
The Evolution of Effort-Reward Imbalance in Workers during the COVID-19 Pandemic in France—An Observational Study in More than 8000 Workers

 , , ,
, , ,  , , ,
, , ,  ,
,  ,
,  , , ,
, , ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
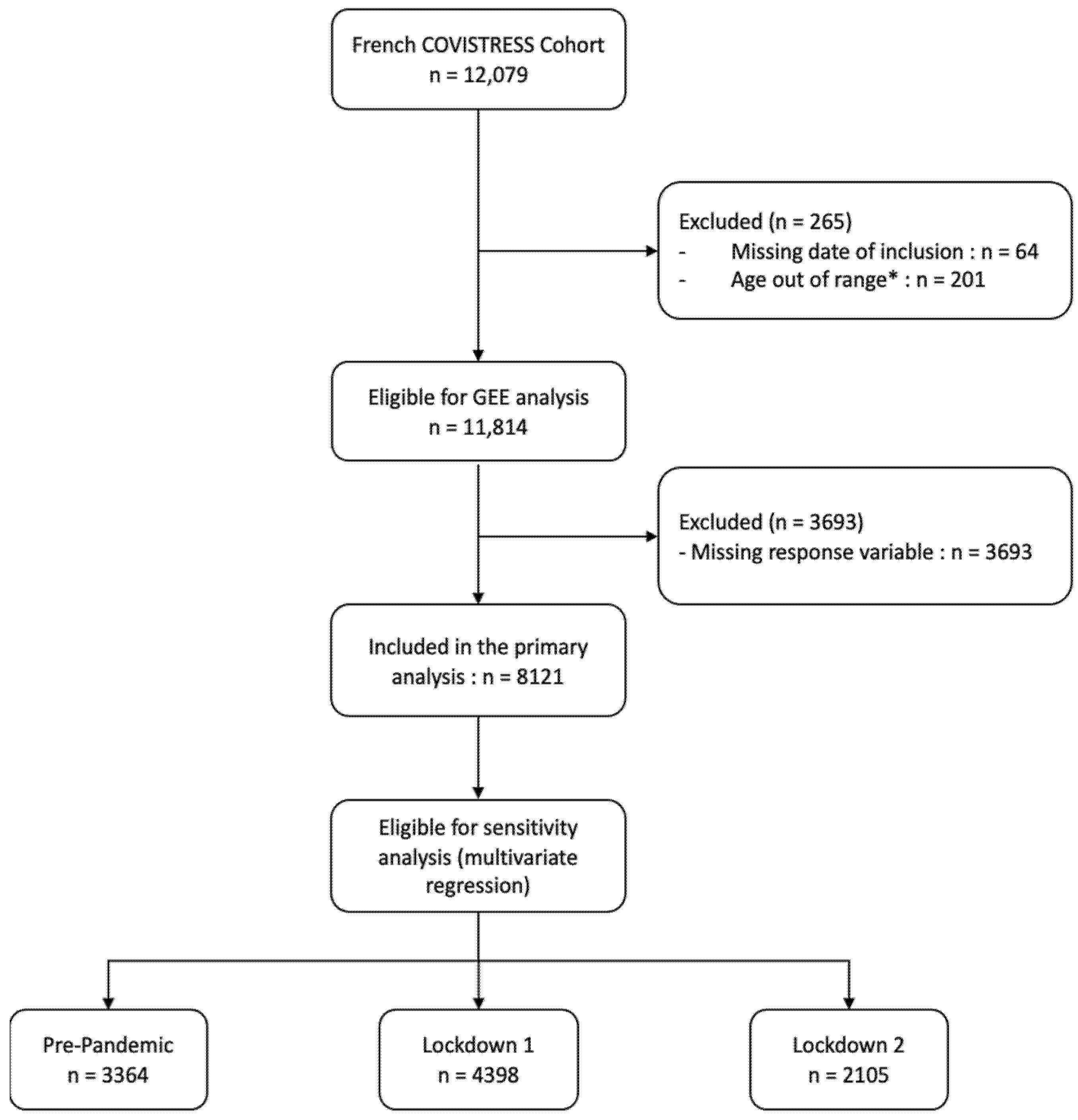
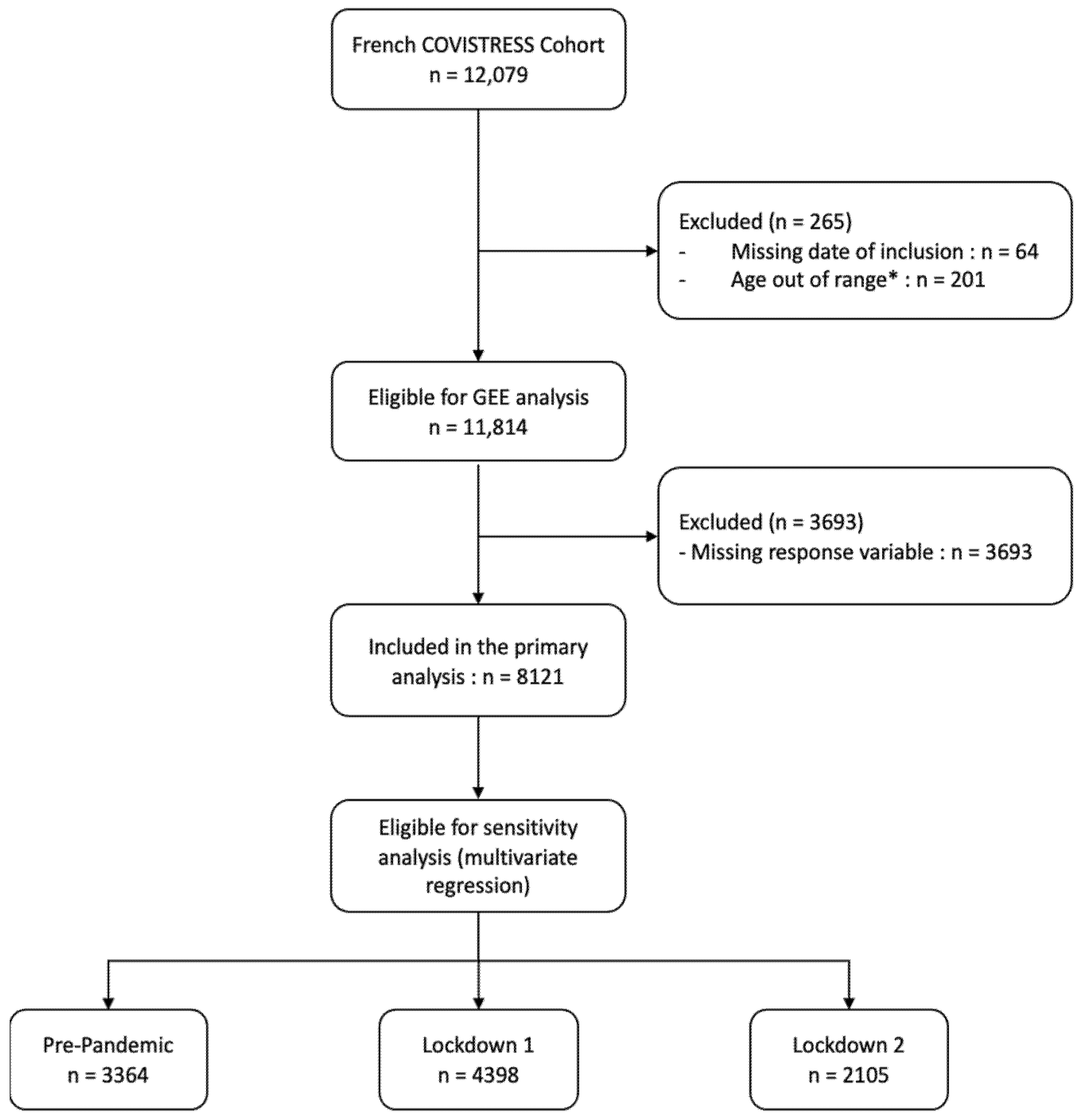
2.2. Participants
2.3. Instrument Survey
2.4. Statistical Analysis
3. Results
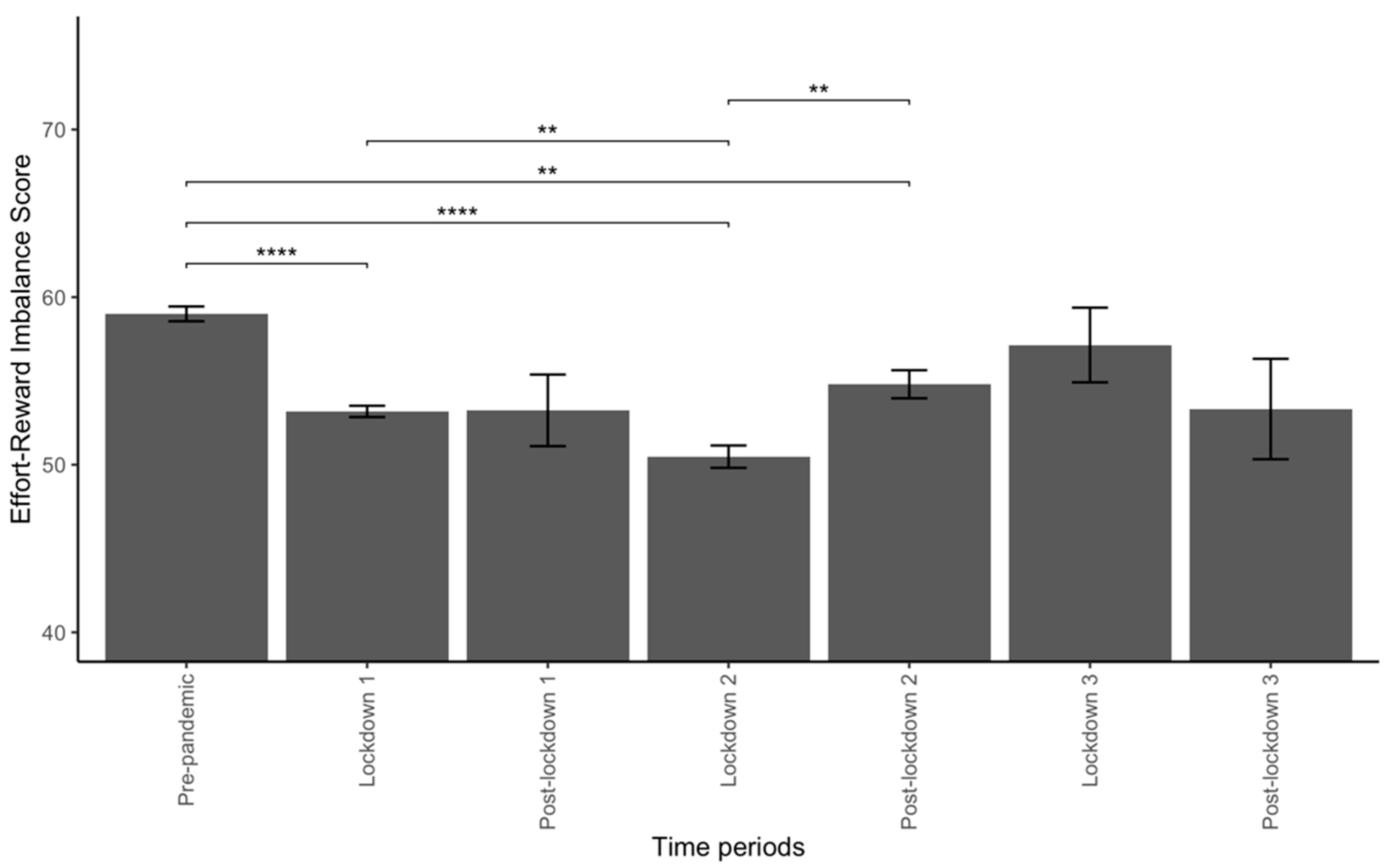
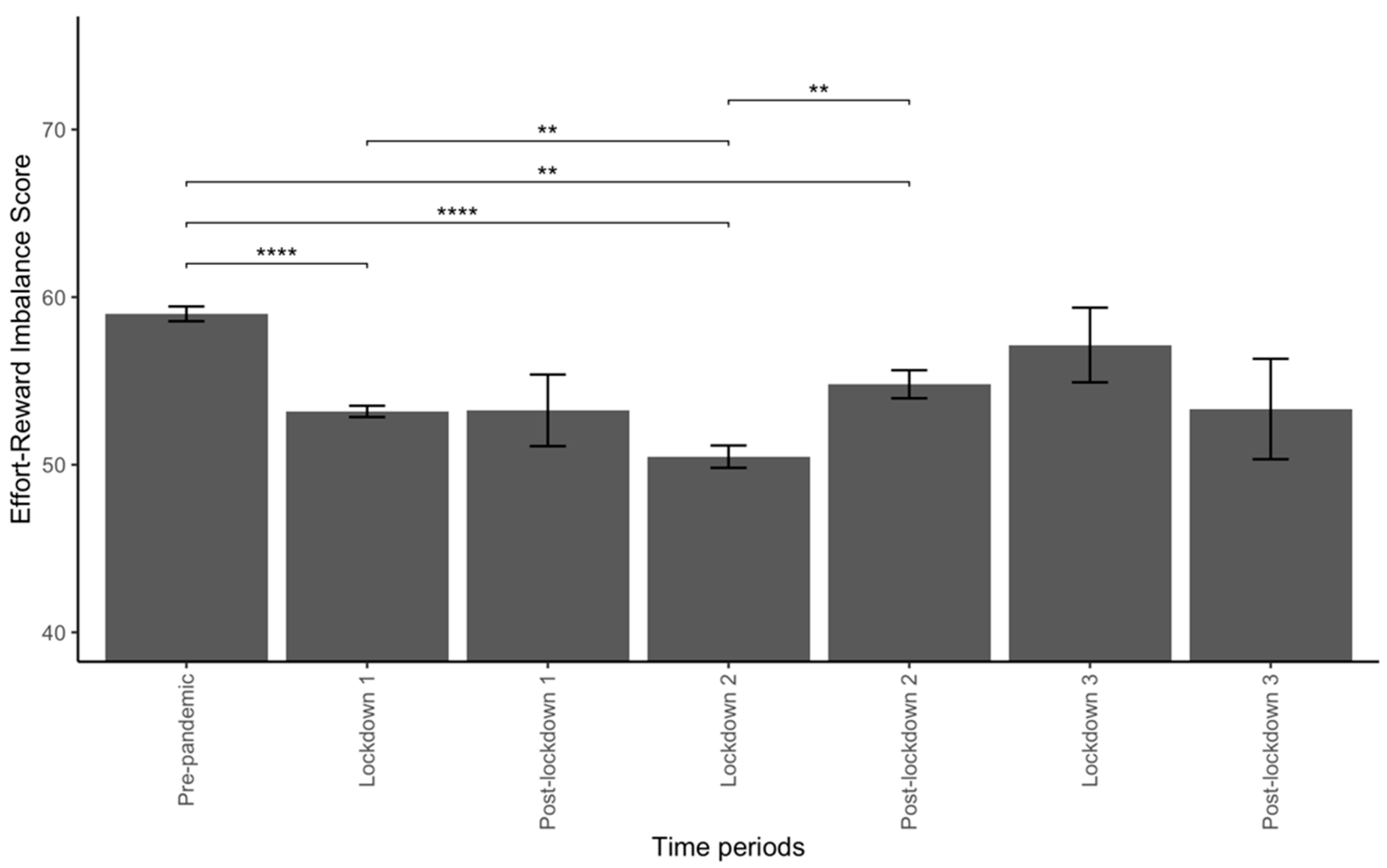
3.1. Variations of ERI during the Pandemic
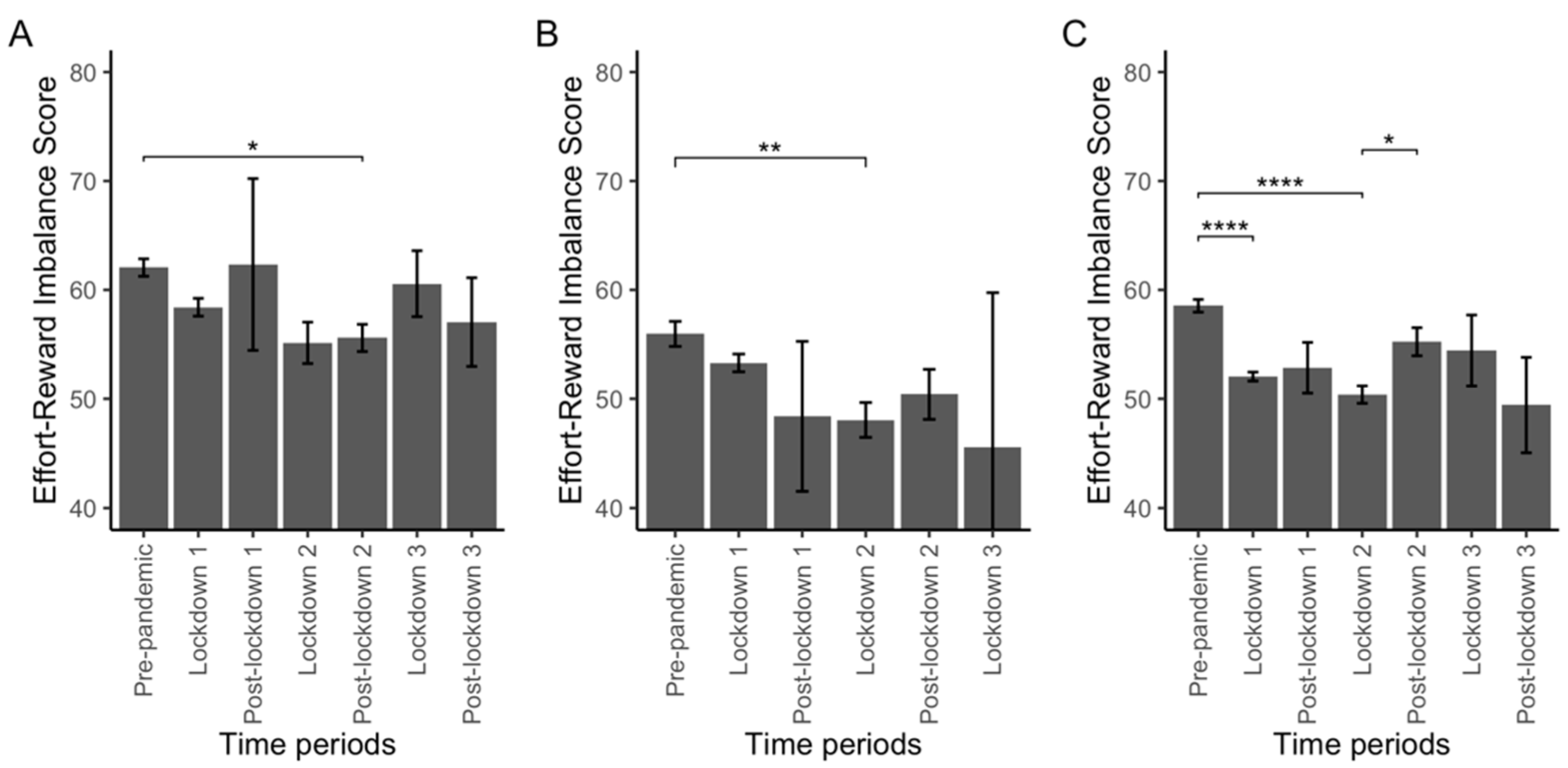
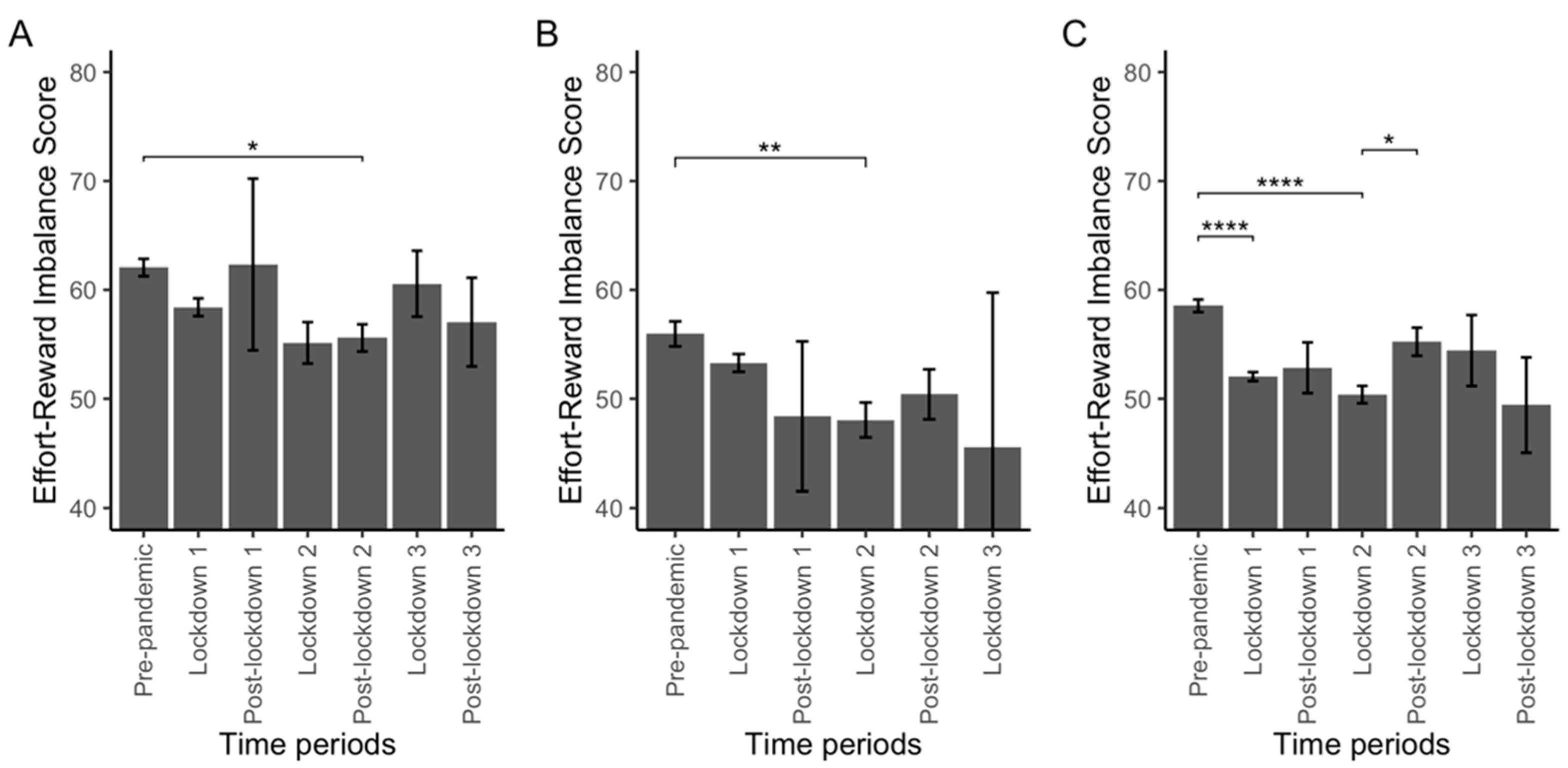
3.2. Variations of ERI by Occupation
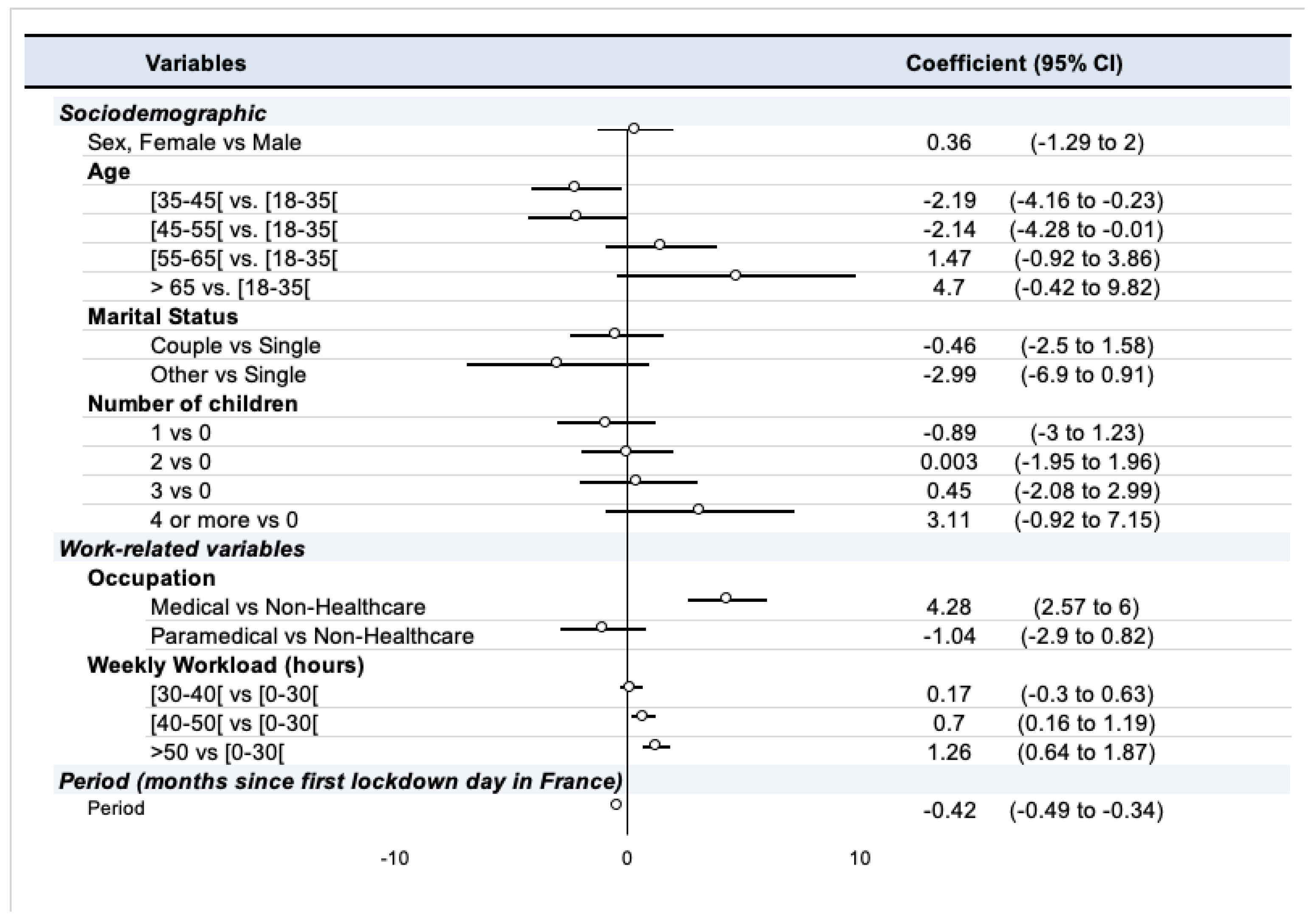
3.3. Factors Influencing ERI during the Pandemic
3.4. Did the influence of factors associated with ERI change during the pandemic?
4. Discussion
4.1. How the ERI Has Evolved over the Course of the Pandemic
4.2. Differences in ERI between Medical and Paramedical Professionals
4.3. Factors Associated with ERI
4.4. How Time Modifies the Strength of the Association between ERI and Its Associated Factors
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garbóczy, S.; Szemán-Nagy, A.; Ahmad, M.S.; Harsányi, S.; Ocsenás, D.; Rekenyi, V.; Al-Tammemi, A.B.; Kolozsvári, L.R. Health Anxiety, Perceived Stress, and Coping Styles in the Shadow of the COVID-19. BMC Psychol. 2021, 9, 53. [Google Scholar] [CrossRef]
- Sandoval-Reyes, J.; Idrovo-Carlier, S.; Duque-Oliva, E.J. Remote Work, Work Stress, and Work–Life during Pandemic Times: A Latin America Situation. Int. J. Environ. Res. Public Health 2021, 18, 7069. [Google Scholar] [CrossRef]
- Galanti, T.; Guidetti, G.; Mazzei, E.; Zappalà, S.; Toscano, F. Work from Home during the COVID-19 Outbreak: The Impact on Employees’ Remote Work Productivity, Engagement and Stress. J. Occup. Environ. Med. 2021. publish ahead of print. [Google Scholar] [CrossRef]
- Murat, M.; Köse, S.; Savaşer, S. Determination of Stress, Depression and Burnout Levels of Front-line Nurses during the COVID-19 Pandemic. Int. J. Ment. Health Nurs. 2021, 30, 533–543. [Google Scholar] [CrossRef]
- Labrague, L.J.; Santos, J.A.A. Fear of COVID-19, Psychological Distress, Work Satisfaction and Turnover Intention among Frontline Nurses. J. Nurs. Manag. 2021, 29, 395–403. [Google Scholar] [CrossRef]
- Minahan, J.; Falzarano, F.; Yazdani, N.; Siedlecki, K.L. The COVID-19 Pandemic and Psychosocial Outcomes Across Age Through the Stress and Coping Framework. Gerontologist 2021, 61, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Manzano García, G.; Ayala Calvo, J.C. The Threat of COVID-19 and Its Influence on Nursing Staff Burnout. J. Adv. Nurs. 2021, 77, 832–844. [Google Scholar] [CrossRef]
- Charles, N.E.; Strong, S.J.; Burns, L.C.; Bullerjahn, M.R.; Serafine, K.M. Increased Mood Disorder Symptoms, Perceived Stress, and Alcohol Use among College Students during the COVID-19 Pandemic. Psychiatry Res. 2021, 296, 113706. [Google Scholar] [CrossRef]
- Ceri, V.; Cicek, I. Psychological Well-Being, Depression and Stress During COVID-19 Pandemic in Turkey: A Comparative Study of Healthcare Professionals and Non-Healthcare Professionals. Psychol. Health Med. 2021, 26, 85–97. [Google Scholar] [CrossRef]
- Apouey, B.; Roulet, A.; Solal, I.; Stabile, M. Gig Workers during the COVID-19 Crisis in France: Financial Precarity and Mental Well-Being. J. Urban Health 2020, 97, 776–795. [Google Scholar] [CrossRef]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.; Yang, P.; Hsu, H.; Su, C.; Chen, C.; Yeh, I.; Wu, Y.; Chen, L. Survey on Perceived Work Stress and Its Influencing Factors among Hospital Staff during the COVID-19 Pandemic in Taiwan. Kaohsiung J. Med. Sci. 2020, 36, 944–952. [Google Scholar] [CrossRef]
- Wardell, J.D.; Kempe, T.; Rapinda, K.K.; Single, A.; Bilevicius, E.; Frohlich, J.R.; Hendershot, C.S.; Keough, M.T. Drinking to Cope During COVID-19 Pandemic: The Role of External and Internal Factors in Coping Motive Pathways to Alcohol Use, Solitary Drinking, and Alcohol Problems. Alcohol. Clin. Exp. Res. 2020, 44, 2073–2083. [Google Scholar] [CrossRef]
- Raudenská, J.; Steinerová, V.; Javůrková, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational Burnout Syndrome and Post-Traumatic Stress among Healthcare Professionals during the Novel Coronavirus Disease 2019 (COVID-19) Pandemic. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef]
- Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. [Google Scholar] [CrossRef] [PubMed]
- Restauri, N.; Sheridan, A.D. Burnout and Posttraumatic Stress Disorder in the Coronavirus Disease 2019 (COVID-19) Pandemic: Intersection, Impact, and Interventions. J. Am. Coll. Radiol. 2020, 17, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Kluge, H.H.P. Statement—Physical and Mental Health Key to Resilience during COVID-19 Pandemic. Available online: https://www.who.int/europe/news/item/26-03-2020-statement-physical-and-mental-health-key-to-resilience-during-covid-19-pandemic (accessed on 14 July 2022).
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak; WHO: Geneva, Switzerland, 2020; pp. 1–6. [Google Scholar]
- National Center for Chronic Disease Prevention and Health Promotion, Division of Population Health Coping with Stress. Coping with Stress. CDC Mental Health. 2022. Available online: https://www.cdc.gov/mentalhealth/stress-coping/cope-with-stress/index.html (accessed on 14 July 2022).
- Siegrist, J. Adverse Health Effects of High-Effort/Low-Reward Conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef]
- Violanti, J.M.; Mnatsakanova, A.; Andrew, M.E.; Allison, P.; Gu, J.K.; Fekedulegn, D. Effort-Reward Imbalance and Overcommitment at Work: Associations with Police Burnout. Police Q. 2018, 21, 440–460. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, J.; Bosma, H.; Peter, R.; Siegrist, J. Job Strain, Effort-Reward Imbalance and Employee Well-Being: A Large-Scale Cross-Sectional Study. Soc. Sci. Med. 2000, 50, 1317–1327. [Google Scholar] [CrossRef]
- Godin, I.; Kittel, F.; Coppieters, Y.; Siegrist, J. A Prospective Study of Cumulative Job Stress in Relation to Mental Health. BMC Public Health 2005, 5, 67. [Google Scholar] [CrossRef]
- Kivimäki, M.; Leino-Arjas, P.; Luukkonen, R.; Riihimäki, H.; Vahtera, J.; Kirjonen, J. Work Stress and Risk of Cardiovascular Mortality: Prospective Cohort Study of Industrial Employees. BMJ 2002, 325, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Vegchel, N.; de Jonge, J.; Bosma, H.; Schaufeli, W. Reviewing the Effort–Reward Imbalance Model: Drawing up the Balance of 45 Empirical Studies. Soc. Sci. Med. 2005, 60, 1117–1131. [Google Scholar] [CrossRef] [PubMed]
- Dey, A.; Majumdar, P.; Saha, A.; Sahu, S. COVID-19 Pandemic Lockdown-Induced Altered Sleep/Wake Circadian Rhythm, Health Complaints and Stress among Traffic Police Personnel in India. Chronobiol. Int. 2021, 38, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Couarraze, S.; Delamarre, L.; Marhar, F.; Quach, B.; Jiao, J.; Avilés Dorlhiac, R.; Saadaoui, F.; Liu, A.S.-I.; Dubuis, B.; Antunes, S.; et al. The Major Worldwide Stress of Healthcare Professionals during the First Wave of the COVID-19 Pandemic—the International COVISTRESS Survey. PLoS ONE 2021, 16, e0257840. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion Fatigue, Burnout, Compassion Satisfaction and Perceived Stress in Healthcare Professionals during the COVID-19 Health Crisis in Spain. J. Creat. Behav. 2020, 29, 4321–4330. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, H.; Chen, J.; Zhang, X.; Yue, X.; Ke, J.; Wang, B.; Peng, C. Emergency Management of Nursing Human Resources and Supplies to Respond to Coronavirus Disease 2019 Epidemic. Int. J. Nurs. Sci. 2020, 7, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Humphries, N.; Morgan, K.; Catherine Conry, M.; McGowan, Y.; Montgomery, A.; McGee, H. Quality of Care and Health Professional Burnout: Narrative Literature Review. Int. J. Health Care Qual. Assur. 2014, 27, 293–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert-Ouimet, M.; Brisson, C.; Vézina, M. Psychosocial Work Stressors, High Family Responsibilities, and Psychological Distress among Women: A 5-year Prospective Study. Am. J. Ind. Med. 2020, 63, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Sperlich, S.; Geyer, S. The Impact of Social and Family-Related Factors on Women’s Stress Experience in Household and Family Work. Int. J. Public Health 2015, 60, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Pereira, B.; Moustafa, F.; Naughton, G.; Lesage, F.-X.; Lambert, C. At-Risk and Intervention Thresholds of Occupational Stress Using a Visual Analogue Scale. PLoS ONE 2017, 12, e0178948. [Google Scholar] [CrossRef] [Green Version]
- Ballinger, G.A. Using Generalized Estimating Equations for Longitudinal Data Analysis. Organ. Res. Methods 2004, 7, 127–150. [Google Scholar] [CrossRef]
- Zeger, S.L.; Liang, K.-Y. Longitudinal Data Analysis for Discrete and Continuous Outcomes. Biometrics 1986, 42, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, K.-Y.; Zeger, S.L. Longitudinal Data Analysis Using Generalized Linear Models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Pan, W. Akaike’s Information Criterion in Generalized Estimating Equations. Biometrics 2001, 57, 120–125. [Google Scholar] [CrossRef]
- INSEE. Tableaux de L’économie Française. Edition 2017; Insee Références; INSEE (Institut national de la statistique et des études économiques): Paris, France, 2017. [Google Scholar]
- INSEE. Activité, Emploi et Chômage en 2019 et en Séries Longues. Enquête Emploi en Continu; Insee Résultats; INSEE (Institut national de la statistique et des études économiques): Paris, France, 2020. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological Distress, Coping Behaviors, and Preferences for Support among New York Healthcare Workers during the COVID-19 Pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ross, J. The Exacerbation of Burnout During COVID-19: A Major Concern for Nurse Safety. J. Perianesthesia Nurs. 2020, 35, 439–440. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, Anxiety, Stress Levels of Physicians and Associated Factors in Covid-19 Pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef]
- Bouziri, H.; Smith, D.R.M.; Descatha, A.; Dab, W.; Jean, K. Working from Home in the Time of COVID-19: How to Best Preserve Occupational Health? Occup. Environ. Med. 2020, 77, 509–510. [Google Scholar] [CrossRef]
- Godeluck, S. Pénuries de Personnel: Les Hôpitaux ne Parviennent pas à se Relever Après Dix-Huit Mois de Covid. Les Echos. 28 October 2021. Available online: https://www.lesechos.fr/economie-france/social/penuries-de-personnel-les-hopitaux-ne-parviennent-pas-a-se-relever-apres-dix-huit-mois-de-covid-1359372 (accessed on 1 February 2022).
- Sauvage, G. Pénurie de Soignants: Le Modèle Hospitalier Français au Bord de la Rupture. France24. 29 October 2021. Available online: https://www.france24.com/fr/france/20211029-p%C3%A9nurie-de-soignants-le-mod%C3%A8le-hospitalier-fran%C3%A7ais-au-bord-de-la-rupture (accessed on 1 February 2022).
- Parmentier, A. “Une Explosion de Burn-Out”: Après le Covid, les Hôpitaux face à une Pénurie de Soignants. L’Express. 12 October 2021. Available online: https://www.lexpress.fr/actualite/societe/sante/une-explosion-de-burn-out-apres-le-covid-les-hopitaux-face-aux-penuries-de-soignants_2160309.html (accessed on 1 February 2022).
- Décret n° 2020-325 du 25 Mars 2020 Relatif à L’activité Partielle. 2020. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000041755956#:~:text=Notice%20%3A%20le%20texte%20modifie%20les,%C3%A9viter%20les%20risques%20de%20licenciement (accessed on 1 June 2022).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Period | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | Pre-Pandemic * | Lockdown 1 | Post-Lockdown 1 | Lockdown 2 | Post-Lockdown 2 | Lockdown 3 | Post-Lockdown 3 | p-Value | |
| (n = 8121) | (n = 3364) | (n = 4398) | (n = 209) | (n = 2105) | (n = 1186) | (n = 138) | (n = 85) | ||
| Gender | |||||||||
| Male | 1957 (24.1%) | 859 (25.5%) | 1002 (22.8%) | 59 (28.2%) | 450 (21.4%) | 381 (32.1%) | 30 (21.7%) | 35 (41.2%) | <0.001 |
| Female | 6143 (75.6%) | 2496 (74.2%) | 3385 (77.0%) | 149 (71.3%) | 1650 (78.4%) | 802 (67.6%) | 108 (78.3%) | 49 (57.6%) | |
| Missing | 21 (0.3%) | 9 (0.3%) | 11 (0.3%) | 1 (0.5%) | 5 (0.2%) | 3 (0.3%) | 0 (0%) | 1 (1.2%) | |
| Age | |||||||||
| under 35 | 2358 (29.0%) | 773 (23.0%) | 1483 (33.7%) | 67 (32.1%) | 449 (21.3%) | 269 (22.7%) | 57 (41.3%) | 33 (38.8%) | <0.001 |
| 35–45 | 2243 (27.6%) | 893 (26.5%) | 1247 (28.4%) | 52 (24.9%) | 571 (27.1%) | 325 (27.4%) | 28 (20.3%) | 20 (23.5%) | |
| 45–55 | 2050 (25.2%) | 940 (27.9%) | 1018 (23.1%) | 56 (26.8%) | 623 (29.6%) | 313 (26.4%) | 27 (19.6%) | 13 (15.3%) | |
| 55-65 | 1257 (15.5%) | 640 (19.0%) | 562 (12.8%) | 29 (13.9%) | 404 (19.2%) | 226 (19.1%) | 23 (16.7%) | 13 (15.3%) | |
| above 65 | 213 (2.6%) | 118 (3.5%) | 88 (2.0%) | 5 (2.4%) | 58 (2.8%) | 53 (4.5%) | 3 (2.2%) | 6 (7.1%) | |
| Marital Status | |||||||||
| as_single | 812 (10.0%) | 752 (22.4%) | 27 (0.6%) | 1 (0.5%) | 509 (24.2%) | 228 (19.2%) | 27 (19.6%) | 20 (23.5%) | <0.001 |
| as_couple | 5045 (62.1%) | 2384 (70.9%) | 2442 (55.5%) | 114 (54.5%) | 1436 (68.2%) | 895 (75.5%) | 98 (71.0%) | 60 (70.6%) | |
| other | 310 (3.8%) | 114 (3.4%) | 182 (4.1%) | 11 (5.3%) | 84 (4.0%) | 28 (2.4%) | 4 (2.9%) | 1 (1.2%) | |
| Missing | 1954 (24.1%) | 114 (3.4%) | 1747 (39.7%) | 83 (39.7%) | 76 (3.6%) | 35 (3.0%) | 9 (6.5%) | 4 (4.7%) | |
| Number of Children | |||||||||
| 0 | 2656 (32.7%) | 949 (28.2%) | 1589 (36.1%) | 79 (37.8%) | 578 (27.5%) | 335 (28.2%) | 50 (36.2%) | 25 (29.4%) | <0.001 |
| 1 | 1298 (16.0%) | 523 (15.5%) | 720 (16.4%) | 24 (11.5%) | 356 (16.9%) | 168 (14.2%) | 19 (13.8%) | 11 (12.9%) | |
| 2 | 2456 (30.2%) | 1100 (32.7%) | 1252 (28.5%) | 60 (28.7%) | 722 (34.3%) | 372 (31.4%) | 30 (21.7%) | 20 (23.5%) | |
| 3 | 975 (12.0%) | 473 (14.1%) | 459 (10.4%) | 24 (11.5%) | 267 (12.7%) | 190 (16.0%) | 18 (13.0%) | 17 (20.0%) | |
| 4 or more | 306 (3.8%) | 164 (4.9%) | 131 (3.0%) | 3 (1.4%) | 81 (3.8%) | 76 (6.4%) | 9 (6.5%) | 6 (7.1%) | |
| Missing | 430 (5.3%) | 155 (4.6%) | 247 (5.6%) | 19 (9.1%) | 101 (4.8%) | 45 (3.8%) | 12 (8.7%) | 6 (7.1%) | |
| Occupation | |||||||||
| other | 5580 (68.7%) | 2060 (61.2%) | 3266 (74.3%) | 163 (78.0%) | 1514 (71.9%) | 537 (45.3%) | 59 (42.8%) | 41 (48.2%) | <0.001 |
| medical | 1196 (14.7%) | 814 (24.2%) | 328 (7.5%) | 21 (10.0%) | 225 (10.7%) | 506 (42.7%) | 72 (52.2%) | 44 (51.8%) | |
| paramedical | 1345 (16.6%) | 490 (14.6%) | 804 (18.3%) | 25 (12.0%) | 366 (17.4%) | 143 (12.1%) | 7 (5.1%) | 0 (0%) | |
| Working hours pre-pandemic (per week) | |||||||||
| <30 | 351 (4.3%) | 333 (9.9%) | 0 (0%) | 0 (0%) | 249 (11.8%) | 83 (7.0%) | 10 (7.2%) | 9 (10.6%) | NA |
| >50 | 506 (6.2%) | 490 (14.6%) | 0 (0%) | 0 (0%) | 158 (7.5%) | 304 (25.6%) | 25 (18.1%) | 19 (22.4%) | |
| 30–40 | 1517 (18.7%) | 1461 (43.4%) | 0 (0%) | 0 (0%) | 1061 (50.4%) | 399 (33.6%) | 39 (28.3%) | 18 (21.2%) | |
| 40–50 | 659 (8.1%) | 641 (19.1%) | 0 (0%) | 0 (0%) | 316 (15.0%) | 273 (23.0%) | 43 (31.2%) | 27 (31.8%) | |
| Missing | 5088 (62.7%) | 439 (13.1%) | 4398 (100%) | 209 (100%) | 321 (15.2%) | 127 (10.7%) | 21 (15.2%) | 12 (14.1%) | |
| Weekly Working Hours during the Pandemic Period | |||||||||
| <30 | 947 (11.7%) | - | 507 (11.5%) | 27 (12.9%) | 276 (13.1%) | 109 (9.2%) | 17 (12.3%) | 11 (12.9%) | <0.001 |
| >50 | 813 (10.0%) | - | 203 (4.6%) | 13 (6.2%) | 199 (9.5%) | 341 (28.8%) | 35 (25.4%) | 22 (25.9%) | |
| 30–40 | 4027 (49.6%) | - | 2538 (57.7%) | 106 (50.7%) | 974 (46.3%) | 353 (29.8%) | 39 (28.3%) | 17 (20.0%) | |
| 40–50 | 1407 (17.3%) | - | 677 (15.4%) | 39 (18.7%) | 345 (16.4%) | 289 (24.4%) | 34 (24.6%) | 23 (27.1%) | |
| Missing | 927 (11.4%) | - | 473 (10.8%) | 24 (11.5%) | 311 (14.8%) | 94 (7.9%) | 13 (9.4%) | 12 (14.1%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delamarre, L.; Tannous, S.; Lakbar, I.; Couarraze, S.; Pereira, B.; Leone, M.; Marhar, F.; Baker, J.S.; Bagheri, R.; Berton, M.; et al. The Evolution of Effort-Reward Imbalance in Workers during the COVID-19 Pandemic in France—An Observational Study in More than 8000 Workers. Int. J. Environ. Res. Public Health 2022, 19, 9113. https://doi.org/10.3390/ijerph19159113
Delamarre L, Tannous S, Lakbar I, Couarraze S, Pereira B, Leone M, Marhar F, Baker JS, Bagheri R, Berton M, et al. The Evolution of Effort-Reward Imbalance in Workers during the COVID-19 Pandemic in France—An Observational Study in More than 8000 Workers. International Journal of Environmental Research and Public Health. 2022; 19(15):9113. https://doi.org/10.3390/ijerph19159113
Chicago/Turabian StyleDelamarre, Louis, Salma Tannous, Ines Lakbar, Sébastien Couarraze, Bruno Pereira, Marc Leone, Fouad Marhar, Julien S. Baker, Reza Bagheri, Mickael Berton, and et al. 2022. "The Evolution of Effort-Reward Imbalance in Workers during the COVID-19 Pandemic in France—An Observational Study in More than 8000 Workers" International Journal of Environmental Research and Public Health 19, no. 15: 9113. https://doi.org/10.3390/ijerph19159113
APA StyleDelamarre, L., Tannous, S., Lakbar, I., Couarraze, S., Pereira, B., Leone, M., Marhar, F., Baker, J. S., Bagheri, R., Berton, M., Rabbouch, H., Zak, M., Sikorski, T., Wasik, M., Nasir, H., Quach, B., Jiao, J., Aviles, R., COVISTRESS Network, ... Dutheil, F. (2022). The Evolution of Effort-Reward Imbalance in Workers during the COVID-19 Pandemic in France—An Observational Study in More than 8000 Workers. International Journal of Environmental Research and Public Health, 19(15), 9113. https://doi.org/10.3390/ijerph19159113