Englewood Cliffs, NJ, USA, 1984. [Google Scholar]
- Nathaniel, A.K. A Grounded Theory of Moral Reckoning in Nursing. Ph.D. Thesis, West Virginia University, Morgantown, WV, USA, 2003. [Google Scholar]
- Corvol, A.; Moutel, G.; Gagnon, D.; Nugue, M.; Saint-Jean, O.; Somme, D. Ethical issues in the introduction of case management for elderly people. Nurs. Eth. 2013, 20, 83–95. [Google Scholar] [CrossRef]
- Sedaghati, A.; Assarroudi, A.; Akrami, R.; Rad, M. Moral distress and its influential factors in the nurses of the nursing homes in khorasan provinces in 2019: A descriptive-correlational study. Iran. J. Nurs. Midwifery Res. 2020, 25, 319–324. [Google Scholar] [CrossRef]
- Preshaw, D.H.; McLaughlin, D.; Brazil, K. Ethical issues in palliative care for nursing homes: Development and testing of a survey instrument. J. Clin. Nurs. 2018, 27, e678–e687. [Google Scholar] [CrossRef] [Green Version]
- Corley, M.C.; Elswick, R.K.; Gorman, M.; Clor, T. Development and evaluation of a MD scale. J. Adv. Nurs. 2001, 33, 250–256. [Google Scholar] [CrossRef]
- Wocial, L.D.; Weaver, M.T. Development and psychometric testing of a new tool for detecting moral distress: The Moral Distress Thermometer. J. Adv. Nurs. 2013, 69, 167–174. [Google Scholar] [CrossRef]
- Spenceley, S.; Caspar, S.; Pijl, E.M. Mitigating Moral Distress in Dementia Care: Implications for Leaders in the Residential Care Sector. Nurs. Leadersh. 2019, 30, 45–59. [Google Scholar] [CrossRef]
- Rittenmeyer, L.; Huffman, D. How professional nurses working in hospital environments experience moral distress: A systematic review. JBI Evid. Synth. 2009, 7, 1234–1291. [Google Scholar] [CrossRef]
- Spenceley, S.; Witcher, C.S.; Hagen, B.; Hall, B.; Kardolus-Wilson, A. Sources of moral distress for nursing staff providing care to residents with dementia. Dementia 2017, 16, 815–834. [Google Scholar] [CrossRef]
- Wocial, L.D.; Slaven, J.E.; Montz, K.; Monahan, P.O.; Hickman, S.E.; Callahan, C.M.; Helft, P.R.; Sachs, G.A.; Inger, L.; Burke, E.S.; et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J. Gen. Intern. Med. 2020, 35, 1405–1412. [Google Scholar] [CrossRef]
- Frennert, S. Moral distress and ethical decision-making of eldercare professionals involved in digital service transformation. Disabil. Rehabil. Assist. Technol. 2020, 1–10. [Google Scholar] [CrossRef]
- Piers, R.D.; Van den Eynde, M.; Steeman, E.; Vlerick, P.; Benoit, D.D.; Van Den Noortgate, N.J. End-of-life care of the geriatric patient and nurses’ moral distress. J. Am. Med. Dir. Assoc. 2012, 13, 7–13. [Google Scholar] [CrossRef]
- Pijl-Zieber, E.M.; Awosoga, O.; Spenceley, S.; Hagen, B.; Hall, B.; Lapins, J. Caring in the wake of the rising tide: Moral distress in residential nursing care of people living with dementia. Dementia 2018, 17, 315–336. [Google Scholar] [CrossRef] [PubMed]
- Wiersma, E.; Marcella, J.; McAnulty, J.; Kelley, M.L. ‘That just breaks my heart’: Moral Concerns of Direct Care Workers Providing Palliative Care in LTC Homes. Can. J. Aging Rev. Can. Vieil. 2019, 38, 268–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, G.; Pennestrì, F.; Rosa, D.; Giannetta, N.; Sala, R.; Mordacci, R.; Manara, D.F. Moral Distress in Community and Hospital Settings for the Care of Elderly People. A Grounded Theory Qualitative Study. Healthcare 2021, 9, 1307. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Froggatt, K.; Brearley, S.G. ‘Powerlessness’ or ‘doing the right thing’—Moral distress among nursing home staff caring for residents at the end of life: An interpretive descriptive study. Palliat. Med. 2017, 31, 853–860. [Google Scholar] [CrossRef] [Green Version]
- Choe, K.; Kim, K.; Lee, K.S. Ethical concerns of visiting nurses caring for older people in the community. Nurs. Eth. 2015, 22, 700–710. [Google Scholar] [CrossRef]
- Holm, A.L.; Severinsson, E. Reflections on the ethical dilemmas involved in promoting self-management. Nurs. Eth. 2014, 21, 402–413. [Google Scholar] [CrossRef] [Green Version]
- Muldrew, D.H.; McLaughlin, D.; Brazil, K. Ethical issues experienced during palliative care provision in nursing homes. Nurs. Eth. 2019, 26, 1848–1860. [Google Scholar] [CrossRef] [Green Version]
| Authors | Study Number | Title (Concept) | Country | Year | Study Mehodology | Target Population | Study Size/N | Definition of Moral Distress | How Moral Distress Was Measured |
|---|---|---|---|---|---|---|---|---|---|
| Choe et al. | 1 | Ethical concerns of visiting nurses caring for older people in the community (ethical dilemmas) | Korea | 2015 | Qualitative interviews | Nurses | 13 | No definition | Prior to the interviews, participants were asked to think of ethical concerns they might have experienced while working as visiting nurses. They were asked an open-ended question: ‘‘What ethical concerns have you ever experienced while working as a visiting nurse? |
| Corvol et al. | 2 | Ethical issues in the introduction of case management for elderly people (ethical dilemmas) | France | 2013 | Qualitative interviews and focus groups | Case managers with different background | 12 | Definition based on Beauchamp and Childress’s principles of biomedical ethics | Open-ended questions related to clients’ choice, cost control, information sharing, and other ethical issues that were not addressed by the interviewer. |
| Frennert | 3 | Moral distress and ethical decision-making of eldercare professionals involved in digital service transformation (moral distress) | Sweden | 2020 | Mixed-method: interview + survey | Various professionals responsible for municipal’s digital service transformation (e.g., head of unit, digitalization strategist, quality assurance developer, chief nurse care services coordinator, and business developer strategist) | interview 10; survey 40 | Adapted and modified from Sidwick (2019) | In a survey, the first question was: “Do you encounter any ethical matters in regard to digital care services in your everyday work practices?” If they answered yes, exploratory open-ended questions followed concerning what kinds of ethical matters were faced, specifically which kinds of digital services, patients, and situations, and their influence on ethical decision-making. |
| Holm & Severinsson | 4 | Reflections on the ethical dilemmas involved in promoting self-management (ethical dilemmas) | Norway | 2014 | Qualitative focus group interviews | Various professionals | 2 focus groups | Definition is based on several previous empirical works | No examples of questions in group sessions. |
| Muldrew et al. | 5 | Ethical issues experienced during palliative care provision in nursing homes (ethical dilemmas) | UK | 2019 | Mixed-method: interview+survey | Various professionals | 23; 198 | Definition is based on several previous empirical works | No examples of interview questions. In a survey moral distress scale developed by Preshaw et al. (2017) |
| Piers et al. | 6 | End-of-life care of the geriatric patient and nurses’ moral distress (moral distress) | Belgium | 2012 | Quantitative survey | Nurses | 222 | Adapted from Schwenzer & Wang (2006) | Modified version of Corley’s moral distress scale |
| Pijl-Zieber et al. | 7 | Caring in the wake of the rising tide: Moral distress in residential nursing care of people living with dementia (moral distress) | Canada | 2018 | Quantitative survey | Various professionals | 389 | Nathaniel definition (2003) | Developed their own moral distress scale based on qualitative interviews |
| Sedaghati et al. | 8 | Moral Distress and its Influential Factors in the Nurses of the Nursing Homes in Khorasan Provinces in 2019: A Descriptive-Correlational Study (moral distress) | Iran | 2020 | Quantitative survey | Nurses | 227 | Own definition | Developed their own moral distress scale based on earlier measurements |
| Spenceley et al. | 9 | Mitigating Moral Distress in Dementia Care: Implications for Leaders in the Residential Care Sector (moral distress) | Canada | 2019 | Mixed method: interviews+survey | Nurses | 389 | Nathaniel definition (2003) | The interviews began with a discussion of the definition of moral distress, followed by prompting questions asking participants to recall specific events or times when they experienced moral distress, how they felt during and after the experience, what effects they experienced that they could attribute to moral distress and what helped, or could help, to reduce moral distress. Based on interviews and literature, researchers developed their own moral distress scale. |
| Spenceley et al. | 10 | Sources of moral distress for nursing staff providing care to residents with dementia (moral distress) | Canada | 2017 | Qualitative interviews | Various professionals | 18 | Jameton’s definition | No information on questions |
| Wiersma et al. | 11 | That just breaks my heart’: Moral Concerns of Direct Care Workers Providing Palliative Care in LTC Homes (moral distress) | Ontario Canada | 2019 | Qualitative focus group interviews | Various professionals | 45 | Definition is based on previous literature | Open-ended questions: participants were asked their understanding of palliative care and quality of life, the role standing of palliative care and quality of life, the role that they played in providing palliative care, the role that the family played in providing palliative care, how the organizational structure facilitated or hindered their abilities in providing palliative care, and what they would change regarding palliative care delivery in their home if they could. |
| Villa et al. | 12 | Moral Distress in Community and Hospital Settings for the Care of Elderly People. A Grounded Theory Qualitative Study (moral distress) | Italy | 2021 | Qualitative interviews | Various professionals | 13 | Jameton’s definition | Open-ended questions aimed at understanding how participants deal with a morally distressing event and explore how their actions and choices are limited or enhanced by environmental triggers. |
| Wocial et al. | 13 | Factors Associated with Physician Moral Distress Caring for Hospitalized Elderly Patients Needing a Surrogate Decision-maker: a Prospective Study (moral distress) | Pennsylvania, USA | 2020 | Quantitative survey | Physicians | 154 | Adapted from Dudinski (2016) | Moral distress thermometer developed by Wocial & Weaver |
| Young et al. | 14 | ‘Powerlessness’ or ‘doing the right thing’—Moral distress among nursing home staff caring for residents at the end of life: An interpretive descriptive study (moral distress) | England | 2017 | Qualitative interviews | Various professionals | 16 | Adapted from Peter (2013) | Interviews started with a reminder of the aim of the research, and the focus was on examining situations where the participants had cared for residents at the end of life, where they had achieved the care outcomes or where they had been unable to achieve them due to circumstances beyond their control. |
| Strategy Main Category | Strategies to Mitigate Moral Distress | Number of Strategies |
|---|---|---|
| 1. Organizational support and education (in 2 studies) | More resources for care (9), increased education (9), increased administrative/leadership support (9), trust from the leaders (12), | 4 |
| 2. Peer support (in 2 studies) | Peer support (9), relying on group morality in decision making (12), sharing feelings and choices with colleagues and the team (12) | 3 |
| 3. Improving selfcare and competence (in 2 studies) | Attention to self-care (9), maintaining soothing behavior (12), understanding how the elderly explicitly or implicitly express their needs (12), psychological support (12) | 4 |
| 4. Defending patients (in 1 study) | Prioritising respect for autonomy over the principle of beneficence (2), refusing to ask intimate questions (2), defending the interests of the client (2) | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikunlaakso, R.; Selander, K.; Weiste, E.; Korkiakangas, E.; Paavolainen, M.; Koivisto, T.; Laitinen, J. Understanding Moral Distress among Eldercare Workers: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 9303. https://doi.org/10.3390/ijerph19159303
Nikunlaakso R, Selander K, Weiste E, Korkiakangas E, Paavolainen M, Koivisto T, Laitinen J. Understanding Moral Distress among Eldercare Workers: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9303. https://doi.org/10.3390/ijerph19159303
Chicago/Turabian StyleNikunlaakso, Risto, Kirsikka Selander, Elina Weiste, Eveliina Korkiakangas, Maria Paavolainen, Tiina Koivisto, and Jaana Laitinen. 2022. "Understanding Moral Distress among Eldercare Workers: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 15: 9303. https://doi.org/10.3390/ijerph19159303
APA StyleNikunlaakso, R., Selander, K., Weiste, E., Korkiakangas, E., Paavolainen, M., Koivisto, T., & Laitinen, J. (2022). Understanding Moral Distress among Eldercare Workers: A Scoping Review. International Journal of Environmental Research and Public Health, 19(15), 9303. https://doi.org/10.3390/ijerph19159303