
COVID-19 School vs. Community-Based Outbreak Trends among New Jersey K–12 Schools during the 2020–2021 School Year

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. COVID-19 Surveillance Data
2.2. Sociodemographic Data
3. Results
3.1. COVID-19 Surveillance Data
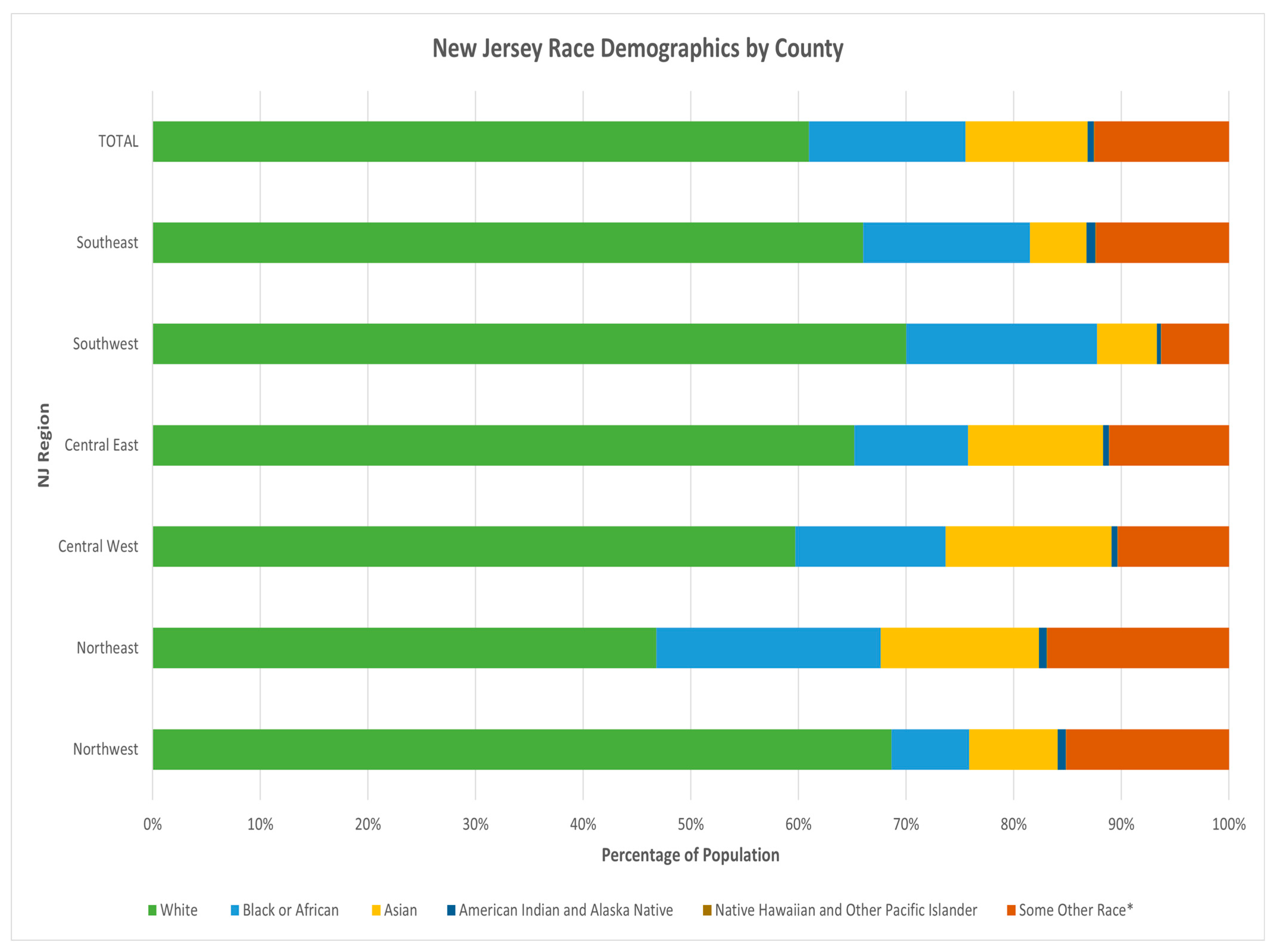
3.2. Sociodemographic Data
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Recommendations for Future Research, Policy, and Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Know What to Expect at Your Child’s K-12 School or Early Care and Education Program. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/groups/expect-school-child-care.html (accessed on 7 March 2022).
- Giardina, J.; Bilinski, A.; Fitzpatrick, M.C.; Kendall, E.A.; Linas, B.P.; Salomon, J.; Ciaranello, A.L. Model-Estimated Association between Simulated US Elementary School–Related SARS-CoV-2 Transmission, Mitigation Interventions, and Vaccine Coverage Across Local Incidence Levels. JAMA Netw. Open 2022, 5, e2147827. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.M.; Omer, S.B.; Gilliam, W.S. Differences in State COVID-19 Vaccine Mandates for Schoolteachers and Childcare Professionals. JAMA Pediatr. 2022, 176, 522. [Google Scholar] [CrossRef]
- Rutgers School of Public Health. NJ Safe Schools Program—Our Mission. Available online: https://sph.rutgers.edu/training/nj-safe-schools/index.html (accessed on 7 March 2022).
- Communicable Disease Service, New Jersey Department of Health. New Jersey COVID-19 Dashboard. 2022. Available online: https://www.nj.gov/health/cd/topics/covid2019_dashboard.shtml (accessed on 21 February 2022).
- Office of New Jersey Governor. New Jersey Executive Orders. 2022. Available online: https://nj.gov/infobank/eo/056murphy/ (accessed on 21 February 2022).
- Communicable Disease Service, Department of Health. COVID-19 Weekly CALI and Variant Surveillance Reports. 2022. Available online: https://www.nj.gov/health/cd/statistics/covid/ (accessed on 14 February 2022).
- United States Census Bureau. Decennial Census: Age and Sex. Explore Census Data. 2022. Available online: https://data.census.gov/cedsci/table?g=0400000US34%240500000&tid=ACSST1Y2019.S0101 (accessed on 21 February 2022).
- United States Census Bureau. Decennial Census: Race. Explore Census Data. 2022. Available online: https://data.census.gov/cedsci/table?g=0400000US34%240500000 (accessed on 21 February 2022).
- NJ Department of Health (NJDOH). NJDOH NJ CALI Report for U.S. CDC MMWR Week 22 (4 June 2022). Available online: https://www.nj.gov/health/cd/documents/topics/NCOV/COVID_19_Report_Week_2022_22.pdf (accessed on 21 June 2022).
- Arco, M.; Cohen, N.N.J. Teachers, Day Care Workers Can Get COVID Vaccine Immediately, Not on Date Previously Announced. Available online: https://www.nj.com/coronavirus/2021/03/nj-teachers-day-care-workers-can-get-covid-vaccine-immediately-not-on-date-previously-announced.html (accessed on 6 October 2021).
- Arco, M.; All, N.J. Residents Age 16 and over Will Be Eligible for COVID Vaccine Beginning April 19, Murphy Announces. Available online: https://www.nj.com/coronavirus/2021/04/all-nj-residents-age-16-and-over-will-be-eligible-for-covid-vaccine-beginning-april-19-murphy-announces.html (accessed on 6 October 2021).


{kind=link}
{kind=link}
{kind=link}
| 5–9 Years | 10–14 Years | 15–17 Years | 18–19 Years | 20–24 Years | |
|---|---|---|---|---|---|
| Northwest | 8.79 | 12.38 | 9.26 | 3.15 | 2.93 |
| Morris County | 9.91 | 15.29 | 10.80 | 1.81 | 2.02 |
| Passaic County | 8.69 | 8.99 | 6.16 | 6.33 | 3.78 |
| Sussex County | 8.84 | 30.62 | 23.75 | 18.43 | 4.47 |
| Warren County | 5.61 | 16.22 | 27.04 | 1.70 | 4.31 |
| Northeast | 9.63 | 10.11 | 7.82 | 2.83 | 1.98 |
| Bergen County | 6.05 | 7.54 | 6.33 | 3.55 | 1.76 |
| Essex County | 21.71 | 13.31 | 9.42 | 2.58 | 2.98 |
| Hudson County | 9.97 | 11.90 | 9.33 | 2.28 | 1.54 |
| Central West | 9.08 | 9.12 | 7.62 | 2.56 | 1.75 |
| Hunterdon County | 20.82 | 11.33 | 7.16 | 10.32 | 1.25 |
| Mercer County | 11.07 | 10.00 | 11.58 | 2.29 | 1.47 |
| Somerset County | 6.57 | 7.79 | 5.68 | 2.33 | 2.82 |
| Central East | 4.21 | 6.10 | 6.03 | 3.91 | 2.29 |
| Middlesex County | 7.41 | 13.56 | 14.39 | 9.62 | 2.97 |
| Monmouth County | 5.25 | 9.74 | 5.71 | 2.14 | 1.29 |
| Ocean County | 1.32 | 1.80 | 2.20 | 2.52 | 1.69 |
| Union County | 17.55 | 18.80 | 14.20 | 3.46 | 4.66 |
| Southwest | 7.45 | 9.35 | 6.87 | 5.48 | 3.68 |
| Burlington County | 6.63 | 11.75 | 7.60 | 4.20 | 2.93 |
| Camden County | 8.77 | 6.68 | 6.69 | 5.18 | 4.33 |
| Gloucester County | 5.68 | 14.93 | 6.36 | 7.67 | 4.02 |
| Salem County | 90.28 | 8.23 | 6.38 | 18.49 | 4.29 |
| Southeast | 12.62 | 20.62 | 13.44 | 7.04 | 3.46 |
| Atlantic County | 8.22 | 19.35 | 10.67 | 13.99 | 4.48 |
| Cape May County | 35.78 | 17.45 | 40.60 | 1.00 | 1.47 |
| Cumberland County | 21.50 | 24.69 | 14.85 | 5.52 | 2.80 |
| Statewide/State of NJ | 6.79 | 8.82 | 7.36 | 3.48 | 2.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aggarwal, J.; Gichura, M.W.; Campbell, M.L.F.; Nguyen, K.T.; Shendell, D.G. COVID-19 School vs. Community-Based Outbreak Trends among New Jersey K–12 Schools during the 2020–2021 School Year. Int. J. Environ. Res. Public Health 2022, 19, 9285. https://doi.org/10.3390/ijerph19159285
Aggarwal J, Gichura MW, Campbell MLF, Nguyen KT, Shendell DG. COVID-19 School vs. Community-Based Outbreak Trends among New Jersey K–12 Schools during the 2020–2021 School Year. International Journal of Environmental Research and Public Health. 2022; 19(15):9285. https://doi.org/10.3390/ijerph19159285
Chicago/Turabian StyleAggarwal, Juhi, Maureen W. Gichura, Maryanne L. F. Campbell, Kimberly T. Nguyen, and Derek G. Shendell. 2022. "COVID-19 School vs. Community-Based Outbreak Trends among New Jersey K–12 Schools during the 2020–2021 School Year" International Journal of Environmental Research and Public Health 19, no. 15: 9285. https://doi.org/10.3390/ijerph19159285
APA StyleAggarwal, J., Gichura, M. W., Campbell, M. L. F., Nguyen, K. T., & Shendell, D. G. (2022). COVID-19 School vs. Community-Based Outbreak Trends among New Jersey K–12 Schools during the 2020–2021 School Year. International Journal of Environmental Research and Public Health, 19(15), 9285. https://doi.org/10.3390/ijerph19159285