
Workplace Interventions to Reduce Occupational Stress for Older Workers: A Systematic Review


Abstract
:1. Introduction
- (1)
- Identify and appraise papers evaluating the effectiveness of workplace stress reduction interventions on older workers.
- (2)
- Describe the types of interventions and measures of effectiveness used
- (3)
- Summarise the evidence of effectiveness of interventions
- (4)
- Identify existing knowledge gaps in the literature which require further research
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
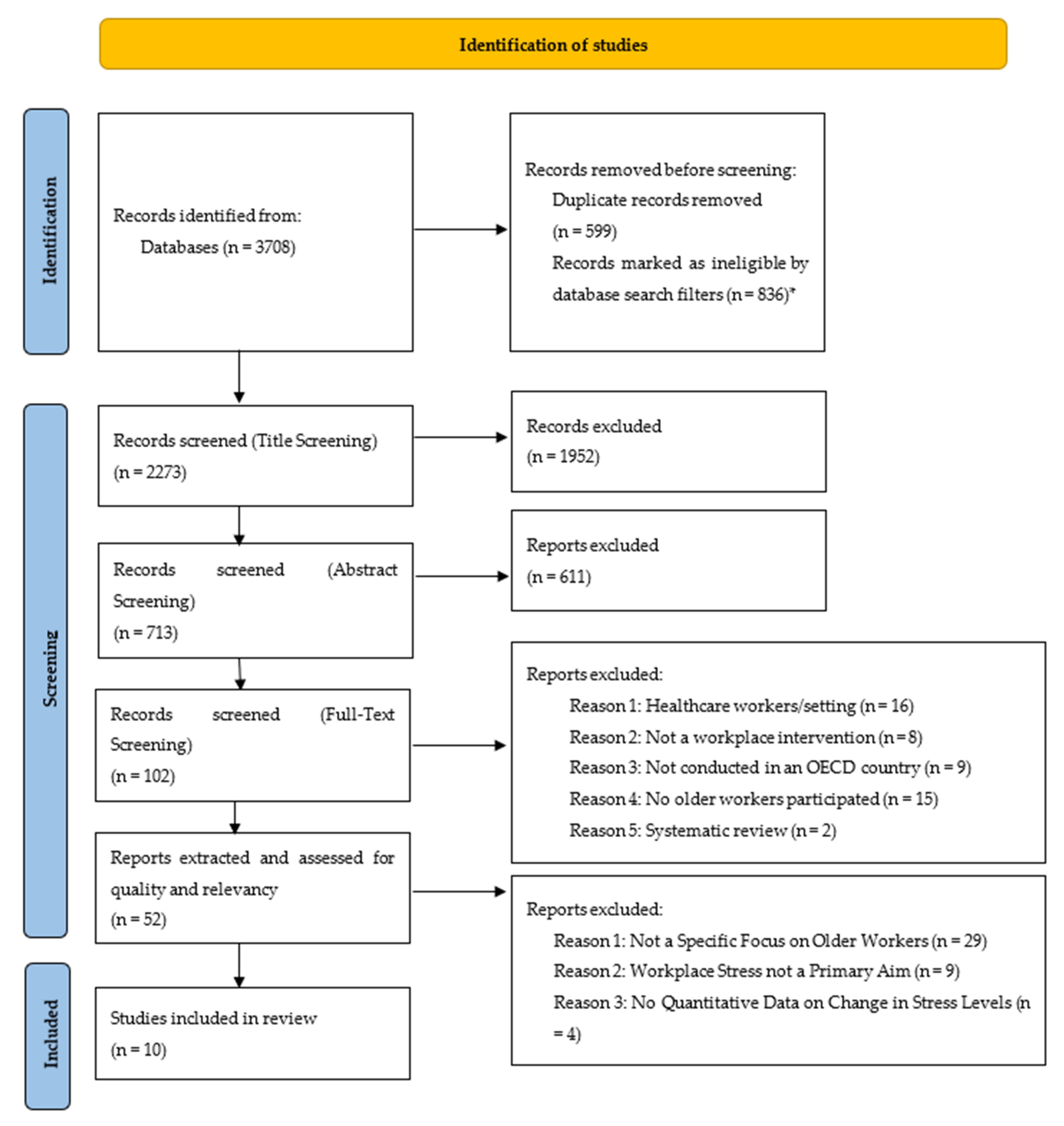
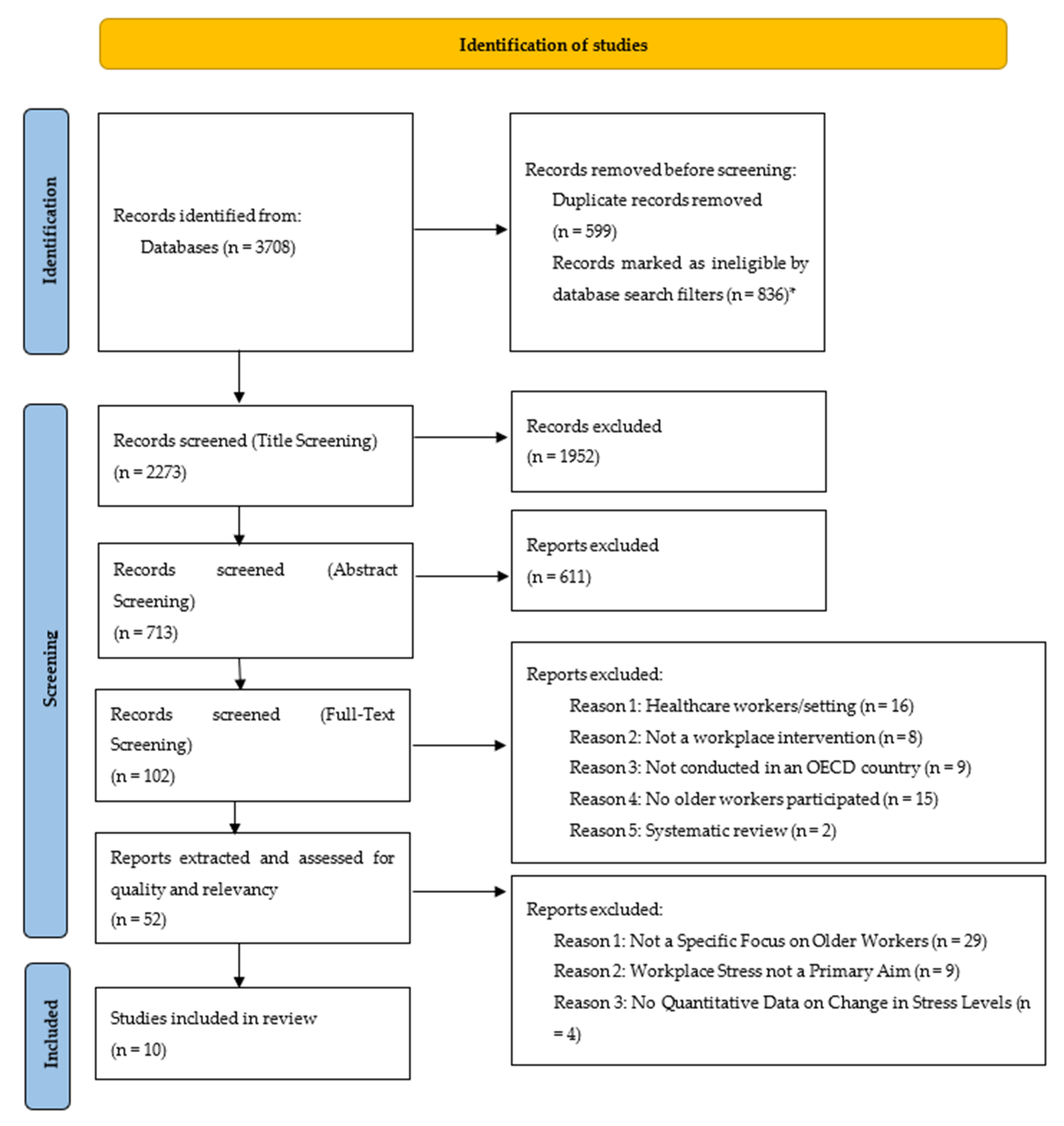
2.3. Study Selection and Screening
2.4. Data Extraction and Critical Appraisal
3. Results
3.1. Characteristics of Included Studies

{kind=link}
| Study (First Author, Year) | Country | Study Design | Focus on Older Workers? | Participant’s Occupation | Age of Participants | No. of Participants (and Dropouts) |
|---|---|---|---|---|---|---|
| Primary Dataset | ||||||
| Hughes, 2011 [17] | United States | Randomised Controlled Trial (RCT) | Yes | University Staff | 51 (Mean) | 423 (56 Dropouts) |
| Malarkey, 2013 [18] | United States | Randomised Controlled Trial | Yes | University Faculty Staff | 50 (Mean) | 186 (0 Dropouts) |
| Cook, 2015 [20] | United States | Randomised Controlled Trial | Yes | Tech Company Workers | 59 (Median) * 50–68 (Range) | 278 (0 Dropouts) |
| Fischetti, 2019 [25] | Italy | Randomised Controlled Trial | Yes | Police Officers | 46.8 (Mean) | 20 (0 Dropouts) |
| Calogiuri, 2016 [26] | Norway | Randomised Controlled Trial | Yes | Office Workers | 49 (Median) * 41–47 (Range) | 14 (3 Dropouts) |
| Secondary Dataset | ||||||
| Aikens, 2014 [19] | United States | Randomised Controlled Trial | No | Chemical Company Employees | 41.5 (Median) * 18–65 (Range) | 89 (23 Dropouts) |
| Largo-Wight, 2017 [21] | United States | Randomised Controlled Trial | No | University Office Staff | 48.8 (Mean) | 37 (0 Dropouts) |
| Limm, 2011 [22] | Germany | Randomised Controlled Trial | No | Lower and Middle Level Managers at a Manufacturing Plant | 40.9 (Mean) 18–65 (Range) | 174 (20 Dropouts) |
| Hoeve, 2021 [23] | Netherlands | Quasi-Experimental | No | Police Officers | 49 (Mean) 30–63 (Range) | 82 (19 Dropouts) |
| Ojala, 2019 [24] | Finland | Non-Randomised Trial | No | Public Sector Workers * | 49.9 (Mean) 21–64 (Range) | 779 (217 Dropouts) |
3.2. Risk of Bias
3.3. Study Methods
3.4. Study Findings
4. Discussion
4.1. Main Findings
4.2. Methodological Considerations
4.3. Interpretation of Findings and Comparison to Previous Studies
4.4. The Significance of the Review and Public Health Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Study Number | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Data Set Decision | PRIMARY DATA SET | PRIMARY DATA SET | PRIMARY DATA SET | PRIMARY DATA SET | PRIMARY DATA SET |
| Study Information | |||||
| Database No. | WoS154 | WoS321 | O1587 | O1320 | O1544 |
| Author(s) | Francesco Fischetti, Stefania Cataldi, Francesca Latino & Gianpiero Greco | Giovanna Calogiuri, Katinka Evensen, Andi Weydahl, Kim Andersson, Grete Patil, Camilla Ihlebæk and Ruth Raanaas | Royer F Cook, Rebekah K Hersch, Dana Schlossberg, Samantha L Leaf | William B. Malarkey, David Jarjoura, Maryanna Klatt | Susan L. Hughes, Rachel B. Seymour, Richard T. Campbell, James W. Shaw, Camille Fabiyi and Rosemary Sokas |
| Year | 2019 | 2016 | 2015 | 2013 | 2011 |
| Link to Article | https://rua.ua.es/dspace/bitstream/10045/96031/1/JHSE_14_Proc4_53.pdf | https://brage.inn.no/inn-xmlui/bitstream/handle/11250/2380639/Work_2015_Calogiuri.pdf?sequence=1&isAllowed=y | https://www.jmir.org/2015/3/e82 | https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3528077/ | https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2010.300082 |
| Access Date | 8 June 2022 | 8 June 2022 | 8 June 2022 | 8 June 2022 | 8 June 2022 |
| Title of Article | “Effectiveness of multilateral training didactic method on physical and mental wellbeing in law enforcement” | Green exercise as a workplace intervention to reduce job stress. Results from a pilot study | A Web-Based Health Promotion Program for Older Workers:Randomized Controlled Trial | Workplace based mindfulness practice and inflammation: a randomized trial. | Comparison of two health-promotion programs for older workers. |
| Country | Italy | Norway | United States | United States | United States |
| Intervention | |||||
| Study Aim | to investigate the effects of an 8-week multilateral training program on physical and mental wellbeing in policemen | to explore possible effects of green-exercise interventions in the workplace on psychological and physiological indicators of stress. | to evaluate the impact of a multimedia Web-based health promotion program on central health attitudes and practices of older workers. | This study focused on working adults who could benefit from lifestyle intervention strategies. In comparing the mindfulness intervention to the lifestyle education program, we focused on three biologic measures of chronic stress and inflammation | to examine the effects of 2 worksite health-promotion interventions (compared with a health-education control) on older workers’ healthy behaviors and health outcomes. |
| Type of Intervention | Multilateral training program on physical and mental well-being | Exercise-based Intervention | Web-based program to address a wide variety of health behavior topics, including physical activity, healthy eating, stress management, and tobacco cessation | Mindfulness Intervention | health-promotion intervention and health-education control |
| Duration of Intervention | 8 Weeks | 2 Weeks | 3 months | 8 weeks | 12 months |
| Location of Intervention | Police Offices | outdoors in a green/nature area or in an indoor exercise-setting | Online intervention | University Offices | at university worksite |
| Study Design | Randomised Controlled Trial | Between Subjects Randomised Controlled Trial | Randomised Controlled Trial | randomized controlled trial | randomized controlled trial |
| Methods | |||||
| How were participants recruited? | recruited in the police offices of the Puglia region (Italy) between January and February 2019, healthy males belonging to the State Police voluntarily participated | healthy employees, sedentary or moderately active, in two workplaces in a small town in the north of Norway who responded to an invitation to participate in the study by e-mail | A recruitment flyer briefly describing the purpose of the study was emailed by company officials to all employees 50 years of age and older (approximately 2500 employees) located in multiple US offices of a global information technology company. The flyer stated that the study was being conducted by a research organization through a grant from the National Institutes of Health. The flyer also explained that participants would receive US $25 for completing the first questionnaire and US $25 for completing the second questionnaire, and that their name would be entered into a drawing in which 1 participant would receive US $500 during each questionnaire round. Interested employees who fit the inclusion criteria (age 50 and older) were instructed to contact the project staff directly by email or telephone. | PARTICIPANTS: were recruited from faculty and staff of The Ohio State University. Advertising promoted the trial as a life style intervention program and the types of interventions were not specified, with participants unaware of the intervention type until the first day of the actual intervention | Participants were recruited via announcements on staff listservs, targeted e-mails, staffed recruitment tables at events in highly trafficked buildings, and flyers posted throughout the university. |
| Occupation of Participants | Police Officers | Office Workers | employees of a large global information technology company | University Faculty Staff | Research participants were older support and academic staff at the University of Illinois at Chicago |
| Specific Focus on Older Workers? | No | No | Yes | Not specific - but mean age is high | Yes |
| Outcome Measurement | the sources of stress and coping strategies, and the physical and mental state of health perceived were measured by the Occupational Stress Indicator and the Short Form-12 | Self-reported affective state was measured by the Physical Activity Affective Scale (PAAS), which place feeling states within four factors corresponding to the quadrants circumplex model of affect and arousal: ‘Positive Affect’, ‘Tranquility’, ‘Negative Affect’, and ‘Fatigue’ AND Two measures of cortisol as an indicator of stress were used: Cortisol Awakening Response (CAR) and serum concentration. Saliva samples were selfadministered by the subjects for the determination of the CAR the morning after each session. | Twelve items assessing the type of strategies one uses to cope with difficult situations and events. Questions are answered on a 4-point scale ranging from 1 (never) to 4 (almost always); higher score = better coping. Typical questions included “I often put things aside for a while to get perspective on them” and “I decide certain problems are not worth worrying about” | CRP, IL-6, Cortisol, BP and Perceived Stress Scale Questionnaires | We investigated change from baseline to 6 months and 12 months in 4 measures of stress. We used the Perceived Stress Scale to measure overall stress during the preceding month. We used a 4-item scale developed by Lorig et al. to assess health-related stress, and we used the Brief COPE to assess use of positive and negative coping behaviors |
| Data Collection Style | Self report questionnaires | Self report questionnaires and Cortisol levels in serum were measured by professional nurses through blood test the morning after each session between 8:00 and 9:00 AM | self report survey | Via blood tests, saliva samples for cortisol and self reported questionnaires | self reported questionnaire |
| How were the Results analysed? | Pre and Post Intervention | Comparison to Control, and Pre and Post Intervention | Comparison to Control, and Pre and Post Intervention | Comparison to Control, and Pre and Post Intervention | Comparison to control and other intervention |
| Results | |||||
| No. of Participants | 20 | 14 | 278 | 186 | 423 |
| Dropout Rate | 0 Dropouts | 11: 3 dropouts/lost to f/u | Zero Dropouts | 16 dropouts/lost to follow up | 56 dropouts/lost to follow up |
| Age of Workers | Mean = 46.8 (SD 3.9) | Range = 41–57 | Participants ranged in age from 50 to 68 years | Mean age = Education group—49, MBI-Id—51 | Mean age = 51, participants were all aged 40 years and older |
| Any other condition of workers? | No | No | No | No—participants were excluded if they had a known condition which enhances inflammation and a psychiatric disorder other than depression | No |
| Change in Stress Levels | experimental group perceived less stress, showed a more realistic attitude towards the various working situations and a greater perception of physical and mental wellbeing than control group (p < 0.05). | Concerning the PAAS components, a significant effect of group was found for Positive Affect when corrected for baseline values, with higher ratings reported by the nature group No significant differences between groups were found for cortisol concentration in serum | There were no differences between the program and control groups on symptoms of distress or coping with stress. The estimated adjusted posttest different between program and control group is 0.01 for Coping with Stress | Cortisol at Baseline in Education group was 0.15, mean at follow up is 0.12; MBI-id group at baseline is 0.10 and followup mean is 0.11. The mindfulness intervention was effective as the MBI-ld group demonstrated greater self reported mindfulness than the education group at 2 months. This difference was sustained at 6 and 12 months: With measures of depression (CES-D), stress (Perceived Stress Scale), sleep quality (PSQI), no significant differences were found at 2-months. The global test across all five produced a p-value of 0.91. The PSS measure, however, asked the questions in reference to the past week rather than the past month as is the standard format, which permitted an evaluation of the intervention at completion.Using an extensive pre and post MBI-ld salivary cortisol sampling protocol we saw no decrease in cortisol levels | No significant differences were seen for COACH or RealAge participants on any of the 4 stress outcomes at either time point |
| Intervention deemed effective/ successful | It has been found that police officers perceived fewer sources of pressure after intervention and specifically: working days are lived with less stress | Green-exercise at the workplace could be a profitable way to manage stress and induce restoration among employees. | Significant program effects were not shown on measures of stress | The trial was designed to test whether MBI-ld was superior to an education control in lowering cortisol, IL-6 and CRP immediately at the end of the interventions. We did not confirm this hypothesis. MBSR in smaller observational studies has been reported by some but not all investigators to lower cortisol levels when the intervention is compared to a wait list control group | The differences in the findings of our respective studies raises important questions about whether a dose---response relationship exists between comprehensiveness of services offered, and whether certain program components, such as incentives, are more effective and more critical than others. |
| Key Conclusions | public policies are needed to promote the practice of physical activities as continuing education, including leisure and sports activities, and to promote the psychological stability, work efficiency, changes in living habits, improvements in wellbeing and, therefore, improvements in quality of life. | it also provides some evidence that green-exercise interventions in the workplace can be a more valuable resource than ‘traditional’ indoor exercise in promoting health among employees, especially reducing psychological as well as physiological stress. | A Web-based health promotion program showed promise for making a significant contribution to the short-term dietary and exercise practices of older working adults. The findings suggest that a multimedia Web-based program could be a promising vehicle for delivering health promotion material to older working adults. | MBI-ld significantly enhanced mindfulness by 2 months and it was maintained for up to a year when compared to the education control. We did not see any significant changes in self-report measures for depressive symptoms, perceived stress, or sleep quality. Most but not all MBSR investigations have found improvements in these areas when the intervention is compared to a wait list control group. We have performed a randomized trial with a compressed MBSR intervention in which instruction and practice occurred in the workplace. This reduced the barriers commonly mentioned for non-participation in MBSR programs. Adherence to the program was greater than 90% for 8 weeks (evidenced by weekly attendance/practice sheets) even though the subjects were unaware that mindfulness meditation was one of the lifestyle interventions being offered. Additionally, mindfulness was achieved and sustained for at least one year. It is possible that a more intense intervention would have produced more significant effects. We conclude that MBI-ld should be more fully investigated as a low-cost self-directed complementary strategy for reducing inflammation. | If we can reach older adults while they are still working and engage them in sustained health-promotion activities, we may be able to delay morbidity onset, thereby reducing cost to employers as well as future Medicare expenditures |
| Discussion | |||||
| Author Identified Weaknesses | the small number of police officers recruited due to the difficulties encountered during the organizational phase in obtaining the necessary authorizations and having the subjects available. Moreover, the voluntary sample is not representative of the entire population of the law enforcement and therefore it is not possible to generalize the results. the results obtained could provide important indications for future studies aimed to know the effects of physical training with a multilateral approach on the occupational stress management | due to a small-sample size, the generalizability of the results is quite limited. Using a between-subjects design represented a further limitation. a within-subjects design was preferred as in previous studies it was shown that nature-based interventions can have long lasting effects on physiological parameters | the reliance on self-reports. because of the particular characteristics of the sample, caution should be exercised in generalizing these findings to workforces that are less educated and affluent | A limitation of our study was omission of wait list control group as the impact of the MBI-ld may have achieved significance in comparison, indicating the. potential impact of such a workplace intervention. | the interventions were tested with staff at an inner-city university who may have had higher levels of education than do workers in other industries. Thus, the generalizability of the findings to workers in other settings requires further testing. |
| Study Number | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|
| Data Set Decision | SECONDARY DATASET | SECONDARY DATASET | SECONDARY DATASET | SECONDARY DATASET | SECONDARY DATASET |
| Study Information | |||||
| Database Number | WoS62 | P144 | O1594 | O1575 | O1130 |
| Author(s) | Machteld Hoeve, Esther L. de Bruin, Floor van Rooij and Susan Bögels | Erin Largo-Wight, Peter S. Wlyudka, Julie W. Merten & Elizabeth A. Cuvelier | Birgitta Ojala, Clas-Håkan Nygård, Heini Huhtala, Philip Bohle and Seppo T. Nikkari | Heribert Limm, Harald Gündel, Mechthild Heinmüller, Birgitt Marten-Mittag, Urs M Nater, Johannes Siegrist, Peter Angerer | Kimberly A. Aikens, John Astin, Kenneth R. Pelletier, Kristin Levanovich, Catherine M. Baase, Yeo Yung Park, and Catherine M. Bodnar |
| Year | 2021 | 2017 | 2019 | 2011 | 2014 |
| Link to Article | https://link.springer.com/content/pdf/10.1007/s12671-021-01631-7.pdf | https://www.tandfonline.com/doi/pdf/10.1080/15555240.2017.1335211?needAccess=true | https://www.mdpi.com/1660-4601/16/1/80 | https://oem.bmj.com/content/68/2/126?casa_token=4CAKgnx0r2wAAAAA%3Acw336eYaWoATNiEpIkpbAJuA7PAdti_Std6nW0lXmrjtAAudRItJdD0TEBaY6Rw8eeCpwbmjVvTs | http://affinityhealthhub.co.uk/d/attachments/mindfulness-goes-to-work-impact-of-an-online-intervention-1498490157.pdf |
| Access Date | 8-June-2022 | 8-June-2022 | 8-June-2022 | 8-June-2022 | 8-June-2022 |
| Title of Article | Effects of a Mindfulness-Based Intervention for Police Officers | Effectiveness and feasibility of a 10-minute employee stress intervention: Outdoor Booster Break | A Cognitive Behavioural Intervention Programme to Improve Psychological Well-Being | Stress management interventions in the workplace improve stress reactivity: a randomised controlled trial. | Mindfulness goes to work: impact of an online workplace intervention. |
| Country | Netherlands | United States | Finland | Germany | Michigan, United States |
| Intervention | |||||
| Study Aim | to increase knowledge on the effects of a mindfulnessbased intervention in police officers and potential mechanisms of change by relating changes in facets of mindful awareness to changes in stress | to explore the feasibility and efficacy of a brief work break outside (Outdoor Booster Break) among office employees. | to evaluate a cognitive behavioural intervention as an early rehabilitation strategy to improve employees’ well-being | to test the long-term effect of this SMI on acute perceived reactions to stress at work (stress reactivity) after 1 year, as the primary endpoint | to determine whether a mindfulness program, created for the workplace, was both practical and efficacious in decreasing employee stress while enhancing resiliency and well-being. |
| Type of Intervention | Mindfulness-based Intervention | Outdoor Booster Break environmental intervention | Cognitive Behavioural Intervention Programme | stress management intervention | online mindfulness workplace intervention |
| Duration of Intervention | 6 Weeks | 4 weeks | 9 months | 8 months | 7 week |
| Location of Intervention | Police offices | University office | Not Specified—facilitated by an interdisciplinary, goal-oriented multi professional team (a doctor, an occupational physiotherapist, an occupational psychologist, and a nurse) | at worksite | Online (at work) |
| Study Design | Quasi Experimental Study Design | Randomised Controlled Trial | Non Randomised Controlled Trial | randomized controlled trial | randomized controlled study |
| Methods | |||||
| How were participants recruited? | Participants were recruited by the Dutch trade union. Before the training, during a company away day, members of the trade union had the opportunity to participate in a mindfulness 2-hour workshop, led by SB and one of the mindfulness trainers, in order to inform them about the possibility of participating in a mindfulness training. | A census of university office staff in the southeast in springtime was invited to participate | Participants were volunteers who met the inclusion criteria for the study: Being employed in the public sector and working as permanent or long-term temporary staff with at least one year of service. | All lower and middle level managers (n¼262), each responsible for a specific unit within production and for the management of 50 workers, on average, were eligible. All participants were invited to a 1.5 h medical and psychological examination by an experienced team consisting of a psychologist (HL) and a physician (MH). Written informed consent was obtained. All volunteers were required to complete a battery of questionnaires, participate in a basic physical examination with blood sampling and collect saliva samples the next working day. This initial health check included feedback to each participant a few days later. | Participants were drawn from a sample of 600 Dow employees, located in Midland, Michigan, who had completed a health risk assessment (comprehensive questionnaire and biometrics) in the preceding 6 months. All employees are invited for health risk assessment with employees in given departments being scheduled throughout the year. This recruitment allowed for study access to a good cross section of employees because the standard process of invitations would include all elements of the employee base. Study participant recruitment occurred from March to April 2012 and consisted of one e-mail notification, which described the free mindfulness-based stress management program. The e-mail notification explained that the purpose of the program was to help employees reduce and manage workplace stress. |
| Occupation of Participants | Police Officers | University office staff | Public sector workers | lower and middle level managers at an international manufacturing plant located in Southern Germany | General employees at a chemical company |
| Specific Focus on Older Workers? | No | No | No | No | No |
| Outcome Measurement | Symptoms of stress were measured by four instruments that measure different types of stress, including general feelings of stress and tension, physical stress, occupational stress during police work, and stress symptoms that are related to a traumatic event (i.e., PTSD symptoms). | Perceived stress was measured two times–at pretest and posttest for both conditions with a self-report perceived stress instrument. The Perceived Stress Questionnaire (PSQ) | The measurement tools used in this study were the Bergen Burnout Inventory (BBI) and the Utrecht Work Engagement Scale (UWES).BBI 15 was used to measure burnout. It includes three sub-dimensions: Exhaustion (five items), cynicism (five items), and sense of inadequacy (five items). UWES 9 was used to define three dimensions of work engagement: Vigour (three items), dedication (three items), and absorption (three items) | Self-reported stress reactivity was measured with the 29-item Stress Reactivity Scale (SRS). Biological stress indices were measured using levels of salivary cortisol as an indicator of hypothalamic-pituitary-adrenal axis activity, and salivary a-amylase, reflecting basal activity of the sympathetic nervous system | The Perceived Stress Scale (PSS-14) was used to assess participants’ levels of psychological stress. The PSS-14 is a well-validated stress measurement tool whose items are designed to tap into how unpredictable, uncontrollable, and overloaded individuals find their lives |
| Data Collection Style | Self report questionnaires | self-reported perceived stress 4-point Likerttype scale from participants | self reported questionnarie | self reported questionnaire and saliva samples | self reported questionnaire |
| How were the Results analysed? | Pre and Post Intervention, plus Follow Up | Comparison to control group, and pre and post intervention | Comparison to Control, and Pre and Post Intervention | Comparison to Control, and Pre and Post Intervention | Comparison to Control, and Pre and Post Intervention |
| Results | |||||
| No. of Participants | 82 | 37 (Treatment had Outdoor Break, Control had Indoor Break) | 779 | 174 | 89 |
| Dropout Rate | 19 dropouts | No Dropout Mentioned | 217 dropouts | 20 dropouts/lost to follow up | 23 dropouts/failed to follow up |
| Age of Workers | 30–63 (mean = 49) | Average age of 48.8 | mean age of subjects was 49.9 years (range 21–64 years) | Mean age = 40.9. Aged 18–65 years with more than 2 years left before retirement | 18-65 |
| Any other condition of workers? | No | No | No | No | No |
| Change in Stress Levels | Improvement in mindful awareness (mindfulness total scale) was marginally significantly associated with a reduction in general feelings of stress and tension. Further, an increase in attention was significantly associated with reductions in general stress and occupational stress. | Observed average posttest stress scores were lower for both the control group and the treatment group (Mean PSQ Stress, Control Pre = 66.25, Control Post 64.25, Treatment Group Pre 65.25, Treatment Group Post 61.25). Posttest stress was 4.22 points lower (95% CI: or the treatment group compared to controls | Total BBI 15 values for the intervention group were 36.9 (standard deviation (SD) 11.8) at baseline and 33.9 (SD 12.3) at follow-up. The change from baseline was −3.0 (p < 0.001). Values for the control group were 37.6 (SD 12.2) at baseline and 37.5 (SD 14.4) at follow-up. The change from baseline was 0.1 (p = 0.912). The difference in changes between groups was statistically significant (p = 0.023). | The reduction in perceived stress reactivity in the intervention group (from 54.5 to 50.2) was significantly higher than in the control group (from 54.5 to 52.7). For cortisol, no effect of the intervention was observed. Self-perceived stress reactivity assesses typical cognitive, emotional and physiological reactions to different stressful situations. High stress reactivity scores have been shown to significantly correlate with a variety of other psychological measures of distress such as depression or anxiety. | perceived stress declined by 23.1% from baseline values in the follow up 6 months. Participants also reported a decline in weekly high stress episodes by 33%, which is a significant downward trend (p < 0.001). |
| Intervention deemed effective/successful | Police officers significantly benefited from the mindfulnessbased intervention | taking a work break in general resulted in a reduction of stress among the employees. All employees benefited from a reduction of generalized stress after 4 weeks of daily work breaks. But, as expected, the participants randomized into the Outdoor Booster Breaks resulted in significantly greater reduction in stress over the 4-week study than the participants who took a standard indoor work break. | The principal finding of this study is a statistically significant improvement in several measures of psychosocial well-being (BBI 15, UWES, stress, depression) for participants who completed the cognitive behavioural intervention programme. | Our approach proved to be feasible in the workplace setting, it was well accepted and it produced selected favourable behavioural and physiological effects | The present findings have significant potential implications for corporate health and human performance. The program studied was a mindfulness intervention, which was modified in length, content, and messaging to fit workplace needs and delivered through an on-line platform that included personal coaching. Overall, the ESs obtained in this study were in the moderate to large range and were either maintained, or further improved, over time. This indicates that a shortened, Web-based mindfulness program can replicate the results of traditionally delivered MBSR. |
| Key Conclusions | Mindfulness-based intervention appears beneficial for police officers. Further, increases in both attention and acceptance skills such as acting with awareness and non-judging seem to be most important in explaining reductions of stress in police officers. | This study points to several implications for employers and worksite health promoters. First, environmental stress interventions such as Outdoor Booster Breaks are relatively simple to implement. Creating healthy workplaces is a health promotion effort that may be more practical and feasible than many other labor-intensive health promotion efforts. Creating a healthful work environment—with the purposeful use of nature contact—is a simple and practical step to improve employee health and productivity. Environmental improvements require little, if any, commitment and effort from the employee. In a way, improving the workplace environment to foster health among employees is one way to “set the employees up for success.” | This study suggests that a cognitive behavioural intervention achieved significant improvements in several measures of mental health. The results imply that this kind of intervention is needed to give early support on mental health issues for the working-age population. | SMI based on work stress theory, is effective in reducing perceived stress reactivity and sympathetic activation in lower and middle management employees. Other mental health parameters and ERI show a tendency towards improvement. These beneficial effects are present 1 year later. | This on-line mindfulness intervention seems to be both practical and effective in decreasing employee stress, while improving resiliency, vigor, and work engagement, thereby enhancing overall employee well-being. |
| Discussion | |||||
| Author Identified Weaknesses | we examined the effectiveness of an adapted corporate mindfulness training. Although adaptations to the work situation of police officers were made, such as in the enquiries and discussion after the meditations and the examples being used in exercises, no cultural adaptations were made to the content of the training, which could have diminished the positive effects. Second, findings might not be generalizable to the entire population of police officers. Although our sample size is larger than most earlier studies on the effects of mindfulness-based intervention in police officers, the number of participants was small due to attrition at post-test and follow-up. senior workers are generally overrepresented in unions in the Netherlands. Therefore, it should be kept in mind that the results may apply only to more experienced police officers and less to relatively young or inexperienced officers. | the sample size and group sizes were small. the generalizability of the findings to male workers. Future researchers should assess the impact of Outdoor Booster Breaks with greater male representation. Also perceived stress was the only outcome measured. | One limitation is that the participants represent a relatively small population in Finland. The intervention and control groups were selected partly according to the participants’ own interests. Question-based research may suffer from bias if the participants feel satisfied with the service and therefore respond positively when they answer the second time. | the effects were only moderate and health effects still have to be demonstrated in longer follow-up studies. This also points to the fact that improving working conditions must remain a primary goal of stress prevention even though this is sometimes hard to attain in practice | this study had results from a relatively small number of participants (n = 79), creating the need for a larger randomized control trial to confirm the results. In addition, 12-month follow-up was not completed to avoid overburdening busy employees. This study limitation precludes us from making a more definitive assessment regarding the long-term effectiveness of the mindfulness intervention |
References
- Roberts, I. Taking age out of the workplace: Putting older workers back in? Work. Employ. Soc. 2006, 20, 67–86. [Google Scholar] [CrossRef]
- Keese, M. Live Longer, Work Longer: A Synthesis Report; OECD Publishing: Paris, France, 2006. [Google Scholar]
- Poscia, A.; Moscato, U.; La Milia, D.; Milovanovic, S.; Stojanovic, J.; Borghini, A.; Collamati, A.; Ricciardi, W.; Magnavita, N. Workplace health promotion for older workers: A systematic review. BMC Health Serv. Res. 2016, 16, 415–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Possible Public Health Implications of Raising the State Pension Age and how to Mitigate Them—Mitigating Increases in the State Pension Age (MISPA). Available online: https://www.ucl.ac.uk/epidemiology-health-care/sites/epidemiology-health-care/files/mispa_long_text_final_version.pdf (accessed on 13 July 2022).
- Bravo, G.; Viviani, C.; Lavallière, M.; Arezes, P.; Martinez, M.; Dianat, I.; Bragança, S.; Castellucci, H. Do older workers suffer more workplace injuries? A systematic review. Int. J. Occup. Saf. Ergnonomics 2020, 28, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Sickness Absence in the UK Labour Market—Office for National Statistics. Available online: https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/labourproductivity/articles/sicknessabsenceinthelabourmarket/2020/ (accessed on 3 June 2022).
- Work-Related Stress and How to Manage It: Overview—Health and Safety Executive. Available online: https://www.hse.gov.uk/stress/overview.htm (accessed on 3 June 2022).
- Health at Work—An Independent Review of Sickness Absence by Dame Carol Black and David Frost CBE. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/181060/health-at-work.pdf (accessed on 3 June 2022).
- Jones, M.; Latreille, P.; Sloane, P.; Staneva, A. Work-related health risks in Europe: Are older workers more vulnerable? Soc. Sci. Med. 2013, 88, 18–29. [Google Scholar] [CrossRef]
- Blackham, A. Extending Working Life for Older Workers: Age Discrimination Law, Policy and Practice; Hart Publishing: Oxford, UK, 2016. [Google Scholar]
- Pieper, C.; Schröer, S.; Eilerts, A. Evidence of Workplace Interventions—A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2019, 16, 3553. [Google Scholar] [CrossRef] [Green Version]
- Page, M.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 1–9. [Google Scholar]
- Sayers, A. Tips and tricks in performing a systematic review. Br. J. Gen. Pract. 2008, 58, 136. [Google Scholar] [CrossRef]
- List of OECD Member Countries—Ratification of the Convention on the OECD—OECD. Available online: https://www.oecd.org/about/document/ratification-oecd-convention.htm (accessed on 3 June 2022).
- Current Retirement Ages—OECD. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/pensions-at-a-glance-2017/current-retirement-ages_pension_glance-2017-9-en;jsessionid=Dka7fyISbXMfYrchrezDCdWH.ip-10-240-5-16 (accessed on 3 June 2022).
- Higgins, J.; Sterne, J.; Savović, J.; Page, M.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10 (Suppl. S1), 29–31. [Google Scholar]
- Hughes, S.; Seymour, R.; Campbell, R.; Shaw, J.; Fabiyi, C.; Sokas, R. Comparison of Two Health-Promotion Programes for Older Workers. Am. J. Public Health 2011, 101, 883–890. [Google Scholar] [CrossRef]
- Malarkey, W.; Jarjoura, D.; Klatt, M. Workplace based mindfulness practice and inflammation: A randomized trial. Brain Behav. Immun. 2013, 27, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Aikens, K.; Astin, J.; Pelletier, K.; Levanovich, K.; Baase, C.; Park, Y.; Bodnar, C. Mindfulness Goes to Work: Impact of an Online Workplace Intervention. J. Occup. Environ. Med. 2014, 56, 721–731. [Google Scholar] [CrossRef] [Green Version]
- Cook, R.; Hersch, R.; Schlossberg, D.; Leaf, S. A Web-Based Health Promotion Program for Older Workers: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e3399. [Google Scholar] [CrossRef]
- Largo-Wight, E.; Wlyudka, P.; Merten, J.; Cuvelier, E. Effectiveness and feasibility of a 10-minute employee stress intervention: Outdoor Booster Break. J. Workplace Behav. Health 2017, 32, 159–171. [Google Scholar] [CrossRef]
- Limm, H.; Gundel, H.; Heinmuller, M.; Marten-Mittag, B.; Nater, U.; Siegrist, J.; Angerer, P. Stress management interventions in the workplace improve stress reactivity: A randomised controlled trial. Occup. Environ. Med. 2011, 68, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Hoeve, M.; de Bruin, E.; van Rooij, F.; Bögels, S. Effects of a Mindfulness-Based Intervention for Police Officers. Mindfulness 2021, 12, 1672–1684. [Google Scholar] [CrossRef]
- Ojala, B.; Nygård, C.; Huhtala, H.; Bohle, P.; Nikkari, S. A Cognitive Behavioural Intervention Programme to Improve Psychological Well-Being. Int. J. Environ. Res. Public Health 2019, 16, 80. [Google Scholar] [CrossRef] [Green Version]
- Fischetti, F.; Cataldi, S.; Latino, F.; Greco, G. Effectiveness of multilateral training didactic method on physical and mental wellbeing in law enforcement. In Proceedings of the Spring Conferences of Sports Science. Costa Blanca Sports Science Events, Alicante, Spain, 14–15 June 2019. [Google Scholar]
- Calogiuri, G.; Evensen, K.; Weydahl, A.; Andersson, K.; Patil, G.; Ihlebæk, C.; Raanaas, R. Green exercise as a workplace intervention to reduce job stress. Results from a pilot study. Work 2016, 53, 99–111. [Google Scholar] [CrossRef] [Green Version]
- Polit, D.; Beck, C. Generalization in quantitative and qualitative research: Myths and strategies. Int. J. Nurs. Stud. 2010, 47, 1451–1458. [Google Scholar] [CrossRef] [Green Version]
- Steenstra, I.; Cullen, K.; Irvin, E.; Van Eerd, D.; Alavinia, M.; Beaton, D.; Geary, J.; Gignac, M.; Gross, D.; Mahood, Q.; et al. A systematic review of interventions to promote work participation in older workers. J. Saf. Res. 2017, 60, 93–102. [Google Scholar] [CrossRef]
- Kingston, A.; Jagger, C. Review of methodologies of cohort studies of older people. Age Ageing 2017, 47, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Crawford, J.; Graveling, R.; Cowie, H.; Dixon, K. The health safety and health promotion needs of older workers. Occup. Med. 2010, 60, 184–192. [Google Scholar] [CrossRef] [Green Version]
- McDonald, J. Measuring Personality Constructs: The Advantages and Disadvantages of Self Reports, Informant Reports and Behavioural Assessments. Enquire 2008, 1, 75–94. [Google Scholar]
- Griffiths, A. Designing and Managing Healthy Work for Older Workers. Occup. Med. 2000, 50, 473–477. [Google Scholar] [CrossRef] [Green Version]
- Tetrick, L.; Winslow, C. Workplace Stress Manager Interventions and Health Promotion. Annu. Rev. Organ. Psychol. Organ. Behav. 2015, 2, 583–603. [Google Scholar] [CrossRef] [Green Version]
- McDaid, D.; Park, A. Investing in mental health and well-being: Findings from the DataPrev project. Health Promot. Int. 2011, 26, 108–139. [Google Scholar] [CrossRef] [Green Version]
| PICO Term | Detail |
|---|---|
| Population | Older workers, in the Organisation for Economic Co-Operation and Development (OECD) country, in non-health sector jobs. |
| Intervention | All interventions occurring in the workplace, including medication, educational and exercise interventions. |
| Control | Comparison with control conditions as described in each of the papers in the review |
| Outcome | Reduced workplace stress |
| Database | Programmes Search Terms | Setting Search Terms | Outcome Search Terms | Papers per Database |
|---|---|---|---|---|
| OvidMedline | Intervention.mp. OR Psychosocial Intervention/ | Workplace/ OR Workplace.mp. | Burnout, Professional/OR | 2444 |
| Occupational Stress.mp. OR | ||||
| Stress, Psychological/OR Occupational Stress/OR Occupational Diseases | ||||
| Scopus | Intervention OR Programme OR Program | Workplace OR Office OR “Work Centre” | “Occupational Stress” OR “Professional Burnout” OR “Psychological Stress” | 701 |
| Web of Science | Intervention OR Programmes OR Program | Workplace * OR Office * OR “Work Centre” | “Occupational Stress” OR “Professional Burnout” OR “Workplace Stress” OR “Job Stress” OR “Psychological Stress” | 964 |
| PsycInfo | Exp Workplace Intervention/OR Intervention.mp. OR exp intervention | Exp Workplace Intervention/OR Workplace.mp. | Occupational Stress.mp. OR exp Occupational Stress/ | 469 |
| Total Papers | 3708 Papers | |||
| Order | Criteria | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|
| 1 | Language | Paper not published in English | |
| 2 | Date of Publication | Published between 1 January 2011–31 July 2021 | |
| 3 | Access to Publication | Full Paper Access via UCL/Online | Paper not fully available online |
| 4 | Type of Paper | Papers without an Abstract | |
| 5 | Publication Type | Original Studies Peer Reviewed Studies | Systematic Reviews Editorials Dissertations Not Fully Published Papers |
| 6 | Setting | Conducted in the UK or an OECD Country Reporting an intervention that was conducted in a workplace | Reporting interventions in health sector workplaces (e.g., a hospital) |
| 7 | Outcome Measured | Quantitative data on workplace stress or anxiety (burnout, perceived stress, measures of cortisol levels, etc.) | Change in outcome level not reported |
| 8 | Population Group | Reporting an intervention which provides data on its effects on older workers in the workforce | Data reported with no desegregation by workers age or no evidence that included workers would be considered as “older” |
| 9 | Study Design | Experimental Designs Randomised Controlled Trials Non-Randomised Trials Before and After Studies | Qualitative papers (i.e., interview, focus group or ethnographic studies reporting experience of impressions) |
| 10 | Study Aim | Where at least one of the objectives of the intervention or programme is to reduce workplace stress |
| Study (Author, Year) | Domain 1 (Randomisation Process) | Domain 2 (Deviations from intended Interventions) | Domain 3 (Missing Outcome Data) | Domain 4 (Measurement of Outcome) | Domain 5 (Selection of the Reported Results) | Domain 6 (Overall Bias) |
|---|---|---|---|---|---|---|
| Hughes, 2011 [17] | 2 | 1 | 2 | 2 | 1 | 2 |
| Malarkey, 2013 [18] | 2 | 1 | 1 | 1 | 1 | 1 |
| Aikens, 2014 [19] | 2 | 2 | 1 | 1 | 1 | 1 |
| Cook, 2015 [20] | 2 | 1 | 2 | 2 | 1 | 2 |
| Largo-Wight, 2017 [21] | 2 | 1 | 1 | 2 | 2 | 2 |
| Limm, 2011 [22] | 2 | 1 | 1 | 2 | 1 | 1 |
| Hoeve, 2021 [23] | 1 | 1 | 1 | 1 | 1 | 1 |
| Ojala, 2019 [24] | 2 | 1 | 2 | 2 | 2 | 2 |
| Fischetti, 2019 [25] | 2 | 1 | 1 | 3 | 2 | 2 |
| Calogiuri, 2016 [26] | 2 | 1 | 2 | 2 | 2 | 2 |
| Study (Author, Year) | Intervention Type | Duration | Location | Outcome Measurement Method | Data Collection Type | Findings | Intervention Deemed Effective? 1 |
|---|---|---|---|---|---|---|---|
| Low risk of bias | |||||||
| Malarkey, 2013 [18] | Psychological | 8 Weeks | Office | Perceived Stress Scale Questionnaire | Self-report | No significant differences were seen at follow-up | No |
| Cortisol Levels | Blood test & Saliva sample | No significant changes were noted | |||||
| Aikens, 2014 [19] | Psychological | 7 Weeks | Online | Perceived Stress Scale Questionnaire | Self-report | 23.1% decline in perceived stress | Yes |
| Limm, 2011 [22] | Psychological | 8 Months | Office | Stress Reactivity Scale (SRS) | Self-report | The reduction in SR in intervention group (from 54.5 to 50.2) was significantly higher than in the control group (from 54.5 to 52.7) | Mixed |
| Salivary Cortisol Levels | Saliva samples | No effect observed | |||||
| Hoeve, 2021 [23] | Psychological | 6 Weeks | Office | Depression, anxiety, and stress scale (DASS) | Self-report | General stress score decreased from a group mean of 1.05 to 0.58 | Yes |
| Police Stress Questionnaire (PSQ-Op) | Self-report | Occupational Stress scores decreased from a group of 3.17 to 2.84 | |||||
| Some bias concerns | |||||||
| Hughes, 2011 [17] | Educational & Psychological | 12 Months | Office | Perceived Stress Scale Questionnaire | Self-report | No quantitative data reported 2 | No |
| Cook, 2015 [20] | Physical & Psychological | 3 Months | Online | Symptoms of Distress Likert scale questionnaire | Self-report | No difference between groups | No |
| Coping with Stress questionnaire | Self-report | No differences between groups on coping with stress | |||||
| Largo-Wight, 2017 [21] | Psychological | 4 Weeks | Outside | Perceived Stress Scale Questionnaire | Self-report | Mean PSSQ score decreased from 62.3 to 61.2 in intervention group, compared to 66.2 to 64.2 decrease from control group | Yes |
| Ojala, 2019 [24] | Psychological | 9 Months | Implied to be in Office | Bergen Burnout Inventory (BBI) | Self-report | Total BBI decreased from 36.9 to 33.9 in intervention group, at follow up | Yes |
| Utrecht Work Engagement Scale (UWES) | Self-report | UWES increased from 4.3 to 4.5 in intervention group, at follow-up | |||||
| Fischetti, 2019 [25] | Physical & Education | 8 Weeks | Office | Occupational Stress Indicator | Self-report | Scores for Job as a source of stress decreased from 30.7 to 25.2 | Yes |
| Short-Form 12 Questionnaire | Self-report | Increases in scores with significant changes from pre- to post-intervention (48.2 to 53.4) | |||||
| Calogiuri, 2016 [26] | Physical | 2 Weeks | Outside | Physical Activity Affective Scale Questionnaire | Self-report | Higher ratings for PAAS, in relation to Positive Affect in the intervention group | Mixed |
| Cortisol Awakening Response (CAR) | Blood Test | No significant differences between groups | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subel, D.; Blane, D.; Sheringham, J. Workplace Interventions to Reduce Occupational Stress for Older Workers: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 9202. https://doi.org/10.3390/ijerph19159202
Subel D, Blane D, Sheringham J. Workplace Interventions to Reduce Occupational Stress for Older Workers: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9202. https://doi.org/10.3390/ijerph19159202
Chicago/Turabian StyleSubel, Daniel, David Blane, and Jessica Sheringham. 2022. "Workplace Interventions to Reduce Occupational Stress for Older Workers: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 15: 9202. https://doi.org/10.3390/ijerph19159202
APA StyleSubel, D., Blane, D., & Sheringham, J. (2022). Workplace Interventions to Reduce Occupational Stress for Older Workers: A Systematic Review. International Journal of Environmental Research and Public Health, 19(15), 9202. https://doi.org/10.3390/ijerph19159202