
What Drives Elderly People in China Away from COVID-19 Information?


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Survey Questionnaire
2.2.1. Sociodemographic Characteristics
2.2.2. Health Information Avoidance Scale (HIAS)
2.2.3. COVID-19 Information Overload Scale (CIOS)
2.2.4. General Self-Efficacy Scale (GSES)
2.2.5. Chinese Version of the Health Anxiety Inventory (CHAI)
2.3. Statistical Methods
3. Results
3.1. Sociodemographic Characteristics of the Participants
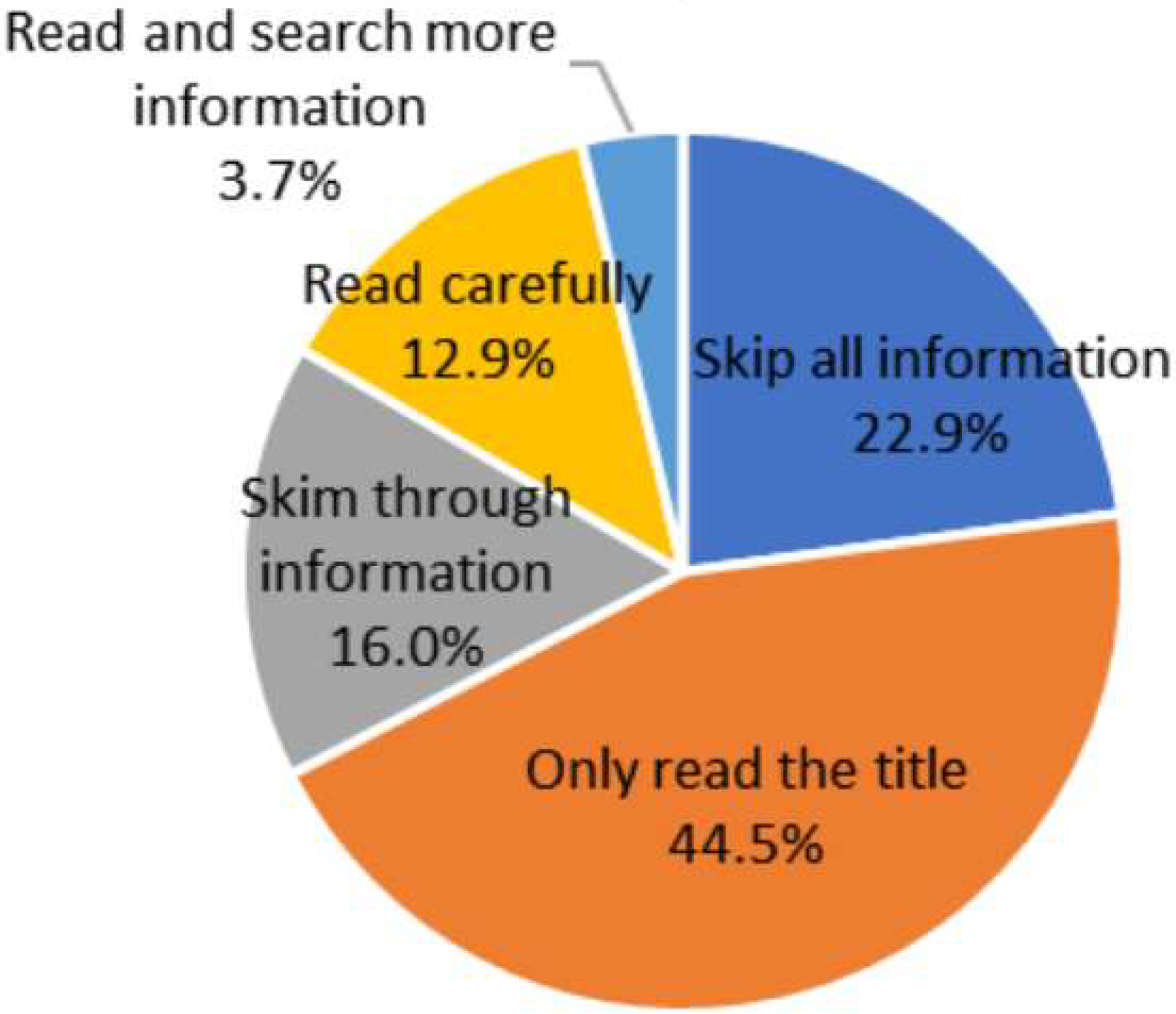
3.2. Avoidance of COVID-19 Information among Elderly People
3.3. COVID-19 Information Overload among Elderly People
3.4. Self-Efficacy of the Elderly
3.5. Health Anxiety among the Elderly
3.6. Comparison of Different Sociodemographic Elderly People’s COVID-19 Information Avoidance
3.7. Multiple-Factor Analysis of COVID-19 Information Avoidance among Elderly People
4. Discussion
4.1. COVID-19 Information Avoidance among Elderly People
4.2. Factors Associated with COVID-19 Information Avoidance among Elderly People
4.3. Recommendations
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, X.; Xu, X.; Cheng, J. Wechatting for health: What motivates older adult engagement with health information. Healthcare 2021, 9, 751. [Google Scholar] [CrossRef] [PubMed]
- Van Pinxteren, M.; Cooper, S.; Colvin, C.J. Barriers and opportunities to using health information in policy implementation: The case of adolescent and youth friendly health services in the Western Cape. Afr. J. Prim. Health Care Fam. Med. 2021, 13, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.; Salami, B.; Salma, J.; Yohani, S.; Amin, M.; Okeke-Ihejirika, P.; Ladha, T. Health information seeking among immigrant families in western Canada. J. Pediatr. Nurs. 2021, 58, 9–14. [Google Scholar] [CrossRef]
- Wang, X.; Shi, J.; Kong, H. Online health information seeking: A review and meta-analysis. Health Commun. 2021, 36, 1163–1175. [Google Scholar] [CrossRef] [PubMed]
- Ansari, A.; Fahimfar, N.; Noruzi, A.; Fahimifar, S.; Hajivalizadeh, F.; Ostovar, A.; Larijani, B.; Sanjari, M. Health information-seeking behavior and self-care in women with osteoporosis: A qualitative study. Arch. Osteoporos. 2021, 16, 78. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhan, W.; Zheng, C.; Zhang, J.; Huang, A.; Hu, S.; Ba-Thein, W. Online health information-seeking behaviors and skills of Chinese college students. BMC Public Health 2021, 21, 736. [Google Scholar] [CrossRef] [PubMed]
- Eibich, P.; Goldzahl, L. Health information provision, health knowledge and health behaviours: Evidence from breast cancer screening. Soc. Sci. Med. 2020, 265, 113505. [Google Scholar] [CrossRef]
- Gao, X.; Wang, Z.; Kong, C.; Fan, H.; Zhang, J.; Wang, J.; Tan, L.; Wang, J. Cross-sectional survey to assess health-care workers’ grief counseling for bereaved families of COVID-19 victims in Wuhan, China. Disaster Med. Public Health Prep. 2021, 30, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, M.; Stark, B.; Werner, A.M.; Tibubos, A.N.; Reichel, J.L.; Pfirrmann, D.; Edelmann, D.; Heller, S.; Mülder, L.M.; Rigotti, T.; et al. Health information seeking among university students before and during the corona crisis-findings from germany. Front. Public Health 2021, 8, 616603. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Yuan, J.; Dong, M.; Yang, L.; Fielding, R.; Lam, W.W.T. Public engagement and government responsiveness in the communications about COVID-19 during the early epidemic stage in China: Infodemiology study on social media data. J. Med. Internet Res. 2020, 22, e18796. [Google Scholar] [CrossRef]
- Berdida, D.J.E.; Grande, R.A.N.; Lopez, V. Filipinos’ health information-seeking behaviors and their implications for COVID-19 vaccination. Public Health Nurs. 2022, 39, 553–561. [Google Scholar] [CrossRef] [PubMed]
- González-Padilla, D.A.; Tortolero-Blanco, L. Social media influence in the COVID-19 pandemic. Int. Braz. J. Urol. 2020, 46, 120–124. [Google Scholar] [CrossRef]
- Valika, T.S.; Maurrasse, S.E.; Reichert, L. A second pandemic? Perspective on information overload in the COVID-19 era. Otolaryngol. Head Neck Surg. 2020, 163, 931–933. [Google Scholar] [CrossRef]
- Soroya, S.H.; Farooq, A.; Mahmood, K.; Isoaho, J.; Zara, S. From information seeking to information avoidance: Understanding the health information behavior during a global health crisis. Inf. Process. Manag. 2021, 58, 102440. [Google Scholar] [CrossRef] [PubMed]
- Lipsey, N.P.; Shepperd, J.A. Powerful audiences are linked to health information avoidance: Results from two surveys. Soc. Sci. Med. 2019, 225, 51–59. [Google Scholar] [CrossRef]
- Brashers, D.E.; Goldsmith, D.J.; Hsieh, E. Information seeking and avoiding in health contexts. Hum. Commun. Res. 2002, 28, 258–271. [Google Scholar] [CrossRef]
- Barbour, J.B.; Rintamaki, L.S.; Ramsey, J.A.; Brashers, D.E. Avoiding health information. J. Health Commun. 2012, 17, 212–229. [Google Scholar] [CrossRef]
- Jung, M.; Ramanadhan, S.; Viswanath, K. Effect of information seeking and avoidance behavior on self-rated health status among cancer survivors. Patient Educ. Couns. 2013, 92, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Hua, J.; Howell, J.L. Coping self-efficacy influences health information avoidance. J. Health Psychol. 2022, 27, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Han, Z. Study on health information avoidance behavior of rural residents in the context of low-risk diseases. Chin. J. Agric. Inf. 2021, 33, 12. [Google Scholar]
- Zhang, J. Status of the public accessing to information and emotional impact during the COVID-19. J. Jinan Uni. 2020, 41, 527–533. [Google Scholar]
- Hudson, A.; Montelpare, W.J. Predictors of Vaccine Hesitancy: Implications for COVID-19 Public Health Messaging. Int. J. Environ. Res. Public Health 2021, 29, 8054. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.; Willis, D.E.; Shah, S.K.; Purvis, R.S.; Shields, X.; McElfish, P.A. “The Risk Seems Too High”: Thoughts and Feelings about COVID-19 Vaccination. Int. J. Environ. Res. Public Health 2021, 18, 8690. [Google Scholar] [CrossRef] [PubMed]
- Aloweidi, A.; Bsisu, I.; Suleiman, A.; Abu-Halaweh, S.; Almustafa, M.; Aqel, M.; Amro, A.; Radwan, N.; Assaf, D.; Abdullah, M.Z.; et al. Hesitancy towards COVID-19 Vaccines: An Analytical Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5111. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Zhou, J. The impact of COVID-19 on Shenzhen and Hong Kong. Shanghai J. City Manag. 2022, 31, 72–78. [Google Scholar]
- Wang, Y.Y. Influential factors on the olds’ avoidance behavior of health Information. Chin. J. Agric. Inf. Explore 2018, 7, 24–29. [Google Scholar]
- Song, S.; Yao, X.; Wen, N. What motivates Chinese consumers to avoid information about the COVID-19 pandemic?: The perspective of the stimulus-organism-response model. Inf. Process. Manag. 2021, 58, 102407. [Google Scholar] [CrossRef] [PubMed]
- Link, E. Information avoidance during health crises: Predictors of avoiding information about the COVID-19 pandemic among german news consumers. Inf. Process. Manag. 2021, 58, 102714. [Google Scholar] [CrossRef]
- Chen, X.; Li, M.; Kreps, G.L. Double burden of COVID-19 knowledge deficit: Low health literacy and high information avoidance. BMC Res. Notes 2022, 15, 27. [Google Scholar] [CrossRef]
- Buneviciene, I.; Bunevicius, R.; Bagdonas, S. COVID-19 media fatigue: Predictors of decreasing interest and avoidance of COVID-19-related news. Public Health 2021, 196, 124–128. [Google Scholar] [CrossRef]
- Siebenhaar, K.U.; Köther, A.K.; Alpers, G.W. Dealing with the COVID-19 infodemic: Distress by information, information avoidance, and compliance with preventive measures. Front. Psychol. 2020, 11, 567905. [Google Scholar] [CrossRef] [PubMed]
- Shuai, Z.; Ma, F.C. Research on the construction of health information avoidance scale. Chin. Lib. Inf. 2020, 64, 3–9. [Google Scholar]
- Yang, Z.; Shen, X.; Kang, K. Development of information overload severity scale in the situation of coronavirus disease 2019 epidemic. Huaxi Med. 2021, 36, 449–452. [Google Scholar]
- Sherer, M.; Maddux, J.E.; Mercandante, B. The self-efficacy scale: Construction and validation. Psychol. Rep. 1982, 51, 663–671. [Google Scholar] [CrossRef]
- Wang, C.; Hu, Z.; Liu, Y. Reliability and validity of general self efficacy scale. Chin. J. Psychol. 2001, 7, 37–40. [Google Scholar]
- Salkovskis, P.; Rimes, K.; Warwick, H.M.C.; Clark, D. The health anxiety inventory: Development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychol. Med. 2002, 32, 843–853. [Google Scholar] [CrossRef]
- Zhou, Y. Reliability and validity of Chinese version of the health anxiety inventory. Chin. J. Clin. Psychol. 2017, 25, 471–474. [Google Scholar]
- Gao, X.; Li, H.; He, W.; Zeng, W. COVID-19 Vaccine Hesitancy Among Medical Students: The Next COVID-19 Challenge in Wuhan, China. Disaster Med. Public Health Prep. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zi, Y. Influencing factors and promotion path of social security in major emergencies. J. Anyang Inst. Technol. 2022, 21, 33–35. [Google Scholar]
- Xie, Y. Psychological status and influencing factors of employees in a disease prevention and control system under the normalization of COVID-19 prevention and control. Chin. J. Dis. Control Prev. 2022, 26, 604–610. [Google Scholar]
- Ai, W.; Hu, G.; Zhao, Y. Research on influencing factors of health information avoidance behavior: Exploration based on meta-analysis. Inf. Doc. Serv. 2021, 42, 63–73. [Google Scholar]
- Gong, W. Triggering and compensation: Generational relations and health information avoidance of the old. Chin. J. Commun. 2018, 40, 47–63. [Google Scholar]

{kind=link}
| Item | Total Points ( ± S) | Average Points of Items (Mean ± S) | Score Rates (%) |
|---|---|---|---|
| HIAS | 30.64 ± 7.70 | 3.06 ± 0.77 | 61.28 |
| Negative emotions | 12.28 ± 4.12 | 3.07 ± 1.03 | 61.40 |
| Cognitive conflict | 8.65 ± 2.26 | 2.88 ± 0.75 | 57.67 |
| Behavioral changes | 9.72 ± 2.40 | 3.24 ± 0.80 | 64.80 |
| Reason | n | % |
|---|---|---|
| COVID-19 has been well controlled in China and there is no need to pay attention to related information. | 527 | 58.1 |
| COVID-19 information can cause negative emotions, such as fear, anxiety and sadness. | 412 | 45.4 |
| I was overwhelmed with too much COVID-19 information. | 612 | 67.5 |
| Too much false COVID-19 information, which is difficult to distinguish. | 223 | 24.6 |
| Most of the COVID-19 information is useless to me. | 512 | 56.4 |
| I have been vaccinated against COVID-19, so I feel safe. | 285 | 31.4 |
| Other | 82 | 9.0 |
| Factor | n (%) | HIAS Total Points ( ± S) | F | p |
|---|---|---|---|---|
| Gender | 3.090 | 0.079 | ||
| Male | 425 (46.9) | 30.16 ± 7.50 | ||
| Female | 482 (53.1) | 31.06 ± 7.85 | ||
| Age | 55.901 | 0.000 | ||
| 60–69 | 417 (46.0) | 27.96 ± 8.21 | ||
| 70–79 | 331 (36.5) | 32.35 ± 6.33 | ||
| >79 | 159 (17.5) | 34.14 ± 6.42 | ||
| Education level | 1.911 | 0.149 | ||
| Primary school | 428 (47.2) | 30.45 ± 7.93 | ||
| Middle school | 392 (43.2) | 31.12 ± 7.13 | ||
| University | 87 (9.6) | 29.46 ± 8.83 | ||
| Employment status | 7.195 | 0.007 | ||
| Employed | 145 (16.0) | 29.08 ± 7.93 | ||
| Retired | 762 (84.0) | 30.94 ± 7.62 | ||
| Marital status | 1.886 | 0.152 | ||
| Married | 624 (68.8) | 30.75 ± 8.15 | ||
| Divorced or widowed | 227 (25.0) | 30.83 ± 6.54 | ||
| Single | 56 (6.2) | 28.71 ± 6.52 | ||
| Have children or not | 39.281 | 0.000 | ||
| Have children | 724 (79.8) | 29.85 ± 7.22 | ||
| Have no children | 183 (20.2) | 33.77 ± 8.68 | ||
| Monthly income | 1.813 | 0.164 | ||
| <USD 620 | 444 (49.0) | 31.04 ± 8.00 | ||
| USD 620–USD 1240 | 308 (34.0) | 30.55 ± 6.97 | ||
| >USD 1240 | 155 (17.1) | 29.69 ± 8.13 | ||
| Place of residence | 2.223 | 0.109 | ||
| Own home | 706 (77.8) | 30.47 ± 7.15 | ||
| Nursing home | 107 (11.8) | 30.37 ± 8.68 | ||
| Other locations | 94 (10.4) | 32.22 ± 10.02 | ||
| Religion | 1.738 | 0.188 | ||
| Nonreligious | 713 (78.6) | 30.47 ± 7.61 | ||
| Religious | 194 (21.4) | 31.29 ± 7.99 | ||
| COVID-19 vaccination | 4.842 | 0.028 | ||
| Unvaccinated | 253 (27.9) | 31.55 ± 6.26 | ||
| Vaccinated | 654 (72.1) | 30.29 ± 8.16 |
| Independent Variable | Regression Coefficient | Standardized Regression Coefficient | t | p |
|---|---|---|---|---|
| Constant | 7.658 | - | 5.623 | <0.001 |
| COVID-19 information overload | 0.381 | 0.253 | 8.153 | <0.001 |
| Age | 2.122 | 0.205 | 6.957 | <0.001 |
| Health anxiety | 0.289 | 0.217 | 6.989 | <0.001 |
| Have children or not | 2.733 | 0.143 | 4.979 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, X.; Ding, F.; Ai, T. What Drives Elderly People in China Away from COVID-19 Information? Int. J. Environ. Res. Public Health 2022, 19, 9509. https://doi.org/10.3390/ijerph19159509
Gao X, Ding F, Ai T. What Drives Elderly People in China Away from COVID-19 Information? International Journal of Environmental Research and Public Health. 2022; 19(15):9509. https://doi.org/10.3390/ijerph19159509
Chicago/Turabian StyleGao, Xudong, Feng Ding, and Ting Ai. 2022. "What Drives Elderly People in China Away from COVID-19 Information?" International Journal of Environmental Research and Public Health 19, no. 15: 9509. https://doi.org/10.3390/ijerph19159509
APA StyleGao, X., Ding, F., & Ai, T. (2022). What Drives Elderly People in China Away from COVID-19 Information? International Journal of Environmental Research and Public Health, 19(15), 9509. https://doi.org/10.3390/ijerph19159509