
Association between Chronotype, Physical Activity and Sedentary Behaviour: A Systematic Review


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Bibliographic Search
2.2. Selection Criteria
2.3. Assessment of Methodological Quality
2.4. Data Extraction
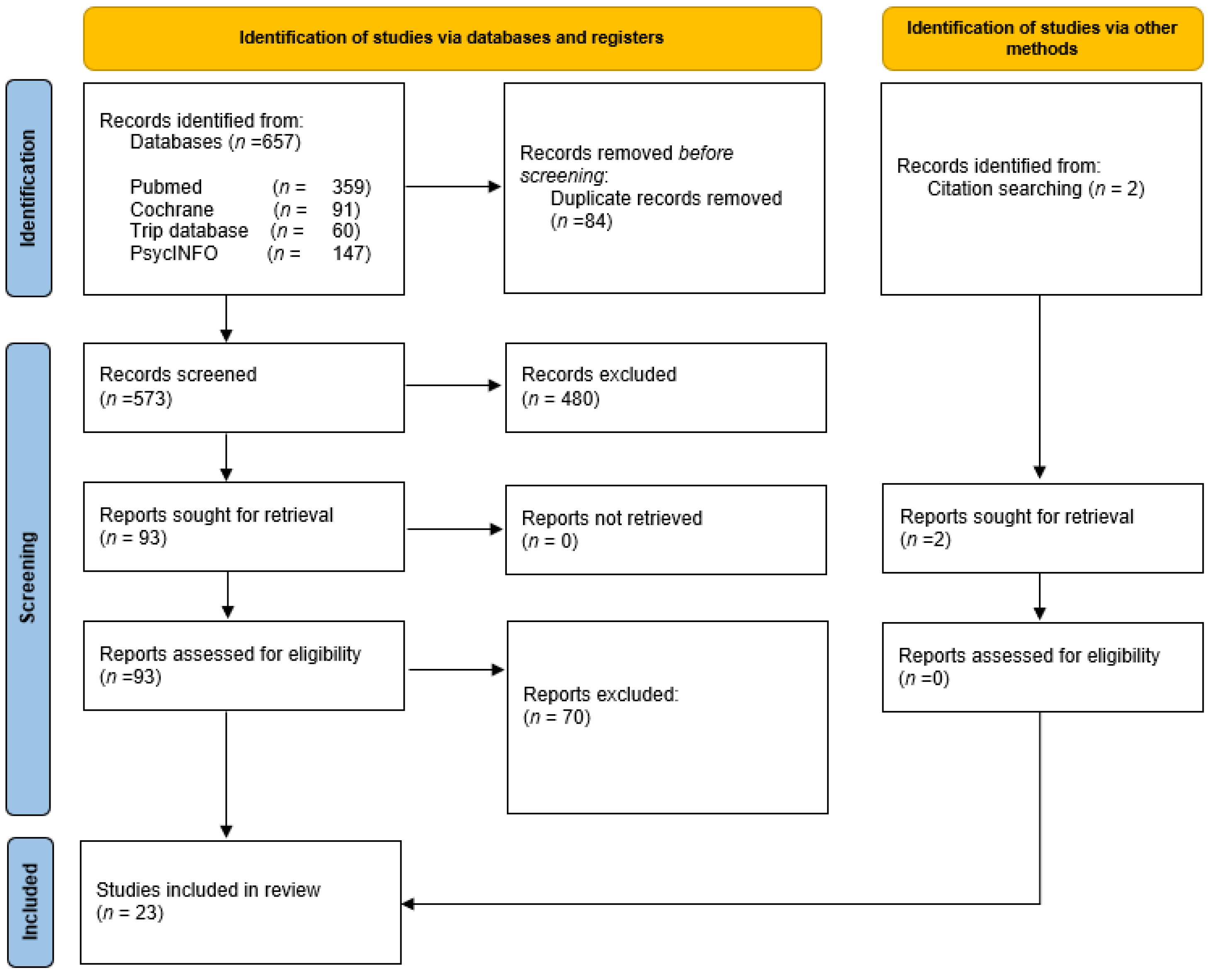
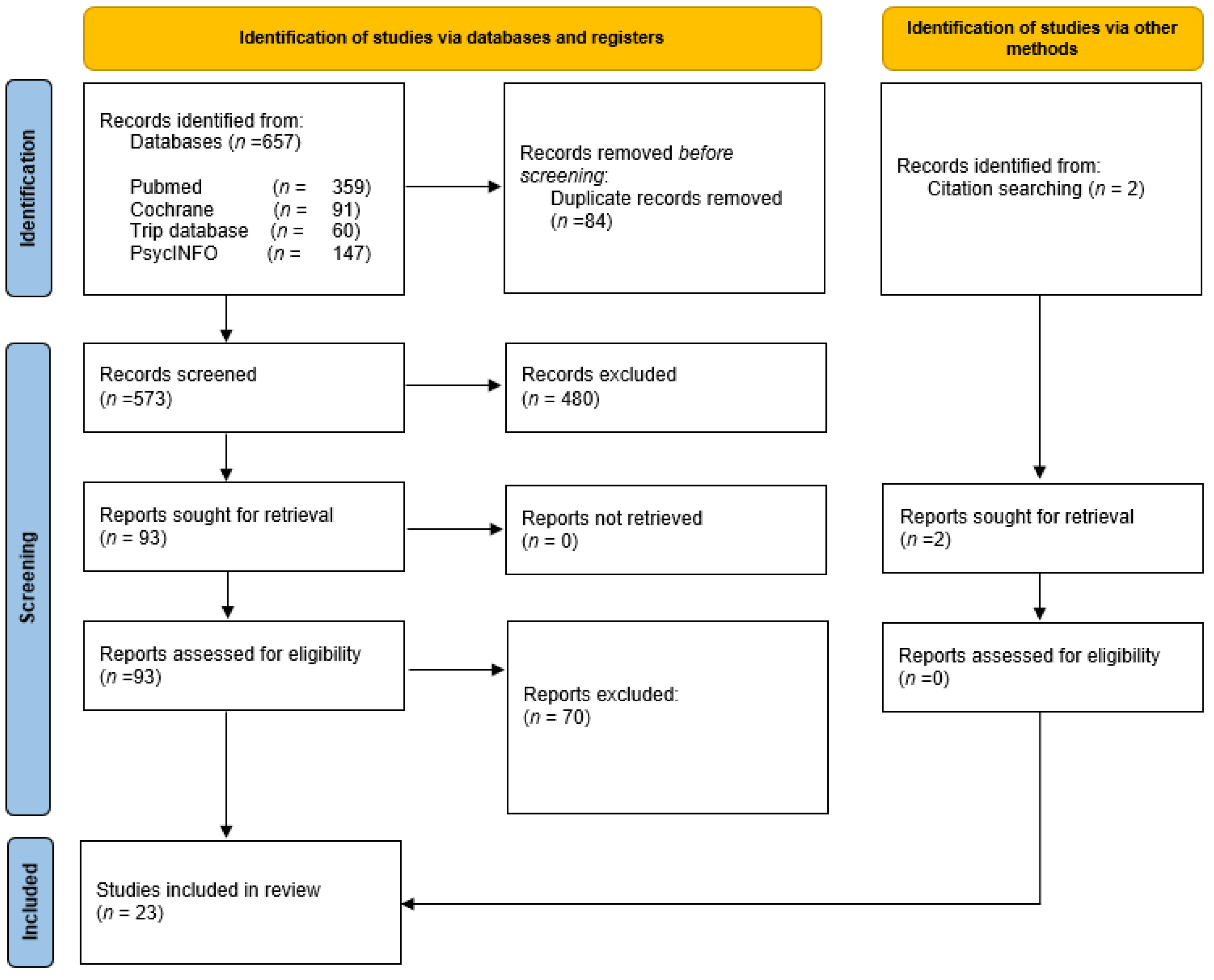
3. Results
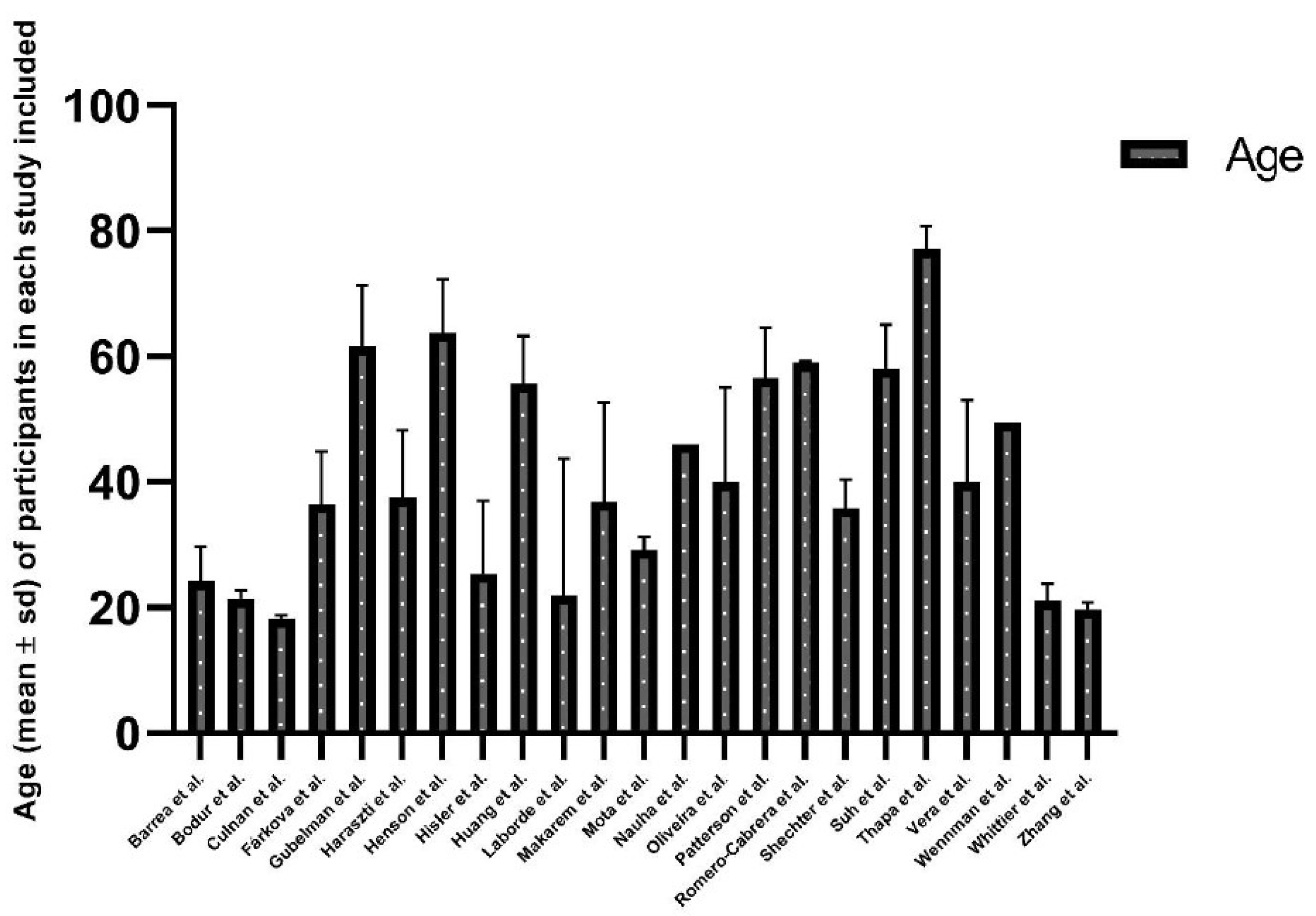
3.1. Characteristics of the Included Studies
3.2. Chronotype and PA Collection Instruments
3.3. Association between Chronotype, PA and SB
4. Discussion
4.1. Main Findings
4.2. Limitations of the Systematic Review
4.3. Practical Implications and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/handle/10665/272722 (accessed on 21 May 2022).
- United Nations General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E (accessed on 21 May 2022).
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Wittmann, M.; Paulus, M.; Roenneberg, T. Decreased Psychological Well-Being in Late ‘Chronotypes’ Is Mediated by Smoking and Alcohol Consumption. Subst. Use Misuse 2010, 45, 15–30. [Google Scholar] [CrossRef]
- Baron, K.G.; Reid, K.J.; Kern, A.S.; Zee, P.C. Role of Sleep Timing in Caloric Intake and BMI. Obesity 2011, 19, 1374–1381. [Google Scholar] [CrossRef]
- Schneider, M.L.D.M.; Vasconcellos, D.C.; Dantas, G.; Levandovski, R.; Caumo, W.; Allebrandt, K.V.; Doring, M.; Hidalgo, M.P.L. Morningness–eveningness, use of stimulants, and minor psychiatric disorders among undergraduate students. Int. J. Psychol. 2011, 46, 18–23. [Google Scholar] [CrossRef]
- Merikanto, I.; Lahti, T.; Kronholm, E.; Peltonen, M.; Laatikainen, T.; Vartiainen, E.; Salomaa, V.; Partonen, T. Evening types are prone to depression. Chronobiol. Int. 2013, 30, 719–725. [Google Scholar] [CrossRef] [Green Version]
- Konttinen, H.; Kronholm, E.; Partonen, T.; Kanerva, N.; Männistö, S.; Haukkala, A. Morningness–eveningness, depressive symptoms, and emotional eating: A population-based study. Chronobiol. Int. 2014, 31, 554–563. [Google Scholar] [CrossRef]
- Taillard, J.; Philip, P.; Claustrat, B.; Capelli, A.; Coste, O.; Chaumet, G.; Sagaspe, P. Time Course of Neurobehavioral Alertness During Extended Wakefulness in Morning- and Evening-Type Healthy Sleepers. Chronobiol. Int. 2011, 28, 520–527. [Google Scholar] [CrossRef]
- Merikanto, I.; Lahti, T.; Puolijoki, H.; Vanhala, M.; Peltonen, M.; Laatikainen, T.; Vartiainen, E.; Salomaa, V.; Kronholm, E.; Partonen, T. Associations of Chronotype and Sleep With Cardiovascular Diseases and Type 2 Diabetes. Chronobiol. Int. 2013, 30, 470–477. [Google Scholar] [CrossRef]
- Reutrakul, S.; Hood, M.M.; Crowley, S.J.; Morgan, M.K.; Teodori, M.; Knutson, K.L.; Van Cauter, E. Chronotype Is Independently Associated With Glycemic Control in Type 2 Diabetes. Diabetes Care 2013, 36, 2523–2529. [Google Scholar] [CrossRef] [Green Version]
- Maukonen, M.; Kanerva, N.; Partonen, T.; Kronholm, E.; Tapanainen, H.; Kontto, J.; Männistö, S. Chronotype differences in timing of energy and macronutrient intakes: A population-based study in adults: Energy/Macronutrient Intake Timing of Chronotypes. Obesity 2017, 25, 608–615. [Google Scholar] [CrossRef] [Green Version]
- Broms, U.; Kaprio, J.; Hublin, C.; Partinen, M.; Madden, P.A.F.; Koskenvuo, M. Evening types are more often current smokers and nicotine-dependent-a study of Finnish adult twins: Evening types are more often nicotine-dependent. Addiction 2011, 106, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Broms, U.; Pennanen, M.; Patja, K.; Ollila, H.; Korhonen, T.; Kankaanpää, A.; Haukkala, A.; Tuulio-Henriksson, A.; Koskenvuo, M.; Kronholm, E.; et al. Diurnal Evening Type is Associated with Current Smoking, Nicotine Dependence and Nicotine Intake in the Population Based National FINRISK 2007 Study. J Addict. Res. Ther. 2012, S2, 002. [Google Scholar] [CrossRef] [Green Version]
- Prat, G.; Adan, A. Influence of Circadian Typology on Drug Consumption, Hazardous Alcohol use, and Hangover Symptoms. Chronobiol. Int. 2011, 28, 248–257. [Google Scholar] [CrossRef]
- Monk, T.H.; Buysse, D.J.; Potts, J.M.; DeGrazia, J.M.; Kupfer, D.J. Morningness-Eveningness and Lifestyle Regularity. Chronobiol. Int. 2004, 21, 435–443. [Google Scholar] [CrossRef]
- Vitale, J.A.; Weydahl, A. Chronotype, Physical Activity, and Sport Performance: A Systematic Review. Sports Med. 2017, 47, 1859–1868. [Google Scholar] [CrossRef] [Green Version]
- Honkalampi, K.; Järvelin-Pasanen, S.; Tarvainen, M.P.; Saaranen, T.; Vauhkonen, A.; Kupari, S.; Perkiö-Mäkelä, M.; Räsänen, K.; Oksanen, T. Heart rate variability and chronotype–a systematic review. Chronobiol. Int. 2021, 38, 1786–1796. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 372, 89. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 15 May 2022). [CrossRef]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic Reviews of Effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 1 October 2021). [CrossRef]
- Bodur, M.; Baspinar, B.; Özçelik, A.Ö. Do sleep quality and caffeine consumption mediate the relationship between late chronotype and body mass index? Food Funct. 2021, 12, 5959–5966. [Google Scholar] [CrossRef]
- Culnan, E.; Kloss, J.D.; Grandner, M. A prospective study of weight gain associated with chronotype among college freshmen. Chronobiol. Int. 2013, 30, 682–690. [Google Scholar] [CrossRef] [Green Version]
- Gubelmann, C.; Heinzer, R.; Haba-Rubio, J.; Vollenweider, P.; Marques-Vidal, P. Physical activity is associated with higher sleep efficiency in the general population: The CoLaus study. Sleep 2018, 41, zsy070. [Google Scholar] [CrossRef]
- Haraszti, R.Á.; Purebl, G.; Salavecz, G.; Poole, L.; Dockray, S.; Steptoe, A. Morningness–eveningness interferes with perceived health, physical activity, diet and stress levels in working women: A cross-sectional study. Chronobiol. Int. 2014, 31, 829–837. [Google Scholar] [CrossRef]
- Hisler, G.C.; Phillips, A.L.; Krizan, Z. Individual Differences in Diurnal Preference and Time-of-Exercise Interact to Predict Exercise Frequency. Ann. Behav. Med. 2017, 51, 391–401. [Google Scholar] [CrossRef]
- Huang, B.H.; Hamer, M.; Duncan, M.J.; Cistulli, P.A.; Stamatakis, E. The bidirectional association between sleep and physical activity: A 6.9 years longitudinal analysis of 38,601 UK Biobank participants. Prev. Med. 2021, 143, 106315. [Google Scholar] [CrossRef]
- Laborde, S.; Guillén, F.; Dosseville, F.; Allen, M.S. Chronotype, sport participation, and positive personality-trait-like individual differences. Chronobiol. Int. 2015, 32, 942–951. [Google Scholar] [CrossRef]
- Makarem, N.; Paul, J.; Giardina, E.G.V.; Liao, M.; Aggarwal, B. Evening chronotype is associated with poor cardiovascular health and adverse health behaviors in a diverse population of women. Chronobiol. Int. 2020, 37, 673–685. [Google Scholar] [CrossRef]
- Mota, M.C.; Waterhouse, J.; De-Souza, D.A.; Rossato, L.T.; Silva, C.M.; Araújo, M.B.J.; Tufik, S.; de Mello, M.T.; Crispim, C.A. Association between chronotype, food intake and physical activity in medical residents. Chronobiol. Int. 2016, 33, 730–739. [Google Scholar] [CrossRef]
- Nauha, L.; Jurvelin, H.; Ala-Mursula, L.; Niemelä, M.; Jämsä, T.; Kangas, M.; Korpelainen, R. Chronotypes and objectively measured physical activity and sedentary time at midlife. Scand. J. Med. Sci. Sports 2020, 30, 1930–1938. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.F.; Marin, T.C.; Apolinário, N.; Rosa-Silva, J.; Azevêdo, L.; Ceciliato, J.; Silva-Batista, C.; Brito, L.C. Association of morningness-eveningness preference with physical activity during the COVID-19 pandemic social distancing: A cross-sectional survey in Brazil. Chronobiol. Int. 2021, 38, 1432–1440. [Google Scholar] [CrossRef] [PubMed]
- Patterson, F.; Malone, S.K.; Lozano, A.; Grandner, M.A.; Hanlon, A.L. Smoking, Screen-Based Sedentary Behavior, and Diet Associated with Habitual Sleep Duration and Chronotype: Data from the UK Biobank. Ann. Behav. Med. 2016, 50, 715–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shechter, A.; St-Onge, M.P. Delayed sleep timing is associated with low levels of free-living physical activity in normal sleeping adults. Sleep Med. 2014, 15, 1586–1589. [Google Scholar] [CrossRef] [Green Version]
- Suh, S.; Yang, H.C.; Kim, N.; Yu, J.H.; Choi, S.; Yun, C.H.; Shin, C. Chronotype Differences in Health Behaviors and Health-Related Quality of Life: A Population-Based Study Among Aged and Older Adults. Behav. Sleep Med. 2017, 15, 361–376. [Google Scholar] [CrossRef]
- Thapa, N.; Kim, B.; Yang, J.G.; Park, H.J.; Jang, M.; Son, H.E.; Kim, G.M.; Park, H. The Relationship between Chronotype, Physical Activity and the Estimated Risk of Dementia in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 3701. [Google Scholar] [CrossRef]
- Wennman, H.; Kronholm, E.; Partonen, T.; Peltonen, M.; Vasankari, T.; Borodulin, K. Evening typology and morning tiredness associates with low leisure time physical activity and high sitting. Chronobiol. Int. 2015, 32, 1090–1100. [Google Scholar] [CrossRef]
- Whittier, A.; Sanchez, S.; Castañeda, B.; Sanchez, E.; Gelaye, B.; Yanez, D.; Williams, M.A. Eveningness Chronotype, Daytime Sleepiness, Caffeine Consumption, and Use of Other Stimulants Among Peruvian University Students. J. Caffeine Res. 2014, 4, 21–27. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiong, Y.; Dong, J.; Guo, T.; Tang, X.; Zhao, Y. Caffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index among Medical Students in Chongqing, China: A Multiple Mediation Model. Int. J. Environ. Res. Public Health 2018, 15, 1721. [Google Scholar] [CrossRef] [Green Version]
- Barrea, L.; Verde, L.; Vetrani, C.; Savastano, S.; Colao, A.; Muscogiuri, G. Chronotype: A tool to screen eating habits in polycystic ovary syndrome? Nutrients 2022, 14, 955. [Google Scholar] [CrossRef]
- Fárková, E.; Schneider, J.; Šmotek, M.; Bakštein, E.; Herlesová, J.; Kopřivová, J.; Šrámková, P.; Pichlerová, D.; Fried, M. Weight loss in conservative treatment of obesity in women is associated with physical activity and circadian phenotype: A longitudinal observational study. Biopsychosoc. Med. 2019, 13, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henson, J.; Rowlands, A.V.; Baldry, E.; Brady, E.M.; Davies, M.J.; Edwardson, C.L.; Yates, T.; Hall, A.P. Physical behaviors and chronotype in people with type 2 diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001375. [Google Scholar] [CrossRef] [PubMed]
- Romero-Cabrera, J.L.; Garaulet, M.; Jimenez-Torres, J.; Alcala-Diaz, J.F.; Navarro, G.M.Q.; Martin-Piedra, L.; Torres-Peña, J.D.; Rodriguez-Cantalejo, F.; Rangel-Zuñiga, O.A.; Yubero-Serrano, E.M. Chronodisruption and diet associated with increased cardiometabolic risk in coronary heart disease patients: The CORDIOPREV study. Transl. Res. 2022, 242, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Vera, B.; Dashti, H.S.; Gómez-Abellán, P.; Hernández-Martínez, A.M.; Esteban, A.; Scheer, F.A.J.L.; Saxena, R.; Garaulet, M. Modifiable lifestyle behaviors, but not a genetic risk score, associate with metabolic syndrome in evening chronotypes. Sci. Rep. 2018, 8, 945. [Google Scholar] [CrossRef] [Green Version]
- Adan, A.; Almirall, H. Horne and Östberg morningness-eveningness questionnaire: A reduced scale. Personal. Individ. Differ. 1991, 12, 241–253. [Google Scholar] [CrossRef]
- Hätönen, T.; Forsblom, S.; Kieseppä, T.; Lönnqvist, J.; Partonen, T. Circadian phenotype in patients with the co-morbid alcohol use and bipolar disorders. Alcohol Alcohol. 2008, 43, 564–568. [Google Scholar] [CrossRef] [Green Version]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between Clocks: Daily Temporal Patterns of Human Chronotypes. J. Biol. Rhythms 2003, 18, 80–90. [Google Scholar] [CrossRef] [Green Version]
- Reiter, A.M.; Sargent, C.; Roach, G.D. Concordance of Chronotype Categorisations Based on Dim Light Melatonin Onset, the Morningness-Eveningness Questionnaire, and the Munich Chronotype Questionnaire. Clocks Sleep 2021, 3, 342–350. [Google Scholar] [CrossRef]
- Dosseville, F.; Laborde, S.; Lericollais, R. Validation of a Chronotype Questionnaire Including an Amplitude Dimension. Chronobiol. Int. 2013, 30, 639–648. [Google Scholar] [CrossRef]
- Smith, C.S.; Reilly, C.; Midkiff, K. Evaluation of three circadian rhythm questionnaires with suggestions for an improved measure of morningness. J. Appl. Psychol. 1989, 74, 728–738. [Google Scholar] [CrossRef]
- Randler, C.; Díaz-Morales, J.F.; Rahafar, A.; Vollmer, C. Morningness–eveningness and amplitude–development and validation of an improved composite scale to measure circadian preference and stability (MESSi). Chronobiol. Int. 2016, 33, 832–848. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erren, T.C.; Reiter, R.J. Revisiting chronodisruption: When the physiological nexus between internal and external times splits in humans. Naturwissenschaften 2013, 100, 291–298. [Google Scholar] [CrossRef]
- Martinez-Nicolas, A.; Martinez-Madrid, M.J.; Almaida-Pagan, P.F.; Bonmati-Carrion, M.A.; Madrid, J.A.; Rol, M.A. Assessing Chronotypes by Ambulatory Circadian Monitoring. Front. Physiol. 2019, 10, 1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Objective | Population | Chronotype Assessment | PA Assessment | Results |
|---|---|---|---|---|---|---|
| Bodur et al., 2021 [26] | Ankara, Turkey | To determine the role of sleep quality and caffeinated beverage consumption on the effect of late chronotype on body mass index (BMI) | n = 661 healthy university students Age (mean ± SD) 21.4 ± 1.38 years | MEQ | 24 h PA record | No significant correlation was found between the chronotype scores and PA levels. |
| Culnan et al., 2013 [27] | USA | To test the relationship between chronotype in relation to BMI, energy expenditure and others | n = 137 colleges freshmen 79 females Age (mean ± SD) 18.25 ± 0.56 | Short version MEQ | Changes in short-IPAQ | Changes in IPAQ did not differ by chronotype. |
| Gubelman et al., 2018 [28] | Lausanne, Switzerland. | To evaluate the association of objective PA and sedentary behaviour (SB) with sleep duration and quality | n = 2649 adults participating in CoLaus study. 53.5% women. Age (mean ± SD) 61.6 ± 9.8 | MEQ | 14 days accelerometer | High PA (RRR = 0.71; CI:0.52–0.97) and low sedentary behaviour (0.64; 0.47; 0.86) were significantly associated with lower likelihood of EC. |
| Haraszti et al., 2014 [29] | Budapest, Hungary | To explore the relationship between morningness–eveningness and perceived health | n = 202 female working at the university. Age (mean ± SD) = 37.5 ± 10.7 years | Composite scale of morningness | Adapted version of short-IPAQ | A significant lower frequency of physical exercise was associated with EC compared to MC (2.28 ± 1.5 vs. 2.85 ± 1.65 times per week; p = 0.042). |
| Hisler et al., 2017 [30] | Iowa, USA | To analyse if diurnal preference predicts variance in exercise frequency | n = 112 university members (students and faculty). 75% females Age (mean ± SD) 25.4 ±11.6 | Composite scale of morningness | -FitBit -IPAQ | Diurnal preference (morningness) was positively correlated with self-reported exercise (r (105) = 0.36) and Fitbit exercise frequency (r (101) = 0.39). |
| Huang et al., 2021 [31] | UK | To analyse the association between sleep and PA | n = 38,601 UK Biobank participants (51% female, Age (mean ± SD) 55.7 ± 7.6 years | Combined sleep pattern variable | Weekly MET (IPAQ short-form) highly active, ≥1200; active, 600 to <1200; inactive <600) | Poor sleep pattern at baseline was associated with physical inactivity at follow-up (AOR = 1.65; 1.45–1.88) and vice versa. |
| Laborde et al., 2015 [32] | France | To explore how chronotype relates to various characteristics of sport training and competition | n = 976 non athletes + 974 athletes Women = 493 + 478 mean age 22.49 mean age: 21.21 | Caen Chronotype Questionnaire | Sports participation | Morningness–eveningness was unrelated to sport participation |
| Makarem et al., 2020 [33] | USA | To evaluate associations of chronotype with overall cardiovascular health (CVH), health behaviours and cardiometabolic risk factors | n = 506 women participants of the GO Red study. Age (mean ± SD) = 37 ± 16 year | MEQ | IPAQ sedentary activities questionnaire | EC compared to MC was associated with greater odds of not meeting PA guidelines OR (95%CI) = 1.78 (1.03–3.07). Higher MEQ scores were also associated with significantly less sedentary time β (SE) = −0.11 (0.03). |
| Mota et al., 2016 [34] | Minas Gerais, Brazil | To analyse the association between chronotype, food intake and PA | n = 72 medical residents 52 women Age (mean ± SD) 29.2 ± 2.0 | MEQ | Baecke questionnaire (BQ) | Chronotype score was positivity associated with leisure-time index (coefficient = 0.26, p = 0.03) and BQ total score (coefficient = 0.27, p = 0.03) |
| Nauha et al., 2020 [35] | Finland | To investigate an association between chronotype and objectively-measured PA and SED | n = 5156 participants Women: 2917 Age: 46 years | Short version MEQ | MET min/day (accelerometers) 14 days | Compared to EC, MC was associated with higher total (B;95%CI) (98.6; [30.2, 167.1] in men and in women (57.8; [10.5, 105.0]. Compared to EC, men with MC had less sedentary time(38.6; [−56.9, −20.2]). |
| Oliveira et al., 2021 [36] | Brazil | To investigate if PA changes might be associated with changes in the morningness–eveningness preference | n = 322 adults practicing social distancing during COVID-19 lockdown. 69% women Age (mean ± SD) 40 ± 15 | Morningness–eveningness questionnaire score | Min/week self-reported questionnaire. | Decrease in the total volume of PA was significantly associated with the increase in eveningness preference. (3.7% p = 0.001) of the variance in the changes in MEQ score) |
| Patterson et al., 2016 [37] | UK | To examine the associations among sleep duration, chronotype and other variables | n = 439 933 participants in the UK Biobank project. 56% female Age (mean ± SD): 56.5 ± 8.1 years | One question self-reported chronotype questionnaire | -Self-reported minutes/week in walking, moderate and vigorous PA. -Self-reported minutes/day using a computer or TV on a typical day. | Early chronotypes reported accruing more mean minutes of walking (0.178; 0.011), moderate (0.172; 0.012) and vigorous activity (0.172; 0.017) and less screen based sedentary behaviour (0.313; 0.011) than late chronotypes (β; SE) |
| Shechter et al., 2014 [38] | USA | To determine if sleep timing and/or quality are related to PA levels. | n = 22 participants 6 females Age range: 30–45 year | -Bedtime and wake-up time and midpoint of sleep (accelerometer) -MEQ | Accelerometers 7–18 days. Sedentary <100 cpm, light PA 100–1951, MVPA >1952 cpm | Later bedtime, wake time and midpoint of sleep are all associated with more time spent in sedentary (p < 0.02) and less time spent in light PA (p < 0.05) and MVPA (p < 0.01). Higher MEQ had a significantly higher percentage of time in MVPA compared to those in the lower MEQ group (4.64% vs. 1.99%). No differences were observed in the low versus high MEQ score subgroups in percentage of time spent in sedentary or light PA. |
| Suh et al., 2016 [39] | Korea | To investigate health behaviours, health-related quality of life (HRQOL) and sleep among chronotypes in a community-based sample | n = 2976 participants of the Korean KoGes study. 83 + 828 + 535 men Age (mean ± SD): 58.02 years ±7.05 | MEQ | METs: seven days PA Recall (retrospective self-reported) | EC were found to have significantly lower levels of PA (MET; SD = 14.54; 23.33) compared to MC (24.70; 30.41) p < 0.0001 |
| Thapa et al., 2020 [40] | Korea | To examine the association between chronotype, daily PA and the estimated risk of dementia | n = 170 community dwelling over 70 102 women Age (mean ± SD): 77.0 years (±3.7 years) | MEQ | Daily PA (accelerometer) | Higher MEQ scores showed a higher volume of PA (r = 0.42, p < 0.005) for aged >75y and (r = 0.31, p < 0.05) for ≤75y. |
| Wennman et al., 2015 [41] | Finland | To operationalize chronotype using analysis for a 6-item scale derived from the original MEQ | n = 4904 participants aged 25–74 years | Short version MEQ | -Leisure time PA, commuting PA, domestic PA (self-reported questionnaire) -Sedentary behaviours: self-reported sitting. | Evening types and the “tired, more-evening type” had higher odds for none to very low (OR [95%CI] = 3.01 [2.00, 4.53] as well as low PA (1.47 [1.01–2.13]), as compared to “morning type”. Evening type was associated with higher odds for more time spent sitting, as compared to “morning type” (1.69 [1.19, 2.41]). |
| Whittier et al., 2014 [42] | Peru | To evaluate patterns of circadian preferences and daytime sleepiness, and to examine the association between the consumption of stimulant beverages and evening chronotype | n = 2581 undergraduate students Age (mean ± SD): 21.1 ± 2.7) 61% women | MEQ | Self-reported PA (yes/no) | PA was not significantly associated with chronotype status. |
| Zhang et al., 2018 [43] | China | To explore whether increased caffeinated drinks consumption and PA can mediate the relationship between late chronotype and BMI. | n = 616 medical students Age (mean ± SD): 19.7 ± 1.1 34.9% male | MEQ | -One question self-reported moderate PA -One question self-reported sedentary behaviour. | Late chronotypes were associated with more sedentary behaviours (B = −0.05, SE = 0.01, p < 0.001) and less PA time (B= 0.12, SE = 0.01, p < 0.001) |
| Author, Year | Country | Objective | Population | Chronotype Assessment | PA Assessment | Results |
|---|---|---|---|---|---|---|
| Barrea et al., 2022 [44] | Italy | To investigate if chronotype categories could be used as tool to screen healthy habits in women with PCOS | n = 112 Women with PCOS Age (mean ± SD) 24.21 ± 5.47 years | MEQ | At least 30 min per day of exercise (yes/no) | EC did less regular exercise (6.3%) compared to MC (64.5%) or neither (39.4%) p < 0.001. |
| Farkova et al., 2019 [45] | Czech Republic | To investigate the association between circadian phenotype and PA in a weight loss programme. | n = 75 women with BMI > 25 Age (mean ± SD) 36.5; SD 8.3 | -MEQ -MCTQ -actigraphy (acrophase) | Actigraphy (mesor) | Parameters referring to the activity are not related to the acrophase. |
| Henson et al., 2020 [46] | Midlands, UK | To analyse association between chronotype and type 2 diabetes. | n = 635 participants with type 2 diabetes. 34.6% female Age (mean ± SD) = 63.8 ± 8.4 years, | MEQ | Accelerometer for 7 days | EC had higher sedentary time (28.7 min/day; 95% CI 8.6 to 48.3) and lower MVPA levels (–9.7; –14.9 to –4.6) compared to MCs. Also, later PA time for EC. |
| Romero-Cabrera et al., 2021 [47] | Spain | To explore whether individual chronotypes were associated with cardiometabolic risk in patients | n = 857 participants in Cordioprev study Age (mean ± SD): 59 ± 0.3 17.2% female | -MEQ -Actigraphy (acrophase of a combined variable TAP) | -Minnesota Leisure-Time PA questionnaire. -Sedentary behaviour | EC (MEQ and objective measures) were less active than MC (201 vs. 251 min/week; p = 0.01) and more sedentary (750 vs. 659 min/week p < 0.01) during the follow-up. |
| Vera et al., 2018 [48] | Spain | To study the relative contributions of genetics, lifestyle and circadian-related physiological characteristics in metabolic risk of evening chronotype | n = 2126 participants of the ONTIME study 1722 women Age (mean ± SD): 40 ± 13 | MEQ | -IPAQ. -Self-reported sitting duration | EC engaged in less physically activity than MC (3230 ± 225 vs. 4283 ± 217; p = 0.001) and spent longer hours sitting per day (8.1 ± 0.1 vs. 7.6 ± 0.1; p = 0.001). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sempere-Rubio, N.; Aguas, M.; Faubel, R. Association between Chronotype, Physical Activity and Sedentary Behaviour: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 9646. https://doi.org/10.3390/ijerph19159646
Sempere-Rubio N, Aguas M, Faubel R. Association between Chronotype, Physical Activity and Sedentary Behaviour: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9646. https://doi.org/10.3390/ijerph19159646
Chicago/Turabian StyleSempere-Rubio, Nuria, Mariam Aguas, and Raquel Faubel. 2022. "Association between Chronotype, Physical Activity and Sedentary Behaviour: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 15: 9646. https://doi.org/10.3390/ijerph19159646
APA StyleSempere-Rubio, N., Aguas, M., & Faubel, R. (2022). Association between Chronotype, Physical Activity and Sedentary Behaviour: A Systematic Review. International Journal of Environmental Research and Public Health, 19(15), 9646. https://doi.org/10.3390/ijerph19159646