
Effects of an Online Supervised Exercise Training in Children with Obesity during the COVID-19 Pandemic

 ,
,  , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
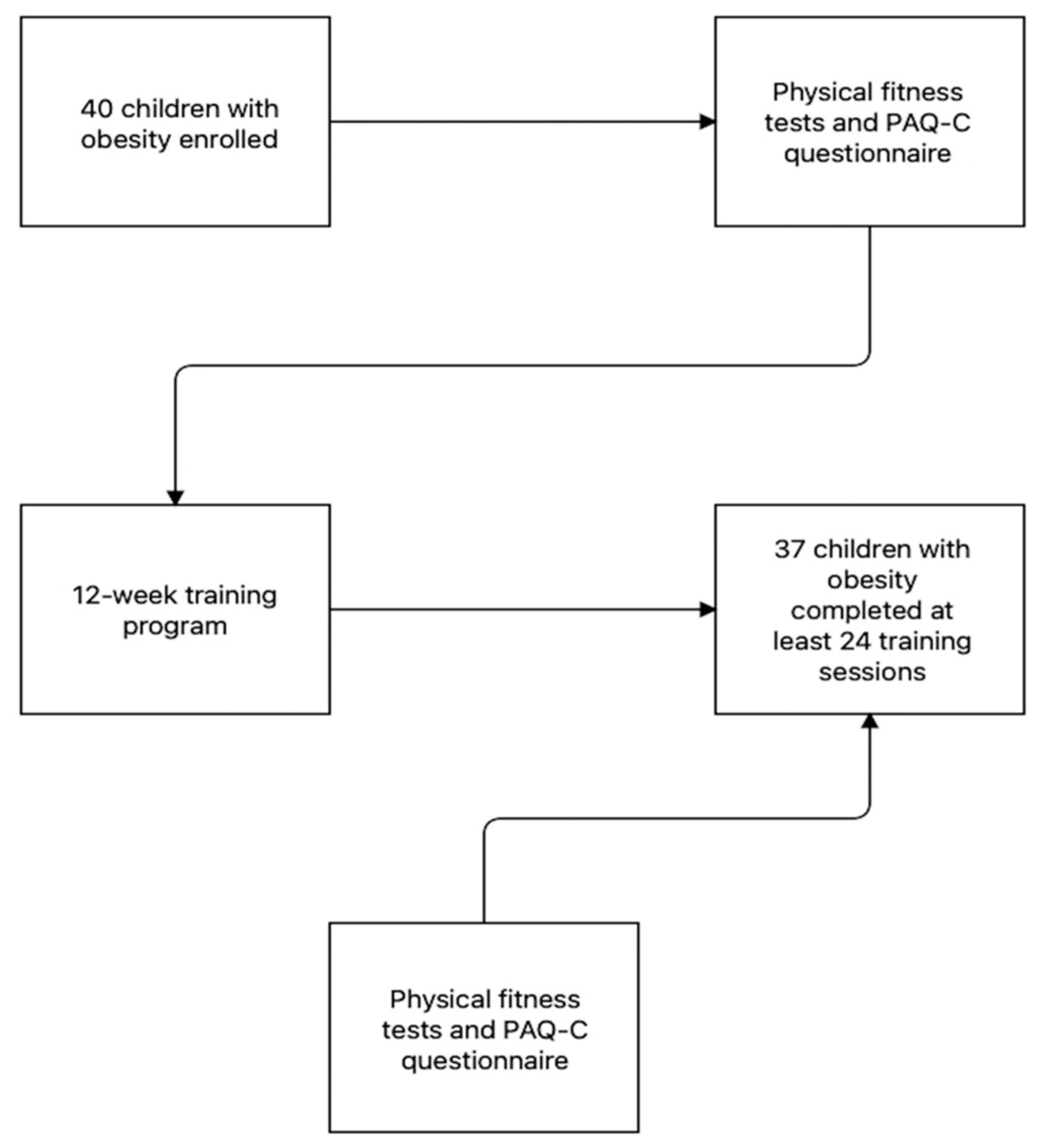
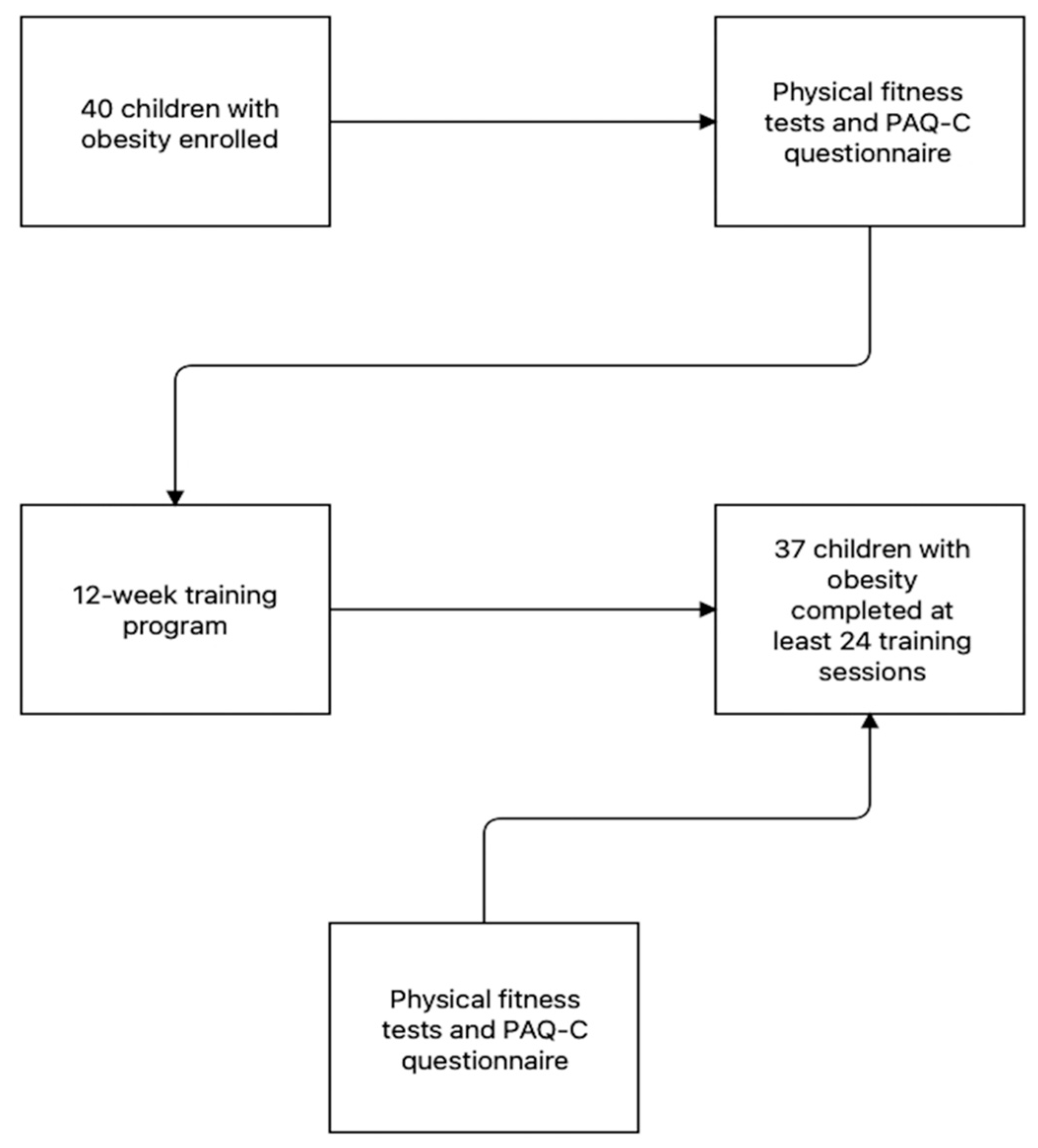
2.1. Participants
2.2. Anthropometric Characteristics
2.3. The Physical Activity Questionnaire for Older Children (PAQ-C)
2.4. Children’s Effort Rating Table
2.5. Physical Fitness Tests
2.6. Standing Broad Jump (SBJ)
2.7. 6 Min Walking Test (6MWT)
2.8. 5 × 10 m Sprint Test
2.9. Training Protocol
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gatti, A.; Pugliese, L.; Carnevale Pellino, V.; Del Bianco, M.; Vandoni, M.; Lovecchio, N. Self-Declared Physical Activity Levels and Self-Reported Physical Fitness in a Sample of Italian Adolescents during the COVID-19 Pandemic. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Tornaghi, M.; Lovecchio, N.; Vandoni, M.; Chirico, A.; Codella, R. Physical Activity Levels across COVID-19 Outbreak in Youngsters of Northwestern Lombardy. J. Sports Med. Phys. Fitness 2021, 61, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Dallolio, L.; Marini, S.; Masini, A.; Toselli, S.; Stagni, R.; Bisi, M.C.; Gori, D.; Tessari, A.; Sansavini, A.; Lanari, M.; et al. The Impact of COVID-19 on Physical Activity Behaviour in Italian Primary School Children: A Comparison before and during Pandemic Considering Gender Differences. BMC Public Health 2022, 22, 52. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, Eating Behavior and Physical Activity during COVID-19 Lockdown: A Study of UK Adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef]
- Wijga, A.H.; Scholtens, S.; Bemelmans, W.J.E.; de Jongste, J.C.; Kerkhof, M.; Schipper, M.; Sanders, E.A.; Gerritsen, J.; Brunekreef, B.; Smit, H.A. Comorbidities of Obesity in School Children: A Cross-Sectional Study in the PIAMA Birth Cohort. BMC Public Health 2010, 10, 184. [Google Scholar] [CrossRef] [Green Version]
- Engin, A. The Definition and Prevalence of Obesity and Metabolic Syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar] [CrossRef]
- Valerio, G.; Maffeis, C.; Saggese, G.; Ambruzzi, M.A.; Balsamo, A.; Bellone, S.; Bergamini, M.; Bernasconi, S.; Bona, G.; Calcaterra, V.; et al. Diagnosis, Treatment and Prevention of Pediatric Obesity: Consensus Position Statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics. Ital. J. Pediatr. 2018, 44, 88. [Google Scholar] [CrossRef] [Green Version]
- Arpesella, M.; Campostrini, S.; Gerzeli, S.; Lottaroli, S.; Pane, A.; Traverso, M.; Vandoni, M.; Coppola, L. Obesity Nutritional Aspects and Life Style from a Survey on a Sample of Primary School Pupils in the Pavia Province (Northern Italy). Ital. J. Public Health 2008, 5, 12–17. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 19 May 2022).
- Saltiel, A.R.; Olefsky, J.M. Inflammatory Mechanisms Linking Obesity and Metabolic Disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [Green Version]
- Melo, L.C.; Silva, M.A.M.D.; Calles, A.C.D.N. Obesity and Lung Function: A Systematic Review. Einstein 2014, 12, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting Obesity in Young Adulthood from Childhood and Parental Obesity. N. Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Elagizi, A.; Kachur, S.; Carbone, S.; Lavie, C.J.; Blair, S.N. A Review of Obesity, Physical Activity, and Cardiovascular Disease. Curr. Obes. Rep. 2020, 9, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Nemet, D.; Barkan, S.; Epstein, Y.; Friedland, O.; Kowen, G.; Eliakim, A. Short- and Long-Term Beneficial Effects of a Combined Dietary-Behavioral-Physical Activity Intervention for the Treatment of Childhood Obesity. Pediatrics 2005, 115, e443–e449. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramírez-Vélez, R.; Ramírez-Campillo, R.; Peterson, M.D.; Martínez-Vizcaíno, V. Concurrent Aerobic plus Resistance Exercise versus Aerobic Exercise Alone to Improve Health Outcomes in Paediatric Obesity: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2018, 52, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1·6 Million Participants. Lancet Child. Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Lovecchio, N.; Zago, M. Fitness Differences According to BMI Categories: A New Point of View. J. Sports Med. Phys. Fit. 2019, 59, 298–303. [Google Scholar] [CrossRef]
- Lovecchio, N.; Novak, D.; Sedlacek, J.; Hamar, P.; Milanovic, I.; Radisavljevic-Janic, S.; Emeljanovas, A.; Eid, L.; Zago, M. Physical Fitness for Sedentary Students: A Common Trend from Six European Countries. J. Sports Med. Phys. Fit. 2019, 59, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- Natalucci, V.; Carnevale Pellino, V.; Barbieri, E.; Vandoni, M. Is It Important to Perform Physical Activity During Coronavirus Pandemic (COVID-19)? Driving Action for a Correct Exercise Plan. Front. Public Health 2020, 8, 602020. [Google Scholar] [CrossRef]
- Carnevale Pellino, V.; Giuriato, M.; Ceccarelli, G.; Codella, R.; Vandoni, M.; Lovecchio, N.; Nevill, A.M. Explosive Strength Modeling in Children: Trends According to Growth and Prediction Equation. Appl. Sci. 2020, 10, 6430. [Google Scholar] [CrossRef]
- Kokkinos, P.; Myers, J.; Faselis, C.; Panagiotakos, D.B.; Doumas, M.; Pittaras, A.; Manolis, A.; Kokkinos, J.P.; Karasik, P.; Greenberg, M.; et al. Exercise Capacity and Mortality in Older Men: A 20-Year Follow-up Study. Circulation 2010, 122, 790–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandoni, M.; Calcaterra, V.; Pellino, V.C.; De Silvestri, A.; Marin, L.; Zuccotti, G.V.; Tranfaglia, V.; Giuriato, M.; Codella, R.; Lovecchio, N. “Fitness and Fatness” in Children and Adolescents: An Italian Cross-Sectional Study. Children 2021, 8, 762. [Google Scholar] [CrossRef] [PubMed]
- Vandoni, M.; Lovecchio, N.; Carnevale Pellino, V.; Codella, R.; Fabiano, V.; Rossi, V.; Zuccotti, G.V.; Calcaterra, V. Self-Reported Physical Fitness in Children and Adolescents with Obesity: A Cross-Sectional Analysis on the Level of Alignment with Multiple Adiposity Indexes. Children 2021, 8, 476. [Google Scholar] [CrossRef]
- Tarp, J.; Støle, A.P.; Blond, K.; Grøntved, A. Cardiorespiratory Fitness, Muscular Strength and Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetologia 2019, 62, 1129–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical Fitness in Childhood and Adolescence: A Powerful Marker of Health. Int. J. Obes 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, E.A.; Sui, X.; Brellenthin, A.G.; Lee, D.-C. Physical Activity and Fitness for the Prevention of Hypertension. Curr. Opin. Cardiol. 2018, 33, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Rohatgi, A.; Ayers, C.R.; Willis, B.L.; Haskell, W.L.; Khera, A.; Drazner, M.H.; de Lemos, J.A.; Berry, J.D. Cardiorespiratory Fitness and Classification of Risk of Cardiovascular Disease Mortality. Circulation 2011, 123, 1377–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrann, C.D.; White, J.P.; Salogiannnis, J.; Laznik-Bogoslavski, D.; Wu, J.; Ma, D.; Lin, J.D.; Greenberg, M.E.; Spiegelman, B.M. Exercise Induces Hippocampal BDNF through a PGC-1α/FNDC5 Pathway. Cell Metab. 2013, 18, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory Fitness as a Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and Women: A Meta-Analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [Green Version]
- Calcaterra, V.; Verduci, E.; Vandoni, M.; Rossi, V.; Di Profio, E.; Carnevale Pellino, V.; Tranfaglia, V.; Pascuzzi, M.C.; Borsani, B.; Bosetti, A.; et al. Telehealth: A Useful Tool for the Management of Nutrition and Exercise Programs in Pediatric Obesity in the COVID-19 Era. Nutrients 2021, 13, 3689. [Google Scholar] [CrossRef]
- Vandoni, M.; Codella, R.; Pippi, R.; Carnevale Pellino, V.; Lovecchio, N.; Marin, L.; Silvestri, D.; Gatti, A.; Magenes, V.C.; Regalbuto, C.; et al. Combatting Sedentary Behaviors by Delivering Remote Physical Exercise in Children and Adolescents with Obesity in the COVID-19 Era: A Narrative Review. Nutrients 2021, 13, 4459. [Google Scholar] [CrossRef]
- Calcaterra, V.; Winickoff, J.P.; Klersy, C.; Schiano, L.M.; Bazzano, R.; Montalbano, C.; Musella, V.; Regalbuto, C.; Larizza, D.; Cena, H. Smoke Exposure and Cardio-Metabolic Profile in Youth with Type 1 Diabetes. Diabetol. Metab. Syndr. 2018, 10, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcaterra, V.; De Giuseppe, R.; Biino, G.; Mantelli, M.; Marchini, S.; Bendotti, G.; Madè, A.; Avanzini, M.A.; Montalbano, C.; Cossellu, G. Relation between Circulating Oxidized-LDL and Metabolic Syndrome in Children with Obesity: The Role of Hypertriglyceridemic Waist Phenotype. J. Pediatric Endocrinol. Metab. 2017, 30, 1257–1263. [Google Scholar] [CrossRef] [PubMed]
- Dot, G.; Rafflenbeul, F.; Kerbrat, A.; Rouch, P.; Gajny, L.; Schouman, T. Three-Dimensional Cephalometric Landmarking and Frankfort Horizontal Plane Construction: Reproducibility of Conventional and Novel Landmarks. J. Clin. Med. 2021, 10, 5303. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Grummer-Strawn, L.M. Standard Deviation of Anthropometric Z-Scores as a Data Quality Assessment Tool Using the 2006 WHO Growth Standards: A Cross Country Analysis. Bull. World Health Organ. 2007, 85, 441–448. [Google Scholar] [CrossRef]
- Marshall, W.A.; Tanner, J.M. Variations in Pattern of Pubertal Changes in Girls. Arch. Dis. Child. 1969, 44, 291. [Google Scholar] [CrossRef] [Green Version]
- Marshall, W.A.; Tanner, J.M. Variations in the Pattern of Pubertal Changes in Boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Benítez-Porres, J.; López-Fernández, I.; Raya, J.F.; Álvarez Carnero, S.; Alvero-Cruz, J.R.; Álvarez Carnero, E. Reliability and Validity of the PAQ-C Questionnaire to Assess Physical Activity in Children. J. Sch. Health 2016, 86, 677–685. [Google Scholar] [CrossRef]
- Lamb, K.L. Children’s Ratings of Effort during Cycle Ergometry: An Examination of the Validity of Two Effort Rating Scales. Pediatric Exerc. Sci. 1995, 7, 407–421. [Google Scholar] [CrossRef]
- Skowronski, W.; Horvat, M.; Nocera, J.; Roswal, G.; Croce, R. Eurofit Special: European Fitness Battery Score Variation among Individuals with Intellectual Disabilities. Adapt. Phys. Activ. Q 2009, 26, 54–67. [Google Scholar] [CrossRef]
- Sport, C. of E.C. for the D. of EUROFIT: Handbook for the EUROFIT Tests of Physical Fitness; Sports Division Strasbourg, Council of Europe Publishing and Documentation Service: Strasbourg, France, 1983.
- Tomkinson, G.; Olds, T. Field Tests of Fitness. In Paediatric Exercise Science and Medicine, 2nd ed.; Academic: Oxford, UK, 2008; pp. 109–128. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavón, D.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-Based Fitness Assessment in Young People: The ALPHA Health-Related Fitness Test Battery for Children and Adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef]
- Fernandez-Santos, J.R.; Ruiz, J.R.; Cohen, D.D.; Gonzalez-Montesinos, J.L.; Castro-Piñero, J. Reliability and Validity of Tests to Assess Lower-Body Muscular Power in Children. J. Strength Cond. Res. 2015, 29, 2277–2285. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An Official European Respiratory Society/American Thoracic Society Technical Standard: Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef] [PubMed]
- Vandoni, M.; Correale, L.; Puci, M.V.; Galvani, C.; Codella, R.; Togni, F.; La Torre, A.; Casolo, F.; Passi, A.; Orizio, C.; et al. Six Minute Walk Distance and Reference Values in Healthy Italian Children: A Cross-Sectional Study. PLoS ONE 2018, 13, e0205792. [Google Scholar] [CrossRef]
- Li, A.M.; Yin, J.; Yu, C.C.W.; Tsang, T.; So, H.K.; Wong, E.; Chan, D.; Hon, E.K.L.; Sung, R. The Six-Minute Walk Test in Healthy Children: Reliability and Validity. Eur. Respir. J. 2005, 25, 1057–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donncha, C.M.; Watson, A.W.S.; McSweeney, T.; O’Donovan, D.J. Reliability of Eurofit Physical Fitness Items for Adolescent Males with and without Mental Retardation. Adapt. Phys. Act. Q. 1999, 16, 86–95. [Google Scholar] [CrossRef]
- Meng, C.; Yucheng, T.; Shu, L.; Yu, Z. Effects of School-Based High-Intensity Interval Training on Body Composition, Cardiorespiratory Fitness and Cardiometabolic Markers in Adolescent Boys with Obesity: A Randomized Controlled Trial. BMC Pediatr. 2022, 22, 112. [Google Scholar] [CrossRef] [PubMed]
- Schwingshandl, J.; Sudi, K.; Eibl, B.; Wallner, S.; Borkenstein, M. Effect of an Individualised Training Programme during Weight Reduction on Body Composition: A Randomised Trial. Arch. Dis. Child. 1999, 81, 426–428. [Google Scholar] [CrossRef] [PubMed]
- Son, W.-M.; Sung, K.-D.; Bharath, L.P.; Choi, K.-J.; Park, S.-Y. Combined Exercise Training Reduces Blood Pressure, Arterial Stiffness, and Insulin Resistance in Obese Prehypertensive Adolescent Girls. Clin. Exp. Hypertens. 2017, 39, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Shih, K.-C.; Kwok, C.-F. Exercise Reduces Body Fat and Improves Insulin Sensitivity and Pancreatic β-Cell Function in Overweight and Obese Male Taiwanese Adolescents. BMC Pediatr. 2018, 18, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, C.J.; Rejeski, W.J. Not What, but How One Feels: The Measurement of Affect during Exercise. J. Sport Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Wagner, B.; Seuser, A.; Krüger, S.; Herzig, M.L.; Hilberg, T.; Ay, C.; Hasenöhrl, T.; Crevenna, R. Establishing an Online Physical Exercise Program for People with Hemophilia. Wien. Klin. Wochenschr. 2019, 131, 558–566. [Google Scholar] [CrossRef] [Green Version]
- Antwi, F.; Fazylova, N.; Garcon, M.-C.; Lopez, L.; Rubiano, R.; Slyer, J.T. The Effectiveness of Web-Based Programs on the Reduction of Childhood Obesity in School-Aged Children: A Systematic Review. JBI Libr. Syst. Rev. 2012, 10, 1–14. [Google Scholar] [CrossRef]
- Calcaterra, V.; Iafusco, D.; Pellino, V.C.; Mameli, C.; Tornese, G.; Chianese, A.; Cascella, C.; Macedoni, M.; Redaelli, F.; Zuccotti, G.; et al. “CoVidentary”: An Online Exercise Training Program to Reduce Sedentary Behaviours in Children with Type 1 Diabetes during the COVID-19 Pandemic. J. Clin. Transl. Endocrinol. 2021, 25, 100261. [Google Scholar] [CrossRef]
- Calcaterra, V.; Klersy, C.; Muratori, T.; Telli, S.; Caramagna, C.; Scaglia, F.; Cisternino, M.; Larizza, D. Prevalence of Metabolic Syndrome (MS) in Children and Adolescents with Varying Degrees of Obesity. Clin. Endocrinol. 2008, 68, 868–872. [Google Scholar] [CrossRef]
- Calcaterra, V.; Zuccotti, G. Physical Exercise as a Non-Pharmacological Intervention for Attenuating Obesity-Related Complications in Children and Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 5046. [Google Scholar] [CrossRef]
- Amato, A.; Santoro, N.; Calabrò, P.; Grandone, A.; Swinkels, D.W.; Perrone, L.; del Giudice, E.M. Effect of Body Mass Index Reduction on Serum Hepcidin Levels and Iron Status in Obese Children. Int. J. Obes 2010, 34, 1772–1774. [Google Scholar] [CrossRef] [Green Version]
- Kirk, S.; Zeller, M.; Claytor, R.; Santangelo, M.; Khoury, P.R.; Daniels, S.R. The Relationship of Health Outcomes to Improvement in BMI in Children and Adolescents. Obes. Res. 2005, 13, 876–882. [Google Scholar] [CrossRef]
- Kolsgaard, M.L.P.; Joner, G.; Brunborg, C.; Anderssen, S.A.; Tonstad, S.; Andersen, L.F. Reduction in BMI Z-Score and Improvement in Cardiometabolic Risk Factors in Obese Children and Adolescents. The Oslo Adiposity Intervention Study—A Hospital/Public Health Nurse Combined Treatment. BMC Pediatr. 2011, 11, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinehr, T.; Lass, N.; Toschke, C.; Rothermel, J.; Lanzinger, S.; Holl, R.W. Which Amount of BMI-SDS Reduction Is Necessary to Improve Cardiovascular Risk Factors in Overweight Children? J. Clin. Endocrinol. Metab. 2016, 101, 3171–3179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcaterra, V.; Vandoni, M.; Debarbieri, G.; Larizza, D.; Albertini, R.; Arpesella, M.; Bernardi, L. Deep Breathing Improves Blunted Baroreflex Sensitivity in Obese Children and Adolescents with Insulin Resistance. Int. J. Cardiol. 2013, 168, 1614–1615. [Google Scholar] [CrossRef]
- Olson, K.L.; Neiberg, R.H.; Espeland, M.A.; Johnson, K.C.; Knowler, W.C.; Pi-Sunyer, X.; Staiano, A.E.; Wagenknecht, L.E.; Wing, R.R. Look AHEAD Research Group Waist Circumference Change during Intensive Lifestyle Intervention and Cardiovascular Morbidity and Mortality in the Look AHEAD Trial. Obesity 2020, 28, 1902–1911. [Google Scholar] [CrossRef] [PubMed]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-Height Ratio Is a Better Screening Tool than Waist Circumference and BMI for Adult Cardiometabolic Risk Factors: Systematic Review and Meta-Analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas Fuentes, G.; Bawaked, R.A.; Martínez González, M.Á.; Corella, D.; Subirana Cachinero, I.; Salas-Salvadó, J.; Estruch, R.; Serra-Majem, L.; Ros, E.; Lapetra Peralta, J.; et al. Association of Physical Activity with Body Mass Index, Waist Circumference and Incidence of Obesity in Older Adults. Eur. J. Public Health 2018, 28, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Pancar, Z.; Özdal, M.; Çinar, V. The effect of 4-weekly low intensity physical activity program in thyroid hormone levels in obese and overweight children. Eur. J. Phys. Educ. Sport Sci. 2017, 3, 11. [Google Scholar]
- Bethea, T.C.; Berry, D.; Maloney, A.E.; Sikich, L. Pilot Study of an Active Screen Time Game Correlates with Improved Physical Fitness in Minority Elementary School Youth. Games Health J. 2012, 1, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.; Chen, C.; Sui, M.; Xue, L.; Wang, J. Exercise Training Improved Body Composition, Cardiovascular Function, and Physical Fitness of 5-Year-Old Children With Obesity or Normal Body Mass. Pediatr. Exerc. Sci. 2017, 29, 245–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pienaar, A.E.; Du Toit, D.; Truter, L. The Effect of a Multidisciplinary Physical Activity Intervention on the Body Composition and Physical Fitness of Obese Children. J. Sports Med. Phys. Fit. 2013, 53, 415–427. [Google Scholar]
- Romero-Pérez, E.M.; González-Bernal, J.J.; Soto-Cámara, R.; González-Santos, J.; Tánori-Tapia, J.M.; Rodríguez-Fernández, P.; Jiménez-Barrios, M.; Márquez, S.; de Paz, J.A. Influence of a Physical Exercise Program in the Anxiety and Depression in Children with Obesity. Int. J. Environ. Res. Public Health 2020, 17, 4655. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-J.; Noh, B.; An, K.-O. Impact of Synchronous Online Physical Education Classes Using Tabata Training on Adolescents during COVID-19: A Randomized Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 10305. [Google Scholar] [CrossRef] [PubMed]
- Molina-Garcia, P.; Mora-Gonzalez, J.; Migueles, J.H.; Rodriguez-Ayllon, M.; Esteban-Cornejo, I.; Cadenas-Sanchez, C.; Plaza-Florido, A.; Gil-Cosano, J.J.; Pelaez-Perez, M.A.; Garcia-Delgado, G.; et al. Effects of Exercise on Body Posture, Functional Movement, and Physical Fitness in Children with Overweight/Obesity. J. Strength Cond. Res. 2020, 34, 2146–2155. [Google Scholar] [CrossRef]
- Muros, J.J.; Salvador Pérez, F.; Zurita Ortega, F.; Gámez Sánchez, V.M.; Knox, E. The Association between Healthy Lifestyle Behaviors and Health-Related Quality of Life among Adolescents. J. Pediatr. 2017, 93, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The Influence of Physical Activity, Sedentary Behavior on Health-Related Quality of Life among the General Population of Children and Adolescents: A Systematic Review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef] [Green Version]
- Benítez-Porres, J.; Alvero-Cruz, J.R.; Sardinha, L.B.; López-Fernández, I.; Carnero, E.A. Cut-off Values for Classifying Active Children and Adolescents Using the Physical Activity Questionnaire: PAQ-C and PAQ-A. Nutr. Hosp. 2016, 33, 564. [Google Scholar] [CrossRef]

{kind=link}
| Warm-Up (5–10 min) | Aerobic Interval Training (20 min) | Muscular Strength (20 min) | Cool-Down (5–10 min) | |
|---|---|---|---|---|
| Type of exercises | Mobility exercises (e.g.,. head, lower and upper body mobility routine) | Motor tales (e.g., “a journey through the woods”, children imagined being in the woods completing different tasks, which included different aerobic activities (run, jumping, march …) | Strength circuit for children (e.g., semi-squat, push-up, glute bridge, triceps dip … all exercises were performed free weight) | Yoga for children (e.g., child pose, reverse warrior, cobra pose, seated forward fold, corpse pose …) |
| Active music video (the music video was performed by children imitating the dancers) | Animal walks (e.g., bear crawl, frog jump, bunny hop, dinosaur walk) | Imitation games (e.g., imitation of multiple sport techniques and gestures) | ||
| Intensity | 4–5 CERT | 7–8 CERT | 7–8 CERT | 3–4 CERT |
| Before TP | After TP | p-Value | |
|---|---|---|---|
| Weight -kilograms (kg) -percentiles § | 65.74 ±17.88 97.18 ± 3.58 | 65.80 ± 15.77 97.20 ± 4.0 | 0.78 0.96 |
| Height -meters -percentiles § | 1.49 ± 0.10 50.90 ± 31.38 | 1.51 ± 0.11 59.70 ± 32.06 | 0.36 0.28 |
| Waist Circumference (cm) | 90.54 ± 11.21 | 88.22 ±10.86 | 0.027 * |
| WHtR | 0.59 ± 0.13 | 0.56 ± 0.12 | 0.005 * |
| BMI | 28.74 ± 4.10 | 28.50 ± 3.55 | >0.05 |
| -BMI z-score -percentiles § | 2.20 ± 0.22 99.37 ± 0.89 | 2.16 ± 0.25 98.89 ± 1.86 | 0.006 ** 0.19 |
| Before | After | p-Value | Effect Size | |
|---|---|---|---|---|
| SBJ (cm) | 99.29 ± 20.16 | 109.29 ± 22.84 | <0.001 *** | 0.853 |
| 6MWT (m) | 479.50 ± 61.11 | 534 ± 61.08 | <0.001 *** | 1.08 |
| 5 × 10 m (s) | 19.91 ± 2.45 | 18.93 ± 1.91 | 0.014 * | 0.496 |
| Before | After | p-Value | Effect Size | |
|---|---|---|---|---|
| CERT 6MWT | 4.00 (3.00–6.00; 3) | 5.00 (2.75–6.25; 3.50) | 0.638 | 0.080 |
| CERT 5 × 10 m | 5.00 (4.00–7.00; 3.00) | 5.00 (4.00–7.00; 3.00) | 0.245 | 0.184 |
| PAQ-C | 1.97 (1.65–2.24; 0.585) | 2.27 (1.78–2.59; 0.810) | 0.050 * | 0.400 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vandoni, M.; Carnevale Pellino, V.; Gatti, A.; Lucini, D.; Mannarino, S.; Larizza, C.; Rossi, V.; Tranfaglia, V.; Pirazzi, A.; Biino, V.; et al. Effects of an Online Supervised Exercise Training in Children with Obesity during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9421. https://doi.org/10.3390/ijerph19159421
Vandoni M, Carnevale Pellino V, Gatti A, Lucini D, Mannarino S, Larizza C, Rossi V, Tranfaglia V, Pirazzi A, Biino V, et al. Effects of an Online Supervised Exercise Training in Children with Obesity during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(15):9421. https://doi.org/10.3390/ijerph19159421
Chicago/Turabian StyleVandoni, Matteo, Vittoria Carnevale Pellino, Alessandro Gatti, Daniela Lucini, Savina Mannarino, Cristiana Larizza, Virginia Rossi, Valeria Tranfaglia, Agnese Pirazzi, Valentina Biino, and et al. 2022. "Effects of an Online Supervised Exercise Training in Children with Obesity during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 15: 9421. https://doi.org/10.3390/ijerph19159421
APA StyleVandoni, M., Carnevale Pellino, V., Gatti, A., Lucini, D., Mannarino, S., Larizza, C., Rossi, V., Tranfaglia, V., Pirazzi, A., Biino, V., Zuccotti, G., & Calcaterra, V. (2022). Effects of an Online Supervised Exercise Training in Children with Obesity during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(15), 9421. https://doi.org/10.3390/ijerph19159421