
Inequity in Access and Delivery of Virtual Care Interventions: A Scoping Review

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
- Published in English
- Published between January 2010 and January 2021
- Studies exploring equity in ambulatory services offered virtually
- Carried out in OECD countries
- Empirical studies
- Published in language other than English
- Published before January 2010
- Studies not exploring equity in ambulatory services offered virtually
- Studies exploring robotic/tele-surgery
- Studies carried outside OECD countries
- Commentary/review/opinion pieces
2.3. Data Extraction
2.4. Data Mapping
3. Results
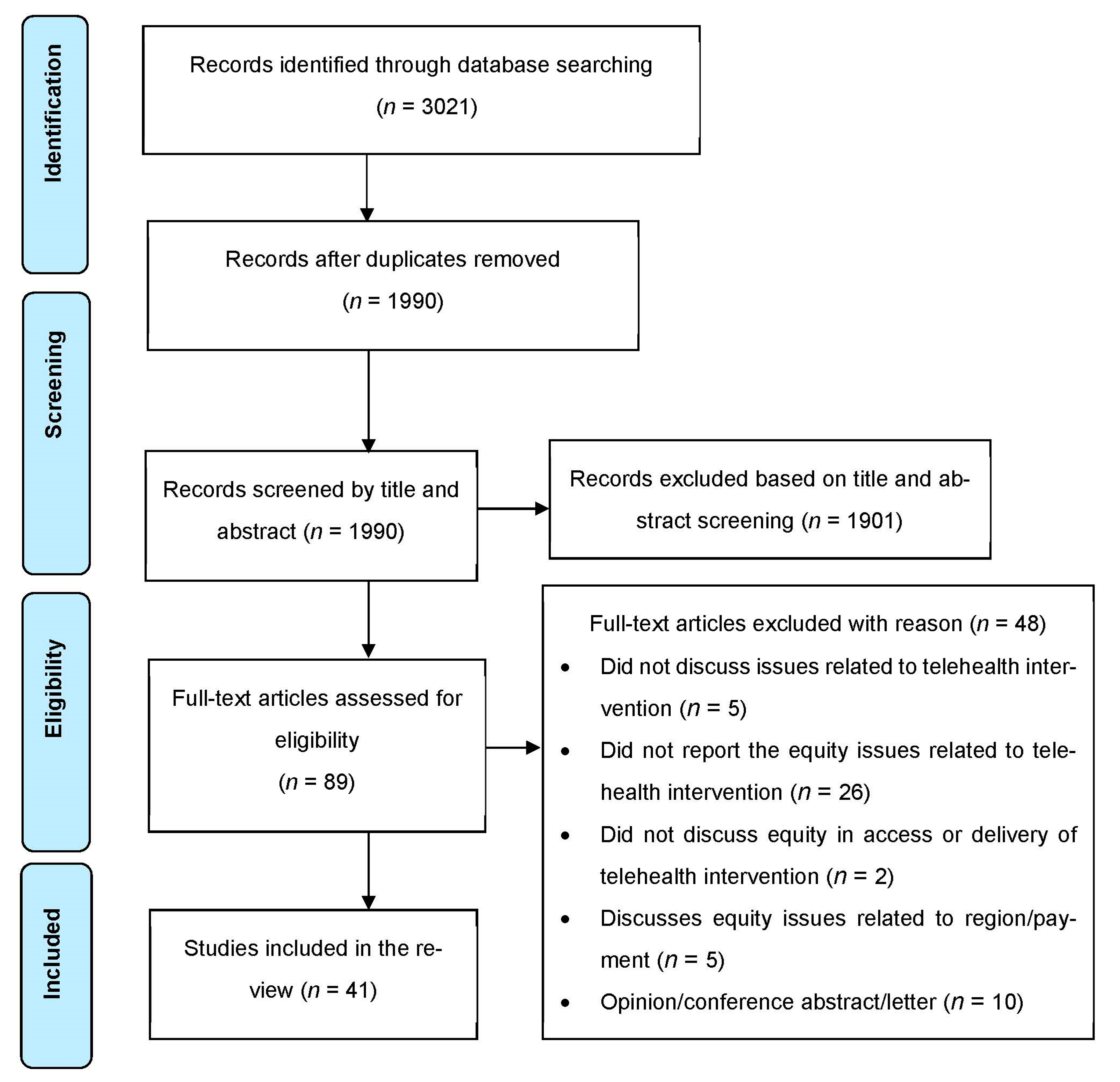
3.1. Search Results
3.2. Study Settings
3.3. Study Designs
3.4. Type of Participants
3.5. Virtual Care Modalities
3.6. Types of Inequity Issues Identified/Addressed
3.6.1. Cultural and Ethnic Inequities
3.6.2. Sociodemographic and Socio-Economic Inequities
3.6.3. Inequity Issues Related to Digital/eHealth Literacy
3.6.4. Technological Inequities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Whitehead, M.; Dahlgren, G. Policies and Strategies to Promote Social Equity in Health; Institute for Future Studies: Stockholm, Sweden, 1991. [Google Scholar]
- Braveman, P.; Gruskin, S. Defining equity in health. J. Epidemiol. Community Health 2003, 57, 254–258. [Google Scholar] [CrossRef]
- Braveman, P. What are health disparities and health equity? We need to be clear. Public Health Rep. 2014, 129 (Suppl. S2), 5–8. [Google Scholar] [CrossRef] [PubMed]
- Baciu, A.; Negussie, Y.; Geller, A.; Weinstein, J.N.; National Academies of Sciences Engineering and Medicine. The root causes of health inequity. In Communities in Action: Pathways to Health Equity; National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Marrie, R.A.; Leung, S.; Tyry, T.; Cutter, G.R.; Fox, R.; Salter, A. Use of eHealth and mHealth technology by persons with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 27, 13–19. [Google Scholar] [CrossRef]
- Levesque, J.-F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Inequities and Their Causes. 2018. Available online: https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes (accessed on 18 May 2022).
- The Lancet. Taking urgent action on health inequities. Lancet 2020, 395, 659. [Google Scholar] [CrossRef]
- Friel, S.; Marmot, M.G. Action on the social determinants of health and health inequities goes global. Annu. Rev. Public Health 2011, 32, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; You, J.; Wright, J.; Guthridge, S.L.; Lee, A.H. Health inequity in the northern territory, Australia. Int. J. Equity Health 2013, 12, 79. [Google Scholar] [CrossRef] [PubMed]
- Flavel, J.; McKee, M.; Freeman, T.; Musolino, C.; van Eyk, H.; Tesfay, F.H.; Baum, F. The need for improved Australian data on social determinants of health inequities. Med. J. Aust. 2022, 216, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Subirats, I.; Vargas, I.; Mogollón-Pérez, A.S.; De Paepe, P.; Da Silva, M.R.F.; Unger, J.P.; Borrell, C.; Vázquez, M.L. Inequities in access to health care in different health systems: A study in municipalities of central Colombia and north-eastern Brazil. Int. J. Equity Health 2014, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Woodward, A.; Kawachi, I. Why reduce health inequalities? J. Epidemiol. Community Health 2000, 54, 923–929. [Google Scholar] [CrossRef]
- Agency for Clinical Innovation. Virtual Care in Practice; Agency for Clinical Innovation: St. Leonards, NSW, Australia, 2021.
- Khairat, S.; Haithcoat, T.; Liu, S.; Zaman, T.; Edson, B.; Gianforcaro, R.; Shyu, C.R. Advancing health equity and access using telemedicine: A geospatial assessment. J. Am. Med. Inform. Assoc. 2019, 26, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, W.; Zhou, K.; Waddell, E.; Myers, T.; Dorsey, E.R. Improving Access to Care: Telemedicine Across Medical Domains. Annu. Rev. Public Health 2021, 42, 463–481. [Google Scholar] [CrossRef]
- Katzow, M.W.; Steinway, C.; Jan, S. Telemedicine and health disparities during COVID-19. Pediatrics 2020, 146, e20201586. [Google Scholar] [CrossRef] [PubMed]
- Velasquez, D.; Mehrotra, A. Ensuring the growth of telehealth during COVID-19 does not exacerbate disparities in care. Health Aff. Blog 2020, 10, 1–306. [Google Scholar] [CrossRef]
- Harris-Roxas, B. The Impact and Effectiveness of Equity Focused Health Impact Assessment in Health Service Planning. Ph.D. Thesis, University of New South Wales, Sydney, Australia, 2014. [Google Scholar]
- Chauhan, V.; Galwankar, S.; Arquilla, B.; Garg, M.; Di Somma, S.; El-Menyar, A.; Krishnan, V.; Gerber, J.; Holland, R.; Stawicki, S.P. Novel coronavirus (COVID-19): Leveraging telemedicine to optimize care while minimizing exposures and viral transmission. J. Emergencies Trauma Shock. 2020, 13, 20. [Google Scholar]
- Hollander, J.E.; Carr, B.G. Virtually perfect? Telemedicine for COVID-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef] [PubMed]
- Denadai, R. COVID-19 pandemic as a driver for spreading virtual care globally: The future starts now. Clinics 2020, 75, e1967. [Google Scholar] [CrossRef] [PubMed]
- López, L.; Green, A.R.; Tan-McGrory, A.; King, R.S.; Betancourt, J.R. Bridging the digital divide in health care: The role of health information technology in addressing racial and ethnic disparities. Jt. Comm. J. Qual. Patient Saf. 2011, 37, 437–445. [Google Scholar] [CrossRef]
- Wong, B.L.H.; Maaß, L.; Vodden, A.; van Kessel, R.; Sorbello, S.; Buttigieg, S.; Odone, A.; Section, D.H.; European Public Health Association. The dawn of digital public health in Europe: Implications for public health policy and practice. Lancet Reg. Health-Eur. 2022, 14, 100316. [Google Scholar] [CrossRef] [PubMed]
- Fisk, M.; Livingstone, A.; Pit, S.W. Telehealth in the context of COVID-19: Changing perspectives in Australia, the United Kingdom, and the United States. J. Med. Internet Res. 2020, 22, e19264. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, O.R.; Dearing, C.; Jagers, D.; Shaw, M.J.; Raffan, F.; Jones, A.; Taggart, R.; Sinclair, T.; Anderson, T.; Ritchie, A.G. Virtual health care for community management of patients with COVID-19 in Australia: Observational cohort study. J. Med. Internet Res. 2021, 23, e21064. [Google Scholar] [CrossRef] [PubMed]
- Legler, S.; Diehl, M.; Hilliard, B.; Olson, A.; Markowitz, R.; Tignanelli, C.; Melton, G.B.; Broccard, A.; Kirsch, J.; Usher, M. Evaluation of an intrahospital telemedicine program for patients admitted with COVID-19: Mixed methods study. J. Med. Internet Res. 2021, 23, e25987. [Google Scholar] [CrossRef] [PubMed]
- Raffan, F.; Anderson, T.; Sinclair, T.; Shaw, M.; Amanatidis, S.; Thapa, R.; Nilsson, S.J.; Jagers, D.; Wilson, A.; Haigh, F. The Virtual Care Experience of Patients Diagnosed With COVID-19. J. Patient Exp. 2021, 8, 23743735211008310. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Pollock, D.; Davies, E.L.; Peters, M.D.; Tricco, A.C.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H.; Munn, Z. Undertaking a scoping review: A practical guide for nursing and midwifery students, clinicians, researchers, and academics. J. Adv. Nurs. 2021, 77, 2102–2113. [Google Scholar] [CrossRef]
- Alam, K.; Mahumud, R.A.; Alam, F.; Keramat, S.A.; Erdiaw-Kwasie, M.O.; Sarker, A.R. Determinants of access to eHealth services in regional Australia. Int. J. Med. Inform. 2019, 131, 103960. [Google Scholar] [CrossRef]
- Foley, K.; Freeman, T.; Ward, P.; Lawler, A.; Osborne, R.; Fisher, M. Exploring access to, use of and benefits from population-oriented digital health services in Australia. Health Promot. Int. 2020, 26, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.; Butow, P.; Sze, M.; Young, J.; Goldstein, D. Reducing disparity in outcomes for immigrants with cancer: A qualitative assessment of the feasibility and acceptability of a culturally targeted telephone-based supportive care intervention. Supportive Care Cancer 2013, 21, 2297–2301. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Arora, S.; Kurji, A.K.; Tennant, M.T. Dismantling sociocultural barriers to eye care with tele-ophthalmology: Lessons from an Alberta Cree community. Clin. Investig. Med. Med. Clin. Exp. 2013, 36, E57–E63. [Google Scholar] [CrossRef] [PubMed]
- Mangin, D.; Parascandalo, J.; Khudoyarova, O.; Agarwal, G.; Bismah, V.; Orr, S. Multimorbidity, eHealth and implications for equity: A cross-sectional survey of patient perspectives on eHealth. BMJ Open 2019, 9, e023731. [Google Scholar] [CrossRef] [PubMed]
- Arighi, A.; Fumagalli, G.G.; Carandini, T.; Pietroboni, A.M.; De Riz, M.A.; Galimberti, D.; Scarpini, E. Facing the digital divide into a dementia clinic during COVID-19 pandemic: Caregiver age matters. Neurol. Sci. 2021, 42, 1247–1251. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Luo, Y.; Yu, X.; Wen, J.; Mason, E.; Li, W.; Jalali, M.S. Patients’ Perceptions of Barriers and Facilitators to the Adoption of E-Hospitals: Cross-Sectional Study in Western China. J. Med. Internet Res. 2020, 22, e17221. [Google Scholar] [CrossRef] [PubMed]
- Ernsting, C.; Stühmann, L.M.; Dombrowski, S.U.; Voigt-Antons, J.N.; Kuhlmey, A.; Gellert, P. Associations of Health App Use and Perceived Effectiveness in People with Cardiovascular Diseases and Diabetes: Population-Based Survey. JMIR Mhealth Uhealth 2019, 7, e12179. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.H.; Bradway, M.; Broz, J.; Claudi, T.; Henriksen, Ø.; Wangberg, S.C.; Årsand, E. Inequalities in the Use of eHealth Between Socioeconomic Groups Among Patients with Type 1 and Type 2 Diabetes: Cross-Sectional Study. J. Med. Internet Res. 2019, 21, e13615. [Google Scholar] [CrossRef]
- Leng, S.; MacDougall, M.; McKinstry, B. The acceptability to patients of video-consulting in general practice: Semi-structured interviews in three diverse general practices. J. Innov. Health Inform. 2016, 23, 141. [Google Scholar] [CrossRef]
- Campos-Castillo, C.; Anthony, D. Racial and ethnic differences in self-reported telehealth use during the COVID-19 pandemic: A secondary analysis of a US survey of internet users from late March. J. Am. Med. Inform. Assoc. 2021, 28, 119–125. [Google Scholar] [CrossRef]
- Gordon, N.P.; Hornbrook, M.C. Older adults’ readiness to engage with eHealth patient education and self-care resources: A cross-sectional survey. BMC Health Serv. Res. 2018, 18, 220. [Google Scholar] [CrossRef]
- Khoong, E.C.; Butler, B.A.; Mesina, O.; Su, G.; DeFries, T.B.; Nijagal, M.; Lyles, C.R. Patient interest in and barriers to telemedicine video visits in a multilingual urban safety-net system. J. Am. Med. Inform. Assoc. 2020, 28, 349–353. [Google Scholar] [CrossRef]
- Nelson, L.A.; Mulvaney, S.A.; Gebretsadik, T.; Ho, Y.X.; Johnson, K.B.; Osborn, C.Y. Disparities in the use of a mHealth medication adherence promotion intervention for low-income adults with type 2 diabetes. J. Am. Med. Inform. Assoc. 2016, 23, 12–18. [Google Scholar] [CrossRef]
- Pierce, R.P.; Stevermer, J.J. Disparities in use of telehealth at the onset of the COVID-19 public health emergency. J. Telemed. Telecare 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Potdar, R.; Thomas, A.; DiMeglio, M.; Mohiuddin, K.; Djibo, D.A.; Laudanski, K.; Dourado, C.M.; Leighton, J.C.; Ford, J.G. Access to internet, smartphone usage, and acceptability of mobile health technology among cancer patients. Supportive Care Cancer 2020, 28, 5455–5461. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.A.; Betancourt, J.R.; Sequist, T.D.; Ganguli, I. Differences in the use of telephone and video telemedicine visits during the COVID-19 pandemic. Am. J. Manag. Care 2021, 27, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Severe, J.; Tang, R.; Horbatch, F.; Onishchenko, R.; Naini, V.; Blazek, M.C. Factors Influencing Patients’ Initial Decisions Regarding Telepsychiatry Participation During the COVID-19 Pandemic: Telephone-Based Survey. JMIR Form. Res. 2020, 4, e25469. [Google Scholar] [CrossRef] [PubMed]
- Spooner, K.K.; Salemi, J.L.; Salihu, H.M.; Zoorob, R.J. eHealth patient-provider communication in the United States: Interest, inequalities, and predictors. J. Am. Med. Inform. Assoc. 2017, 24, e18–e27. [Google Scholar] [CrossRef]
- Tam, S.; Wu, V.F.; Williams, A.M.; Girgis, M.; Sheqwara, J.Z.; Siddiqui, F.; Chang, S.S. Disparities in the Uptake of Telemedicine During the COVID-19 Surge in a Multidisciplinary Head and Neck Cancer Population by Patient Demographic Characteristics and Socioeconomic Status. JAMA Otolaryngol. Head Neck Surg. 2020, 147, 209–211. [Google Scholar] [CrossRef]
- Tong, T.; Myers, A.K.; Bissoonauth, A.A.; Pekmezaris, R.; Kozikowski, A. Identifying the barriers and perceptions of non-Hispanic black and Hispanic/Latino persons with uncontrolled type 2 diabetes for participation in a home Telemonitoring feasibility study: A quantitative analysis of those who declined participation, withdrew or were non-adherent. Ethn. Health 2020, 25, 485–494. [Google Scholar]
- Van Veen, T.; Binz, S.; Muminovic, M.; Chaudhry, K.; Rose, K.; Calo, S.; Rammal, J.A.; France, J.; Miller, J.B. Potential of mobile health technology to reduce health disparities in underserved communities. West. J. Emerg. Med. 2019, 20, 799–803. [Google Scholar] [CrossRef]
- Wang, Y.; Do, D.P.; Wilson, F.A. Immigrants’ Use of eHealth Services in the United States, National Health Interview Survey, 2011–2015. Public Health Rep. 2018, 133, 677–684. [Google Scholar] [CrossRef]
- Weber, E.; Miller, S.J.; Astha, V.; Janevic, T.; Benn, E. Characteristics of telehealth users in NYC for COVID-related care during the coronavirus pandemic. J. Am. Med. Inform. Assoc. 2020, 27, 1949–1954. [Google Scholar] [CrossRef]
- Blundell, A.R.; Kroshinsky, D.; Hawryluk, E.B.; Das, S. Disparities in telemedicine access for Spanish-speaking patients during the COVID-19 crisis. Pediatric Dermatol. 2020, 38, 947–949. [Google Scholar] [CrossRef]
- Gilson, S.F.; Umscheid, C.A.; Laiteerapong, N.; Ossey, G.; Nunes, K.J.; Shah, S.D. Growth of Ambulatory Virtual Visits and Differential Use by Patient Sociodemographics at One Urban Academic Medical Center During the COVID-19 Pandemic: Retrospective Analysis. JMIR Med. Inform. 2020, 8, e24544. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Magit, A.E.; Carvalho, D. Equal Access to Telemedicine during COVID-19 Pandemic: A Pediatric Otolaryngology Perspective. Laryngoscope 2020, 131, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Kemp, M.T.; Williams, A.M.; Sharma, S.B.; Biesterveld, B.E.; Wakam, G.K.; Matusko, N.; Wilson, J.K.; Cohen, M.S.; Alam, H.B. Barriers associated with failed completion of an acute care general surgery telehealth clinic visit. Surgery 2020, 168, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Schifeling, C.H.; Shanbhag, P.; Johnson, A.; Atwater, R.C.; Koljack, C.; Parnes, B.L.; Vejar, M.M.; Farro, S.A.; Phimphasone-Brady, P.; Lum, H.D. Disparities in Video and Telephone Visits Among Older Adults During the COVID-19 Pandemic: Cross-Sectional Analysis. JMIR Aging 2020, 3, e23176. [Google Scholar] [CrossRef] [PubMed]
- Abel, E.A.; Shimada, S.L.; Wang, K.; Ramsey, C.; Skanderson, M.; Erdos, J.; Godleski, L.; Houston, T.K.; Brandt, C.A. Dual Use of a Patient Portal and Clinical Video Telehealth by Veterans with Mental Health Diagnoses: Retrospective, Cross-Sectional Analysis. J. Med. Internet Res. 2018, 20, e11350. [Google Scholar] [CrossRef] [PubMed]
- Chunara, R.; Zhao, Y.; Chen, J.; Lawrence, K.; Testa, P.A.; Nov, O.; Mann, D.M. Telemedicine and healthcare disparities: A cohort study in a large healthcare system in New York City during COVID-19. J. Am. Med. Inform. Assoc. 2021, 28, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Darrat, I.; Tam, S.; Boulis, M.; Williams, A.M. Socioeconomic Disparities in Patient Use of Telehealth During the Coronavirus Disease 2019 Surge. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 287–295. [Google Scholar] [CrossRef]
- Eberly, L.A.; Kallan, M.J.; Julien, H.M.; Haynes, N.; Khatana, S.A.M.; Nathan, A.S.; Snider, C.; Chokshi, N.P.; Eneanya, N.D.; Takvorian, S.U.; et al. Patient Characteristics Associated with Telemedicine Access for Primary and Specialty Ambulatory Care During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2031640. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, D.H.; Lee, L.; Huynh, S.; Haskell, T.P. Health Inequalities in the Use of Telehealth in the United States in the Lens of COVID-19. Popul. Health Manag. 2020, 23, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Wegermann, K.; Wilder, J.; Parish, A.; Niedzwiecki, D.; Gellad, Z.F.; Muir, A.J.; Patel, Y. Black, older, unmarried, and medicaid patients were less likely to complete hepatology video visits during COVID-19. Hepatology 2020, 72 (Suppl. S1), 382A–383A. [Google Scholar]
- Trief, P.M.; Izquierdo, R.; Eimicke, J.P.; Teresi, J.A.; Goland, R.; Palmas, W.; Shea, S.; Weinstock, R.S. Adherence to diabetes self care for white, African-American and Hispanic American telemedicine participants: 5 year results from the IDEATel project. Ethn. Health 2013, 18, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.M.; Hefner, J.L.; Fareed, N.; Huerta, T.R.; McAlearney, A.S. Exploring the Digital Divide: Age and Race Disparities in Use of an Inpatient Portal. Telemed. E-Health 2020, 26, 603–613. [Google Scholar] [CrossRef]
- Guendelman, S.; Broderick, A.; Mlo, H.; Gemmill, A.; Lindeman, D. Listening to Communities: Mixed-Method Study of the Engagement of Disadvantaged Mothers and Pregnant Women with Digital Health Technologies. J. Med. Internet Res. 2017, 19, e240. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.P.; Hornbrook, M.C. Differences in Access to and Preferences for Using Patient Portals and Other eHealth Technologies Based on Race, Ethnicity, and Age: A Database and Survey Study of Seniors in a Large Health Plan. J. Med. Internet Res. 2016, 18, e50. [Google Scholar] [CrossRef]
- Ferguson, J.M.; Jacobs, J.; Yefimova, M.; Greene, L.; Heyworth, L.; Zulman, D.M. Virtual Care Expansion in the Veterans Health Administration During the COVID-19 Pandemic: Clinical Services and Patient Characteristics Associated with Utilization. J. Am. Med. Inform. Assoc. JAMIA 2021, 28, 453–462. [Google Scholar] [CrossRef]
- Shiferaw, K.B.; Mengiste, S.A.; Gullslett, M.K.; Zeleke, A.A.; Tilahun, B.; Tebeje, T.; Wondimu, R.; Desalegn, S.; Mehari, E.A. Healthcare providers’ acceptance of telemedicine and preference of modalities during COVID-19 pandemics in a low-resource setting: An extended UTAUT model. PLoS ONE 2021, 16, e0250220. [Google Scholar] [CrossRef] [PubMed]
- Isautier, J.M.; Copp, T.; Ayre, J.; Cvejic, E.; Meyerowitz-Katz, G.; Batcup, C.; Bonner, C.; Dodd, R.H.; Nickel, B.; Pickles, K.; et al. Lessons from the COVID-19 pandemic: People’s experiences and satisfaction with telehealth during the COVID-19 pandemic in Australia. MedRxiv 2020. [Google Scholar] [CrossRef]
- Crawford, A.; Serhal, E. Digital health equity and COVID-19: The innovation curve cannot reinforce the social gradient of health. J. Med. Internet Res. 2020, 22, e19361. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of Telehealth During the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- DelliFraine, J.L.; Dansky, K.H. Home-based telehealth: A review and meta-analysis. J. Telemed. Telecare 2008, 14, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Freed, J.; Lowe, C.; Flodgren, G.; Binks, R.; Doughty, K.; Kolsi, J. Telemedicine: Is it really worth it? A perspective from evidence and experience. J. Innov. Health Inform. 2018, 25, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, Z.; Zhao, J.; Shi, Y. Impact of telemedicine on healthcare service system considering patients’ choice. Discret. Dyn. Nat. Soc. 2019, 2019, 7642176. [Google Scholar] [CrossRef]
- Kruse, C.S.; Krowski, N.; Rodriguez, B.; Tran, L.; Vela, J.; Brooks, M. Telehealth and patient satisfaction: A systematic review and narrative analysis. BMJ Open 2017, 7, e016242. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Barraket, J.; Wilson, C.; Holcombe-James, I.; Kennedy, J.; Rennie, E.; Ewing, S.; MacDonald, T. Measuring Australia’s Digital Divide: The Australian Digital Inclusion Index 2020; RMIT and Swinburne University of Technology: Melbourne, Australia, 2020. [Google Scholar]
- Clare, C.A. Telehealth and the digital divide as a social determinant of health during the COVID-19 pandemic. Netw. Modeling Anal. Health Inform. Bioinform. 2021, 10, 26. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sl. | Search Terms |
|---|---|
| 1 | “telemedicine” [MeSH Terms] OR “telemedicine” [Text Word] |
| 2 | “tele medicine” [Text Word] |
| 3 | “telehealth” [Text Word] |
| 4 | “tele health” [Text Word] |
| 5 | “tele-health” [Text Word] |
| 6 | “e-health” [Text Word] |
| 7 | “teletherapy” [Text Word] |
| 8 | “virtual care” [Text Word] |
| 9 | “virtual health” [Text Word] |
| 10 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 |
| 11 | “disparit*” [Text Word] |
| 12 | “health equity” [MeSH Terms] OR “health equity” [Text Word] |
| 13 | “equit*” [Text Word] |
| 14 | “inequit*” [Text Word] |
| 15 | “inequalit*” [Text Word] |
| 16 | “healthcare disparities” [MeSH Terms] OR “health care disparities” [Text Word] |
| 17 | “health status disparities” [MeSH Terms] OR “health status disparities” [Text Word] |
| 18 | 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 |
| 19 | 10 and 18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mistry, S.K.; Shaw, M.; Raffan, F.; Johnson, G.; Perren, K.; Shoko, S.; Harris-Roxas, B.; Haigh, F. Inequity in Access and Delivery of Virtual Care Interventions: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 9411. https://doi.org/10.3390/ijerph19159411
Mistry SK, Shaw M, Raffan F, Johnson G, Perren K, Shoko S, Harris-Roxas B, Haigh F. Inequity in Access and Delivery of Virtual Care Interventions: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9411. https://doi.org/10.3390/ijerph19159411
Chicago/Turabian StyleMistry, Sabuj Kanti, Miranda Shaw, Freya Raffan, George Johnson, Katelyn Perren, Saito Shoko, Ben Harris-Roxas, and Fiona Haigh. 2022. "Inequity in Access and Delivery of Virtual Care Interventions: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 15: 9411. https://doi.org/10.3390/ijerph19159411
APA StyleMistry, S. K., Shaw, M., Raffan, F., Johnson, G., Perren, K., Shoko, S., Harris-Roxas, B., & Haigh, F. (2022). Inequity in Access and Delivery of Virtual Care Interventions: A Scoping Review. International Journal of Environmental Research and Public Health, 19(15), 9411. https://doi.org/10.3390/ijerph19159411