
Survey of Pharmacists’ Knowledge, Attitudes, and Practices (KAP) concerning COVID-19 Infection Control after Being Involved in Vaccine Preparation: A Cross-Sectional Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
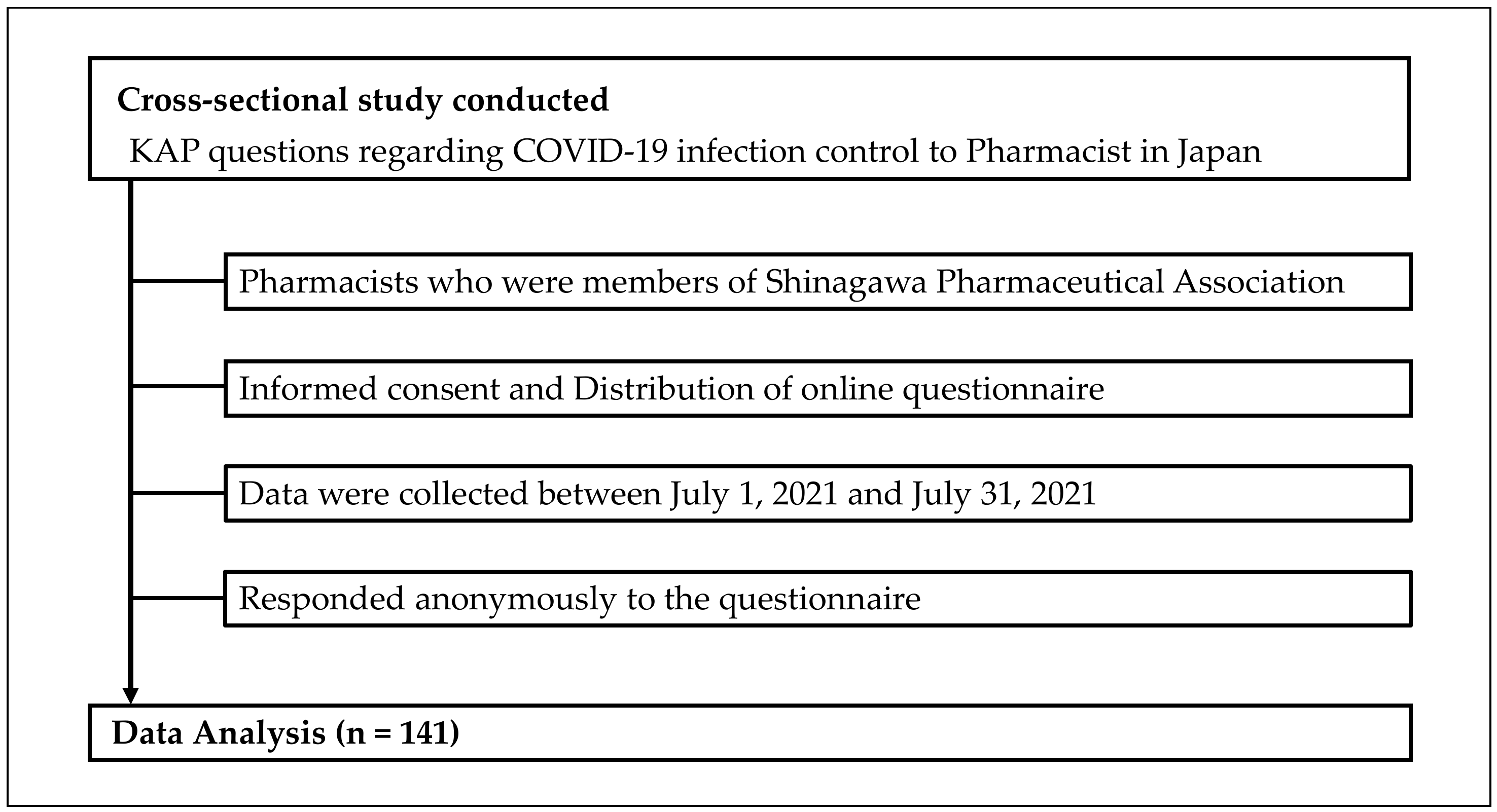
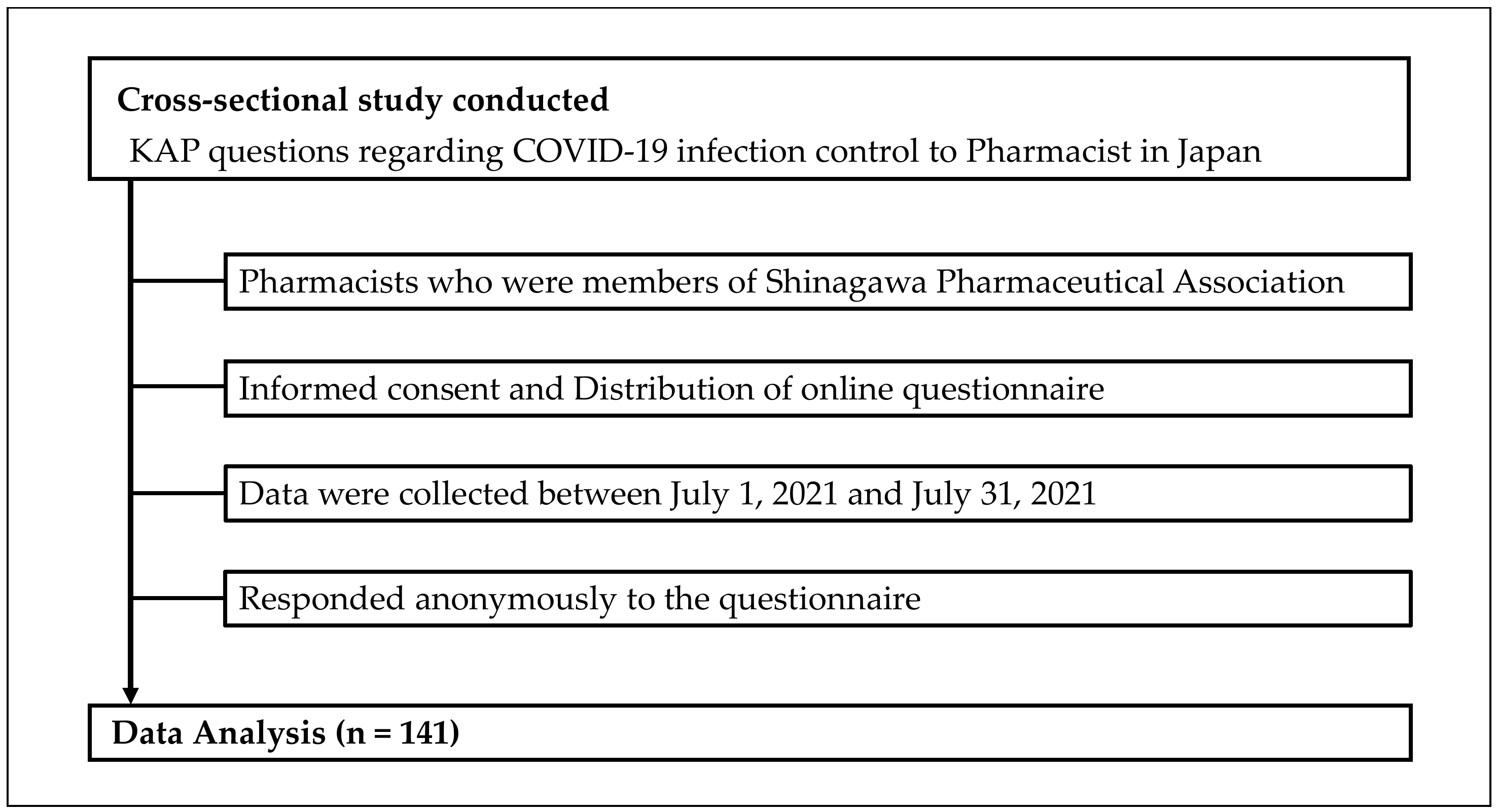
2.1. Study Design and Setting
2.2. Content of the Survey Instrument
2.3. Definition of Terms
2.4. Study Variables
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Participant Information
3.2. Pharmacists’ Knowledge of COVID-19
3.3. Attitudes of Pharmacists regarding COVID-19
3.4. Practices of Pharmacists regarding COVID-19
3.5. Correlations between Knowledge, Attitude, and Practice Scores
3.6. Relationship between Participants’ Attributes and KAP Scores
3.7. Extraction of Factors Associated with KAP Scores by Stepwise Logistic Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe Acute Respiratory Syndrome coronavirus-2 (SARS-CoV-2): A Global Pandemic and Treatment Strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- PAHO. WHO Characterizes COVID-19 as a Pandemic. Available online: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=15756:who-characterizes-covid-19-as-a-pandemic&Itemid=1926&lang=en (accessed on 23 June 2022).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 23 June 2022).
- WHO. Considerations in Adjusting Public Health and Social Measures in the Context of COVID-19 Interim Guidance. Available online: https://www.who.int/publications/i/item/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance (accessed on 23 June 2022).
- Venegas-Vera, A.V.; Colbert, G.B.; Lerma, E.V. Positive and Negative Impact of Social Media in the COVID-19 Era. Rev. Cardiovasc. Med. 2020, 21, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.; Malik, M.; Raees, V.; Anwar, A. Role of Mass Media and Public Health Communications in the COVID-19 Pandemic. Cureus 2020, 12, e10453. [Google Scholar] [CrossRef]
- Hoffmann, C.; Wolf, E. Older Age Groups and Country-Specific Case Fatality Rates of COVID-19 in Europe, USA and Canada. Infection 2021, 49, 111–116. [Google Scholar] [CrossRef]
- Huang, Q.; Jackson, S.; Derakhshan, S.; Lee, L.; Pham, E.; Jackson, A.; Cutter, S.L. Urban-Rural Differences in COVID-19 Exposures and Outcomes in the South: A Preliminary Analysis of South Carolina. PLoS ONE 2021, 16, e0246548. [Google Scholar] [CrossRef]
- Agomo, C.O. The Role of Community Pharmacists in Public Health: A Scoping Review of the Literature. J. Pharm. Health Serv. Res. 2012, 3, 25–33. [Google Scholar] [CrossRef]
- Visacri, M.B.; Figueiredo, I.V.; Lima, T.M. Role of Pharmacist during the COVID-19 Pandemic: A Scoping Review. Res. Soc. Adm. Pharm. 2021, 17, 1799–1806. [Google Scholar] [CrossRef]
- Gravlee, E.; Pittman, E.; Sparkmon, W.; Imeri, H.; Cox, H.F.; Barnard, M. COVID-19 Vaccination Engagement and Barriers among Mississippi Pharmacists. Pharmacy 2021, 9, 167. [Google Scholar] [CrossRef]
- Mukattash, T.L.; Jarab, A.S.; Abu Farha, R.K.; Nusair, M.B.; Al Muqatash, S. Pharmacists’ Perspectives on Providing the COVID-19 Vaccine in Community Pharmacies. J. Pharm. Health Serv. Res. 2021, 12, 313–316. [Google Scholar] [CrossRef]
- Liu, S.; Luo, P.; Tang, M.; Hu, Q.; Polidoro, J.P.; Sun, S.; Gong, Z. Providing Pharmacy Services during the Coronavirus Pandemic. Int. J. Clin. Pharm. 2020, 28, 299–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoudjafari, Z.; Alexander, M.; Roddy, J.; Shaw, R.; Shigle, T.L.; Timlin, C.; Culos, K. American Society for Transplantation and Cellular Therapy Pharmacy Special Interest Group Position Statement on Pharmacy Practice Management and Clinical Management for COVID-19 in Hematopoietic Cell Transplantation and Cellular Therapy Patients in the United States. Biol. Blood Marrow Transplant. 2020, 26, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Cadogan, C.A.; Hughes, C.M. On the Frontline against COVID-19: Community Pharmacists’ Contribution during a Public Health Crisis. Res. Soc. Adm. Pharm. 2021, 17, 2032–2035. [Google Scholar] [CrossRef] [PubMed]
- Mallhi, T.H.; Liaqat, A.; Abid, A.; Khan, Y.H.; Alotaibi, N.H.; Alzarea, A.I.; Tanveer, N.; Khan, T.M. Multilevel Engagements of Pharmacists during the COVID-19 Pandemic: The Way Forward. Front. Public Health 2020, 8, 561924. [Google Scholar] [CrossRef]
- WHO. A Guide to Developing Knowledge, Attitude and Practice Surveys. Available online: https://apps.who.int/iris/bitstream/handle/10665/43790/9789241596176_eng.pdf?sequence=1 (accessed on 23 June 2022).
- Salman, M.; Mustafa, Z.; Asif, N.; Zaidi, H.A.; Shehzadi, N.; Khan, T.M.; Saleem, Z.; Hussain, K. Knowledge, Attitude and Preventive Practices Related to COVID-19 among Health Professionals of Punjab Province of Pakistan. J. Infect. Dev. Ctries. 2020, 14, 707–712. [Google Scholar] [CrossRef]
- Mohammed Basheeruddin Asdaq, S.; Alshrari, A.S.; Imran, M.; Sreeharsha, N.; Sultana, R. Knowledge, attitude and practices of healthcare professionals of Riyadh, Saudi Arabia towards covid-19: A cross-sectional study. Saudi J. Biol. Sci. 2021, 28, 5275–5282. [Google Scholar] [CrossRef]
- Yi, Z.M.; Song, Z.W.; Li, X.Y.; Hu, Y.; Cheng, Y.C.; Wang, G.R.; Zhao, R.S. The Implementation of a FIP Guidance for COVID-19: Insights from a Nationwide Survey. Ann. Transl. Med. 2021, 9, 1479. [Google Scholar] [CrossRef]
- Tsiga-Ahmed, F.I.; Amole, T.G.; Musa, B.M.; Nalado, A.M.; Agoyi, O.B.; Galadanci, H.S.; Salihu, H.M. COVID 19: Evaluating the Knowledge, Attitude and Preventive Practices of Healthcare Workers in Northern Nigeria. Int. J. Matern. Child Health AIDS 2021, 10, 88–97. [Google Scholar] [CrossRef]
- Kambayashi, D.; Manabe, T.; Kawade, Y.; Hirohara, M. Knowledge, Attitudes, and Practices regarding COVID-19 among Pharmacists Partnering with Community Residents: A National Survey in Japan. PLoS ONE 2021, 16, e0258805. [Google Scholar] [CrossRef]
- Hussain, I.; Majeed, A.; Saeed, H.; Hashmi, F.K.; Imran, I.; Akbar, M.; Chaudhry, M.O.; Rasool, M.F. A National Study to Assess Pharmacists’ Preparedness against COVID-19 during Its Rapid Rise Period in Pakistan. PLoS ONE 2020, 15, e0241467. [Google Scholar] [CrossRef]
- Tesfaye, Z.T.; Yismaw, M.B.; Negash, Z.; Ayele, A.G. COVID-19-related Knowledge, Attitude and Practice among Hospital and Community Pharmacists in Addis Ababa, Ethiopia. Integr. Pharm. Res. Pract. 2020, 9, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Karasneh, R.; Al-Azzam, S.; Muflih, S.; Soudah, O.; Hawamdeh, S.; Khader, Y. Media’s Effect on Shaping Knowledge, Awareness Risk Perceptions and Communication Practices of Pandemic COVID-19 among Pharmacists. Res. Soc. Adm. Pharm. 2021, 17, 1897–1902. [Google Scholar] [CrossRef] [PubMed]
- Kaliyaperumal, K. Guideline for Conducting a Knowledge, Attitude and Practice (KAP) Study. AECS Illum. 2004, 4, 7–9. [Google Scholar] [CrossRef]
- Olum, R.; Chekwech, G.; Wekha, G.; Nassozi, D.R.; Bongomin, F. Coronavirus Disease-2019: Knowledge, Attitude, and Practices of Health Care Workers at Makerere University Teaching Hospitals, Uganda. Front. Public Health 2020, 8, 181. [Google Scholar] [CrossRef]
- Le An, P.; Huynh, G.; Nguyen, H.T.N.; Pham, B.D.U.; Nguyen, T.V.; Tran, T.T.T.; Tran, T.D. Knowledge, Attitude, and Practice towards COVID-19 among Healthcare Students in Vietnam. Infect. Drug Resist. 2021, 14, 3405–3413. [Google Scholar] [CrossRef]
- Desalegn, Z.; Deyessa, N.; Teka, B.; Shiferaw, W.; Hailemariam, D.; Addissie, A.; Abagero, A.; Kaba, M.; Abebe, W.; Nega, B.; et al. COVID-19 and the Public Response: Knowledge, Attitude and Practice of the Public in Mitigating the Pandemic in Addis Ababa, Ethiopia. PLoS ONE 2021, 16, e0244780. [Google Scholar] [CrossRef]
- Yousaf, M.A.; Noreen, M.; Saleem, T.; Yousaf, I. A Cross-Sectional Survey of Knowledge, Attitude, and Practices (KAP) Toward Pandemic COVID-19 among the General Population of Jammu and Kashmir, India. Soc. Work Public Health 2020, 35, 569–578. [Google Scholar] [CrossRef]
- Malik, U.R.; Atif, N.; Hashmi, F.K.; Saleem, F.; Saeed, H.; Islam, M.; Jiang, M.; Zhao, M.; Yang, C.; Fang, Y. Knowledge, Attitude, and Practices of Healthcare Professionals on COVID-19 and Risk Assessment to Prevent the Epidemic Spread: A Multicenter Cross-Sectional Study from Punjab, Pakistan. Int. J. Environ. Res. Public Health 2020, 17, 6395. [Google Scholar] [CrossRef]
- Mahanta, P.; Deka, H.; Sarma, B.; Konwar, R.; Thakuria, K.D.; Kalita, D.; Singh, S.G.; Eshori, L. Knowledge, Attitude, Practice and Preparedness toward COVID-19 Pandemic among Healthcare Workers in Designated COVID Hospitals of a North-Eastern State of India. Hosp. Top. 2021, 1–10. [Google Scholar] [CrossRef]
- Limbu, D.K.; Piryani, R.M.; Sunny, A.K. Healthcare Workers’ Knowledge, Attitude and Practices during the COVID-19 Pandemic Response in a Tertiary Care Hospital of Nepal. PLoS ONE 2020, 15, e0242126. [Google Scholar] [CrossRef]
- Qutob, N.; Awartani, F. Knowledge, Attitudes and Practices (KAP) towards COVID-19 among Palestinians during the COVID-19 Outbreak: A Cross-Sectional Survey. PLoS ONE 2021, 16, e0244925. [Google Scholar] [CrossRef]
- Zhong, B.L.; Luo, W.; Li, H.M.; Zhang, Q.Q.; Liu, X.G.; Li, W.T.; Li, Y. Knowledge, Attitudes, and Practices towards COVID-19 among Chinese Residents during the Rapid Rise Period of the COVID-19 Outbreak: A Quick Online Cross-Sectional Survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Bjorvatn, B.; Chung, F.; Holzinger, B.; Partinen, M.; Penzel, T.; Ivers, H.; Wing, Y.K.; Chan, N.Y.; Merikanto, I.; et al. Insomnia, Anxiety, and Depression during the COVID-19 Pandemic: An International Collaborative Study. Sleep Med. 2021, 87, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Albahri, A.H.; Alnaqbi, S.A.; Alnaqbi, S.A.; Alshaali, A.O.; Shahdoor, S.M. Knowledge, Attitude, and Practice Regarding COVID-19 Among Healthcare Workers in Primary Healthcare Centers in Dubai: A Cross-Sectional Survey. Front. Public Health 2021, 9, 617679. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Lozada, O.; Galvez, C.A.; Castro-Alzate, E.; Bonilla-Asalde, C.A. Factors Associated with Knowledge, Attitudes and Preventive Practices towards COVID-19 in Health Care Professionals in Lima, Peru. F1000Research 2021, 10, 582. [Google Scholar] [CrossRef]
- Noreen, K.; Rubab, Z.E.; Umar, M.; Rehman, R.; Baig, M.; Baig, F. Knowledge, Attitudes, and Practices against the Growing Threat of COVID-19 among Medical Students of Pakistan. PLoS ONE 2020, 15, e0243696. [Google Scholar] [CrossRef]
- Hesaraki, M.; Akbarizadeh, M.; Ahmadidarrehsima, S.; Moghadam, M.P.; Izadpanah, F. Knowledge, Attitude, Practice and Clinical Recommendations of Health Care Workers towards COVID-19: A Systematic Review. Rev. Environ. Health 2021, 36, 345–357. [Google Scholar] [CrossRef]

{kind=link}
| Variable | |
|---|---|
| Age (years) | 44.8 ± 11.9 |
| Sex, n (%) | |
| Men | 49 (34.8%) |
| Women | 92 (65.2%) |
| Marital status, n (%) | |
| Married | 97 (68.8%) |
| Unmarried | 44 (31.2%) |
| Academic background, n (%) | |
| 4-year university | 93 (66.0%) |
| 6-year university | 32 (22.7%) |
| Master’s degree/Doctoral degree | 16 (11.3%) |
| Pharmacist career, n (%) | |
| Less than 10 years | 46 (32.6%) |
| 10 years or more and less than 20 years | 39 (27.7%) |
| Over 20 years | 56 (39.7%) |
| Information source of COVID-19, n (%) | |
| Official website and media of the WHO or CDC | 32 (22.7%) |
| Official government website and media | 101 (71.6%) |
| Media such as news (TV, radio, internet, magazines, and newspapers) | 124 (87.9%) |
| Social media (Facebook, Twitter, and Instagram) | 50 (35.5%) |
| Word of mouth from family/friends | 28 (19.9%) |
| Original paper | 12 (8.5%) |
| I don’t remember | 2 (1.4%) |
| Correct Answer | Incorrect Answer | Don’t Know | ||
|---|---|---|---|---|
| K1 | COVID-19 is caused by beta coronavirus. | 59 (41.8%) | 16 (11.3%) | 66 (46.8%) |
| K2 | COVID-19 is transmitted by food intake. | 100 (70.9%) | 24 (17.0%) | 17 (12.1%) |
| K3 | Common clinical symptoms of COVID-19 are fever, dry cough, dyspnea, and malaise. | 128 (90.8%) | 8 (5.7%) | 5 (3.5%) |
| K4 | Sneezing, runny nose, stuffy nose, and headache are less common symptoms of COVID-19. | 36 (25.5%) | 96 (68.1%) | 9 (6.4%) |
| K5 | PCR can be used to diagnose COVID-19. | 126 (89.4%) | 11 (7.8%) | 4 (2.8%) |
| K6 | Washing your hands with soap and water for at least 30 s is effective in preventing COVID-19 infection. | 132 (93.6%) | 6 (4.3%) | 3 (2.1%) |
| K7 | Loss of taste and smell is characteristic of COVID 19 infection. | 129 (91.5%) | 9 (6.4%) | 3 (2.1%) |
| K8 | Symptom-free COVID-19 patients (during the incubation period) do not spread the virus to others. | 136 (96.5%) | 0 (0%) | 5 (3.5%) |
| K9 | COVID-19 infection spreads through the infected person’s respiratory droplets. | 137 (97.2%) | 1 (0.7%) | 3 (2.1%) |
| K10 | The incubation period of coronavirus is 1 to 14 days. | 126 (89.4%) | 8 (5.7%) | 7 (5.0%) |
| K11 | Elderly people, patients with chronic illness, DM, COPD can be severe. | 137 (97.2%) | 0 (0%) | 4 (2.8%) |
| K12 | Shaking hands and avoiding crowded areas and public transport can prevent COVID-19 infection. | 135 (95.7%) | 2 (1.4%) | 4 (2.8%) |
| K13 | Keeping social distance is effective in preventing the spread of COVID-19. | 135 (95.7%) | 1 (0.7%) | 5 (3.5%) |
| K14 | Antibiotics are the first-line drug if COVID-19 infection is suspected or confirmed. | 121 (85.8%) | 8 (5.7%) | 12 (8.5%) |
| K15 | Early response and supportive care are effective in recovering from infection, as there is no effective treatment for COVID-19. | 123 (87.2%) | 8 (5.7%) | 10 (7.1%) |
| K16 | Isolating and treating individuals infected with COVID-19 is an effective way to break the chain of infection. | 138 (97.9%) | 0 (0%) | 3 (2.1%) |
| K17 | Large-scale group activities can spread COVID-19 infection. | 138 (97.9%) | 0 (0%) | 3 (2.1%) |
| Knowledge Score | 14.4 ± 2.5 | |||
| Yes | No | ||
|---|---|---|---|
| A1 | I would like to be vaccinated with COVID-19 (answer “yes” if already vaccinated). | 133 (94.3%) | 8 (5.7%) |
| A2 | I am motivated to be involved in citizens’ vaccination work (such as vaccine filling). | 112 (79.4%) | 29 (20.6%) |
| A3 | I don’t think there is any problem even if vaccination by a pharmacist is approved as in overseas. | 96 (68.1%) | 45 (31.9%) |
| A4 | If vaccination by a pharmacist is approved, I am willing to vaccinate the public. | 90 (63.8%) | 51 (36.2%) |
| A5 | If vaccination by a pharmacist is approved at a dispensing pharmacy like overseas, I think it will be a great advantage for local residents. | 115 (81.6%) | 26 (18.4%) |
| A6 | If vaccination becomes possible at local pharmacies, I think it can contribute to improving the vaccination rate of local residents. | 116 (82.3%) | 25 (17.7%) |
| A7 | I think pharmacists can contribute to vaccination of local residents from the public health and social aspects. | 129 (91.5%) | 12 (8.5%) |
| A8 | In order to popularize antibody testing, I think it’s okay for pharmacists to do antibody testing at pharmacies. | 109 (77.3%) | 32 (22.7%) |
| A9 | I think that vaccination can prevent the spread of COVID-19. | 133 (94.3%) | 8 (5.7%) |
| A10 | Ultimately, I think we can completely control the infection of COVID-19. | 45 (31.9%) | 96 (68.1%) |
| A11 | I think healthcare professionals need to be aware of all information regarding COVID-19. | 122 (86.5%) | 19 (13.5%) |
| A12 | I think all information related to COVID-19 needs to be shared with other healthcare professionals. | 136 (96.5%) | 5 (3.5%) |
| A13 | I think the spread of COVID-19 can be prevented by taking the precautionary measures indicated by WHO and the government. | 97 (68.8%) | 44 (31.2%) |
| A14 | I think it is necessary to use gowns, gloves, masks, and face shields when dealing with patients with COVID-19. | 117 (83.0%) | 24 (17.0%) |
| A15 | I think it is the pharmacist’s social mission to work together to curb the spread of COVID-19 infection. | 138 (97.9%) | 3 (2.1%) |
| A16 | I understand that this infection is very infectious. | 138 (97.9%) | 3 (2.1%) |
| Attitude score | 13.0 ± 2.6 | ||
| Yes | No | ||
|---|---|---|---|
| P1 | I have attended workshop for COVID-19 infection prevention. | 76 (53.9%) | 65 (46.1%) |
| P2 | I keep a social distance with others to prevent infection. | 138 (97.9%) | 3 (2.1%) |
| P3 | When I touch the front door, which is touched by an unspecified number of people, I open and close it while being careful of infection. | 120 (85.1%) | 21 (14.9%) |
| P4 | I wash my hands with soap routinely. | 138 (97.9%) | 3 (2.1%) |
| P5 | I avoid crowds as much as possible. | 129 (91.5%) | 12 (8.5%) |
| P6 | I avoid meeting friends and relatives. | 125 (88.7%) | 16 (11.3%) |
| P7 | I try not to touch my eyes, nose, and mouth as much as possible. | 124 (87.9%) | 17 (12.1%) |
| P8 | When dealing with the belongings of a patient suspected of having a corona infection, I take care to prevent infection. | 136 (96.5%) | 5 (3.5%) |
| P9 | I try not to take the elevator as much as possible. | 58 (41.1%) | 83 (58.9%) |
| P10 | When I sneeze or cough, I cover my nose and mouth with a tissue or handkerchief. | 137 (97.2%) | 4 (2.8%) |
| P11 | To prevent infection, I always try to throw used tissue in the trash. | 138 (97.9%) | 3 (2.1%) |
| Practice score | 9.4 ± 1.4 | ||
| Correlation (r) | p Value | |
|---|---|---|
| Knowledge and Attitude | 0.44 | <0.001 |
| Knowledge and Practice | 0.21 | 0.01 |
| Attitude and Practice | 0.32 | <0.001 |
| Characteristics | Category | Good Knowledge | Good Attitude | Good Practice | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | ||
| Age | 20–29 years | 1 | 1 | 1 | ||||||
| 30–39 years | 6.3 | 1.58–25.08 | 0.009 | 1.11 | 0.34–3.64 | 0.859 | 2.49 | 0.64–9.70 | 0.188 | |
| 40–49 years | 11.1 | 2.52–48.84 | 0.001 | 1.75 | 0.54–5.67 | 0.351 | 1.85 | 0.53–6.38 | 0.332 | |
| 50–59 years | 3.75 | 1.06–13.31 | 0.041 | 1.06 | 0.32–3.48 | 0.923 | 1.33 | 0.38–4.67 | 0.659 | |
| 60 over | 16.2 | 1.78–147.06 | 0.013 | 1.00 | 0.27–3.74 | 1.000 | 2.46 | 0.51–11.80 | 0.260 | |
| Sex | Men | 0.52 | 0.21–1.28 | 0.154 | 1.00 | 0.48–2.09 | 0.996 | 0.53 | 0.23–1.20 | 0.126 |
| Women | 1 | 1 | 1 | |||||||
| Marital Status | Married | 2.93 | 1.18–7.31 | 0.021 | 0.42 | 0.18–0.97 | 0.041 | 1.97 | 0.86–4.54 | 0.110 |
| Unmarried | 1 | 1 | 1 | |||||||
| Academic background | 4-year university | 1 | 1 | 1 | ||||||
| 6-year university | 0.30 | 0.11–0.78 | 0.014 | 0.70 | 0.30–1.59 | 0.391 | 1.04 | 0.40–2.74 | 0.934 | |
| Master’s degree/Doctoral degree | 0.94 | 0.19–4.70 | 0.939 | 2.06 | 0.55–7.79 | 0.285 | 2.04 | 0.43–9.71 | 0.370 | |
| Pharmacist career | Less than 10 years | 1 | 1 | 1 | ||||||
| 10 years or more and less than 20 years | 1.22 | 0.43–3.41 | 0.708 | 2.27 | 0.85–6.06 | 0.101 | 1.73 | 0.57–5.21 | 0.331 | |
| Over 20 years | 4.09 | 1.20–13.87 | 0.024 | 0.98 | 0.44–2.19 | 0.955 | 1.04 | 0.41–2.60 | 0.934 | |
| Source of information on COVID-19 | Official website and media of the WHO or CDC | 1.48 | 0.46–4.71 | 0.509 | 1.99 | 0.79–5.02 | 0.145 | 2.19 | 0.70–6.83 | 0.176 |
| Official government website and media | 1.8 | 0.71–4.58 | 0.215 | 2.48 | 1.16–5.31 | 0.019 | 1.35 | 0.57–3.21 | 0.498 | |
| Media such as news (TV, radio, internet, magazines, and newspapers) | 1.11 | 0.29–4.24 | 0.874 | 0.4 | 0.11–1.48 | 0.172 | 0.77 | 0.21–2.88 | 0.697 | |
| Social media (Facebook, Twitter, and Instagram) | 1.04 | 0.41–2.65 | 0.941 | 1.05 | 0.50–2.19 | 0.907 | 1.13 | 0.48–2.64 | 0.784 | |
| Word of mouth from family/friends | 0.65 | 0.23–1.84 | 0.416 | 0.4 | 0.17–0.92 | 0.032 | 0.48 | 0.19–1.21 | 0.121 | |
| Original paper | 0.35 | 0.09–1.26 | 0.108 | 0.97 | 0.28–3.39 | 0.956 | 1.39 | 0.29–6.70 | 0.684 | |
| Characteristics | Category | Good Knowledge | Good Attitude | ||||
|---|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p Value | Adjusted OR | 95% CI | p Value | ||
| Age | 20–29 years | 1 | |||||
| 30–39 years | 6.3 | 1.58–25.08 | 0.009 | ||||
| 40–49 years | 11.1 | 2.52–48.84 | 0.001 | ||||
| 50–59 years | 3.75 | 1.06–13.31 | 0.041 | ||||
| 60 over | 16.2 | 1.78–147.06 | 0.013 | ||||
| Sex | Men | ||||||
| Women | |||||||
| Marital Status | Married | 0.37 | 0.15–0.90 | 0.029 | |||
| Unmarried | 1 | ||||||
| Academic background | 4-year university | ||||||
| 6-year university | |||||||
| Master’s degree/Doctoral degree | |||||||
| Pharmacist career | Less than 10 years | ||||||
| 10 years or more and less than 20 years | |||||||
| Over 20 years | |||||||
| Source of information on COVID-19 | Official website and media of the WHO or CDC | ||||||
| Official government website and media | 2.81 | 1.26–6.26 | 0.012 | ||||
| Media such as news (TV, radio, internet, magazines, and newspapers) | |||||||
| Social media (Facebook, Twitter, and Instagram) | |||||||
| Word of mouth from family/friends | 0.38 | 0.16–0.91 | 0.030 | ||||
| Original paper | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wakui, N.; Kikuchi, M.; Ebizuka, R.; Yanagiya, T.; Togawa, C.; Matsuoka, R.; Ikarashi, N.; Yamamura, M.; Shirozu, S.; Machida, Y.; et al. Survey of Pharmacists’ Knowledge, Attitudes, and Practices (KAP) concerning COVID-19 Infection Control after Being Involved in Vaccine Preparation: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 9035. https://doi.org/10.3390/ijerph19159035
Wakui N, Kikuchi M, Ebizuka R, Yanagiya T, Togawa C, Matsuoka R, Ikarashi N, Yamamura M, Shirozu S, Machida Y, et al. Survey of Pharmacists’ Knowledge, Attitudes, and Practices (KAP) concerning COVID-19 Infection Control after Being Involved in Vaccine Preparation: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9035. https://doi.org/10.3390/ijerph19159035
Chicago/Turabian StyleWakui, Nobuyuki, Mayumi Kikuchi, Risa Ebizuka, Takahiro Yanagiya, Chikako Togawa, Raini Matsuoka, Nobutomo Ikarashi, Miho Yamamura, Shunsuke Shirozu, Yoshiaki Machida, and et al. 2022. "Survey of Pharmacists’ Knowledge, Attitudes, and Practices (KAP) concerning COVID-19 Infection Control after Being Involved in Vaccine Preparation: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 15: 9035. https://doi.org/10.3390/ijerph19159035
APA StyleWakui, N., Kikuchi, M., Ebizuka, R., Yanagiya, T., Togawa, C., Matsuoka, R., Ikarashi, N., Yamamura, M., Shirozu, S., Machida, Y., Suzuki, K., & Kato, H. (2022). Survey of Pharmacists’ Knowledge, Attitudes, and Practices (KAP) concerning COVID-19 Infection Control after Being Involved in Vaccine Preparation: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(15), 9035. https://doi.org/10.3390/ijerph19159035