
Effects of Physical Activity Interventions on Health Outcomes among Older Adults Living with HIV: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.3. Data Sources and Search Strategy
2.4. Selection Process
2.5. Data Extraction
2.6. Risk-of-Bias Assessment
2.7. Effect Measures and Synthesis Methods
3. Results
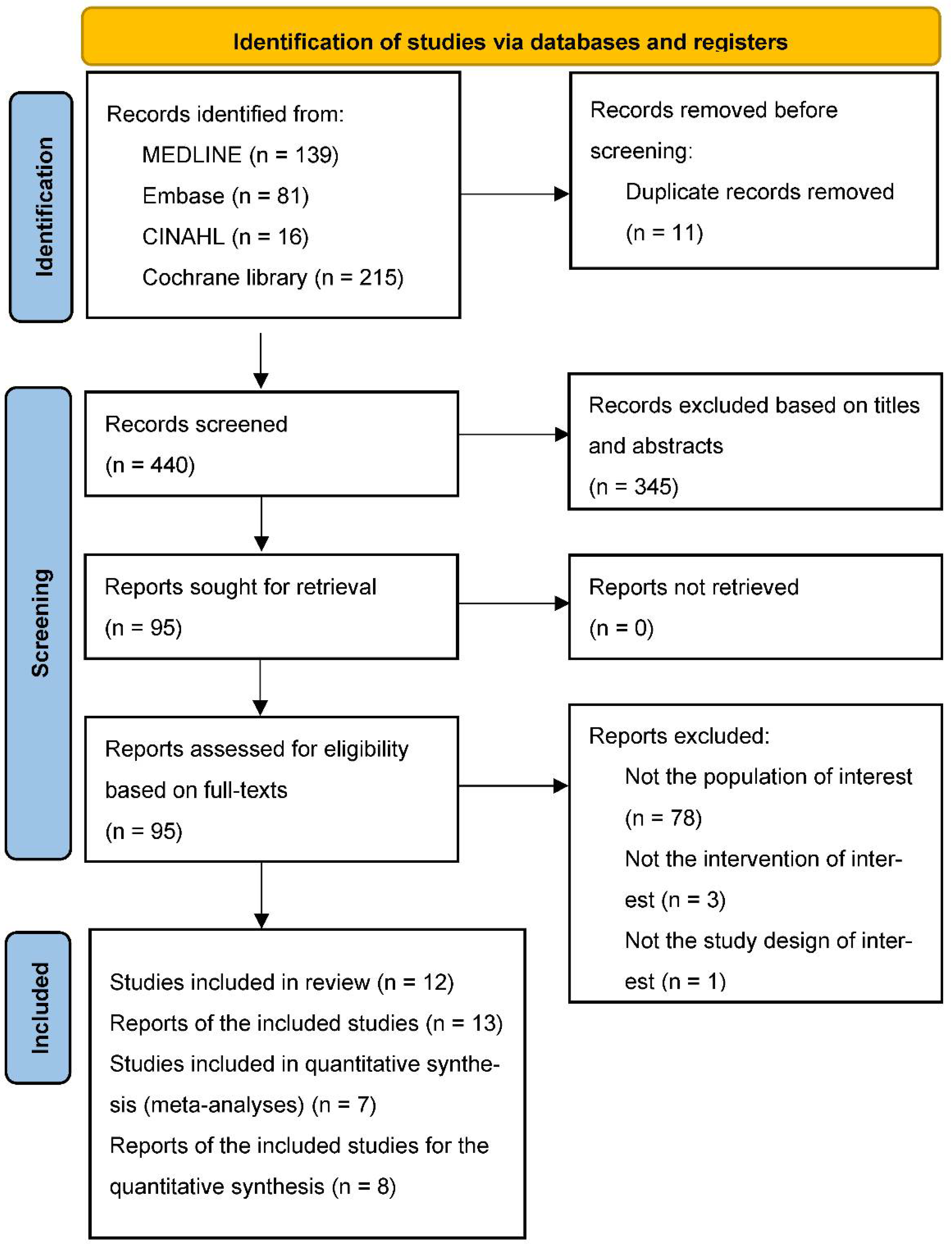
3.1. Study Selection
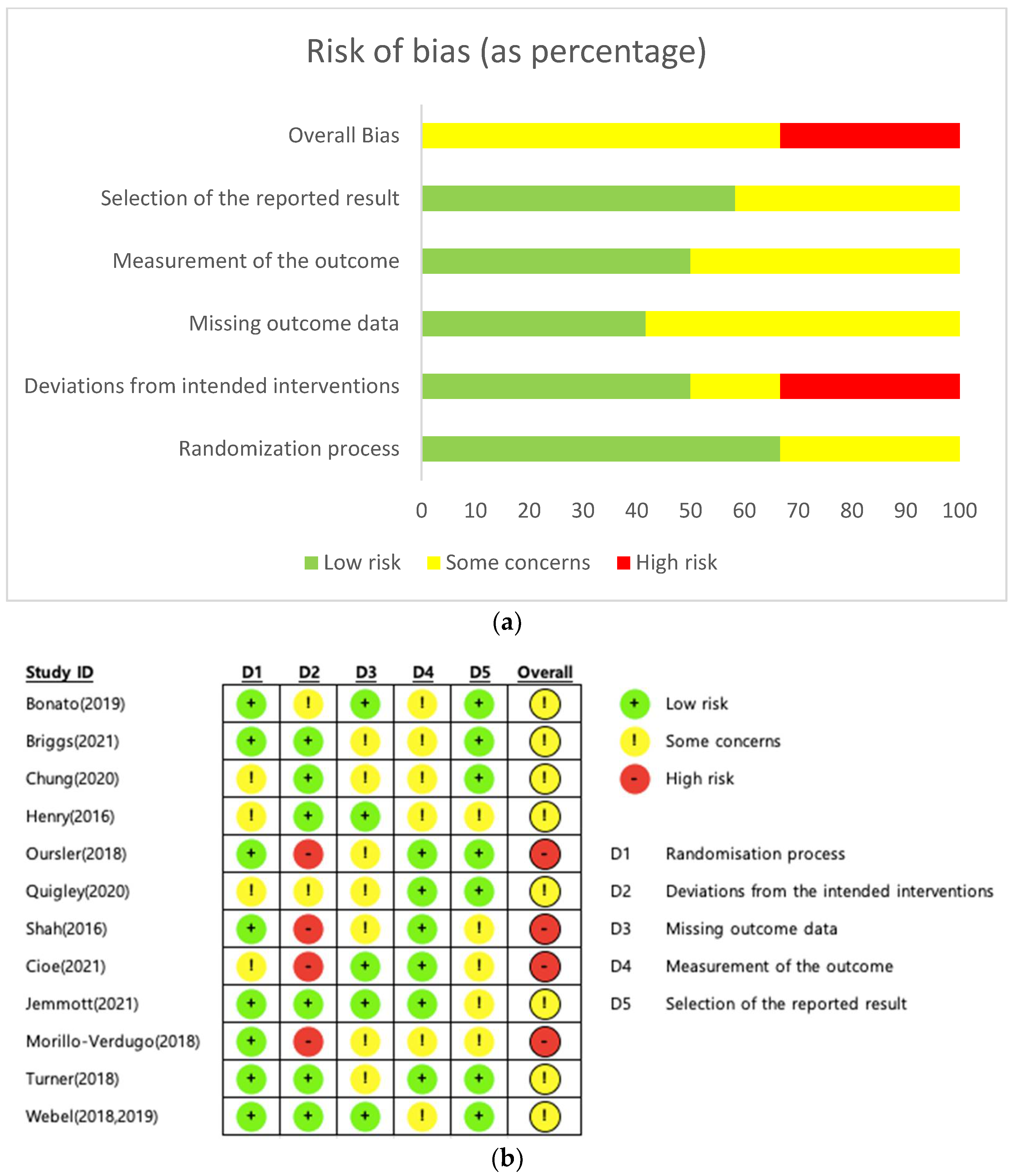
3.2. Risk-of-Bias
3.3. Study Characteristics
3.4. Study Participants’ Characteristics
3.5. Intervention Characteristics
3.6. Physical and Phycological Health Outcomes
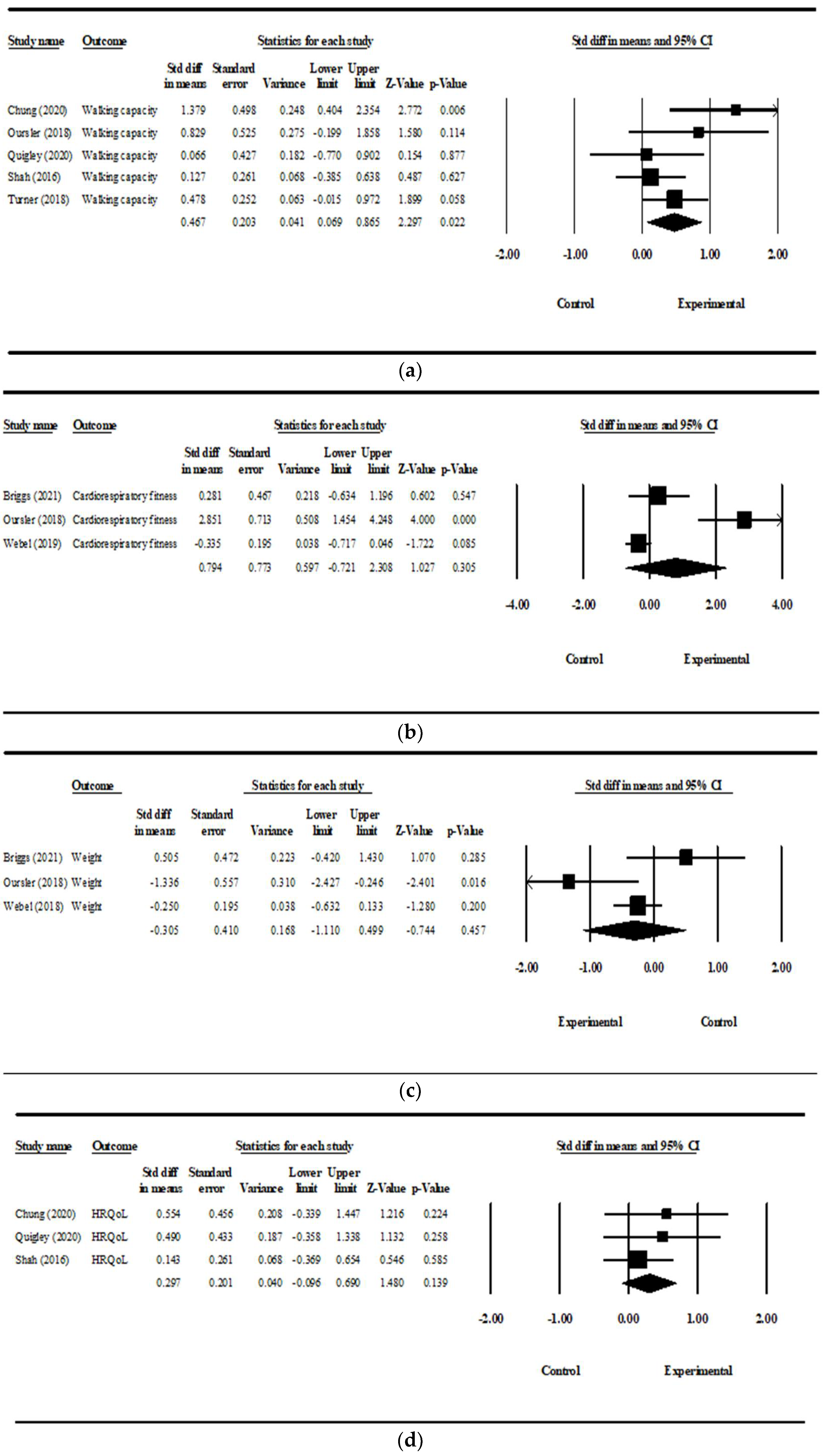
3.7. Effects of Physical Activity Interventions
3.8. Sensitivity Analysis and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marcus, J.L.; Chao, C.R.; Leyden, W.A.; Xu, L.; Quesenberry, C.P., Jr.; Klein, D.B.; Towner, W.J.; Horberg, M.A.; Silverberg, M.J. Narrowing the gap in life expectancy between HIV-infected and HIV-uninfected individuals with access to care. J. Acquir. Immune Defic. Syndr. 2016, 73, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samji, H.; Cescon, A.; Hogg, R.S.; Modur, S.P.; Althoff, K.N.; Buchacz, K.; Napravnik, S.; Rourke, S.B.; Sterling, T.R.; Silverberg, M.J.; et al. Closing the gap: Increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS ONE 2013, 8, e81355. [Google Scholar] [CrossRef] [PubMed]
- Wing, E.J. HIV and aging. Int. J. Infect. Dis. 2016, 53, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Joint United Nations Programme on HIV/AIDS [UNAIDS]. UNAIDS Program Coordinating Board Session on Ageing and HIV. Available online: https://www.unaids.org/sites/default/files/media_asset/20161125_UNAIDS_PCB39_HIV-Ageing_EN.pdf (accessed on 25 April 2022).
- Smit, M.; Brinkman, K.; Geerlings, S.; Smit, C.; Thyagarajan, K.; van Sighem, A.; de Wolf, F.; Hallett, T.B. Future challenges for clinical care of an ageing population infected with HIV: A modelling study. Lancet Infect. Dis. 2015, 15, 810–818. [Google Scholar] [CrossRef] [Green Version]
- Department of Health and Human Services (Panel on Antiretroviral Guidelines for Adults and Adolescents). Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Available online: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/archive/AdultandAdolescentGL_2021_08_16.pdf (accessed on 20 April 2022).
- Blanco, J.R.; Negredo, E.; Bernal, E.; Blanco, J. Impact of HIV infection on aging and immune status. Expert Rev. Anti-Infect. Ther. 2021, 19, 719–731. [Google Scholar] [CrossRef]
- Negredo, E.; Back, D.; Blanco, J.R.; Blanco, J.; Erlandson, K.M.; Garolera, M.; Guaraldi, G.; Mallon, P.; Moltó, J.; Serra, J.A.; et al. Aging in HIV-infected subjects: A new scenario and a new view. BioMed Res. Int. 2017, 2017, 5897298. [Google Scholar] [CrossRef] [Green Version]
- Alford, K.; Vera, J.H. Cognitive impairment in people living with HIV in the ART era: A review. Br. Med. Bull. 2018, 127, 55–68. [Google Scholar] [CrossRef]
- Rubin, L.H.; Maki, P.M. HIV, depression, and cognitive impairment in the era of effective antiretroviral therapy. Curr. HIV/AIDS Rep. 2019, 16, 82–95. [Google Scholar] [CrossRef]
- Erlandson, K.M.; Karris, M.Y. HIV and aging: Reconsidering the approach to management of comorbidities. Infect. Dis. Clin. 2019, 33, 769–786. [Google Scholar] [CrossRef]
- Ozemek, C.; Erlandson, K.M.; Jankowski, C.M. Physical activity and exercise to improve cardiovascular health for adults living with HIV. Prog. Cardiovasc. Dis. 2020, 63, 178–183. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Safreed-Harmon, K.; Kamarulzaman, A.; Anderson, J.; Leite, R.B.; Behrens, G.; Waters, L. Consensus statement on the role of health systems in advancing the long-term well-being of people living with HIV. Nat. Commun. 2021, 12, 4450. [Google Scholar] [CrossRef] [PubMed]
- Montoya, J.L.; Jankowski, C.M.; O’Brien, K.K.; Webel, A.R.; Oursler, K.K.; Henry, B.L.; Moore, D.J.; Erlandson, K.M. Evidence-informed practical recommendations for increasing physical activity among persons living with HIV. AIDS 2019, 33, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Mugisha, J.; Richards, J.; De Hert, M.; Probst, M.; Stubbs, B. Physical activity correlates in people living with HIV/AIDS: A systematic review of 45 studies. Disabil. Rehabil. 2018, 40, 1618–1629. [Google Scholar] [CrossRef] [Green Version]
- Briggs, B.C.; Ryan, A.S.; Sorkin, J.D.; Oursler, K.K. Feasibility and effects of high-intensity interval training in older adults living with HIV. J. Sports Sci. 2021, 39, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Oursler, K.K.; Sorkin, J.D.; Ryan, A.S.; Katzel, L.I. A pilot randomized aerobic exercise trial in older HIV-infected men: Insights into strategies for successful aging with HIV. PLoS ONE 2018, 13, e0198855. [Google Scholar] [CrossRef] [Green Version]
- Webel, A.R.; Jenkins, T.; Vest, M.; Oliveira, V.H.; Longenecker, C.T.; Liu, J.; Josephson, R. Cardiorespiratory fitness is associated with inflammation and physical activity in HIV+ adults. AIDS 2019, 33, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.N.; Majeed, Z.; Yoruk, Y.B.; Yang, H.; Hilton, T.N.; McMahon, J.M.; Hall, W.J.; Walck, D.; Luque, A.E.; Ryan, R.M. Enhancing physical function in HIV-infected older adults: A randomized controlled clinical trial. Health Psychol. 2016, 35, 563–573. [Google Scholar] [CrossRef]
- Zech, P.; Perez-Chaparro, C.; Schuch, F.; Wolfarth, B.; Rapp, M.; Heissel, A. Effects of aerobic and resistance exercise on cardiovascular parameters for people living with HIV: A meta-analysis. J. Assoc. Nurses AIDS Care 2019, 30, 186–205. [Google Scholar] [CrossRef]
- Quiles, N.N.; Piao, L.; Ortiz, A. The effects of exercise on lipid profile and blood glucose levels in people living with HIV: A systematic review of randomized controlled trials. AIDS Care 2020, 32, 882–889. [Google Scholar] [CrossRef]
- Ferrari, S.B.; Oliveira, G.H.D.; Ferraz Simões, C.; Vissoci, J.R.N.; Peres, S.B.; Moraes, S.M.F.D. Effects of exercise modality and intensity on the CD4 count in people with HIV: A systematic review and meta-analysis. AIDS Care 2022, 34, 163–172. [Google Scholar] [CrossRef]
- Heissel, A.; Zech, P.; Rapp, M.A.; Schuch, F.B.; Lawrence, J.B.; Kangas, M.; Heinzel, S. Effects of exercise on depression and anxiety in persons living with HIV: A meta-analysis. J. Psychosom. Res. 2019, 126, 109823. [Google Scholar] [CrossRef] [PubMed]
- Nosrat, S.; Whitworth, J.W.; Ciccolo, J.T. Exercise and mental health of people living with HIV: A systematic review. Chronic Illn. 2017, 13, 299–319. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.3 (Updated February 2022); John Wiley & Sons: Hoboken, NJ, USA, 2022; Available online: www.training.cochrane.org/handbook (accessed on 25 April 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; Turrini, F.; Meloni, A.; Plebani, M.; Brambilla, E.; Giordani, A.; Vitobello, C.; Caccia, R.; Piacentini, M.F.; La Torre, A.; et al. A mobile application for exercise intervention in people living with HIV. Med. Sci. Sports Exerc. 2020, 52, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk-of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.3 (Updated February 2022); John Wiley & Sons: Hoboken, NJ, USA, 2022; Available online: www.training.cochrane.org/handbook (accessed on 25 April 2022).
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.H.; Lou, V.W. Effects of supervised exercise on physical health and quality of life among older adults living with HIV in Hong Kong. J. Assoc. Nurses AIDS Care 2020, 31, 353–358. [Google Scholar] [CrossRef]
- Henry, B.L.; Moore, D.J. Preliminary findings describing participant experience with iSTEP, an mHealth intervention to increase physical activity and improve neurocognitive function in people living with HIV. J. Assoc. Nurses AIDS Care 2016, 27, 495–511. [Google Scholar] [CrossRef] [Green Version]
- Jemmott, J.B., III; Jemmott, L.S.; Zhang, J.; Icard, L.D.; Kelly, T.A.; Frank, I.; Bellamy, S.L. Effects of a health promotion intervention on physical activity in African American men Living with HIV: Randomized controlled trial. AIDS Patient Care STDS 2021, 35, 377–384. [Google Scholar] [CrossRef]
- Quigley, A.; Brouillette, M.J.; Gahagan, J.; O’Brien, K.K.; MacKay-Lyons, M. Feasibility and impact of a yoga intervention on cognition, physical function, physical activity, and affective outcomes among people living with HIV: A randomized controlled pilot trial. J. Int. Assoc. Provid. AIDS Care 2020, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Turner, B.J.; Liang, Y.; Simmonds, M.J.; Rodriguez, N.; Bobadilla, R.; Yin, Z. Randomized trial of chronic pain self-management program in the community or clinic for low-income primary care patients. J. Gen. Intern. Med. 2018, 33, 668–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webel, A.R.; Moore, S.M.; Longenecker, C.T.; Currie, J.; Davey, C.H.; Perazzo, J.; Abdus, S.; Josephson, R.A. A randomized controlled trial of the SystemCHANGE intervention on behaviors related to cardiovascular risk in HIV+ adults. J. Acquir. Immune Defic. Syndr. 2018, 78, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Cioe, P.A.; Merrill, J.E.; Gordon, R.E.; Guthrie, K.M.; Freiberg, M.; Williams, D.M.; Risica, P.M.; Kahler, C.W. Personalized feedback improves cardiovascular risk perception and physical activity levels in persons with HIV: Results of a pilot randomized clinical trial. AIDS Care 2021, 33, 786–794. [Google Scholar] [CrossRef] [PubMed]
- Morillo-Verdugo, R.; Robustillo-Cortés, M.D.L.A.; Martín-Conde, M.T.; Callejón-Callejón, G.; Cid-Silva, P.; Moriel-Sánchez, C.; Tortajada-Goitia, B.; Almeida-González, C.V. Effect of a structured pharmaceutical care intervention versus usual care on cardiovascular risk in HIV patients on antiretroviral therapy: INFAMERICA study. Ann. Pharmacother. 2018, 52, 1098–1108. [Google Scholar] [CrossRef]
- Chetty, L.; Cobbing, S.; Chetty, V. Physical Activity and Exercise for Older People Living with HIV: A Scoping Review. HIV/AIDS (Auckland) 2021, 13, 1079–1090. [Google Scholar] [CrossRef]
- Thomas, J.G.; Bond, D.S.; Raynor, H.A.; Papandonatos, G.D.; Wing, R.R. Comparison of smartphone-based behavioral obesity treatment with gold standard group treatment and control: A randomized trial. Obesity 2019, 27, 572–580. [Google Scholar] [CrossRef]
- Feinstein, M.J.; Hsue, P.Y.; Benjamin, L.A.; Bloomfield, G.S.; Currier, J.S.; Freiberg, M.S.; Grinspoon, S.K.; Levin, J.; Longenecker, C.T.; Post, W.S. Characteristics, prevention, and management of cardiovascular disease in people living with HIV: A scientific statement from the American Heart Association. Circulation 2019, 140, e98–e124. [Google Scholar] [CrossRef]
- Bijker, R.; Jiamsakul, A.; Uy, E.; Kumarasamy, N.; Ditango, R.; Chaiwarith, R.; Wong, W.W.; Avihingsanon, A.; Sun, L.P.; Yunihastuti, E.; et al. Cardiovascular disease-related mortality and factors associated with cardiovascular events in the TREAT Asia HIV Observational Database (TAHOD). HIV Med. 2019, 20, 183–191. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Saquetto, M.B.; Alves, I.G.; Martinez, B.P.; Vieira, J.P.B.; Brites, C. Effects of exercise interventions on aerobic capacity and health-related quality of life in people living with HIV/AIDS: Systematic review and network meta-analysis. Phys. Ther. 2021, 101, pzab092. [Google Scholar] [CrossRef]
- Enright, P.L.; McBurnie, M.A.; Bittner, V.; Tracy, R.P.; McNamara, R.; Arnold, A.; Newman, A.B. The 6-min walk test: A quick measure of functional status in elderly adults. Chest 2003, 123, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Cesareo, A.; Reni, G.; Biffi, E. Wearable inertial sensors to assess gait during the 6-minute walk test: A systematic review. Sensors 2020, 20, 2660. [Google Scholar] [CrossRef] [PubMed]
- Salvi, D.; Poffley, E.; Orchard, E.; Tarassenko, L. The mobile-based 6-minute walk test: Usability study and algorithm development and validation. JMIR Mhealth Uhealth 2020, 8, e13756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, B.R.; McDowell, C.P.; Hallgren, M.; Meyer, J.D.; Lyons, M.; Herring, M.P. Association of efficacy of resistance exercise training with depressive symptoms: Meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiatry 2018, 75, 566–576. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Country | Target Population | Age (Mean, Years) | Sample Size (Recruitment) | Sex | ||
|---|---|---|---|---|---|---|---|
| IG | CG | IG | CG | ||||
| Interventions focused only on physical activity | |||||||
| Bonato (2020) [27] | Italy | Adults living with HIV | 52.0 a | 50.0 a | 20 | 18 | 82.4% male |
| Briggs (2021) [16] | US | Sedentary adults living with HIV who were 50 years and older | 63.4 | 60.1 | 13 | 13 | 94.7% male |
| Chung (2020) [33] | Hong Kong | Physically inactive adults living with HIV | 66.5 | 70.3 | 11 | 10 | 75% male |
| Henry (2016) [34] | US | Adults with HIV-associated neurocognitive impairment diagnosis | 49.6 | 51.8 | 11 | 10 | 85.7% male |
| Oursler (2018) [17] | US | Sedentary adults living with HIV who were 50 years and older | 57.4 | 57.4 | 11 | 11 | 100% male |
| Quigley (2020) [36] | Canada | Adults living with HIV | 50.7 | 60.2 | 11 | 11 | 68.2% male |
| Shah (2016) [19] | US | Adults living with HIV with mild-to-moderate functional limitations | 54.6 | 56.2 | 33 | 34 | 61.0% male |
| Interventions involving physical activity | |||||||
| Cioe (2021) [39] | US | Adults living with HIV | 48.8 | 53.9 | 19 | 21 | 60.0% male |
| Jemmott (2021) [35] | US | African American middle-aged men living with HIV | 53.6 | 54.2 | 152 | 150 | 100.0% male |
| Morillo-Verdugo (2018) [40] | Spain | Adults living with HIV receiving ART with at least 1 drug for the treatment of CVD or diabetes and at a moderate or high risk of CVD | 53.6 b | 53.6 b | 26 | 33 | 90.6% male |
| Turner (2018) [37] | US | Adults living with HIV with chronic lower back or lower extremity pain, and who were prescribed opioid analgesics | 56.9 | 56.2 | 53 | 58 | 45.0% male |
| Webel (2018) [38]; Webel (2019) [18] | US | Adults living with HIV at high risk for developing CVD | 52.3 | 53.3 | 54 | 53 | 64.5% male |
| First Author (Year) | Title of Intervention | Intervention Description | Mode of Delivery | Period; Time/Session; Frequency | Provider of Intervention | Comparison Condition | Intervention Adherence |
|---|---|---|---|---|---|---|---|
| Interventions focused only on physical activity | |||||||
| Bonato (2020) [27] | A mobile application and aerobic exercise intervention (Progetto appfitness) | (1) Weeks 1–4, with direct coach supervision, with training intensity set at 60–70% of maximal heart rate; (2) Weeks 5–16, without coach supervision, at a training intensity of 70–80% of maximal heart rate, which is expected to improve aerobic fitness, (3) a weekly notification of training plan and prescription through the mobile app | Face-to-face and mobile application | 16 weeks; 1 h; 3 times/week | Professional coach | Aerobic exercise excluding mobile application use | (1) Coach supervision (weeks 1–4): 100%; (2) autonomous training (weeks 5–16): 60% (median) |
| Briggs (2021) [16] | High-intensity interval AEX combined with resistance training | (1) Weeks 1–4, participants started at 50–60% HRR for 15 min and were progressed until they reached at least 30 min at 60% HRR; (2) weeks 5–16, the intensity was increased as tolerated to 70–80% HRR, and duration was titrated to the goal of 30–40 min of high-intensity AEX | Face-to-face | 16 weeks; 15–45 min; 3 times/week | Exercise physiologist | Unchanged physical activity level and then delayed high-intensity interval training combined with resistance training | Median attendance rate: 89% |
| Chung (2020) [33] | Supervised exercise | Moderate-intensity exercise (maintained 50–70% of heart rate) combined with aerobic and resistance training in the form of group-based training sessions for two to three participants | Face-to-face | 8 weeks; 45 min; 2 times/week | Physiotherapist | Being advised to continue routine daily activities, and self-motivated exercise was allowed | 96.3% program attendance rate to completion |
| Henry (2016) [34] | iSTEP (SMS/MMS intervention) | Interactive and personalized daily text messages, step count monitoring with a pedometer, text, and MMS feedback of physical activity changes over time, message reminders tailored to each participant’s barriers and preferred activities, and weekly goal-setting | Mobile phone | 16 weeks; not reported; 3 times/day | N/A | Text messages 3 times a day throughout the 16 weeks about HIV symptoms and mood | (1) Responding to text messages: 89%; (2) reporting the daily step counts: 92% |
| Oursler (2018) [17] | High-intensity aerobic exercise | Starting with aerobic exercise training for 20–30 min at 50–60% of HRR, progressively increasing by 10% of HRR each week so that within 5–7 weeks the aerobic exercise sessions lasted 30–45 min at 70–85% of HRR and at the end of the 16 weeks lasted 40–45 min at 75–90% of HRR | Face-to-face | 16 weeks; 20–45 min; 3 times/week | Exercise physiologist | Moderate-intensity aerobic exercise | Mean attendance rate: 89% |
| Quigley (2020) [36] | Yoga intervention | Group-based yoga classes with classes consisting of seated meditation, breathing exercises, shoulder, neck, and back stretches, and sun salutations (either seated or standing), standing poses, balance poses, abdominal and back-bend poses, and cool-down stretches and final rest | Face-to-face | 12 weeks; 60 min; 3 times/week | Yoga instructor | Usual care | Mean attendance rate: 82% |
| Shah (2016) [19] | Physical activity counseling intervention based on self-determination theory | Counseling program for personal decision making, while giving the support needed to ensure proper education: (1) the first counseling session (60-min): understanding participants’ interests, values, and behaviors and encouraging them to discuss barriers to physical activity and solutions to overcoming them; (2) autonomy supportive sessions: follow-up telephone counseling sessions to facilitate setting appropriate physical activity goals | Face-to-face and telephone calls | 12 weeks; 60 min for 1st session, 15–30 min for phone calls; 2 times/month | Physician and mental health therapist, physical therapist | Usual care | 93% of participants participated in at least four out of six counseling sessions |
| Interventions combining physical activity with other health-related contents | |||||||
| Cioe (2021) [39] | CVD-PRAI | Personalized feedback and motivational interviewing: (1) Session 1, discussion of CVD risk and modifiable risk factors, advice for behavior change and setting goals, and providing related literature; (2) Session 2, summary of the prior session, review of goals, addressing barriers to change, and discussion of strategies for maintaining long-term behavior change | Face-to-face and mobile phone (text message) | 4 weeks; 45 min; 2 sessions; daily text message during week 1, weekly during week 2–4 | Nurse | Brief health education to improve heart-healthy behaviors | 90% of participants completed all sessions |
| Jemmott (2021) [35] | “Men Together Making a Difference” health promotion intervention | Brainstorming, educational games, and interactive activities including physical exercise and videos, to increase adherence to guidelines for physical activity, diet, and colon cancer screening | Face-to-face | 3 weeks; 1 h; 3 times/week | Trained facilitator | One 60-min small group session | 100% of participants attended 1st week and 97% attended 2nd and 3rd week |
| Morillo-Verdugo (2018) [40] | Structured pharmaceutical care intervention | Intensive pharmaceutical care to reduce cardiovascular risk: (1) pharmacotherapeutic follow-up of all medication taken by the patient to work toward achieving pharmacotherapeutic objectives related to cardiovascular risk; (2) recommendations for improving diet, exercise, and smoking cessation; (3) providing leaflets on cardiovascular risk prevention and an individual motivational interview; (4) periodic contacts by sending text messages with content related to healthy living habits and health promotion | Face-to-face, leaflet, and mobile phone (text message) | 48 weeks; not reported; 5 visits/48 weeks; weekly text message during week 1–4, then periodically until the end of the follow-up period | Pharmacist | Unchanged physical activity level | Not reported |
| Turner (2018) [37] | “Living Better Beyond Pain" program (chronic pain self-management program) | Pain self-management program: (1) one-on-one lectures for pain self-management topics and exercise demonstration; (2) providing additional materials included activity logs with personal goals, program DVDs (walking exercises, self-massage techniques), exercise mats, tennis balls for massage, and multi-pronged self-massage tools | Face-to-face and telephone | 24 weeks; 30–45 min; 6 times/6 months; at least one phone call between visits | Health educator | Pain self-management program in the community setting | 62.1% of participants completed all measures; 36% attended all of meetings |
| Webel (2018) [38]; Webel (2019) [19] | Lifestyle behavior intervention (“System CHANGE") | Group sessions for: (1) behavior change techniques to achieve a specific participant-defined goal to improve lifestyle behaviors (physical activity and diet); (2) education that emphasized a diet consisting of low-energy-density foods through increased fresh fruits, vegetables, and whole grains; (3) discussion about the types of physical activity, issues that may interfere with sufficient activity, and techniques to modify the participants’ physical environment to encourage activity and eating a healthy diet; (4) discussion on how to incorporate healthy eating and physical activity into the participant’s daily routine | Face-to-face | 6 weeks; 1 h; 1 time/week | Health educator | Pamphlet that contained information on healthy eating and physical activity | 90% of the participants attended at least half of the sessions and 60% attended at least 5 sessions |
| Health Outcomes | How Assessed (Studies That Assessed the Outcomes) |
|---|---|
| Walking capacity | |
| 6-min walk | Measuring the distance a participant walked in six minutes for evaluaton of walking capacity [17,19,33,37] |
| Gait speed | Measuring the time it takes to walk a specific distance as quickly and safely as possible for evaluation of dynamic balance performance [19,36] |
| Cardiorespiratory fitness | |
| VO2 peak | Measuring oxygen uptake at peak exercise performance during graded exercise test by treadmill [16,17,27] or bicycle ergometer [18] for evaluation of cardiorespiratory fitness |
| Time on treadmill | Measuring total exercise duration of a graded exercise treadmill test for evaluation of exercise endurance [16,17] |
| Body composition and weight | |
| Body fat percent | Calculating total fat mass divided by total body mass after measuring fat mass and lean mass by dual-energy X-ray absorptiometry [16,17] or bioimpedentiometry [27] |
| Fat mass | Measuring fat mass by dual-energy X-ray absorptiometry [16,17] |
| Weight | Measuring body weight using a scale [16,17,38] |
| Metabolic parameters | |
| Total cholesterol | Testing total cholesterol by laboratory analysis after overnight fasting and blood draw [16,17,27,40] |
| LDL cholesterol | Testing low-density lipoprotein (LDL) cholesterol by laboratory analysis after overnight fasting and blood draw [16,17,27,40] |
| HDL cholesterol | Testing high-density lipoprotein (HDL) cholesterol by laboratory analysis after overnight fasting and blood draw [16,17,27,40] |
| Triglycerides | Testing triglyceride by laboratory analysis after overnight fasting and blood draw [16,17,27,40] |
| Psychological profile | |
| Depression | Assessing depressive symptoms using self-reported questionnaires such as Beck Depression Inventory-II [19], Psychological Monitoring of Overtraining and Staleness [27], and Hospital Anxiety and Depression Scale [36] |
| Health-related quality of life | Assessing health-related quality of life using self-reported questionnaires such as Short-Form Health Survey (36-item) [19,33], and Medical Outcomes Survey-HIV [36] |
| Study Omitted | Pooled Estimate | 95% Confidence Interval | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Chung (2020) [33] | 0.323 | 0.011 | 0.634 | 0.042 |
| Oursler (2018) [17] | 0.426 | −0.028 | 0.879 | 0.066 |
| Quigley (2020) [36] | 0.560 | 0.092 | 1.028 | 0.019 |
| Shah (2016) [19] | 0.607 | 0.130 | 1.085 | 0.013 |
| Turner (2018) [37] | 0.507 | −0.076 | 1.090 | 0.088 |
| Pooled (random effect) | 0.467 | 0.069 | 0.865 | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, M.-S.; Noh, D. Effects of Physical Activity Interventions on Health Outcomes among Older Adults Living with HIV: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8439. https://doi.org/10.3390/ijerph19148439
Shim M-S, Noh D. Effects of Physical Activity Interventions on Health Outcomes among Older Adults Living with HIV: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(14):8439. https://doi.org/10.3390/ijerph19148439
Chicago/Turabian StyleShim, Mi-So, and Dabok Noh. 2022. "Effects of Physical Activity Interventions on Health Outcomes among Older Adults Living with HIV: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 14: 8439. https://doi.org/10.3390/ijerph19148439
APA StyleShim, M.-S., & Noh, D. (2022). Effects of Physical Activity Interventions on Health Outcomes among Older Adults Living with HIV: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(14), 8439. https://doi.org/10.3390/ijerph19148439