
“Truly Listen to Us”: Recommendations for Health Professionals to Bolster Wellbeing of Nonbinary Individuals


Abstract
:1. Introduction
1.1. Trans and Nonbinary Healthcare
1.2. Cisnormativity and Erasure in Healthcare
1.3. Gender-Affirming Healthcare
1.4. Nonbinary Access to Healthcare
1.5. Significance of the Study
2. Materials and Methods
2.1. Participatory Action Research
2.2. PhotoVoice
Virtual Adaptation
2.3. Recruitment and Sampling
2.4. Data Collection and Analysis
- What emerging themes do you hear as we have discussed these priorities for change to promote wellbeing in our lives and the lives of our communities?
- How would you recommend the information about wellbeing (e.g., promotive and corrosive factors) applied to practice with nonbinary communities to bolster wellbeing?
- How would you recommend the information about wellbeing (e.g., promotive and corrosive factors) applied to policy with nonbinary communities to bolster wellbeing?
3. Results
3.1. Sample
3.2. Healthcare Experiences
So this one can be kind-of triggery…I’ve had really bad experiences particularly with gynecological health…my hormones are not standard…I tend to run low on estrogen, high on testosterone…[providers] try hormone therapies and they try this and they try that and “oh, we don’t understand why that’s painful and like”—or “that’s just how it is for some women, you should, you know”.
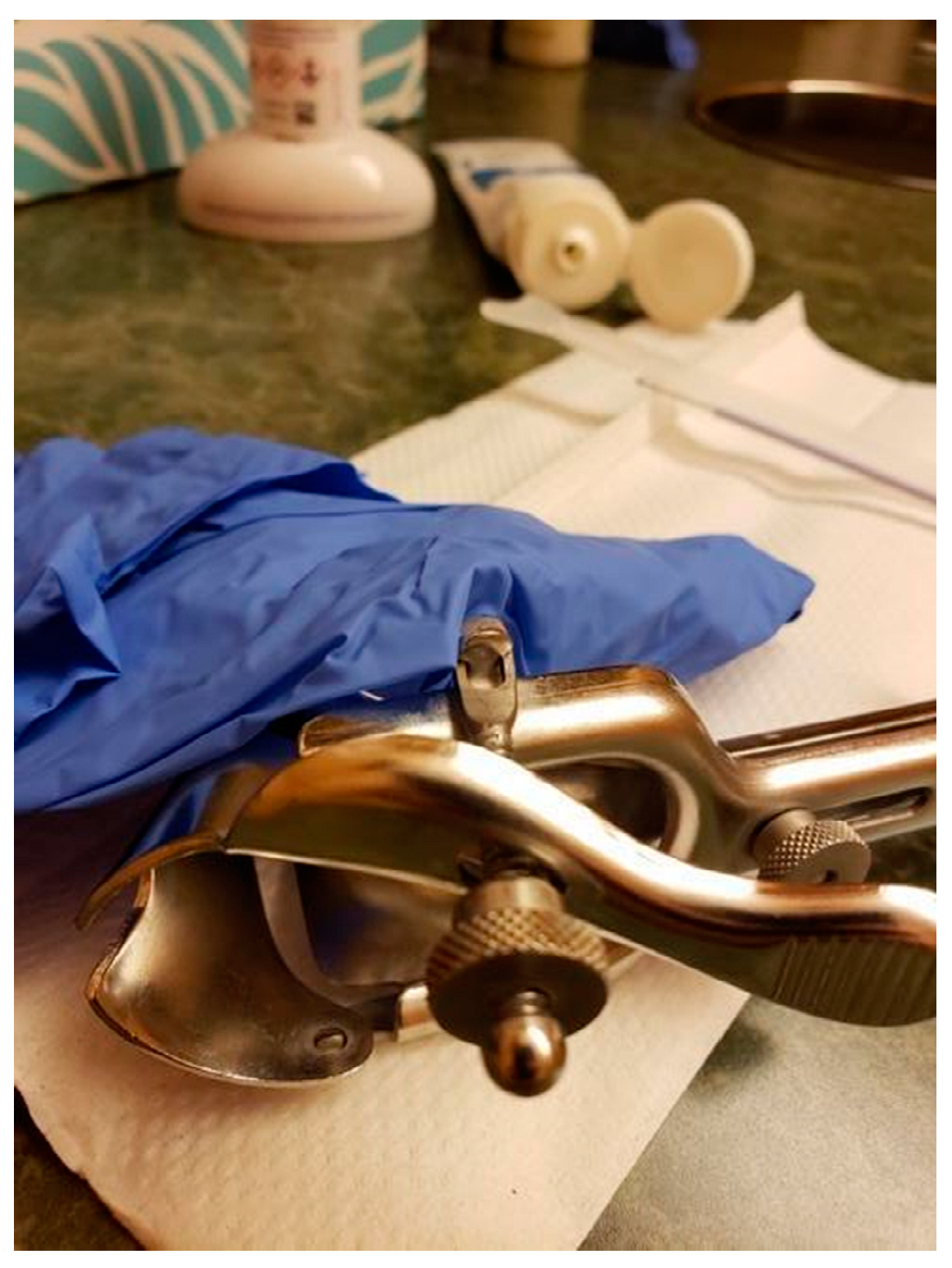
Contrasted with my current situation where I have a very affirming gynecological practice and a doctor I trust and they make every effort every time I go in to make me as comfortable and [be] as affirming as possible. They’re willing to talk to me about the fact that I have female partners, they’re willing to talk to me about the fact that I’m poly [Polyamorous, which is a relationship structure characterized by multiple consenting romantic and/or sexual relationships]. They’re willing to talk to me about consent-based STD [sexually transmitted diseases] and STI [sexually transmitted infections] testing and they’ve never shamed me for it…When I started seeing her there was some education. She asked questions and she listened, and so when she asked for resources, she’s like “oh, do you have anybody you would recommend reading?” And I gave her a couple of books. Six months later when I went in for another checkup, she had read them and she’d looked at them and remembered. Now when I go in, like it’s in my file and people in the practice know and continue to affirm [me]. At one point they changed their intake forms and they’re like “Will you look at our new intake forms and see if you would add anything and they added a line for, you know, your legal name? And then they added “what would you like us to call you in the office” as a line. They added multiple genders and were welcoming people to define for themselves. It makes me so much more appreciative of having a medical care provider who is compassionate and who is dedicated to at least educating themselves…above and beyond just being affirming, they’re being proactive and that’s been a game changer. (HG) (see Figure 1)
I really need queer and trans people to just listen to me, say that it sucks being limited because of my fatness without telling me that being skinny is hard, too. I’ve been really moving away from body positivity narratives in spaces recently and more towards fat liberation politics because I think that body positivity feels nice and inclusive, [but] it never actually does anything for me—I just feel more shitty about myself because I can’t make myself love my body. But I think that a fat liberation channels anger better. Like why is it that fatness precludes people from practicing medical transition—that’s actually completely arbitrary. The way that fat phobia and transphobia combine in medical settings has caused real serious problems for me that aren’t always even just about transition care, but that are just about trying to get regular healthcare from a doctor as a fat trans person is not possible…and so yeah…I need people to get on board with fat liberation.
The surgeon’s office technically has a BMI [body mass index] restriction and so I’m chubby…I’m nervous because the clinic didn’t tell me anything and I’m assuming that they would think I’m fine or would have told me if I’m not fine so I’m in this weird—“am I gonna be fat-shamed by the medical field today?”
3.3. Accessing Healthcare
I switched my ob/gyn to the trans clinic because—well, the one that I had was very…you know, “you’re a girl and you want to have kids” and I’m like I’m just here to check off the box and be done. I’m feeling really dysphoric and uncomfortable with you rather than recognized for my gender and that type of thing…It is frustrating, but it’s also definitely invalidating because you have to sit through a very uncomfortable situation anyway because nobody really wants to be at the doctor and misgendered. It’s like I’m already not feeling well, you have to kick me while I’m down, too?
In the Midwest where transgender clinics are not as common or Planned Parenthood [a common provider of gender-affirming OBGYN and hormone care] is being defunded, that type of thing and so having spaces for us to get healthcare without having to revert back to our assigned gender or having to explain to your doctor.
3.4. Recommendations for Healthcare Providers
3.5. Recommendations for Improving Interpersonal Care
I want to just navigate the world as me and be seen for me and no automatic assumptions based on my voice or my breasts or my body shape or anything like that—it really is just a blank slate in some way of just being able to then show the world who I am.
The difference in the internal reality and how then I interact differently with the world because I can interact from a place of sovereignty and power and self-assurance—I like who I am and I like how I interact with people better…much more comfortable with boundaries and like “these are for my wellbeing, please don’t cross them”.
I think that a lot of times when someone says “ok, I need to learn about how to be better to queer people”—they just Google it and are just like “what is queer?” Ok, “what is they/them?” So we have this very sanitized way of learning…but I think it’s so much important to listen to individual people—their voices and their experiences and to find that shared humanity because I think when you find that shared humanity—that puts you in a place where you really do feel in your heart that you want to help ensure that our wellbeing is good.
3.5.1. Recommendations for Increasing Access to Gender-Affirming Care
I am one of the trans people with dysphoria, but I also don’t believe you have to have dysphoria to be trans and I will fight anybody who says otherwise…I don’t think we should be forcing…diagnosis…we shouldn’t be forcing mental health problems on people because they happen to have their own sort of gender dysphoria or like gender journey. (Jynx)
The fact that [access to gender-affirming resources] is becoming so normalized is great and the fact that I get to have all of these tools is really incredible…[as] more people are able to get things they need to be more themselves…I can only imagine how much happier people [will be] because of that—I know I am. (Kai) (see Figure 6)
I’d recommend that more LGBTQ+ and non-LGBTQ+ groups work to increase the representation of non-binary perspectives in the services and resources they provide. For instance, a mental-health-focused non-profit or resource center could actively solicit the insights of non-binary people to better provide resources to that community.
3.5.2. Recommendations for Advocating for Environmental and Policy Changes
[I]nclusive policy that creates wider access to affirming healthcare. Medicare for all is a great step, but we also need to go further and create policies that help healthcare to be more affirming and understanding of the unique issues that we face.
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lykens, J.E.; LeBlanc, A.J.; Bockting, W.O. Healthcare experiences amongyoung adults who identify as genderqueer or nonbinary. LGBT Health 2018, 5, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Markman, E.R. Gender identity disorder, the gender binary, and transgender oppression: Implications for ethical social work. Smith Coll. Stud. Soc. Work. 2011, 81, 314–327. [Google Scholar] [CrossRef]
- Stroumsa, D. The state of transgender health care: Policy, law, and medical frameworks. Am. J. Public Health 2014, 104, e31–e38. Available online: http://proxy195.nclive.org/login?url=https://search.proquest.com/docview/1508767081?accountid=14968 (accessed on 24 February 2020). [CrossRef]
- Kinney, M.K. Learning to Thrive in a Binary World: Understanding the Gendered Experiences of Nonbinary Individuals and Ways to Bolster Wellbeing. Publication No. 28647919. Ph.D. Thsies, Indiana University, Bloomington, IN, USA, 2021. [Google Scholar]
- Riggle, E.D.; Rostosky, S.S. A Positive View of LGBTQ: Embracing Identity and Cultivating Well-Being; Rowman & Littlefield Publishers: Lanham, MD, USA, 2012. [Google Scholar]
- Matsuno, E.; Budge, S.L. Non-binary/genderqueer identities: A critical review of the literature. Curr. Sex. Health Rep. 2017, 9, 116–120. [Google Scholar] [CrossRef]
- Moradi, B.; Tebbe, E.A.; Brewster, M.E.; Budge, S.L.; Lenzen, A.; Ege, E.; Schuch, E.; Arango, S.; Angelone, N.; Mender, E.; et al. A Content Analysis of Literature on Trans People and Issues. Couns. Psychol. 2016, 47, 960–995. [Google Scholar] [CrossRef]
- Cosgrove, D.; Bozlak, C.; Reid, P. Service barriers for gender nonbinary young adults: Using photovoice to understand support and stigma. Affilia 2021, 36, 220–239. [Google Scholar] [CrossRef]
- Cosgrove, D. “I am allowed to be myself”: A photovoice exploration of non-binary identity development and meaning-making. J. Gay Lesbian Soc. Serv. 2021, 33, 78–102. [Google Scholar] [CrossRef]
- Moradi, B.; Mohr, J.J.; Worthington, R.L.; Fassinger, R.E. Counseling psychology research on sexual (orientation) minority issues: Conceptual and methodological challenges and opportunities. J. Couns. Psychol. 2009, 56, 5–22. [Google Scholar] [CrossRef]
- Vincent, B.W. Non-Binary Gender Identity Negotiations: Interactions with Queer Communities and Medical Practice. Ph.D. Thesis, University of Leeds, Leeds, UK, 2016. F4399122A9BDE589. [Google Scholar]
- James, S.E.; Herman, J.L.; Rankin, S.; Keisling, M.; Mottet, L.; Anafi, M. The Report of the 2015 U.S. Transgender Survey; National Center for Transgender Equality: Washington, DC, USA, 2016. [Google Scholar]
- Budge, S.L.; Rossman, H.K.; Howard, K.A. Coping and psychological distress among genderqueer individuals: The moderating effect of social support. J. LGBT Issues Couns. 2014, 8, 95–117. [Google Scholar] [CrossRef]
- Harrison, J.; Grant, J.; Herman, J.L. A gender not listed here: Genderqueers, gender rebels, and otherwise in the national transgender discrimination survey. LGBTQ Policy J. Harv. Kennedy Sch. 2012, 2, 13–24. [Google Scholar]
- Kcomt, L. Profound health-care discrimination experienced by transgender people: Rapid systematic review. Soc. Work. Health Care 2019, 58, 201–219. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.M.; Mottet, L.A.; Tanis, J.; Harrison, J.; Herman, J.L.; Keisling, M. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey; National Center for Transgender Equality and the National Gay and Lesbian Task Force: Washington, DC, USA, 2011. [Google Scholar]
- Giblon, R.; Bauer, G.R. Health care availability, quality, and unmet need: A comparison of transgender and cisgender residents of Ontario, Canada. BMC Health Serv. Res. 2017, 17, 283–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, A.; Agardh, A.; Asamoah, B.O. Self-reported discrimination in healthcare settings based on recognizability as transgender: A cross-sectional study among U.S. citizens. Arch. Sex. Behav. 2017, 47, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Stotzer, R.L.; Silverschanz, P.; Wilson, A. Gender identity and social services: Barriers to care. J. Soc. Serv. Res. 2013, 39, 63–77. [Google Scholar] [CrossRef]
- Frohard-Dourlent, H.; Dobson, S.; Clark, B.A.; Doull, M.; Saewyc, E.M. ‘I would have preferred more options’: Accounting for non-binary youth in health research. Nurs. Inq. 2017, 24, e12150. [Google Scholar] [CrossRef]
- Kinney, M.K.; Meininger, E.T.; Wiener, S.E. Transgender and nonbinary youth and access to medical care. In Social Work and Health Care Practice with Transgender and Nonbinary Individuals and Communities: Voices for Equity, Inclusion, and Resilience; Kattari, S.K., Kinney, M.K., Kattari, L., Walls, N.E., Eds.; Taylor and Francis: Oxfordshire, UK, 2021; pp. 29–41. [Google Scholar]
- Lacombe-Duncan, A.; Kattari, S.K.; Kattari, L. Transgender and nonbinary adults and access to medical care. In Social Work and Health Care Practice with Transgender and Nonbinary Individuals and Communities: Voices for Equity, Inclusion, and Resilience; Kattari, S.K., Kinney, M.K., Kattari, L., Walls, N.E., Eds.; Taylor and Francis: Oxfordshire, UK, 2021; pp. 42–56. [Google Scholar]
- Namaste, V. Invisible Lives: The Erasure of Transsexual and Transgendered People; University of Chicago Press: Chicago, IL, USA, 2000. [Google Scholar]
- Bauer, G.R.; Hammond, R.; Travers, R.; Kaay, M.; Hohenadel, K.M.; Boyce, M. I don’t think this is theoretical; this is our lives”: How erasure impacts health care for transgender people. J. Assoc. Nurses AIDS Care 2009, 20, 348–361. [Google Scholar] [CrossRef]
- Collazo, A.; Austin, A.; Craig, S.L. Facilitating transition among transgender clients: Components of effective clinical practice. Clin. Soc. Work. J. 2013, 41, 228–237. [Google Scholar] [CrossRef]
- Bradford, J.; Reisner, S.L.; Honnold, J.A.; Xavier, J. Experiences of transgender-related discrimination and implications for health: Results from the Virginia Transgender Health Initiative Study. Am. J. Public Health 2013, 103, 1820–1829. [Google Scholar] [CrossRef]
- Pitts, M.K.; Couch, C.; Mulcare, H.; Croy, S.; Mitchell, A. Transgender people in Australia and New Zealand: Health, well-being and access to health services. Fem. Psychol. 2009, 19, 475–495. [Google Scholar] [CrossRef]
- Gridley, S.J.; Crouch, J.M.; Evans, Y.; Eng, W.; Antoon, E.; Lyapustina, M.; Schimmel-Bristow, A.; Woodward, J.; Dundon, K.; Schaff, R.; et al. Youth and caregiver perspectives on barriers to gender-affirming health care for transgender youth. J. Adolesc. Health 2016, 59, 254–261. [Google Scholar] [CrossRef] [Green Version]
- Kattari, S.K.; Atteberry-Ash, B.; Kinney, M.K.; Walls, N.E.; Kattari, L. One size does not fit all: Differential transgender health experiences by gender identity and sexual orientation. Soc. Work. Health Care 2019, 58. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, E. Enhancing transgender health care. Am. J. Public Health 2001, 91, 869–872. [Google Scholar] [PubMed] [Green Version]
- Cruz, T.M. Assessing access to care for transgender and gender nonconforming people: A consideration of diversity in combating discrimination. Soc. Sci. Med. 2014, 110, 65–73. [Google Scholar] [CrossRef]
- Lewis, J. Resilience among Transgender Adults Who Identify as Genderqueer: Implications for Health and Mental Health Treatment. Doctoral Dissertation, ProQuest Information & Learning, Ann Arbor, MI, USA, 2008. [Google Scholar]
- Macapagal, K.; Bhatia, R.; Greene, G.J. Differences in healthcare access, use, and experiences within a community sample of racially diverse lesbian, gay, bisexual, transgender, and questioning emerging adults. LGBT Health 2016, 3, 434–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reisner, S.L.; Hughto, J.M. Comparing the health of non-binary and binary transgender adults in a statewide non-probability sample. PLoS ONE 2019, 14, e0221583. [Google Scholar] [CrossRef]
- Coleman, E.; Bockting, W.; Botzer, M.; Cohen-Kettenis, P.; DeCuypere, G.; Feldman, J.; Fraser, L.; Green, J.; Knudson, G.; Meyer, W.J.; et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. Int. J. Transgenderism 2012, 13, 165–232. [Google Scholar] [CrossRef]
- Hidalgo, M.A.; Ehrensaft, D.; Tishelman, A.C.; Clark, L.F.; Garofalo, R.; Rosenthal, S.M.; Spack, N.P.; Olson, J. The Gender Affirmative Model: What we know and what we aim to learn. Hum. Dev. 2013, 56, 285–290. [Google Scholar] [CrossRef]
- Keo-Meier, C.; Ehrensaft, D. (Eds.) The Gender Affirmative Model: A New Approach to Supporting Gender Diverse and Transgender Children; American Psychological Association: Washington, DC, USA, 2018. [Google Scholar]
- Rider, G.N.; Vencill, J.A.; Berg, D.R.; Becker-Warner, R.; Candelario-Pérez, L.; Spencer, K.G. The gender affirmative lifespan approach (GALA): A framework for competent clinical care with nonbinary clients. Int. J. Transgenderism 2019, 20, 275–288. [Google Scholar] [CrossRef]
- Yelland, A. Chest surgeries. In Genderqueer and Non-Binary Genders; Richards, C., Bouman, W.P., Barker, M.J., Eds.; Palgrave Macmillan: London, UK, 2017; pp. 225–245. [Google Scholar]
- Unicare. Sex Reassignment Surgery: CG-SURG-27 Revised. Available online: https://www.unicare.com/medicalpolicies/guidelines/gl_pw_a051166.htm (accessed on 16 February 2017).
- Unicare. Sex Reassignment Surgery: CG-SURG-27 Revised. Available online: https://www.unicare.com/medicalpolicies/guidelines/gl_pw_a051166.htm (accessed on 25 April 2018).
- APA. APA Task Force on Gender Identity and Gender Variance; APA: Washington, DC, USA, 2008. [Google Scholar]
- Kemmis, S.; McTaggart, R. Critical Participatory Action Research; The SAGE: London, UK, 2014. [Google Scholar]
- Lawson, H.A.; Caringi, J.; Pyles, L.; Bozlak, C.; Jurkowski, J. Participatory Action Research; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Walter, M. Participatory Action Research. Social Research Methods. In Social Research Methods; Bryman, A., Ed.; The Falmer Press: London, UK, 2009; pp. 151–158. [Google Scholar]
- Cordeiro, L.; Soares, C.B.; Rittenmeyer, L. Unscrambling method and methodology in action research traditions: Theoretical conceptualization of praxis and emancipation. Qual. Res. 2016, 17, 395–407. [Google Scholar] [CrossRef]
- Kramer, C.S.; Cosgrove, D.; Mountz, S.; Lee, E. Finding a place for my research to belong: Experiences of early-career social work participatory action researchers in neoliberal academia. Crit. Radic. Soc. Work. 2021, 9, 269–287. [Google Scholar] [CrossRef]
- Lewin, K. Action research and minority problems. In Resolving Social Conflicts; Lewin, G.W., Ed.; Harper & Row: New York, NY, USA, 1946. [Google Scholar]
- Freire, P. Pedagogy of the Oppressed; Herder & Herder: Freiburg, Germany, 1970. [Google Scholar]
- Freire, P. Education for Critical Consciousness; The Seabury Press: New York, NY, USA, 1973. [Google Scholar]
- Hall, B.L. Participatory research, popular knowledge and power: A personal reflection. Convergence 1981, 14, 6–17. [Google Scholar]
- Park, P. What is participatory research? A theoretical and methodological perspective. In Voices of Change: Participatory Research in the United States and Canada; Praeger: Westport, CT, USA, 1993; pp. 1–19. [Google Scholar]
- Brown, P.A. Participatory research: A new paradigm for social work. In Education and Research for Empowerment Practice; Gutiérrez, L., Nurius, P., Eds.; Center for Policy and Practice Research, School of Social Work, University of Washington: Seattle, WA, USA, 1994; pp. 293–303. [Google Scholar]
- Higley, D. Bending the Binary: Effects of Nonbinary Gender Media Representations on Disposition Formation and Media enjoyment. Master’s Thesis, University of Central Florida, Orlando, FL, USA, 2019. [Google Scholar]
- Wenhold, H.; Harrison, K. Emerging adults and gender norms: Everyday life experiences, media perceptions, attitudes, and future expectations. Gend. Issues 2021, 38, 420–437. [Google Scholar] [CrossRef]
- Cosgrove, D.; Simpson, F.; Dreslinski, S.; Kihm, T. Photovoice as a transformative methodology for nonbinary young adults. J. LGBT Youth 2022. [Google Scholar] [CrossRef]
- Wang, C.C.; Burris, M.A. PhotoVoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, S.E. Bridging activism and the academy: Exposing environmental injustices through the feminist ethnographic method of Photovoice. Hum. Ecol. Rev. 2015, 21, 27–58. [Google Scholar] [CrossRef]
- Maguire, P. Doing participatory research: A feminist approach. Amherst: University of Massachusetts, Center for International Education, School of Education. Research & Practice 1987. Available online: http://scholarworks.umass.edu/cie_participatoryresearchpractice/1 (accessed on 10 May 2021).
- Bender, K.; Barman-Adhikari, A.; DeChants, J.; Haffejee, B.; Anyon, Y.; Begun, S.; Portillo, A.; Dunn, K. Asking for Change: Feasibility, acceptability, and preliminary outcomes of a manualized PhotoVoice intervention with youth experiencing homelessness. Child. Youth Serv. Rev. 2017, 81, 379–389. [Google Scholar] [CrossRef]
- Catalani, C.; Minkler, M. PhotoVoice: A review of the literature in health and public health. Health Educ. Behav. 2010, 37, 424–451. [Google Scholar] [CrossRef]
- Wang, C.C. PhotoVoice: A participatory action research strategy applied to women’s health. J. Women’s Health 1999, 8, 185–192. [Google Scholar] [CrossRef]
- Beh, A.; Bruyere, B.L.; Lolosoli, S. Legitimizing local perspectives in conservation through community based research: A Photovoice study in Samburu, Kenya. Soc. Nat. Resour. 2013, 26, 1390–1406. [Google Scholar] [CrossRef]
- Carlson, E.D.; Engebretson, J.; Chamberlain, R.M. Photovoice as a social process of critical consciousness. Qual. Health Res. 2006, 16, 836–852. [Google Scholar] [CrossRef]
- Capous-Desyllas, M.; Mountz, S. Using Photovoice Methodology to Illuminate the Experiences of LGBTQ Former Foster Youth. Child Youth Serv. 2019, 40, 267–307. [Google Scholar] [CrossRef]
- Bardhoshi, G.; Grieve, K.; Swanston, J.; Suing, M.; Booth, J. Illuminating the On-Campus Experience of LGBTQ Students Through Photovoice. J. Coll. Couns. 2018, 21, 194–209. [Google Scholar] [CrossRef]
- Christensen, M.C.; Capous-Desyllas, M.; Arczynski, A.V. Photovoice as a Multilevel Tool for Gender and Sexual Identity Exploration. Fam. Soc. 2020, 101, 219–231. [Google Scholar] [CrossRef]
- Ingrey, J. Shadows and light: Pursuing gender justice through students’ PhotoVoice projects of the washroom spaces. J. Curric. Theor. 2013, 29, 174–190. [Google Scholar]
- Instructure. 2020. Canvas Security Overview. Available online: https://www.instructure.com/canvas/security (accessed on 12 June 2020).
- Hergenrather, K.C.; Rhodes, S.D.; Cowan, C.A.; Bardhoshi, G.; Pula, S. PhotoVoice as community-based participatory research: A qualitative review. Am. J. Health Behav. 2009, 33, 686–698. [Google Scholar] [CrossRef] [Green Version]
- Houle, J.; ç, S.; Radziszewski, S.; Boileau, G.; Morin, P.; Leloup, X.; Bohémier, H.; Robert, S. Public housing tenants’ perspective on residential environment and positive well-being: An empowerment-based PhotoVoice study and its implications for social work. J. Soc. Work. 2018, 18, 703–731. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory, 2nd ed.; Sage: London, UK, 2014. [Google Scholar]
- Bindman, J.; Ngo, A.; Zamudio-Haas, S.; Sevelius, J. Health Care Experiences of Patients with Nonbinary Gender Identities. Transgender Health 2021. [Google Scholar] [CrossRef]
- Eckstrand, K.L.; Ng, H.; Potter, J. Affirmative and responsible health care for people with nonconforming gender identities and expressions. AMA J. Ethics 2016, 18, 1107–1118. [Google Scholar]
- Hastings, J.; Bobb, C.; Wolfe, M.; Amaro Jimenez, Z.; Amand, C.S. Medical care for nonbinary youth: Individualized gender care beyond a binary framework. Pediatric Ann. 2021, 50, e384–e390. [Google Scholar] [CrossRef]
- Motmans, J.; Nieder, T.O.; Bouman, W.P. Transforming the paradigm of nonbinary transgender health: A field in transition. Int. J. Transgenderism 2009, 20, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Association of American Medical Colleges. Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who Are LGBT, Gender Nonconforming, or Born with DSD: A Resource for Medical Educators. Association of American Medical Colleges. 2014. Available online: https://store.aamc.org/implementing-curricular-and-institutional-climate-changes-to-improve-health-care-for-individuals-who-are-lgbt-gender-nonconforming-or-born-with-dsd-a-resource-for-medical-educators.html (accessed on 25 July 2021).
- Giffort, D.M.; Underman, K. The relationship between medical education and transhealth disparities: A call to research. Sociol. Compass 2016, 10, 999–1013. [Google Scholar] [CrossRef]
- Safer, J.D.; Coleman, E.; Feldman, J.; Gaarofalo, R.; Hembree, W.; Radix, A.; Sevelius, J. Barriers to healthcare for transgender individuals. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 168–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vance, S.R.; Halpern-Felsher, B.L.; Rosenthal, S.M. Health care providers’ comfort with and barriers to care of transgender youth. J. Adolesc. Health 2015, 56, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Bos, H.; de Haas, S.; Kuyper, L. Lesbian, gay, and bisexual adults: Childhood gender nonconformity, childhood trauma, and sexual victimization. J. Interpers. Violence 2016, 34, 496–515. [Google Scholar] [CrossRef]
- Roberts, A.L.; Rosario, M.; Slopen, N.; Calzo, J.P.; Austin, S.B. Childhood gender nonconformity, bullying victimization, and depressive symptoms across adolescence and early adulthood: An 11-year longitudinal study. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Eckstrand, K.L.; Sciolla, A.F.; Potter, J. Trauma and resilience in the lives of people who are or may be LGBT, gender nonconforming, and/or born with DSD: Implications for clinical care and health outcomes. In Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who Are LGBT, Gender Nonconforming, or Born With DSD; Association of American Medical Colleges, Ed.; Association of American Medical Colleges: Washington, DC, USA, 2014; pp. 32–39. [Google Scholar]
- Perrin, P.B.; Sutter, M.E.; Trujillo, M.A.; Henry, R.S.; Pugh, M., Jr. The minority strengths model: Development and initial path analytic validation in racially/ethnically diverse LGBTQ individuals. J. Clin. Psychol. 2020, 76, 118–136. [Google Scholar] [CrossRef]
- Sears, B.; Conron, K.J.; Flores, A.R. The Impact of the Fall 2020 COVID-19 Surge on LGBT Adults in the US; The Williams Institutes: Los Angeles, CA, USA, 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M | sd | |
|---|---|---|
| Age (range: 19–50) | 30.00 | 7.40 |
| f | % | |
| Race | ||
| Multiracial 1 | 1 | 5.9 |
| White | 16 | 94.1 |
| Ethnicity | ||
| Eskinazi | 1 | 5.9 |
| German Irish | 1 | 5.9 |
| Native American | 1 | 5.9 |
| Non-Hispanic | 3 | 17.6 |
| Non-Latinx | 1 | 5.9 |
| White | 5 | 29.4 |
| “White-washed” | 1 | 5.9 |
| Chose not to respond | 4 | 23.5 |
| Current Gender (multiple) | ||
| Agender | 2 | 11.8 |
| Genderfluid | 2 | 11.8 |
| Gender-neutral | 1 | 5.9 |
| Genderqueer | 5 | 29.4 |
| Nonbinary | 12 | 70.6 |
| Transgender | 1 | 5.9 |
| Transmasculine | 2 | 11.8 |
| Pronouns 2 (multiple) | ||
| He/him/his | 3 | 17.6 |
| She/her/hers | 2 | 11.8 |
| They/them/their | 17 | 100.0 |
| Assigned sex at birth 3 | ||
| Assigned female at birth | 10 | 58.8 |
| Assigned male at birth | 1 | 5.9 |
| Intersex | 1 | 5.9 |
| Chose not to respond | 5 | 29.4 |
| Identify as disabled/someone with a disability 4 | 9 | 52.9 |
| Identify as neurodiverse/someone with neurodiversity 5 | 7 | 41.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinney, M.K.; Cosgrove, D. “Truly Listen to Us”: Recommendations for Health Professionals to Bolster Wellbeing of Nonbinary Individuals. Int. J. Environ. Res. Public Health 2022, 19, 9032. https://doi.org/10.3390/ijerph19159032
Kinney MK, Cosgrove D. “Truly Listen to Us”: Recommendations for Health Professionals to Bolster Wellbeing of Nonbinary Individuals. International Journal of Environmental Research and Public Health. 2022; 19(15):9032. https://doi.org/10.3390/ijerph19159032
Chicago/Turabian StyleKinney, M. Killian, and Darren Cosgrove. 2022. "“Truly Listen to Us”: Recommendations for Health Professionals to Bolster Wellbeing of Nonbinary Individuals" International Journal of Environmental Research and Public Health 19, no. 15: 9032. https://doi.org/10.3390/ijerph19159032
APA StyleKinney, M. K., & Cosgrove, D. (2022). “Truly Listen to Us”: Recommendations for Health Professionals to Bolster Wellbeing of Nonbinary Individuals. International Journal of Environmental Research and Public Health, 19(15), 9032. https://doi.org/10.3390/ijerph19159032