
Restored Life of Elite Athletes after Spinal Cord Injury

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
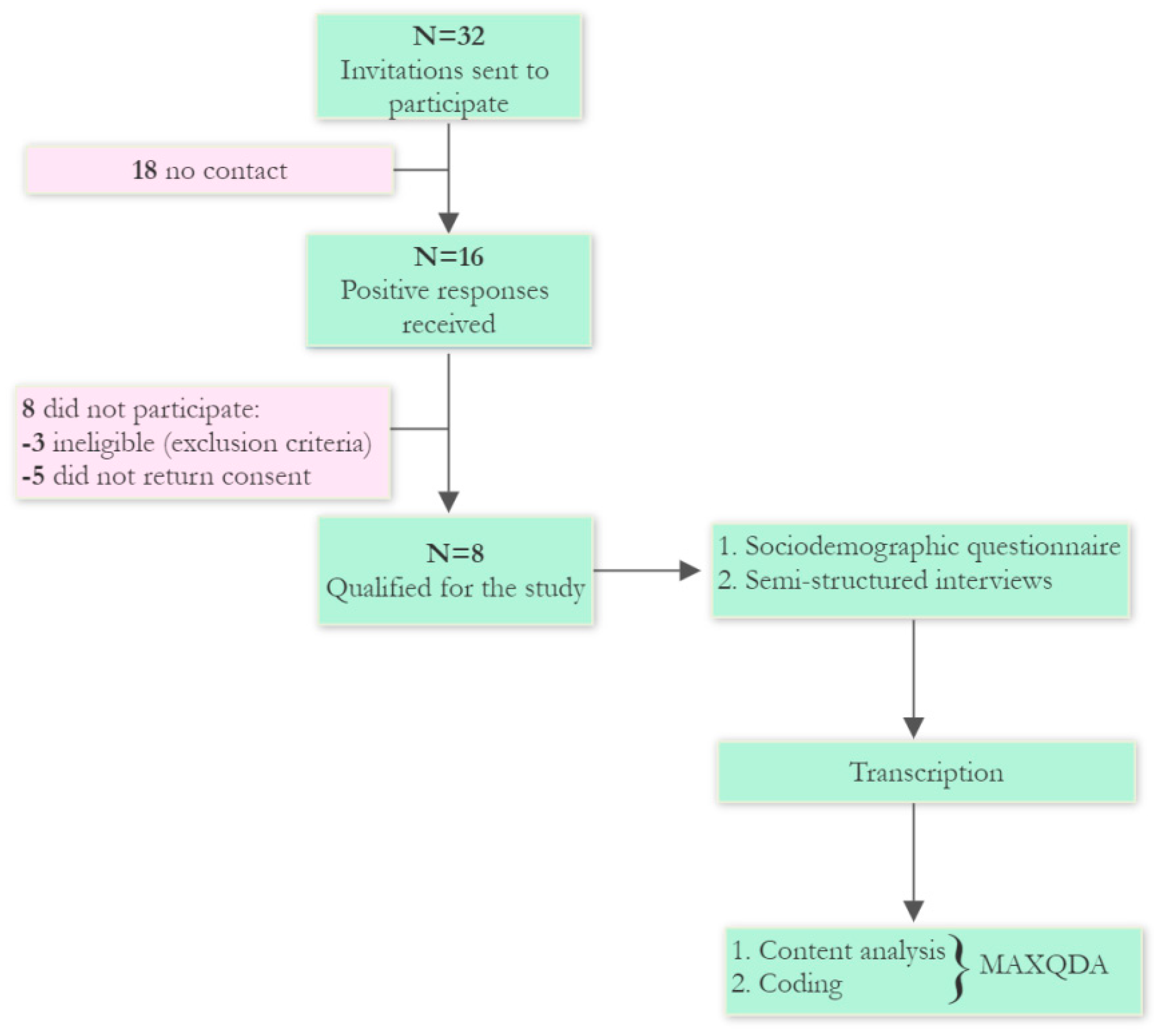
2.1. Participants
2.2. Study Design
2.3. Data Processing and Analysis
3. Results
3.1. Coping—An Early Adaptive Pattern
P1: It is really difficult, your mental challenge is to keep going. Everything was a challenge when I woke up.
P4: There were some dark days, and I really struggled initially but I had such a lot of support
P2: I interrupted him ‘That means I’m paralyzed from now on. Is that right?’ and then he said ‘Yes’ that was the moment that brought some tears to my eyes. Then he continued talking immediately what was very important because he said ‘I have to remind that today I have a healthy head, a healthy mindset, and quite healthy hands, and these components make sure that I can have quite normal life. Yea and maybe this was the most important sentence in this whole journey which I’m since that day.
P3: From the very beginning I had a positive and fighting attitude. I didn’t understand myself fully but I didn’t have a single moment of breakdown.
P7: I think in psychology it is described somehow, some kind of denial that I can do it. That 99 out of 100 couldn’t make it, but I can make it. This is related to what I said, that after the accident I spent several years on rehabilitation, that very hard, professional work will have some effect, and although history teaches us that in some cases there is no effect. I explained to myself that there was no effect because these people were not determined enough, but I explained to myself that if I spent years I would think I would succeed.
P5: It was good that I had the hope that I had. I was 100-percent convinced that I was going to walk out of hospital. Without this hope, it would be so much more depressing.
3.2. Sports Identity
P8: My life has always revolved around sports because my dad was a sportsman Well, I must have been soaked in it like a shell of an egg and this sport was absorbed by me as well Well, there was still some soccer later on because there was also speedway Well, I ended up on this speedway the way I ended up, Skiing and cycling were also passions that I continue somewhere now because I also ski and cycle, so it was such a cool life because maybe in the summer I rode speedway, cycling and then came winter. Since autumn I was already skiing because I also had a ski school. Also I was teaching skiing some trips we organized, training for children for adults of all ages and such a life to envy…
P2: They also knew about that I was a sportsman so I could handle some things a bit better.
P5: My identity has always been of an athlete and so now not to have that as my identity was frightening really scary during that time. ..... I think all of these things sort of happening when they happen gaining my confidence back from tennis and basketball. You know sort of being more outgoing. Where is for a while i was such an introvert because I didn’t know I was not comfortable with myself. So you know it’s taking a long years. You know what I think it’s different for everyone in a chair. I learned to be totally ok with myself and that changed a lot for me not only in sport and to make the connections that I’ve made and to be able to talk about you know an accident and my process and my journey throughout the whole thing.
P7: I saw it and it made me feel really stupid, ashamed. Because I saw, let’s call it broadly, people like me, and they were lifting such weights…How do we count these circles? How many are there? And at that moment the athletic soul was awakened, the perversity that I also have to here. And that was the beginning.
P8:…in fact life didn’t end that you can still do sports, maybe a little bit in a different form because unfortunately for that you need some kind of special equipment, but it was possible. Well there was some kind of a signal that I was saying that he can continue to do that skiing that I used to do before the accident, I’m still doing it, and that’s how it went.
P3: I still sometimes take part in, appear at the start or finish line of, for the benefit of the earth, or marathons, also supporting runners, because I myself enjoyed running before the accident. And after the accident, from friend to friend, it so happened that I also support the runners. Also at some stops, finish line or start I am with them. I don’t run marathons with them because my arms would fall off, but at least this way I spend time with them
3.3. Adjustment—A Long-Term Adaptive Pattern
3.3.1. Finding the Meaning of the Accident
P4: I believe, my accident happened for a reason so I can support young people who have a similar injury to me but don’t have that support I received.
3.3.2. Sources of Motivation
P1: After some time I was able to keep myself standing, it was so good for my mental condition, it was so inspiring and motivating.
P2: When you see other people being proud of you because you just managed to move in the wheelchair.
P3: I watch motivational speakers on youtube who are also struggling and overcoming these barriers.
P7: Negative motivation, I will tell you what it is, in short, it means that when someone throws obstacles under my feet and is motivated by some, I don’t know, malice, which I experienced. This motivates me very much to show them, to rub their noses in it.
3.3.3. Acceptance of Disability
P5: I didn’t want to be around anyone in a wheelchair because that made me really realise that was my world but when I did and it was when I started to go out to the tennis practices and I would hang out with everyone that was playing at the time. It makes it a little bit more bearable and so like. I ended up I love the fact that I’m part of this community.
P2: Training, working, being outside, that wheelchair live is possible.
P4: For once I didn’t feel pity because of my situation. That’s amazing.
P3: I try to show that a person in a wheelchair is not a freak but a normal person who needs normality, tenderness, and to be with other people.
P8: Some companies motivate employees and show them that they are complaining having actually everything having arms, legs they are there complaining that they don’t want something and this shows them that they are half the guy that is 50% and doing twice as much work as them.
3.3.4. Goals
P2: I have reached all my milestones. In my situation now my goal is to improve my walking on crutches, or without crutches.
P2: I want to raise the focus of the public when they build things to think about disable.
P4: The ambitions in my life is to make a foundation full of friends and spread the word about disability. I think as well we are changing the world for many disabled people, we empower them to do their best, make the most of their lives, try to look at the positives of their lives. That is massively important in this situation. We just try to give people hope that they can move on with their life. We try to give them a purpose to wake up every morning. that’s really important.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goraczko, A.; Zurek, A.; Lachowicz, M.; Kujawa, K.; Zurek, G. Is Self-Efficacy Related to the Quality of Life in Elite Athletes after Spinal Cord Injury? Int. J. Environ. Res. Public Health 2021, 18, 10866. [Google Scholar] [CrossRef] [PubMed]
- Andresen, S.R.; Biering-Sørensen, F.; Hagen, E.M.; Nielsen, J.F.; Bach, F.W.; Finnerup, N.B. Pain, Spasticity and Quality of Life in Individuals with Traumatic Spinal Cord Injury in Denmark. Spinal Cord 2016, 54, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Liem, N.R.; McColl, M.A.; King, W.; Smith, K.M. Aging with a Spinal Cord Injury: Factors Associated with the Need for More Help with Activities of Daily Living. Arch. Phys. Med. Rehabil. 2004, 85, 1567–1577. [Google Scholar] [CrossRef]
- Barker, R.N.; Kendall, M.D.; Amsters, D.I.; Pershouse, K.J.; Haines, T.P.; Kuipers, P. The Relationship between Quality of Life and Disability across the Lifespan for People with Spinal Cord Injury. Spinal Cord 2009, 47, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Murray, A. Prevalence of Depression After Spinal Cord Injury: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 133–140. [Google Scholar] [CrossRef]
- Müller, R.; Landmann, G.; Béchir, M.; Hinrichs, T.; Arnet, U.; Jordan, X.; Brinkhof, M.W.G. Chronic Pain, Depression and Quality of Life in Individuals with Spinal Cord Injury: Mediating Role of Participation. J. Rehabil. Med. 2017, 49, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Ko, H.-Y. Current Epidemiology of Spinal Cord Injuries. In Management and Rehabilitation of Spinal Cord Injuries; Ko, H.-Y., Ed.; Springer Nature: Singapore, 2022; pp. 233–249. ISBN 978-981-19022-8-4. [Google Scholar]
- Fitzharris, M.; Cripps, R.A.; Lee, B.B. Estimating the Global Incidence of Traumatic Spinal Cord Injury. Spinal Cord 2014, 52, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Furlan, J.C.; Sakakibara, B.M.; Miller, W.C.; Krassioukov, A.V. Global Incidence and Prevalence of Traumatic Spinal Cord Injury. Can. J. Neurol. Sci. 2013, 40, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.W.; Eng, J.J.; Tator, C.H.; Krassioukov, A. Spinal Cord Injury Research Evidence Team Epidemiology of Sport-Related Spinal Cord Injuries: A Systematic Review. J. Spinal Cord Med. 2016, 39, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Trieschmann, R.B. The Psychological, Social, and Vocational Adjustment to Spinal Cord Injury. Annu. Rev. Rehabil. 1980, 1, 304–318. [Google Scholar] [PubMed]
- Sprangers, M.A.; Schwartz, C.E. Integrating Response Shift into Health-Related Quality of Life Research: A Theoretical Model. Soc. Sci. Med. 1999, 48, 1507–1515. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin/Heidelberg, Germany, 1984; ISBN 9780826141927. [Google Scholar]
- Craig, A.; Tran, Y. Psychological Aspects Associated with Spinal Cord Injury Rehabilitation: New Directions and Best Evidence; Nova Science Publishers: Hauppauge, NY, USA, 2008. [Google Scholar]
- Craig, A.; Tran, Y.; Middleton, J. Theory of Adjustment Following Severe Neurological Injury: Evidence Supporting the Spinal Cord Injury Adjustment Model; Nova Science Publishers: Hauppauge, NY, USA, 2017; ISBN 978-1-5361-0795-1. [Google Scholar]
- Elfström, M.L.; Rydén, A.; Kreuter, M.; Persson, L.-O.; Sullivan, M. Linkages between Coping and Psychological Outcome in the Spinal Cord Lesioned: Development of SCL-Related Measures. Spinal Cord 2002, 40, 23–29. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Quale, A.J.; Schanke, A.-K. Resilience in the Face of Coping with a Severe Physical Injury: A Study of Trajectories of Adjustment in a Rehabilitation Setting. Rehabil. Psychol. 2010, 55, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Kennedy, P.; Galatzer-Levy, I.R.; Lude, P.; Elfström, M.L. Trajectories of Resilience, Depression, and Anxiety Following Spinal Cord Injury. Rehabil. Psychol. 2012, 57, 236–247. [Google Scholar] [CrossRef]
- Pollard, C.; Kennedy, P. A Longitudinal Analysis of Emotional Impact, Coping Strategies and Post-Traumatic Psychological Growth Following Spinal Cord Injury: A 10-Year Review. Br. J. Health Psychol. 2007, 12, 347–362. [Google Scholar] [CrossRef]
- Craig, A.R.; Hancock, K.M.; Dickson, H.G. A Longitudinal Investigation into Anxiety and Depression in the First 2 Years Following a Spinal Cord Injury. Spinal Cord 1994, 32, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, R.; Calhoun, L. Trauma & Transformation: Growing in the Aftermath of Suffering; Sage: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Byra, S. Basic Hope and Posttraumatic Growth in People with Traumatic Paraplegia—The Mediating Effect of Acceptance of Disability. Spinal Cord 2019, 57, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Kalpakjian, C.Z.; McCullumsmith, C.B.; Fann, J.R.; Richards, J.S.; Stoelb, B.L.; Heinemann, A.W.; Bombardier, C.H. Post-Traumatic Growth Following Spinal Cord Injury. J. Spinal Cord Med. 2014, 37, 218–225. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Smith, J.L.; McManus, A. A Review on Transitional Implications for Retiring Elite Athletes: What Happens When the Spotlight Dims? Open Sports Sci. J. 2009, 1, 45–49. [Google Scholar] [CrossRef]
- McVeigh, S.A.; Hitzig, S.L.; Craven, B.C. Influence of Sport Participation on Community Integration and Quality of Life: A Comparison between Sport Participants and Non-Sport Participants with Spinal Cord Injury. J. Spinal Cord Med. 2009, 32, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Szeliga, E.; Brzozowska-Magoń, A.; Borys, R.; Wolan-Nieroda, A.; Walicka-Cupryś, K. The Relationship between Physical Activity Level and Functional Status of Subjects with High Spinal Cord Injury. Int. J. Environ. Res. Public Health 2022, 19, 1787. [Google Scholar] [CrossRef] [PubMed]
- Silveira, S.L.; Ledoux, T.; Cottingham, M.; Hernandez, D.C. Association among Practice Frequency on Depression and Stress among Competitive US Male Wheelchair Rugby Athletes with Tetraplegia. Spinal Cord 2017, 55, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Tasiemski, T.; Osinska, M. Sport in People with Tetraplegia: Review of Recent Literature. Trends Sport Sci. 2013, 20, 81–88. [Google Scholar]
- Hawkins, C.; Coffee, P.; Soundy, A. Considering How Athletic Identity Assists Adjustment to Spinal Cord Injury: A Qualitative Study. Physiotherapy 2014, 100, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Sparkes, A.C. Men, Sport, Spinal Cord Injury, and Narratives of Hope. Soc. Sci. Med. 2005, 61, 1095–1105. [Google Scholar] [CrossRef]
- Badenhorst, M.; Brown, J.C.; Lambert, M.I.; Van Mechelen, W.; Verhagen, E. Quality of Life among Individuals with Rugby-Related Spinal Cord Injuries in South Africa: A Descriptive Cross-Sectional Study. BMJ Open 2018, 8, e020890. [Google Scholar] [CrossRef]
- Kallio, H.; Pietilä, A.-M.; Johnson, M.; Kangasniemi, M. Systematic Methodological Review: Developing a Framework for a Qualitative Semi-Structured Interview Guide. J. Adv. Nurs. 2016, 72, 2954–2965. [Google Scholar] [CrossRef]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of Data Collection in Qualitative Research: Interviews and Focus Groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef]
- van Diemen, T.; van Nes, I.J.W.; van Laake-Geelen, C.C.M.; Spijkerman, D.; Geertzen, J.H.B.; Post, M.W.M. SELF-SCI Group Learning Self-Care Skills after Spinal Cord Injury: A Qualitative Study. BMC Psychol. 2021, 9, 155. [Google Scholar] [CrossRef] [PubMed]
- Zuchetto, M.A.; Schoeller, S.D.; Tholl, A.D.; Lima, D.K.S.; Neves da Silva Bampi, L.; Ross, C.M. The Meaning of Hope for Individuals with Spinal Cord Injury in Brazil. Br. J. Nurs. 2020, 29, 526–532. [Google Scholar] [CrossRef]
- Sparkes, A.C.; Smith, B. Sport, Spinal Cord Injuries, Embodied Masculinities, and Narrative Identity Dilemmas. Men Masc. 2002, 4, 258–285. [Google Scholar] [CrossRef]
- Booth, R. “He Wasn’t Prepared for a Second-Class Life”: Why Injured Rugby Star Went to Switzerland to Die. The Guardian, 18 October 2008. [Google Scholar]
- Tasiemski, T.; Brewer, B.W. Athletic Identity, Sport Participation, and Psychological Adjustment in People with Spinal Cord Injury. Adapt. Phys. Act. Q. 2011, 28, 233–250. [Google Scholar] [CrossRef] [PubMed]
- Sparkes, A.C. Athletic Identity: An Achilles’ Heel to the Survival of Self. Qual. Health Res. 1998, 8, 644–664. [Google Scholar] [CrossRef]
- Perrier, M.-J.; Sweet, S.N.; Strachan, S.M.; Latimer-Cheung, A.E. I Act, Therefore I Am: Athletic Identity and the Health Action Process Approach Predict Sport Participation among Individuals with Acquired Physical Disabilities. Psychol. Sport Exerc. 2012, 13, 713–720. [Google Scholar] [CrossRef]
- Nicholls, E.; Lehan, T.; Plaza, S.L.O.; Deng, X.; Romero, J.L.P.; Pizarro, J.A.A.; Carlos Arango-Lasprilla, J. Factors Influencing Acceptance of Disability in Individuals with Spinal Cord Injury in Neiva, Colombia, South America. Disabil. Rehabil. 2012, 34, 1082–1088. [Google Scholar] [CrossRef]
- Perrier, M.-J.; Shirazipour, C.H.; Latimer-Cheung, A.E. Sport Participation among Individuals with Acquired Physical Disabilities: Group Differences on Demographic, Disability, and Health Action Process Approach Constructs. Disabil. Health J. 2015, 8, 216–222. [Google Scholar] [CrossRef]
- Athelstan, G.T.; Crewe, N.M. Psychological Adjustment to Spinal Cord Injury as Related to Manner of Onset of Disability. Rehabil. Couns. Bull. 1979, 22, 311–319. [Google Scholar]


{kind=link}
| Participant | Age | Gender | Nationality | Level of SCI | Years since Injury | Discipline before SCI | Sport after SCI |
|---|---|---|---|---|---|---|---|
| P1 | 41 | Male | British | C3/4 | 14 | BMX dirt jumps | No |
| P2 | 29 | Male | Austrian | C6/7 | 5 | Ski jumping | Rugby, skiing |
| P3 | 24 | Female | Polish | Th11/12 | 6 | Karate | Wheelchair dancing |
| P4 | 37 | Male | British | C4/5 | 16 | Rugby | No |
| P5 | 45 | Female | Canadian | Th12/L1 | 14 | Mountain Biking | Wheelchair basketball |
| P6 | 31 | Male | British | Th6 | 15 | Motocross | Car race |
| P7 | 40 | Male | Polish | Th11 | 17 | Judo | Canoe |
| P8 | 47 | Male | Polish | L1/2 | 15 | Speedway | Hand cycling |
| Category | Subcategory | Quotation |
|---|---|---|
| Coping | Struggles | P1: It is really difficult, your mental challenge is to keep going. Everything was a challenge when I woke up. |
| Fighting Spirit | P7: I got into rehabilitation, intensive rehabilitation, which was replacing my sports training, and it lasted a couple of years. P8: “The sports anger in me woke up, I said to the doctor, you’ll see I’ll prove it to you I’ll come in on crutches, whatever. | |
| Athletic Identity | Fans’ support | P1: I was very lucky because it was quite public. I was highlighted a lot from my crash. People in sports insurance were amazing, they have set up the fund, and people were donating money |
| The advantage of being an athlete | P3: Karate before the accident taught me perseverance and diligence, which came in very handy later in this daily struggle. | |
| Interaction with the sports community | P2: The connection is still here and it’s always fun to watch them at their training, and it’s even more fun when I try to use their exercises for my training. And another thing is I just stand before coach exam, so I can train young ski jumpers. I wanted to stay here because i really lived in this area because of ski jumping and training. This is the middle point of my life. | |
| P4: with Leicester Tigers, I coach sometimes. I support beneficiaries for Leicester tigers charity. It’s pretty good really | ||
| P5: and that gave me purpose and that was helpful for me but when that race ended and all through, but it gave me a purpose to get out of bed and to do something and so that was the that was sort of the baby steps. | ||
| Adjustment | Finding the meaning of the accident | P2: I stopped to complain about things which I cannot change. That I think, was one of the best things i learned because this save so much energy. P3: For sure life is reevaluating and I am so positive people admire me because I don’t worry about trivial things. P4: I believe, my accident happened for a reason so I can support young people who have a similar injury to me but don’t have that support I received. |
| Motivation sources | P1: My kids, yeah. That’s the main thing that keeps me going. P1: After some time I was able to keep myself standing, it was so good for my mental condition, it was so inspiring and motivating. P2: When you see other people being proud of you because you just managed to move in the wheelchair. | |
| Disability acceptance | P5: I ended up I love the fact that I’m part of this community. | |
| Goals, plans | P1: I just want to do more motivational talks, raise my boys, they are great kids. P2: I want to raise the focus of the public when they build things to think about disable P4: The ambitions in my life is to make a foundation full of friends and spread the word about disability. I think as well we are changing the world for many disabled people, we empower them to do their best, make the most of their lives, try to look at the positives of their lives P6: at the minute my big goal is to compete the best I can with my disability in racing. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zurek, G.; Goraczko, A.; Żurek, A.; Lachowicz, M.; Kujawa, K. Restored Life of Elite Athletes after Spinal Cord Injury. Int. J. Environ. Res. Public Health 2022, 19, 8441. https://doi.org/10.3390/ijerph19148441
Zurek G, Goraczko A, Żurek A, Lachowicz M, Kujawa K. Restored Life of Elite Athletes after Spinal Cord Injury. International Journal of Environmental Research and Public Health. 2022; 19(14):8441. https://doi.org/10.3390/ijerph19148441
Chicago/Turabian StyleZurek, Grzegorz, Agata Goraczko, Alina Żurek, Maciej Lachowicz, and Katarzyna Kujawa. 2022. "Restored Life of Elite Athletes after Spinal Cord Injury" International Journal of Environmental Research and Public Health 19, no. 14: 8441. https://doi.org/10.3390/ijerph19148441
APA StyleZurek, G., Goraczko, A., Żurek, A., Lachowicz, M., & Kujawa, K. (2022). Restored Life of Elite Athletes after Spinal Cord Injury. International Journal of Environmental Research and Public Health, 19(14), 8441. https://doi.org/10.3390/ijerph19148441