
Patient Care via Video Consultations: Piloting and S.W.O.T. Analysis of a Family Medicine Digitally Synchronous Seminar for Medical Students



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Research Objectives
- Telemedicine research level:
- To what extent can telemedicine skills be fostered in students participating in the seminar?
- Family medicine research level:
- 2.
- To what extent can family medicine competencies be promoted among students participating in the seminar?
- Didactic research level:
- 3.
- How is the didactic concept of the teaching project assessed by the participating students?
- 4.
- What are the strengths and weaknesses of the learning concept according to the participating students and teachers?
- 5.
- What are the opportunities and risks for the future?
2.2. Participants of the Seminar
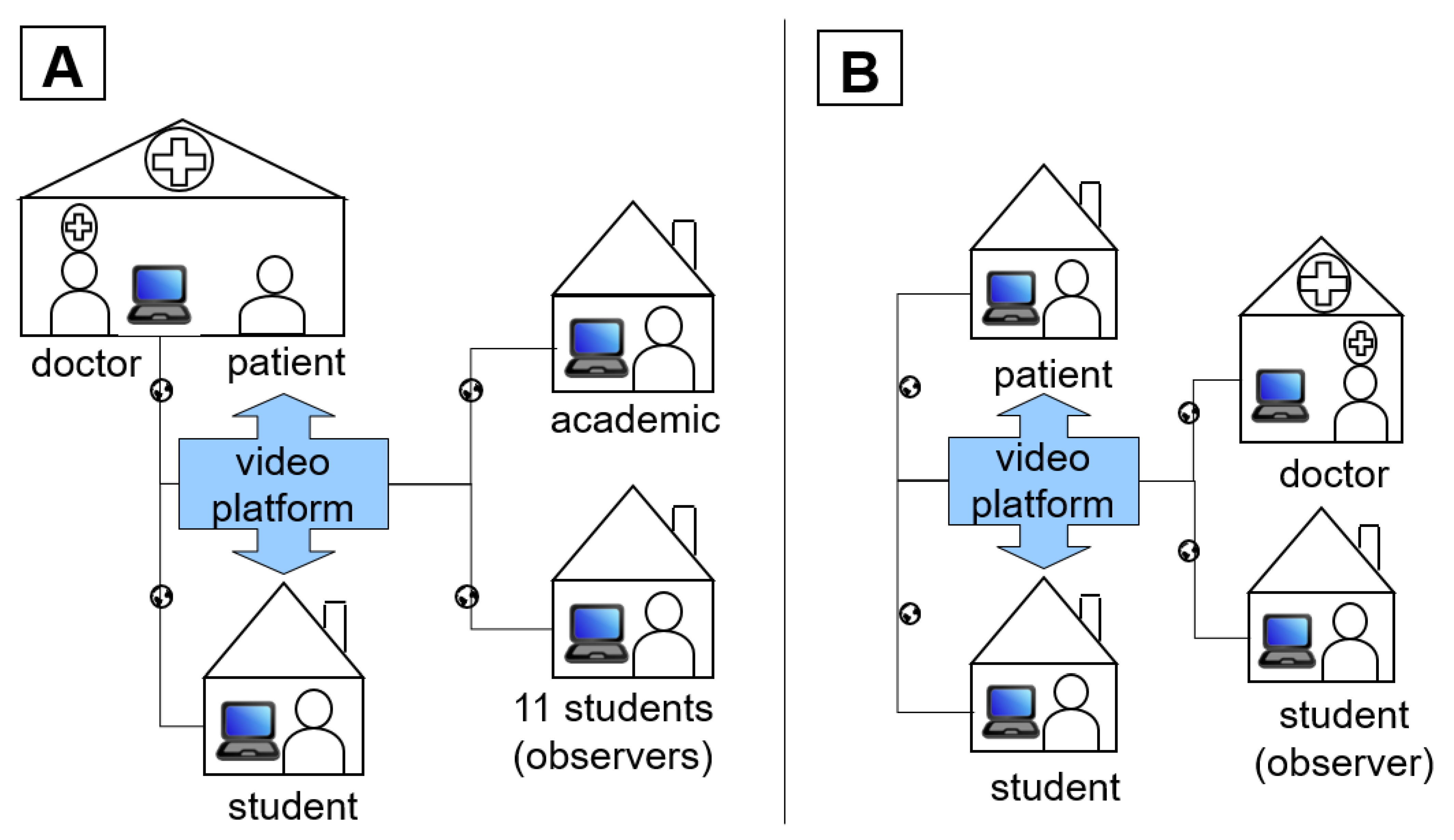
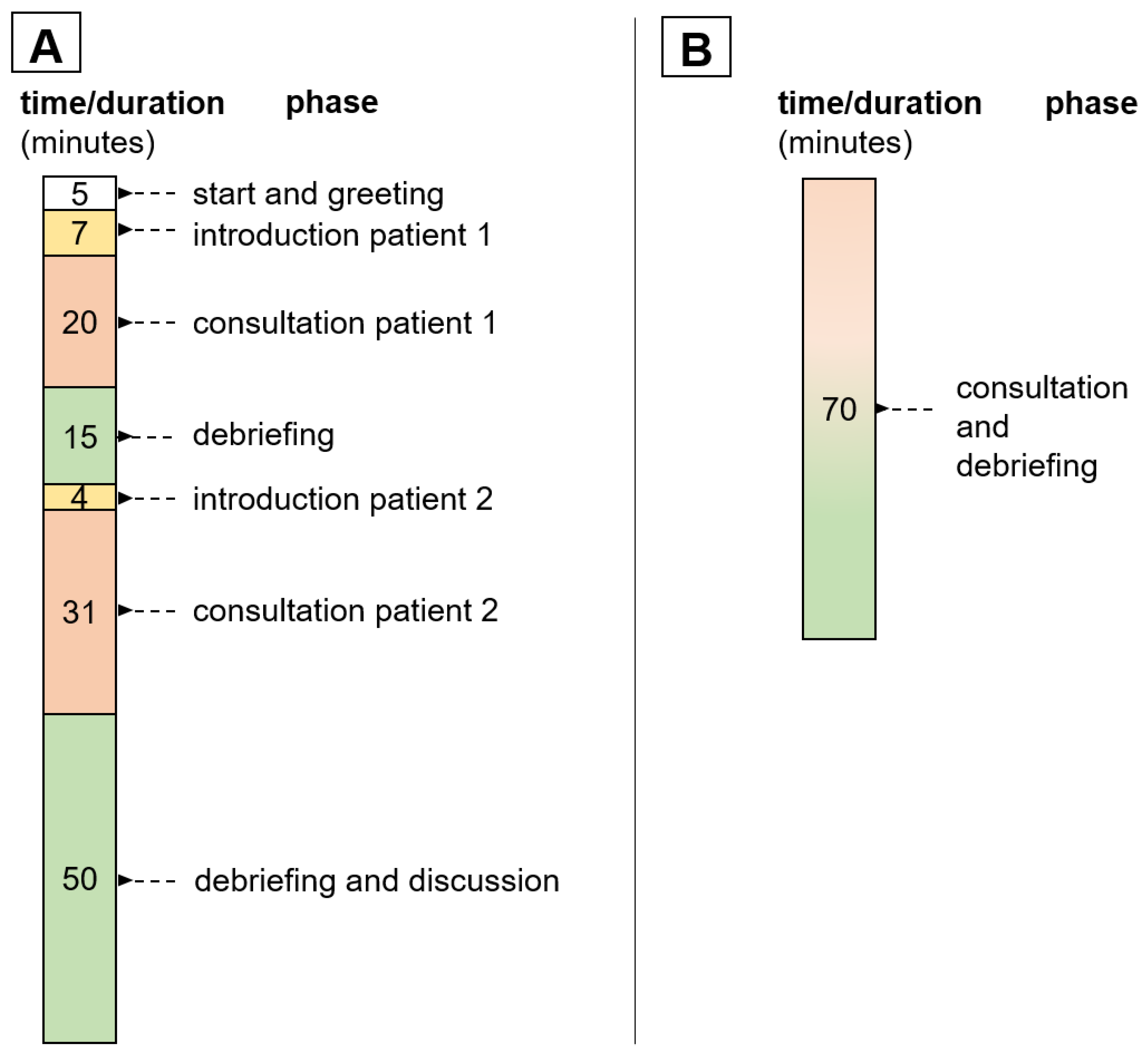
2.3. Teaching Project Concept
2.4. Evaluation and Protocol
2.5. S.W.O.T. Analysis
3. Results
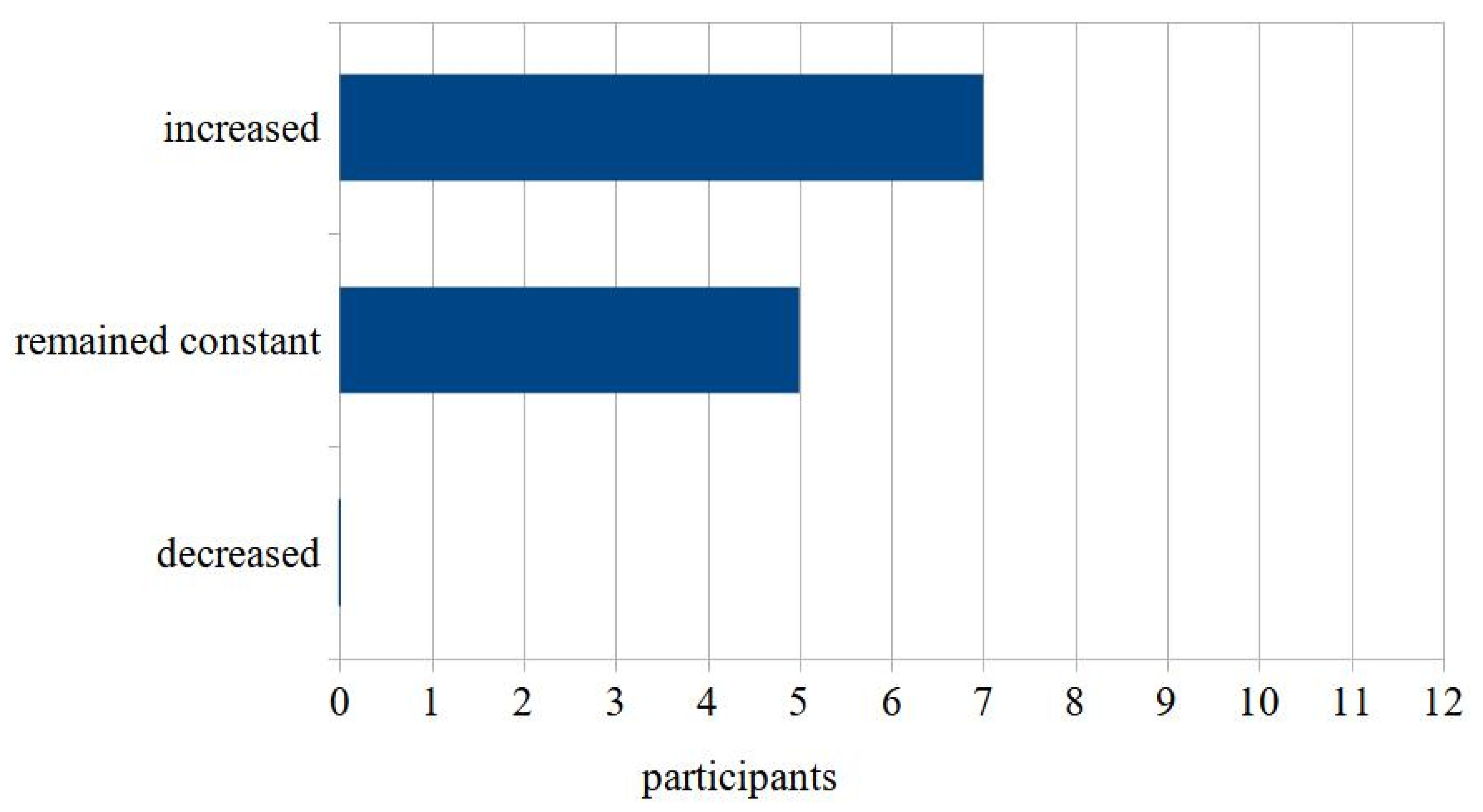
3.1. Telemedicine Research Level
3.2. Family Medicine Research Level
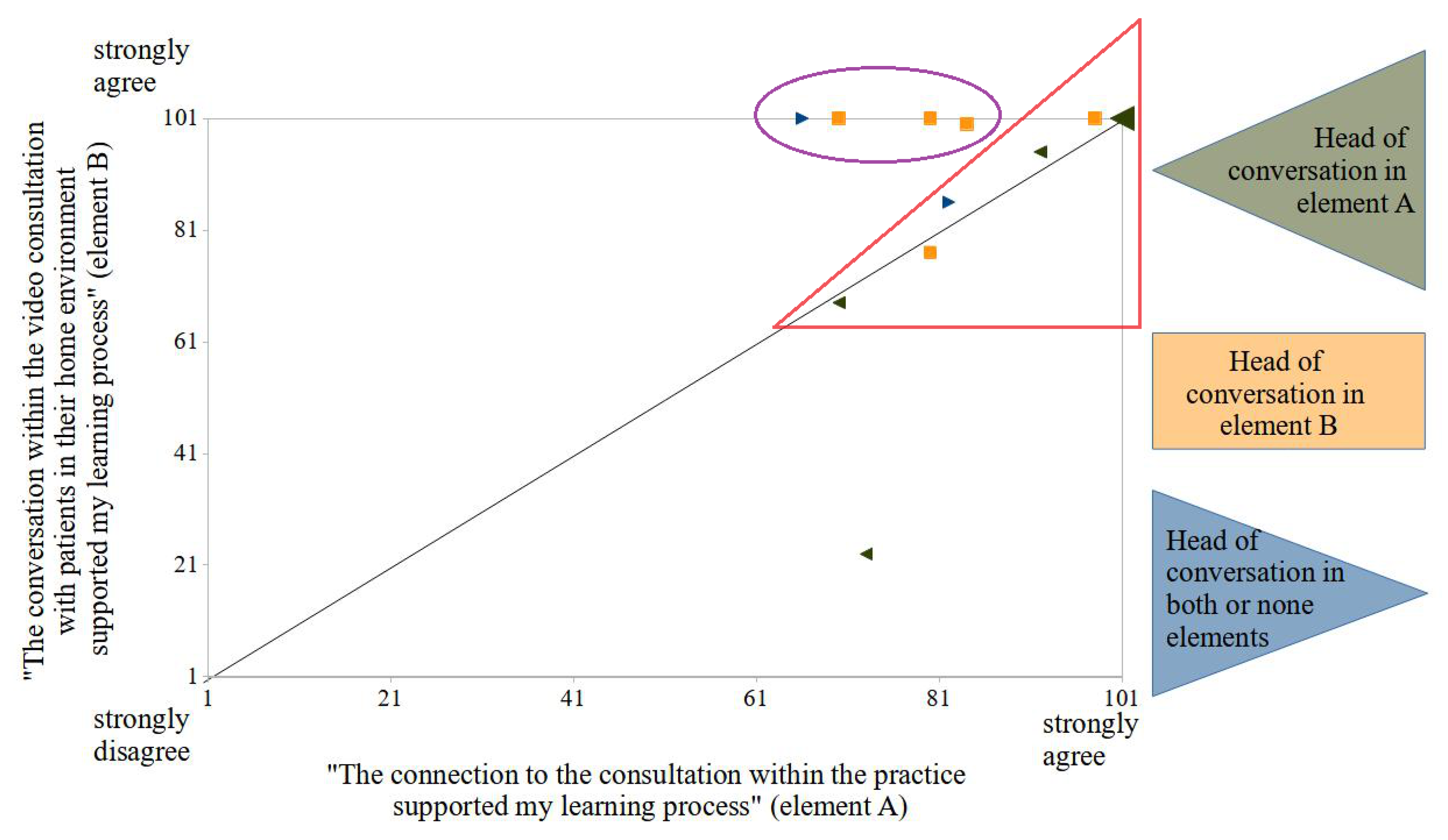
3.3. Didactic Research Level and S.W.O.T. Analysis
3.3.1. Strengths
3.3.2. Weaknesses
3.3.3. Opportunities
3.3.4. Risks
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donaghy, E.; Atherton, H.; Hammersley, V.; McNeilly, H.; Bikker, A.; Robbins, L.; Campbell, J.; McKinstry, B. Acceptability, benefits, and challenges of video consulting: A qualitative study in primary care. Br. J. Gen. Pract. 2019, 69, e586–e594. [Google Scholar] [CrossRef] [PubMed]
- Mold, F.; Hendy, J.; Lai, Y.-L.; De Lusignan, S. Electronic consultation in primary care between providers and patients: Systematic review. JMIR Med. Inform. 2019, 7, e13042. [Google Scholar] [CrossRef]
- Qian, M.; Jiang, J. COVID-19 and social distancing. J. Public Health 2020, 30, 259–261. [Google Scholar] [CrossRef]
- Phadke, N.A.; del Carmen, M.G.; Goldstein, S.A.; Vagle, J.; Hidrue, M.K.; Botti, E.S.; Wasfy, J.H. Trends in ambulatory electronic consultations during the COVID-19 pandemic. J. Gen. Intern. Med. 2020, 35, 3117–3119. [Google Scholar] [CrossRef]
- Obermann, K.; Brendt, I.; Hagen, J. Ärzte im Zukunftsmarkt Gesundheit 2020: Ärztliche Arbeit und Nutzung von Videosprechstunden Während der COVID-19-Pandemie; Stiftung Gesundheit, Health Innovation Hub.: Deutschland, Germany, 2020; Available online: https://www.stiftung-gesundheit.de/pdf/studien/aerzte-im-zukunftsmarktgesundheit_2020_1.pdf (accessed on 2 June 2022).
- Johnsen, T.M.; Norberg, B.L.; Kristiansen, E.; Zanaboni, P.; Austad, B.; Krogh, F.H.; Getz, L. Suitability of video consultations during the COVID-19 pandemic lockdown: Cross-sectional survey among norwegian general practitioners. J. Med. Internet. Res. 2021, 23, e26433. [Google Scholar] [CrossRef]
- Richardson, E.; Aissat, D.; Williams, G.A.; Fahy, N. Keeping what works: Remote consultations during the COVID-19 pandemic. Eurohealth 2020, 26, 73–76. [Google Scholar]
- Sharma, S.C.; Sharma, S.; Thakker, A.; Sharma, G.; Roshan, M.; Varakantam, V. Revolution in UK general practice due to COVID-19 pandemic: A cross-sectional survey. Cureus 2020, 12, e9573. [Google Scholar] [CrossRef] [PubMed]
- TeleMedicon. Available online: https://www.ohnearztpraxis.de/ (accessed on 16 June 2022).
- Shaw, S.E.; Seuren, L.M.; Wherton, J.; Cameron, D.; A’Court, C.; Vijayaraghavan, S.; Morris, J.; Bhattacharya, S.; Greenhalgh, T. Video consultations between patients and clinicians in diabetes, cancer, and heart failure services: Linguistic ethnographic study of videomediated interaction. J. Med. Internet. Res. 2020, 22, e18378. [Google Scholar] [CrossRef] [PubMed]
- No Classrooms, No Clinics: Medical Education during a Pandemic. Available online: https://www.aamc.org/news-insights/no-classrooms-no-clinics-medical-education-during-pandemic (accessed on 16 June 2022).
- Bramstedt, K.A.; Prang, M.; Dave, S.; Shin, P.N.H.; Savy, A.; Fatica, R.A. Telemedicine as an ethics teaching tool for medical students within the nephrology curriculum. Prog. Transplant. 2014, 24, 294–297. [Google Scholar] [CrossRef]
- Sukumar, S.; Zakaria, A.; Lai, C.J.; Sakumoto, M.; Khanna, R.; Choi, N. Designing and implementing a novel virtual rounds curriculum for medical students’ internal medicine clerkship during the COVID-19 pandemic. MedEdPORTAL 2021, 17, 11106. [Google Scholar] [CrossRef]
- Marini, C.P.; Ritter, G.; Sharma, C.; McNelis, J.; Goldberg, M.; Barrera, R. The effect of robotic telerounding in the surgical intensive care units impact on medical education. J. Robot Surg. 2015, 9, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Everard, K.; Schiel, K. Changes in family medicine clerkship teaching due to the COVID-19 pandemic. Fam. Med. 2021, 53, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Outpatient Clinical Student Rotation without Direct Patient Contact: Leveraging Care Transitions to Benefit Students and Patients. Available online: https://www.aamc.org/resource-library/clinical-teaching-and-learning-experiences/outpatient-clinical-student-rotation-without-direct-patient-contact-leveraging-caretransitions (accessed on 16 June 2022).
- Colley, S. Learning Psychiatry in Lockdown—A Different Type of Bedside Manner. BMJ Opin. 2020. Available online: https://blogs.bmj.com/bmj/2020/10/07/learning-psychiatry-in-lockdown-a-different-type-of-bedside-manner/ (accessed on 16 June 2022).
- Weber, A.M.; Dua, A.; Chang, K.; Jupalli, H.; Rizwan, F.; Chouthai, A.; Chen, C. An outpatient telehealth elective for displaced clinical learners during the COVID-19 pandemic. BMC Med. Educ. 2021, 21, 174. [Google Scholar] [CrossRef] [PubMed]
- Chike-Harris, K.E.; Durham, C.; Logan, A.; Smith, G.; DuBose-Morris, R. Integration of telehealth education into the health care provider curriculum: A review. Telemed. J. E-Health Off. J. Am. Telemed. Assoc. 2021, 27, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R.K.; Cooley, D.; Collins, P.B.; Caudle, J.; Coren, J. Transforming a clerkship with telemedicine. J. Osteopath. Med. 2021, 121, 43–47. [Google Scholar] [CrossRef]
- Richter-Kuhlmann, E. Medizinstudium: Neue Approbationsordnung 2025. Dtsch. Arztebl. 2020, 117, A-2335/B-1970. [Google Scholar]
- Jiménez-Rodríguez, D.; Ruiz-Salvador, D.; Salvador, M.R.; Pérez-Heredia, M.; Ronda, F.M.; Arrogante, O. Consensus on criteria for good practices in video consultation: A delphi study. Int. J. Environ. Res. Public Health 2020, 17, 5396. [Google Scholar] [CrossRef]
- Albrecht, M.; Otten, M.; Sander, M. PraxisBarometer Digitalisierung 2021. IGES 2022, pp. 3–11. Available online: https://www.kbv.de/html/praxisbarometer.php (accessed on 6 July 2022).
- Nationaler Kompetenzbasierter Lernzielkatalog Medizin. Available online: https://nklm.de/zend/menu (accessed on 6 July 2022).
- Klinge, K.; Bleckwenn, M. Telemedizin: Rechtlicher Rahmen, Einsatzgebiete und Limitationen [Telemedicine—Legal framework, medical applications and limits]. MMW Fortschr. Med. 2021, 163, 42–49. [Google Scholar] [CrossRef]
- Dedeilia, A.; Sotiropoulos, M.; Hanrahan, J.G.; Janga, D.; Dedeilias, P.; Sideris, M. Medical and surgical education challenges and innovations in the COVID-19 era: A systematic review. In Vivo 2020, 34 (Suppl. S3), 1603–1611. [Google Scholar] [CrossRef]
- Waseh, S.; Dicker, A.P. Telemedicine training in undergraduate medical education: Mixedmethods review. JMIR Med. Educ. 2019, 5, e12515. [Google Scholar] [CrossRef] [Green Version]
- Kunstmann, W.; Wollgarten, D.; Helmich, P.; Koneczny, N.; Butzlaff, M. Allgemeinmedizin im Medizinstudium: Das Lehrpraxenprogramm der Universität Witten/Herdecke. ZFA 2003, 79, 399–404. [Google Scholar] [CrossRef]
- Agarwall, P.K. A combined approach in prolonged COVID-19 pandemic to teach undergraduate surgery students—Future primary care physicians. J. Fam. Med. Prim. Care 2020, 9, 5480–5483. [Google Scholar] [CrossRef] [PubMed]
- Cannon, P.; Lumsden, L.; Waas, V. An innovative and authentic way of learning how to consult remotely in response to the COVID-19 pandemic. Educ. Prim. Care 2022, 33, 53–58. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Problem | Solution Approach |
|---|---|
| Picture blurred | Use of a tripod except for ultrasounds, otherwise the camera is too far away from the screen |
| Moderate picture quality | Optimized lighting (frontal/side) |
| View of patient from below | Tablet stands elevated on a tripod |
| Mouth–nose protection hides facial expressions and makes communication difficult | The primary care physician attends the meeting from another room during the history taking, so that the patients can remove their mouth–nose protection |
| Image section only on patient’s face | Second camera in the room, also to observe the gait pattern |
| Category | Participants Answers |
|---|---|
| Prior knowledge | Medical history experiences Family medicine experience to help focus and recognize the difference between face-to-face and remote treatment Two completed family medicine internships Prior knowledge of internal medicine, especially pharmacological Broad general knowledge of various diseases from a variety of specialties |
| Setting | Empathy |
| Motivation Appreciative attitude towards patients and teachers | |
| Equipment | Stable internet connection |
| Functioning terminal with good camera, microphone, headphones | |
| Quiet environment during patient interviews | |
| Second screen if necessary |
| Strengths | Weaknesses | Opportunities | Threats |
|---|---|---|---|
| Patient contact (T, S) | Pilot project (T) | Lessons for times with & without pandemic (T, S) | Hurdles of incorporation into the curriculum (T) |
| Complement to face-to-face contact (T, S) | Costs (T) | Inclusion (T, S) | Lack of commitment (T) |
| Learning success (T) | Equipment (T) | Alternative teaching formats (T) | Lack of personnel (T) |
| Local flexibility (T) | Time required (T, S) | Integration into a learning context (T) | Professional differences (T) |
| Supraregionality (T) | Technical problems (T, S) | Incorporate teaching practices (T) | Technology problems (T) |
| Teamwork (T, S) | Limited perception (T, S) | Free choice of core topics (T) | Focus on telemedicine (T) |
| Adaptation of technology & learning objectives (T, S) | Extent of learning (T, S) | Application in other subject areas (T) | Data protection (T) |
| Human resources | |||
| Preparation (T, S) | Lack of time (T, S) | Using & developing technological innovations (T) | |
| Voluntary event (T) | Limited treatment occasions (T, S) | Mutual motivation (T) | |
| Focused work (T, S) | Professional differences (T) | Improving patient care (T) | |
| Individualized design of one-on-one consultation hours (T, S) | Communication problems (T) | Closing research gaps (T) | |
| Satisfaction (T) | Data protection (S) | Support development of digital medicine in Germany (T) | |
| Relevance of video consulting hours (T, S) | Lack of quality guidelines (T) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Särchen, F.; Springborn, S.; Mortsiefer, A.; Ehlers, J. Patient Care via Video Consultations: Piloting and S.W.O.T. Analysis of a Family Medicine Digitally Synchronous Seminar for Medical Students. Int. J. Environ. Res. Public Health 2022, 19, 8922. https://doi.org/10.3390/ijerph19158922
Särchen F, Springborn S, Mortsiefer A, Ehlers J. Patient Care via Video Consultations: Piloting and S.W.O.T. Analysis of a Family Medicine Digitally Synchronous Seminar for Medical Students. International Journal of Environmental Research and Public Health. 2022; 19(15):8922. https://doi.org/10.3390/ijerph19158922
Chicago/Turabian StyleSärchen, Franziska, Susanne Springborn, Achim Mortsiefer, and Jan Ehlers. 2022. "Patient Care via Video Consultations: Piloting and S.W.O.T. Analysis of a Family Medicine Digitally Synchronous Seminar for Medical Students" International Journal of Environmental Research and Public Health 19, no. 15: 8922. https://doi.org/10.3390/ijerph19158922
APA StyleSärchen, F., Springborn, S., Mortsiefer, A., & Ehlers, J. (2022). Patient Care via Video Consultations: Piloting and S.W.O.T. Analysis of a Family Medicine Digitally Synchronous Seminar for Medical Students. International Journal of Environmental Research and Public Health, 19(15), 8922. https://doi.org/10.3390/ijerph19158922